


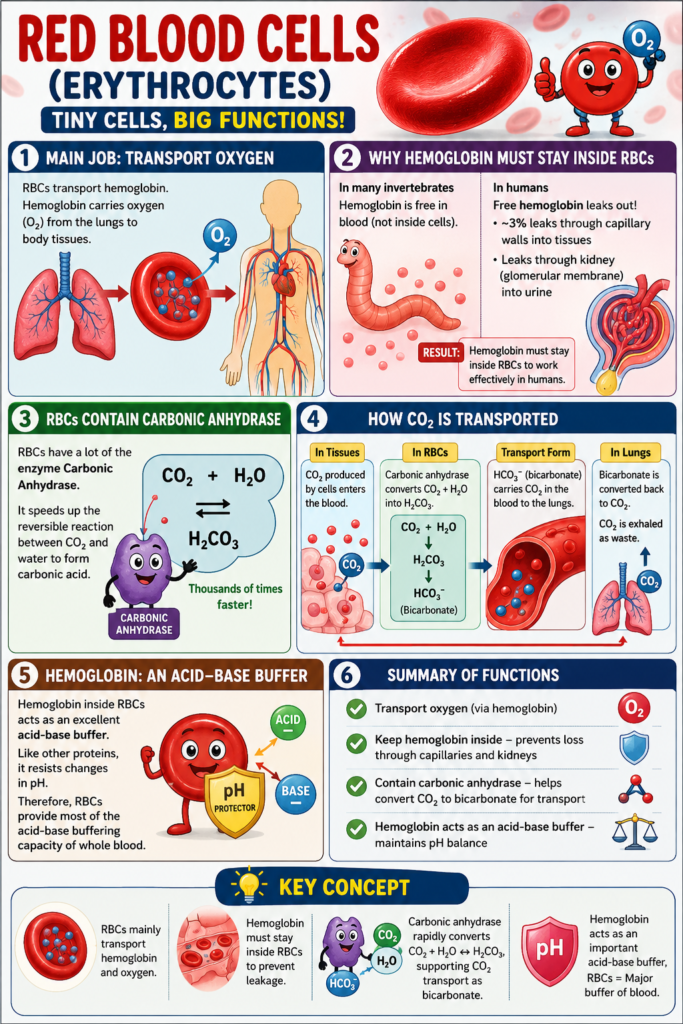
- Red blood cells (RBCs), also called erythrocytes, mainly transport hemoglobin.
- Hemoglobin carries oxygen from the lungs to the body tissues.
- In many invertebrate animals, hemoglobin circulates freely in the blood and is not enclosed inside RBCs.
- In humans, if hemoglobin is free in the plasma, about 3% leaks through the capillary membrane into the tissue spaces each time blood passes through the capillaries.
- Free hemoglobin can also leak through the glomerular membrane of the kidneys into the glomerular filtrate.
- Therefore, hemoglobin must remain inside RBCs to perform its function effectively in humans.
- RBCs have important functions other than carrying hemoglobin.
- They contain a large amount of the enzyme carbonic anhydrase.
- Carbonic anhydrase speeds up the reversible reaction between carbon dioxide (CO₂) and water (H₂O) to form carbonic acid (H₂CO₃).
- This enzyme increases the reaction speed by several thousand times.
Reaction:
CO₂ + H₂O ⇌ H₂CO₃
- Because this reaction is very fast, blood can transport large amounts of carbon dioxide as bicarbonate ions (HCO₃⁻).
- Bicarbonate carries carbon dioxide from the tissues to the lungs.
- In the lungs, bicarbonate is converted back into carbon dioxide (CO₂).
- The carbon dioxide is then exhaled as a waste product.
- Hemoglobin inside RBCs is an excellent acid-base buffer.
- Like most proteins, hemoglobin helps resist changes in pH.
- Therefore, RBCs provide most of the acid-base buffering capacity of whole blood.
KEY CONCEPT
- The main function of RBCs is to transport hemoglobin and oxygen.
- Hemoglobin must stay inside RBCs to prevent loss through capillaries and kidneys.
- RBCs contain carbonic anhydrase, which rapidly converts CO₂ and water into carbonic acid and supports CO₂ transport as bicarbonate.
- Hemoglobin also acts as an important acid-base buffer, making RBCs the major buffering component of whole blood.
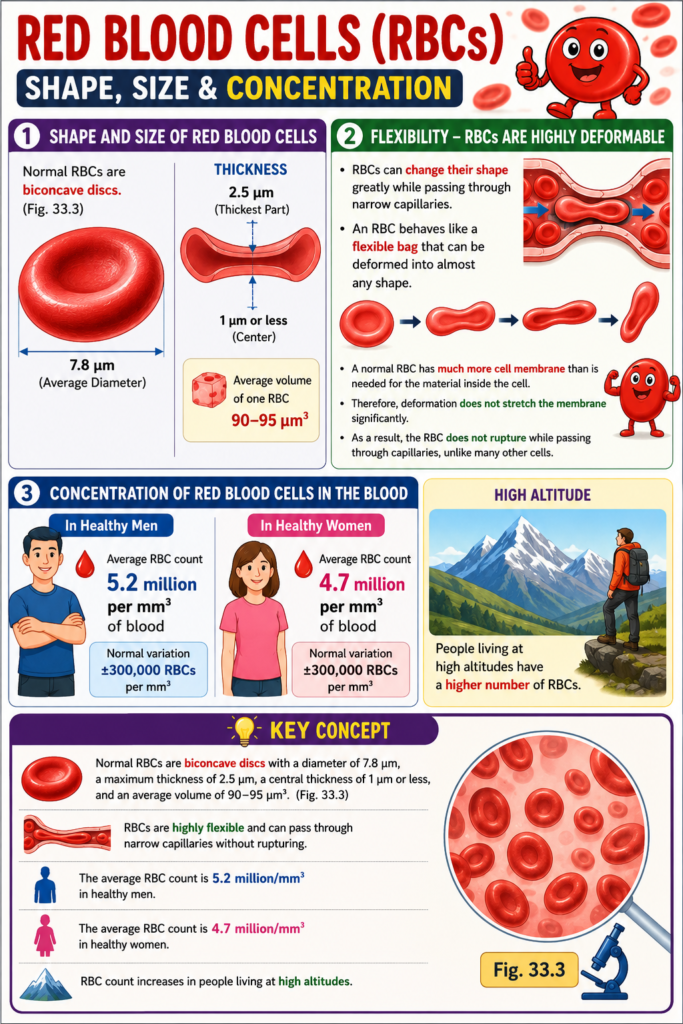
Shape and Size of Red Blood Cells
- Normal RBCs are biconcave discs.
- (Fig. 33.3)
- The average diameter of a normal RBC is about 7.8 micrometers (µm).
- The thickness at the thickest part is about 2.5 micrometers (µm).
- The thickness at the center is about 1 micrometer (µm) or less.
- The average volume of one RBC is 90–95 cubic micrometers (µm³).
- RBCs can change their shape greatly while passing through narrow capillaries.
- An RBC behaves like a flexible bag that can be deformed into almost any shape.
- A normal RBC has much more cell membrane than is needed for the material inside the cell.
- Therefore, deformation does not stretch the membrane significantly.
- As a result, the RBC does not rupture while passing through capillaries, unlike many other cells.
Concentration of Red Blood Cells in the Blood
- In healthy men, the average RBC count is 5.2 million per cubic millimeter (mm³) of blood.
- Normal variation is ±300,000 RBCs per cubic millimeter.
- In healthy women, the average RBC count is 4.7 million per cubic millimeter (mm³) of blood.
- Normal variation is ±300,000 RBCs per cubic millimeter.
- People living at high altitudes have a higher number of RBCs.
KEY CONCEPT
- Normal RBCs are biconcave discs with a diameter of 7.8 µm, a maximum thickness of 2.5 µm, a central thickness of 1 µm or less, and an average volume of 90–95 µm³.
- (Fig. 33.3)
- RBCs are highly flexible and can pass through narrow capillaries without rupturing.
- The average RBC count is 5.2 million/mm³ in healthy men and 4.7 million/mm³ in healthy women, with higher counts in people living at high altitudes.
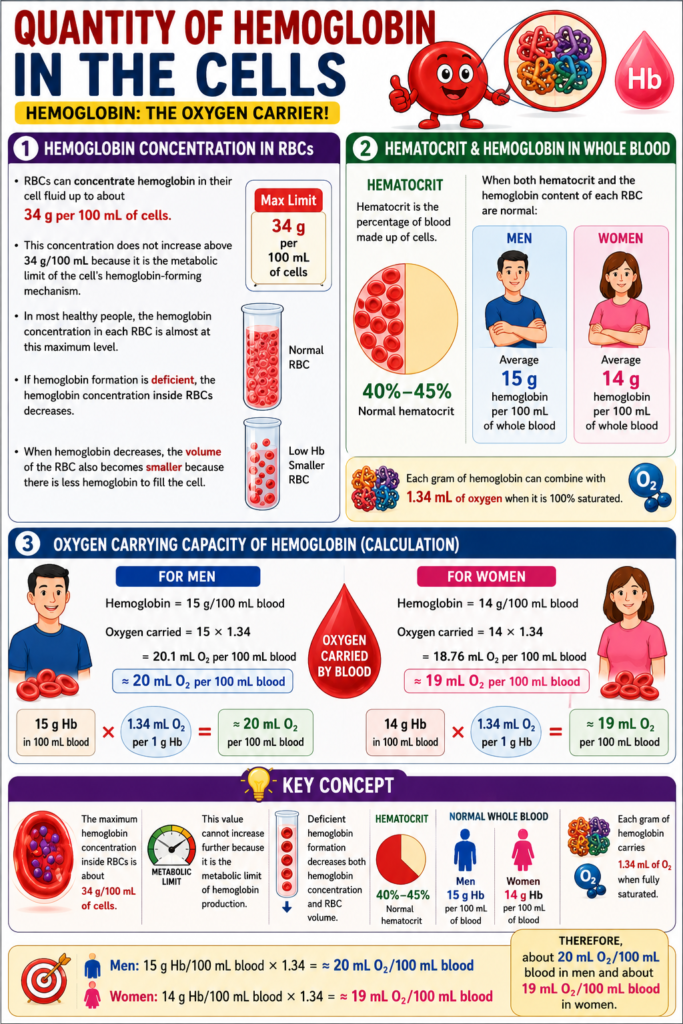
Quantity of Hemoglobin in the Cells
- RBCs can concentrate hemoglobin in their cell fluid up to about 34 g per 100 mL of cells.
- This concentration does not increase above 34 g/100 mL because it is the metabolic limit of the cell’s hemoglobin-forming mechanism.
- In most healthy people, the hemoglobin concentration in each RBC is almost at this maximum level.
- If hemoglobin formation is deficient, the hemoglobin concentration inside RBCs decreases.
- When hemoglobin decreases, the volume of the RBC also becomes smaller because there is less hemoglobin to fill the cell.
- Hematocrit is the percentage of blood made up of cells.
- The normal hematocrit is 40%–45%.
- When both the hematocrit and the hemoglobin content of each RBC are normal:
- Men have an average of 15 g of hemoglobin per 100 mL of whole blood.
- Women have an average of 14 g of hemoglobin per 100 mL of whole blood.
- Each gram of hemoglobin can combine with 1.34 mL of oxygen when it is 100% saturated.
Calculation
For Men:
- Hemoglobin = 15 g/100 mL blood
- Oxygen carried = 15 × 1.34
- = 20.1 mL O₂ per 100 mL blood
- ≈ 20 mL O₂ per 100 mL blood
For Women:
- Hemoglobin = 14 g/100 mL blood
- Oxygen carried = 14 × 1.34
- = 18.76 mL O₂ per 100 mL blood
- ≈ 19 mL O₂ per 100 mL blood
KEY CONCEPT
- The maximum hemoglobin concentration inside RBCs is about 34 g/100 mL of cells.
- This value cannot increase further because it is the metabolic limit of hemoglobin production.
- Deficient hemoglobin formation decreases both hemoglobin concentration and RBC volume.
- Normal hematocrit is 40%–45%.
- Normal whole blood contains about 15 g hemoglobin/100 mL in men and 14 g/100 mL in women.
- Each gram of hemoglobin carries 1.34 mL of oxygen when fully saturated.
- Therefore, about 20 mL O₂/100 mL blood can be carried in men and about 19 mL O₂/100 mL blood in women.
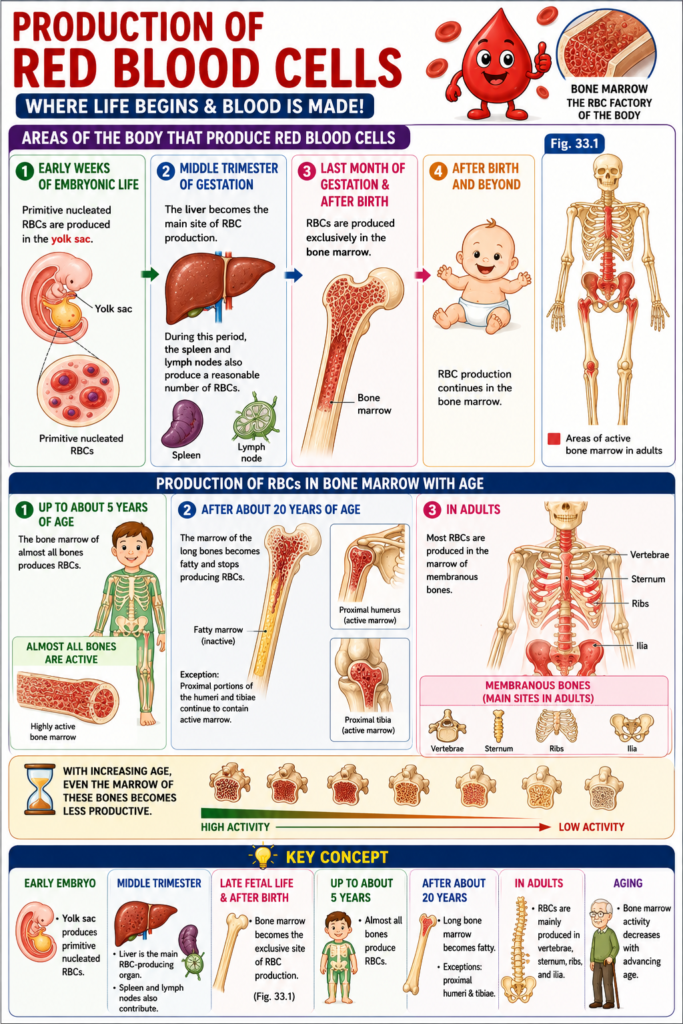
PRODUCTION OF RED BLOOD CELLS
Areas of the Body That Produce Red Blood Cells
- During the early weeks of embryonic life, primitive nucleated RBCs are produced in the yolk sac.
- During the middle trimester of gestation, the liver becomes the main site of RBC production.
- During this period, the spleen and lymph nodes also produce a reasonable number of RBCs.
- During the last month of gestation and after birth, RBCs are produced exclusively in the bone marrow.
- (Fig. 33.1)
- Until about 5 years of age, the bone marrow of almost all bones produces RBCs.
- After about 20 years of age, the marrow of the long bones becomes fatty and stops producing RBCs.
- The proximal portions of the humeri and tibiae are exceptions and continue to contain active marrow.
- After 20 years of age, most RBCs are produced in the marrow of membranous bones.
- These membranous bones include the vertebrae, sternum, ribs, and ilia.
- With increasing age, even the marrow of these bones becomes less productive.
KEY CONCEPT
- Early embryo: Yolk sac produces primitive nucleated RBCs.
- Middle trimester: Liver is the main RBC-producing organ; spleen and lymph nodes also contribute.
- Late fetal life and after birth: Bone marrow becomes the exclusive site of RBC production.
- (Fig. 33.1)
- Up to about 5 years: Almost all bones produce RBCs.
- After about 20 years: Long bone marrow becomes fatty, except the proximal humeri and tibiae.
- In adults: RBCs are mainly produced in the vertebrae, sternum, ribs, and ilia.
- Bone marrow activity decreases with advancing age.
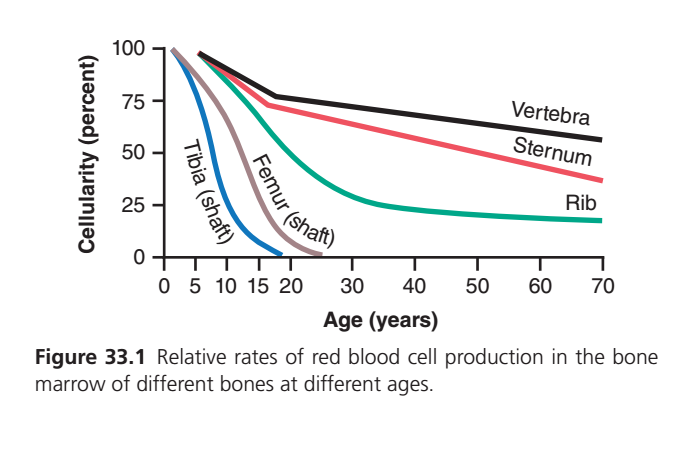
This graph is one of the most important physiology graphs for understanding how red bone marrow (hematopoietic marrow) changes with age. If you understand the concept behind each line, you will never have to memorize it.
Figure Concept
What is this graph showing?
The graph shows:
How much red blood cell (RBC) production occurs in the bone marrow of different bones at different ages.
Remember:
- 100% cellularity = Bone marrow is almost completely active in making blood cells (red marrow).
- 0% cellularity = Bone marrow has become yellow marrow (fatty marrow) and no longer produces significant RBCs.
First Understand the Axes
X-axis (Horizontal)
Age (Years)
Moves from:
Birth → Childhood → Teenage → Adult → Old age
Y-axis (Vertical)
Cellularity (%)
This means:
How much of the bone marrow is active blood-forming marrow.
Example:
| Cellularity | Meaning |
|---|---|
| 100% | Almost all marrow is producing blood cells |
| 75% | Most marrow still active |
| 50% | Half active, half fatty |
| 25% | Mostly fatty marrow |
| 0% | Almost completely yellow marrow |
Basic Rule to Remember
At Birth
Almost every bone in the body contains red marrow.
Therefore,
Every line starts near 100%.
Why?
Because a newborn is growing rapidly and needs enormous numbers of blood cells.
As Age Increases…
Something important happens.
Red marrow slowly changes into yellow marrow.
This process is called
Marrow conversion
Red marrow
↓
Yellow (fatty) marrow
↓
Less RBC production
Now Understand Each Line
① Tibia (Blue Line)
This is the fastest falling line.
What happens?
Birth
↓
Very active marrow
↓
Rapid decline during childhood
↓
Almost zero by about 20 years.
Why?
The tibia shaft is a long bone.
Long bone shafts are the first bones to lose red marrow.
Nature says:
“We don’t need blood production here anymore.”
So the marrow becomes fatty very early.
Easy Story
Imagine the tibia is a factory.
At birth:
100 workers.
Age 5:
70 workers.
Age 10:
30 workers.
Age 15:
5 workers.
Age 20:
Factory closed.
No more RBC production.
MBBS Pearl
Adult tibial shaft is not an important site for bone marrow aspiration.
② Femur Shaft (Gray Line)
This line falls slightly slower than tibia.
At birth
↓
Very active
↓
Gradual decline
↓
Almost inactive by about 25 years.
Why slower than tibia?
Although both are long bones,
Femur is larger.
It keeps active marrow slightly longer.
Easy Story
The femur factory survives a few extra years compared with the tibia.
Eventually,
It also closes.
Compare Tibia vs Femur
| Tibia | Femur |
|---|---|
| Stops earlier | Stops later |
| Small long bone | Larger long bone |
| Red marrow disappears first | Disappears slightly later |
Important Clinical Point
Adult femoral shaft also has very little red marrow.
Most marrow becomes fat.
③ Rib (Green Line)
Now notice something different.
The line falls,
but never reaches zero.
Birth
↓
100%
↓
Falls gradually
↓
Around adulthood about 25%
↓
Old age still around 15–20%.
Why?
Ribs belong to the axial skeleton.
Axial bones continue producing blood throughout life.
Although activity decreases,
they never completely stop.
Easy Story
The rib factory becomes smaller,
but it never shuts down.
Clinical Importance
Even in old people,
Ribs continue contributing to blood cell production.
④ Sternum (Red Line)
This line decreases even more slowly.
Birth
↓
Highly active
↓
Gradual decline
↓
Still around 40% active at 70 years.
Why?
The sternum is one of the major adult hematopoietic bones.
Its marrow remains red throughout life.
Clinical Importance
Doctors often perform
sternal bone marrow aspiration
because the marrow remains active.
Easy Story
The sternum factory never closes.
It simply reduces the number of workers.
⑤ Vertebra (Black Line)
This is the highest line.
It remains the most active throughout life.
Birth
↓
Nearly 100%
↓
Small decline
↓
Still more than half active even at 70 years.
Why?
Vertebrae are the most important site of adult hematopoiesis.
Your body wants one central place to continue making blood cells throughout life.
That place is the vertebral marrow.
Easy Story
If every factory closes,
the vertebral factory keeps running.
It becomes the body’s main blood-producing center.
Compare All Bones
| Bone | Childhood | Adult | Old Age |
|---|---|---|---|
| Tibia shaft | Very active | Almost none | None |
| Femur shaft | Very active | Almost none | None |
| Rib | Moderately active | Still active | Still active |
| Sternum | Highly active | Highly active | Moderately active |
| Vertebra | Highly active | Highest activity | Highest activity |
Why Does Nature Do This?
Blood production is expensive.
It requires:
- Nutrients
- Oxygen
- Space
- Stem cells
Instead of keeping every bone active forever,
the body concentrates blood formation into axial bones.
This is much more efficient.
Adult Sites of RBC Production (Very High-Yield MBBS Point)
After about 20 years of age, most RBCs are produced in:
- Vertebrae (most active) ⭐⭐⭐⭐⭐
- Sternum
- Ribs
- Pelvis (iliac crest) ⭐⭐⭐⭐⭐
- Skull (small contribution)
- Proximal ends of humerus and femur (limited contribution)
The shafts of long bones (e.g., tibia and femur) contribute very little or not at all in healthy adults.
Clinical Correlation
Bone marrow aspiration
Doctors usually obtain bone marrow samples from:
- Posterior iliac crest (most common site)
- Sternum (selected cases)
Why not the tibia or femoral shaft in adults?
Because these shafts have mostly yellow (fatty) marrow, with minimal blood-forming activity.
One-Line Memory Trick
“Long bone shafts retire early; axial skeleton works for life.”
- Tibia → stops first
- Femur → stops next
- Rib → keeps working slowly
- Sternum → remains active for life
- Vertebra → remains the most active blood-forming site throughout life
KEY CONCEPT
- At birth, almost all bone marrow is red and actively produces RBCs.
- With increasing age, red marrow is gradually replaced by yellow (fatty) marrow, reducing cellularity.
- Long bone shafts (tibia and femur) lose hematopoietic activity early in life.
- Axial skeleton bones (vertebrae, sternum, ribs, and pelvis) retain red marrow and continue producing blood cells throughout adulthood.
- Among all bones, vertebrae maintain the highest marrow cellularity, making them one of the most important lifelong sites of hematopoiesis.
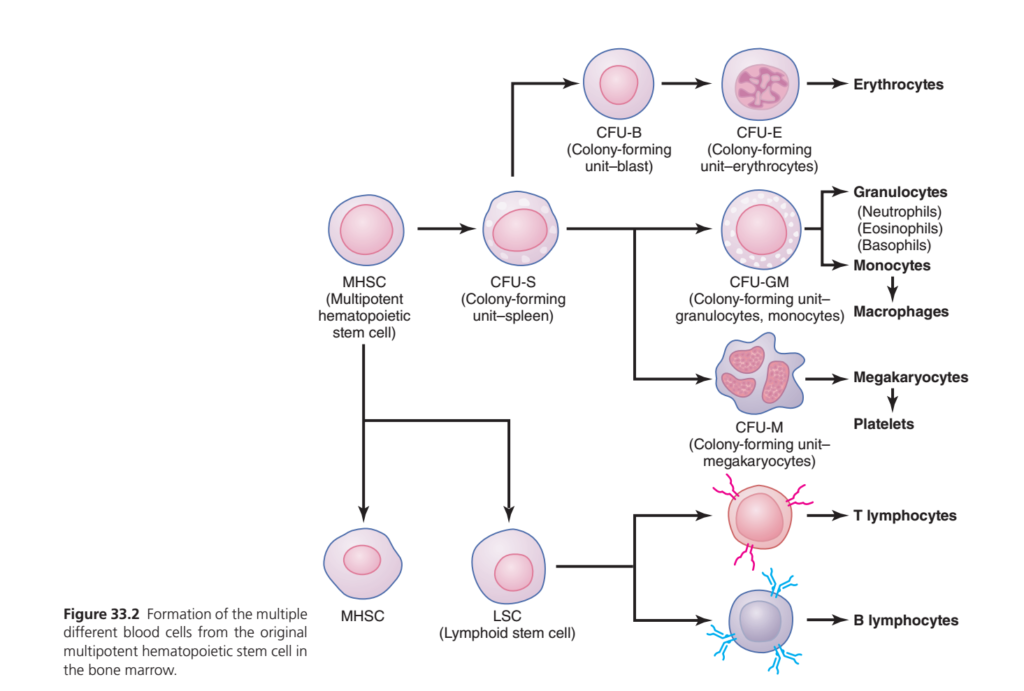
Genesis of Blood Cells
- All blood cells begin their life in the bone marrow.
- They originate from a single type of cell called the multipotent hematopoietic stem cell (MHSC).
- All circulating blood cells are ultimately derived from this stem cell.
- (Fig. 33.2)
- The multipotent hematopoietic stem cell divides repeatedly to produce different types of blood cells.
- A small number of newly formed stem cells remain unchanged.
- These unchanged stem cells stay in the bone marrow to maintain the stem cell supply.
- The number of these stem cells decreases with increasing age.
- Most newly formed stem cells differentiate into other blood cell types shown in Fig. 33.2.
- These intermediate cells are called committed progenitor cells.
- Different hematopoietic progenitor cells produce colonies of specific blood cells when grown in culture.
- A committed progenitor cell that produces erythrocytes is called colony-forming unit–erythrocyte (CFU-E).
- CFU-E gives rise to red blood cells (erythrocytes).
- A committed progenitor cell that produces granulocytes and monocytes is called colony-forming unit–granulocyte, monocyte (CFU-GM).
- Other colony-forming units produce their own specific blood cell types.
- Growth and reproduction of stem cells are controlled by proteins called growth inducers.
- At least four major growth inducers have been identified.
- One growth inducer, interleukin-3 (IL-3), stimulates the growth and reproduction of almost all committed stem cells.
- Other growth inducers stimulate only specific types of stem cells.
- Growth inducers increase the growth of stem cells but do not cause their differentiation.
- Differentiation is controlled by another group of proteins called differentiation inducers.
- Each differentiation inducer causes a specific committed stem cell to mature one or more steps toward a final adult blood cell.
- The production of growth inducers and differentiation inducers is controlled by factors outside the bone marrow.
- For RBCs, prolonged exposure to low oxygen levels stimulates growth, differentiation, and production of large numbers of RBCs.
- For white blood cells, infectious diseases stimulate growth, differentiation, and production of the specific white blood cells needed to fight the infection.
KEY CONCEPT
- All blood cells originate from the multipotent hematopoietic stem cell (MHSC) in the bone marrow.
- (Fig. 33.2)
- Some stem cells remain in the bone marrow to maintain the stem cell pool, while most become committed progenitor cells.
- CFU-E forms erythrocytes (RBCs), and CFU-GM forms granulocytes and monocytes.
- Growth inducers stimulate stem cell growth and reproduction.
- Interleukin-3 (IL-3) stimulates the growth of almost all committed stem cells.
- Differentiation inducers convert committed stem cells into mature blood cells.
- Low oxygen increases RBC production, while infections increase white blood cell production.

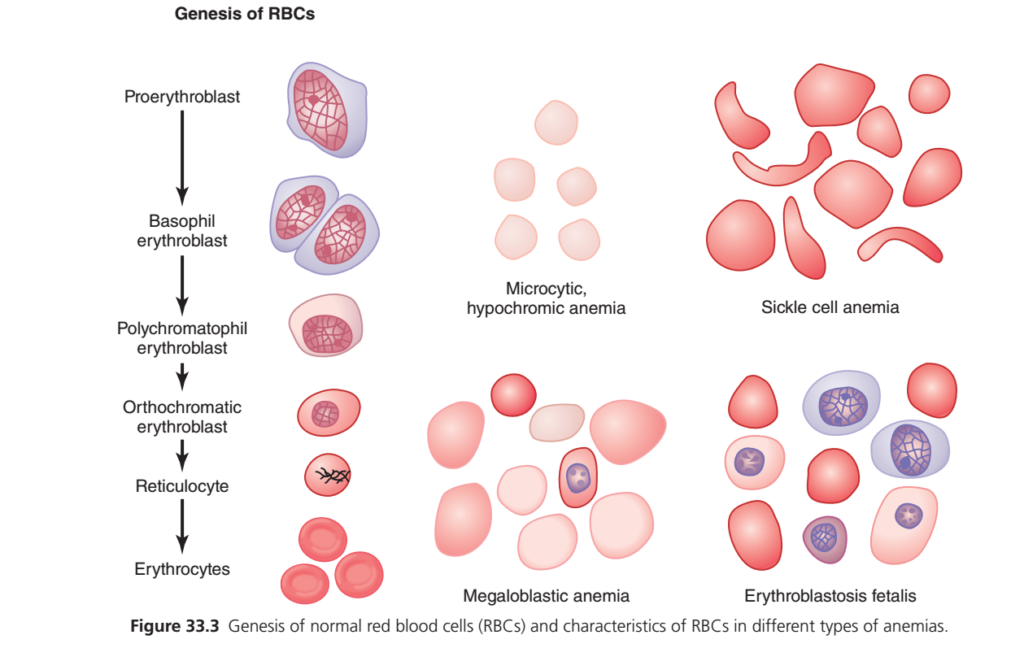
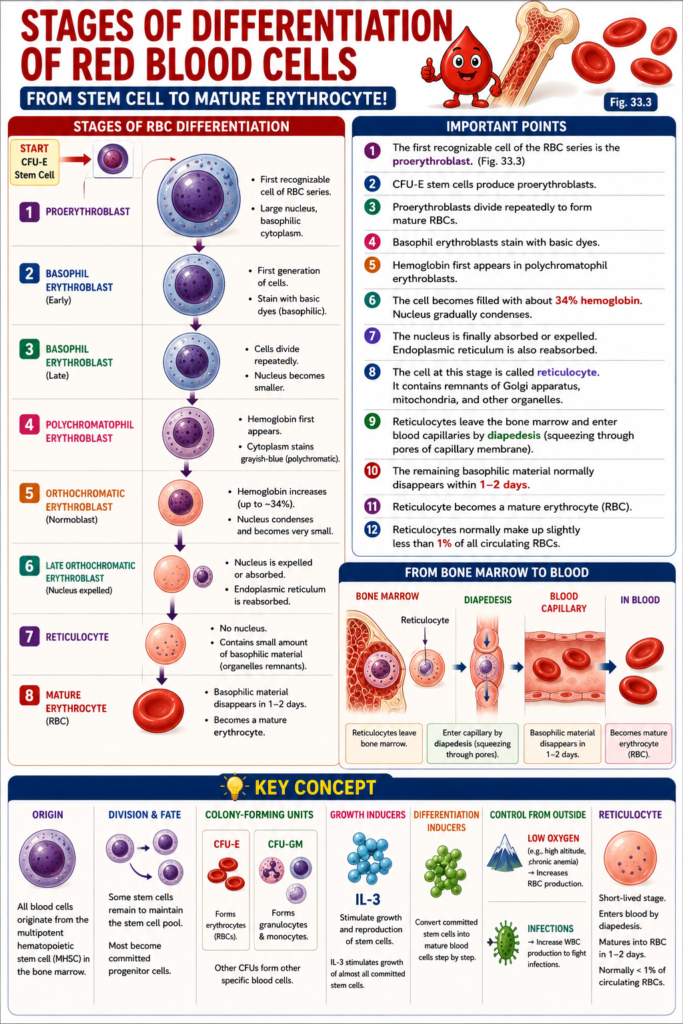
Stages of Differentiation of Red Blood Cells
- The first recognizable cell of the RBC series is the proerythroblast.
- (Fig. 33.3)
- When appropriately stimulated, large numbers of proerythroblasts are produced from CFU-E stem cells.
- After the proerythroblast is formed, it divides many times.
- These repeated divisions eventually produce many mature RBCs.
- The first generation of cells is called basophil erythroblasts.
- These cells are called basophil erythroblasts because they stain with basic dyes.
- Hemoglobin first appears in the polychromatophil erythroblasts.
- In the following generations, the cells become progressively filled with hemoglobin.
- The hemoglobin concentration increases to about 34%.
- The nucleus gradually condenses and becomes very small.
- The remaining nucleus is finally absorbed or expelled from the cell.
- At the same time, the endoplasmic reticulum is also reabsorbed.
- At this stage, the cell is called a reticulocyte.
- A reticulocyte still contains a small amount of basophilic material.
- This basophilic material consists of remnants of the Golgi apparatus, mitochondria, and a few other cytoplasmic organelles.
- During the reticulocyte stage, the cells leave the bone marrow and enter the blood capillaries.
- They enter the capillaries by diapedesis (squeezing through the pores of the capillary membrane).
- The remaining basophilic material normally disappears within 1–2 days.
- The reticulocyte then becomes a mature erythrocyte (RBC).
- Because the reticulocyte stage is short, reticulocytes normally make up slightly less than 1% of all circulating RBCs.
KEY CONCEPT
- The first identifiable RBC precursor is the proerythroblast.
- (Fig. 33.3)
- CFU-E stem cells produce proerythroblasts.
- Proerythroblasts divide repeatedly to form mature RBCs.
- Basophil erythroblasts stain with basic dyes.
- Hemoglobin first appears in polychromatophil erythroblasts.
- The cell becomes filled with about 34% hemoglobin.
- The nucleus and endoplasmic reticulum are removed during maturation.
- The reticulocyte contains remnants of cell organelles and enters the blood by diapedesis.
- Within 1–2 days, the reticulocyte becomes a mature erythrocyte.
- Reticulocytes normally account for slightly less than 1% of circulating RBCs.
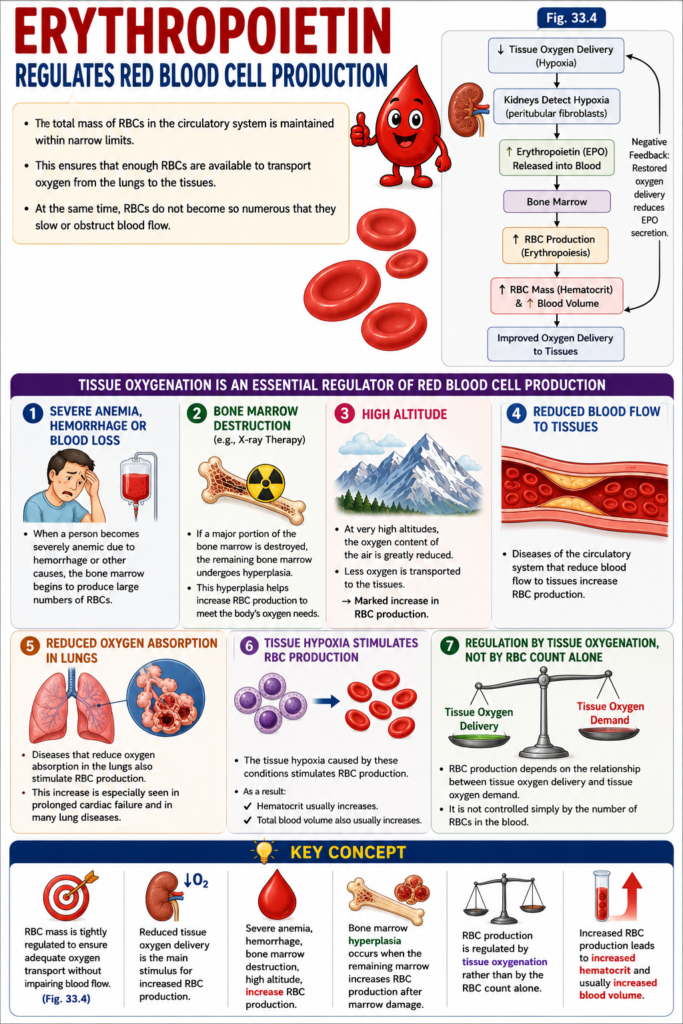
Erythropoietin Regulates Red Blood Cell Production
- The total mass of RBCs in the circulatory system is maintained within narrow limits.
- This ensures that enough RBCs are available to transport oxygen from the lungs to the tissues.
- At the same time, RBCs do not become so numerous that they slow or obstruct blood flow.
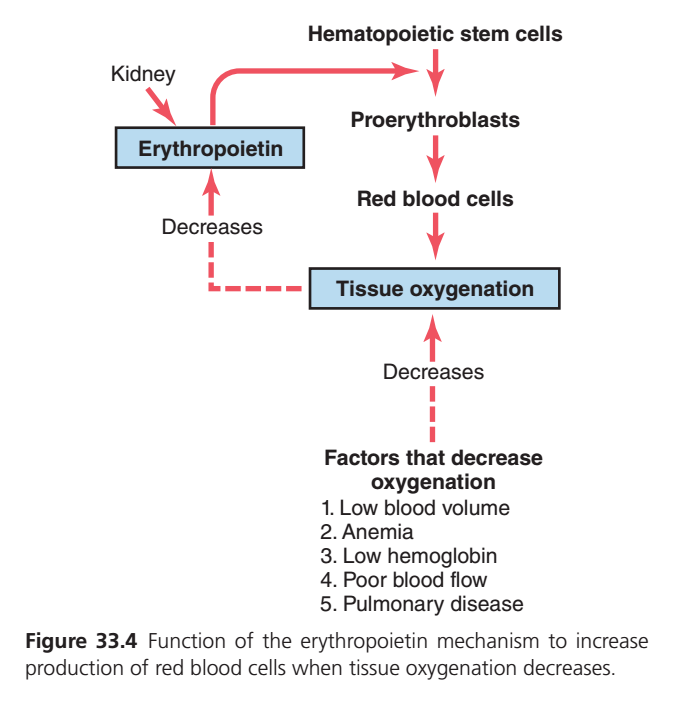
- The mechanism that controls RBC production is shown in (Fig. 33.4).
Tissue Oxygenation Is an Essential Regulator of Red Blood Cell Production
- Any condition that decreases the amount of oxygen delivered to the tissues usually increases RBC production.
- When a person becomes severely anemic due to hemorrhage or other causes, the bone marrow begins to produce large numbers of RBCs.
- If a major portion of the bone marrow is destroyed, especially by X-ray therapy, the remaining bone marrow undergoes hyperplasia.
- This hyperplasia helps increase RBC production to meet the body’s oxygen needs.
- At very high altitudes, the oxygen content of the air is greatly reduced.
- As a result, less oxygen is transported to the tissues.
- This causes a marked increase in RBC production.
- RBC production is controlled by the amount of oxygen delivered to the tissues, not simply by the number of RBCs in the blood.
- RBC production depends on the relationship between tissue oxygen delivery and tissue oxygen demand.
- Diseases of the circulatory system that reduce blood flow to tissues also increase RBC production.
- Diseases that reduce oxygen absorption in the lungs also stimulate RBC production.
- This increase is especially seen in prolonged cardiac failure.
- It is also common in many lung diseases.
- The tissue hypoxia caused by these conditions stimulates RBC production.
- As a result, hematocrit usually increases.
- Total blood volume also usually increases.
KEY CONCEPT
- RBC mass is tightly regulated to ensure adequate oxygen transport without impairing blood flow.
- (Fig. 33.4)
- Reduced tissue oxygen delivery is the main stimulus for increased RBC production.
- Severe anemia, hemorrhage, bone marrow destruction, high altitude, cardiac failure, and lung diseases all increase RBC production.
- Bone marrow hyperplasia occurs when the remaining marrow increases RBC production after marrow damage.
- RBC production is regulated by tissue oxygenation rather than by the RBC count alone.
- Increased RBC production leads to increased hematocrit and usually increased blood volume.
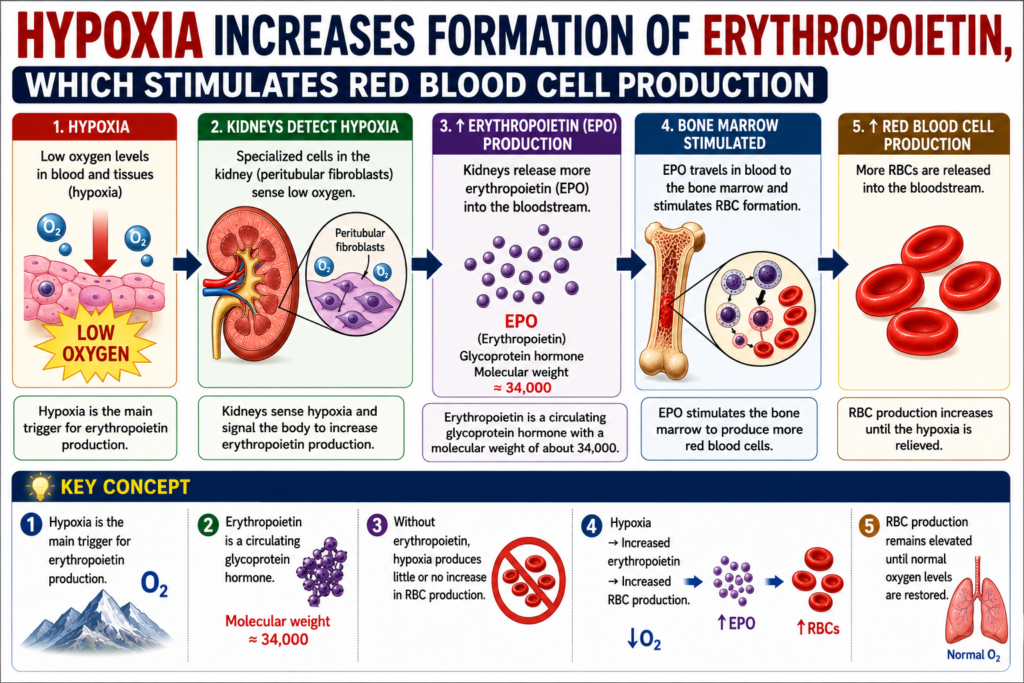
Hypoxia Increases Formation of Erythropoietin, Which Stimulates Red Blood Cell Production
- The main stimulus for increased RBC production during low oxygen (hypoxia) is the hormone erythropoietin.
- Erythropoietin is a circulating glycoprotein hormone.
- Its molecular weight is about 34,000.
- Without erythropoietin, hypoxia has little or no ability to stimulate RBC production.
- When the erythropoietin system is functioning normally, hypoxia causes a marked increase in erythropoietin production.
- The increased erythropoietin then stimulates the production of RBCs.
- RBC production continues to increase until the hypoxia is relieved.
KEY CONCEPT
- Hypoxia is the main trigger for erythropoietin production.
- Erythropoietin is a circulating glycoprotein hormone with a molecular weight of about 34,000.
- Without erythropoietin, hypoxia produces little or no increase in RBC production.
- Hypoxia → Increased erythropoietin → Increased RBC production.
- RBC production remains elevated until normal oxygen levels are restored.
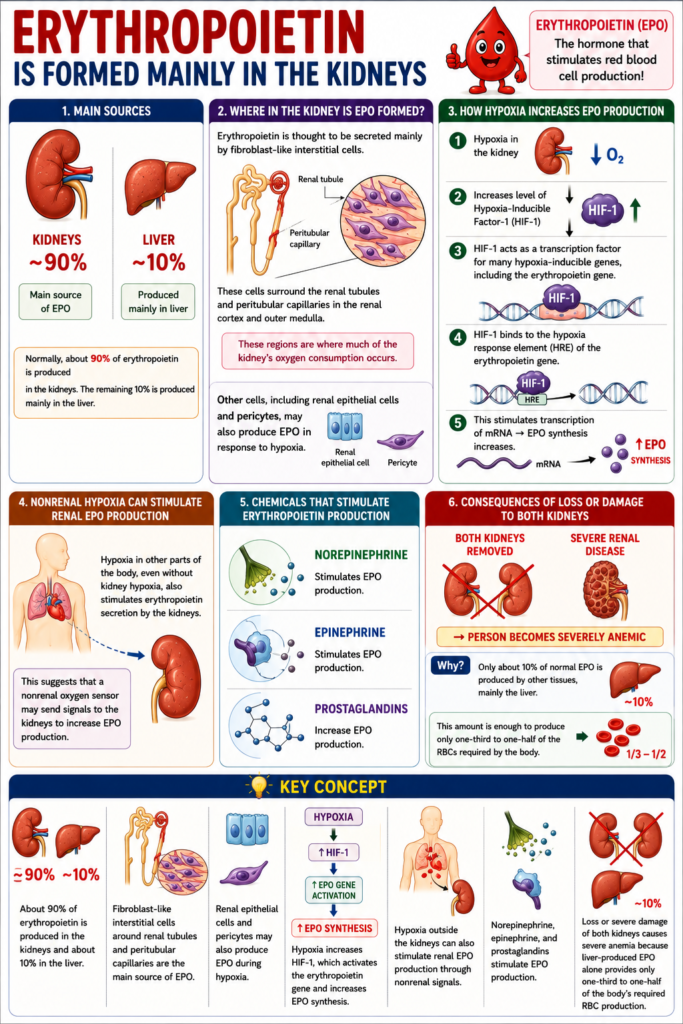
Erythropoietin Is Formed Mainly in the Kidneys
- Normally, about 90% of erythropoietin is produced in the kidneys.
- The remaining 10% is produced mainly in the liver.
- Erythropoietin is thought to be secreted mainly by fibroblast-like interstitial cells.
- These cells surround the renal tubules and peritubular capillaries in the renal cortex and outer medulla.
- These regions are where much of the kidney’s oxygen consumption occurs.
- Other cells, including renal epithelial cells and pericytes, may also produce erythropoietin in response to hypoxia.
- Hypoxia in the kidney increases the level of hypoxia-inducible factor-1 (HIF-1).
- HIF-1 acts as a transcription factor for many hypoxia-inducible genes, including the erythropoietin gene.
- HIF-1 binds to the hypoxia response element of the erythropoietin gene.
- This stimulates transcription of messenger RNA (mRNA).
- As a result, erythropoietin synthesis increases.
- Sometimes hypoxia in other parts of the body, even without kidney hypoxia, also stimulates erythropoietin secretion by the kidneys.
- This suggests that a nonrenal oxygen sensor may send signals to the kidneys to increase erythropoietin production.
- Norepinephrine stimulates erythropoietin production.
- Epinephrine also stimulates erythropoietin production.
- Several prostaglandins also increase erythropoietin production.
- If both kidneys are removed, the person becomes severely anemic.
- Severe renal disease that destroys the kidneys also causes marked anemia.
- This occurs because only about 10% of normal erythropoietin is produced by other tissues, mainly the liver.
- This amount is enough to produce only one-third to one-half of the RBCs required by the body.
KEY CONCEPT
- About 90% of erythropoietin is produced in the kidneys and about 10% in the liver.
- Fibroblast-like interstitial cells around the renal tubules and peritubular capillaries are the main source of erythropoietin.
- Renal epithelial cells and pericytes may also produce erythropoietin during hypoxia.
- Hypoxia increases HIF-1, which activates the erythropoietin gene and increases erythropoietin synthesis.
- Hypoxia outside the kidneys can also stimulate renal erythropoietin production through nonrenal signals.
- Norepinephrine, epinephrine, and prostaglandins stimulate erythropoietin production.
- Loss or severe damage of both kidneys causes severe anemia because liver-produced erythropoietin alone provides only one-third to one-half of the body’s required RBC production.
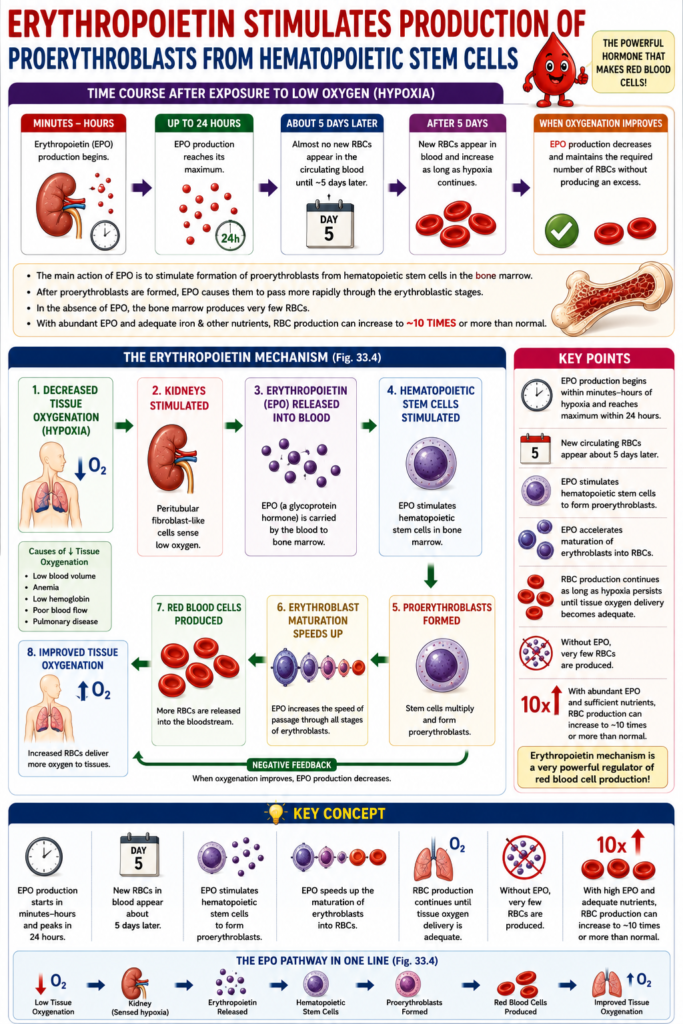
Erythropoietin Stimulates Production of Proerythroblasts From Hematopoietic Stem Cells
- When a person or animal is exposed to a low-oxygen environment, erythropoietin begins to be produced within minutes to hours.
- Erythropoietin production reaches its maximum level within 24 hours.
- Almost no new RBCs appear in the circulating blood until about 5 days later.
- This shows that the main action of erythropoietin is to stimulate the formation of proerythroblasts from hematopoietic stem cells in the bone marrow.
- After proerythroblasts are formed, erythropoietin causes them to pass more rapidly through the different erythroblastic stages.
- This further speeds up the production of new RBCs.
- Rapid RBC production continues as long as the person remains in a low-oxygen state.
- It also continues until enough RBCs have been produced to deliver adequate oxygen to the tissues despite the low oxygen level.
- At that time, erythropoietin production decreases.
- The reduced erythropoietin level maintains the required number of RBCs without producing an excess.
- In the absence of erythropoietin, the bone marrow produces very few RBCs.
- When large amounts of erythropoietin are produced, and sufficient iron and other required nutrients are available, RBC production can increase to about 10 times or more than normal.
- Therefore, the erythropoietin mechanism is a very powerful regulator of RBC production.
- (Fig. 33.4)
- The figure shows the erythropoietin mechanism that increases RBC production when tissue oxygenation decreases.
- Decreased tissue oxygenation stimulates the kidneys.
- The kidneys produce erythropoietin.
- Erythropoietin stimulates hematopoietic stem cells.
- Hematopoietic stem cells form proerythroblasts.
- Proerythroblasts develop into red blood cells.
- The increased RBCs improve tissue oxygenation.
- Factors that decrease tissue oxygenation include:
- Low blood volume
- Anemia
- Low hemoglobin
- Poor blood flow
- Pulmonary disease
KEY CONCEPT
- Erythropoietin production begins within minutes to hours of hypoxia and reaches its maximum within 24 hours.
- New circulating RBCs appear about 5 days later.
- Erythropoietin stimulates hematopoietic stem cells to form proerythroblasts.
- It also accelerates the maturation of erythroblasts into RBCs.
- RBC production continues until tissue oxygen delivery becomes adequate.
- Without erythropoietin, very few RBCs are produced.
- With abundant erythropoietin and adequate nutrients, RBC production can increase to about 10 times or more than normal.
- (Fig. 33.4)
- Low tissue oxygenation → Kidney → Erythropoietin → Hematopoietic stem cells → Proerythroblasts → Red blood cells → Improved tissue oxygenation.
Maturation of Red Blood Cells Requires Vitamin B12 (Cyanocobalamin) and Folic Acid
- Red blood cells (RBCs) are continuously replaced in the body.
- Therefore, the erythropoietic cells of the bone marrow grow and divide very rapidly.
- Because these cells grow so fast, their maturation and production depend greatly on good nutrition.
- Two vitamins are especially important for the final maturation of RBCs:
- Vitamin B12 (Cyanocobalamin)
- Folic acid
- Both vitamin B12 and folic acid are essential for DNA synthesis.
- Each vitamin helps in the formation of thymidine triphosphate.
- Thymidine triphosphate is one of the essential building blocks of DNA.
- If vitamin B12 or folic acid is lacking:
- Nuclear maturation fails.
- Cell division cannot occur normally.
- As a result, erythroblasts in the bone marrow do not multiply rapidly.
- Instead, they mainly produce larger-than-normal RBCs called macrocytes.
- Macrocytes have:
- A thin (flimsy) membrane.
- An irregular shape.
- A large size.
- An oval shape instead of the normal biconcave disc.
- After entering the circulating blood:
- These abnormal RBCs can carry oxygen normally.
- However, they are fragile.
- Their lifespan is only one-half to one-third of the normal RBC lifespan.
- Therefore, deficiency of vitamin B12 or folic acid causes failure of RBC maturation during erythropoiesis.
KEY CONCEPT
- Bone marrow RBC-producing cells require rapid DNA synthesis.
- Vitamin B12 and folic acid are essential for DNA formation.
- Deficiency of either vitamin causes defective nuclear maturation and cell division.
- Large abnormal RBCs (macrocytes) are produced.
- Macrocytes carry oxygen normally but are fragile and have a shortened lifespan.
- Vitamin B12 or folic acid deficiency leads to maturation failure during erythropoiesis.

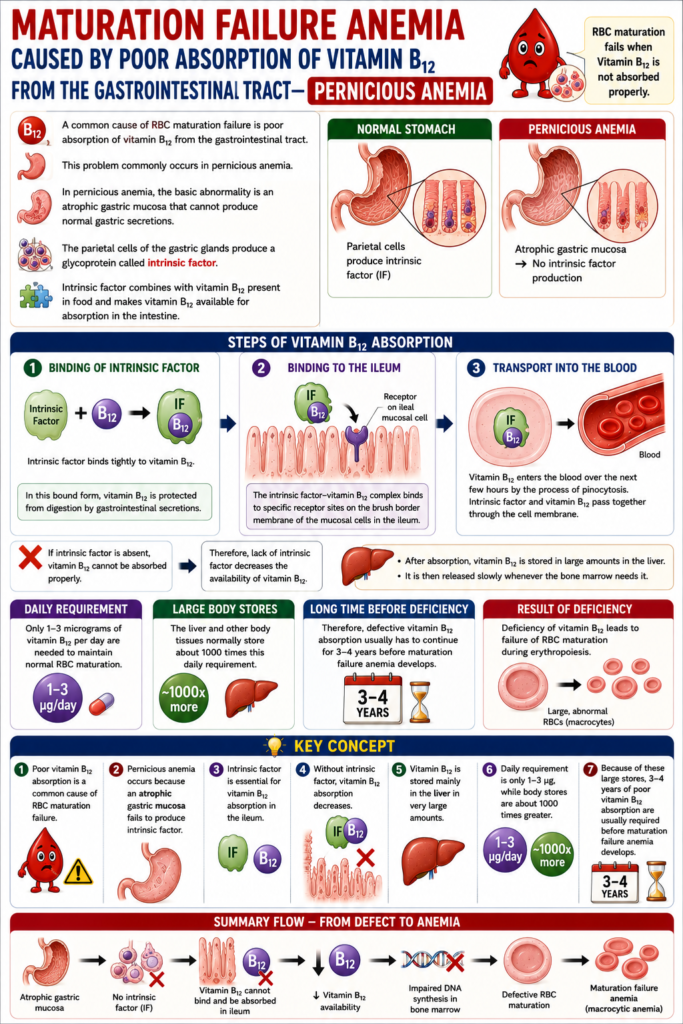
Maturation Failure Anemia Caused By Poor Absorption of Vitamin B12 From the Gastrointestinal Tract—Pernicious Anemia
- A common cause of RBC maturation failure is poor absorption of vitamin B12 from the gastrointestinal tract.
- This problem commonly occurs in pernicious anemia.
- In pernicious anemia, the basic abnormality is an atrophic gastric mucosa.
- The atrophic gastric mucosa cannot produce normal gastric secretions.
- The parietal cells of the gastric glands produce a glycoprotein called intrinsic factor.
- Intrinsic factor combines with vitamin B12 present in food.
- This combination makes vitamin B12 available for absorption in the intestine.
Steps of Vitamin B12 Absorption
1. Binding of Intrinsic Factor
- Intrinsic factor binds tightly to vitamin B12.
- In this bound form, vitamin B12 is protected from digestion by gastrointestinal secretions.
2. Binding to the Ileum
- The intrinsic factor–vitamin B12 complex binds to specific receptor sites.
- These receptor sites are present on the brush border membrane of the mucosal cells in the ileum.
3. Transport Into the Blood
- Vitamin B12 enters the blood over the next few hours.
- It is transported by the process of pinocytosis.
- Intrinsic factor and vitamin B12 pass together through the cell membrane.
- If intrinsic factor is absent, vitamin B12 cannot be absorbed properly.
- Therefore, lack of intrinsic factor decreases the availability of vitamin B12.
- After absorption, vitamin B12 is stored in large amounts in the liver.
- It is then released slowly whenever the bone marrow needs it.
- Only 1–3 micrograms of vitamin B12 per day are needed to maintain normal RBC maturation.
- The liver and other body tissues normally store about 1000 times this daily requirement.
- Therefore, defective vitamin B12 absorption usually has to continue for 3–4 years before maturation failure anemia develops.
KEY CONCEPT
- Poor vitamin B12 absorption is a common cause of RBC maturation failure.
- Pernicious anemia occurs because an atrophic gastric mucosa fails to produce intrinsic factor.
- Intrinsic factor is essential for vitamin B12 absorption in the ileum.
- Without intrinsic factor, vitamin B12 absorption decreases.
- Vitamin B12 is stored mainly in the liver in very large amounts.
- Daily requirement is only 1–3 micrograms, while body stores are about 1000 times greater.
- Because of these large stores, 3–4 years of poor vitamin B12 absorption are usually required before maturation failure anemia develops.
Maturation Failure Anemia Caused By Folic Acid (Pteroylglutamic Acid) Deficiency
- Folic acid (Pteroylglutamic acid) is normally found in:
- Green vegetables
- Some fruits
- Meats, especially liver
- Folic acid is easily destroyed during cooking.
- People with gastrointestinal absorption disorders may not absorb folic acid properly.
- One such disorder is sprue, a disease of the small intestine.
- Sprue causes chronic diarrhea.
- People with sprue often have serious difficulty absorbing:
- Folic acid
- Vitamin B12
- Therefore, in many cases of maturation failure anemia, the cause is poor intestinal absorption of both folic acid and vitamin B12.
KEY CONCEPT
- Folic acid is present in green vegetables, some fruits, and especially liver.
- Cooking can easily destroy folic acid.
- Gastrointestinal absorption disorders reduce folic acid absorption.
- Sprue is a small intestinal disease that causes chronic diarrhea and poor absorption of folic acid and vitamin B12.
- Deficiency of folic acid and vitamin B12 absorption is a common cause of maturation failure anemia.
