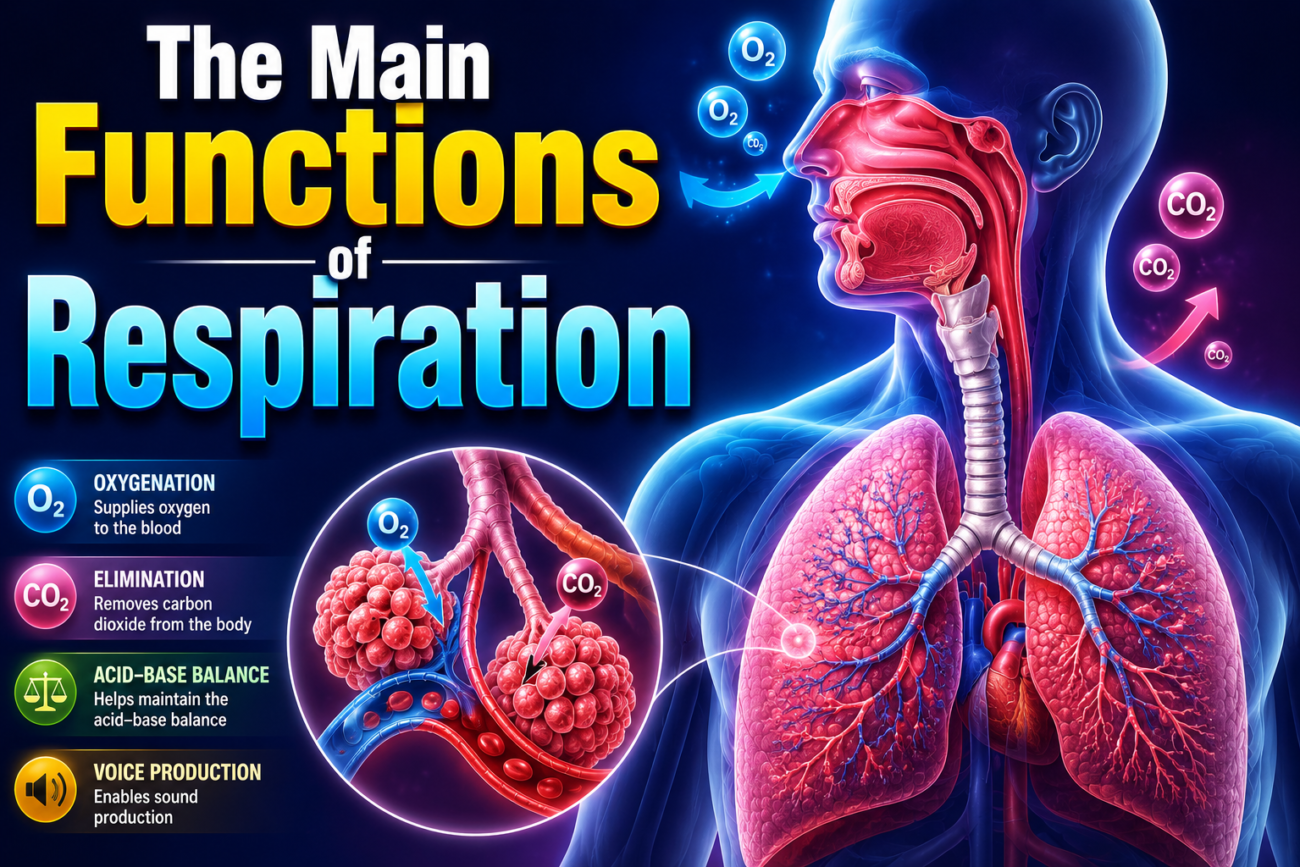
Main Functions of Respiration
- The main function of respiration is to provide oxygen (O₂) to the body’s tissues.
- Another main function is to remove carbon dioxide (CO₂) from the body.
Four Major Components of Respiration
1. Pulmonary Ventilation
- Pulmonary ventilation is the movement of air into and out of the lungs.
- It includes:
- Air entering from the atmosphere into the lung alveoli.
- Air leaving the lung alveoli back to the atmosphere.
2. Diffusion of Oxygen and Carbon Dioxide
- Oxygen (O₂) diffuses from the alveoli into the blood.
- Carbon dioxide (CO₂) diffuses from the blood into the alveoli.
3. Transport of Oxygen and Carbon Dioxide
- The blood and body fluids transport:
- Oxygen (O₂) from the lungs to the body’s tissue cells.
- Carbon dioxide (CO₂) from the tissue cells back to the lungs.
4. Regulation of Ventilation and Respiration
- The body regulates pulmonary ventilation.
- The body also regulates other aspects of respiration.
Chapter Coverage
- This chapter discusses pulmonary ventilation.
- The next five chapters explain:
- Other respiratory functions.
- The physiology of special respiratory abnormalities.
Key Concept
Respiration supplies O₂ to tissues, removes CO₂, and consists of four major components: pulmonary ventilation, gas diffusion, gas transport, and regulation of ventilation.
MECHANICS OF PULMONARY VENTILATION
Figure Mentioned: Fig. 38.1 – Shows the two methods of lung expansion and contraction and the mechanism of external and internal intercostal muscles during inspiration and expiration.
Muscles That Cause Lung Expansion and Contraction
- The lungs expand and contract in two ways:
- By downward or upward movement of the diaphragm, which lengthens or shortens the chest cavity.
- By elevation or depression of the ribs, which increases or decreases the anteroposterior (AP) diameter of the chest cavity.
- Fig. 38.1 shows these two methods.
Diaphragm During Quiet Breathing
- Normal quiet breathing is accomplished mainly by the diaphragm.
- During inspiration, the diaphragm contracts.
- The contracting diaphragm pulls the lower surfaces of the lungs downward.
- During expiration, the diaphragm relaxes.
- The elastic recoil of the lungs, chest wall, and abdominal structures compresses the lungs.
- Air is expelled from the lungs.
Diaphragm During Heavy Breathing
- During heavy breathing, elastic recoil alone is not enough for rapid expiration.
- Extra force is produced mainly by contraction of the abdominal muscles.
- The abdominal muscles push the abdominal contents upward against the bottom of the diaphragm.
- This compresses the lungs and helps force air out.
Rib Cage Expansion
- The second method of lung expansion is by raising the rib cage.
- In the normal resting position, the ribs slope downward.
- This allows the sternum to fall backward toward the vertebral column.
- When the rib cage is elevated:
- The ribs project almost directly forward.
- The sternum moves forward, away from the spine.
- This increases the anteroposterior (AP) diameter of the chest.
- During maximum inspiration, the AP diameter is about 20% greater than during expiration.
- Therefore:
- Muscles that elevate the chest cage are muscles of inspiration.
- Muscles that depress the chest cage are muscles of expiration.
Muscles of Inspiration
- The external intercostal muscles are the most important muscles that raise the rib cage.
- Other muscles that assist are:
- Sternocleidomastoid muscles – lift the sternum upward.
- Anterior serrati – lift many ribs.
- Scaleni – lift the first two ribs.
Muscles of Expiration
- The main muscles that pull the rib cage downward are:
- Abdominal recti
- Internal intercostal muscles
- The abdominal recti:
- Pull the lower ribs downward.
- Compress the abdominal contents upward against the diaphragm.
Mechanism of External and Internal Intercostal Muscles
- Fig. 38.1 also shows how the external and internal intercostal muscles produce inspiration and expiration.
- During expiration, the ribs are angled downward.
- The external intercostal muscles run forward and downward.
- When they contract:
- They pull the upper ribs forward relative to the lower ribs.
- This creates leverage that raises the ribs upward.
- Inspiration occurs.
- The internal intercostal muscles run in the opposite direction.
- They create opposite leverage.
- Therefore, they pull the ribs downward and function as muscles of expiration.
Key Concept
- The lungs expand by diaphragm contraction and rib cage elevation. Quiet breathing mainly depends on the diaphragm, heavy breathing recruits abdominal muscles, external intercostals produce inspiration, and internal intercostals together with abdominal muscles produce expiration.
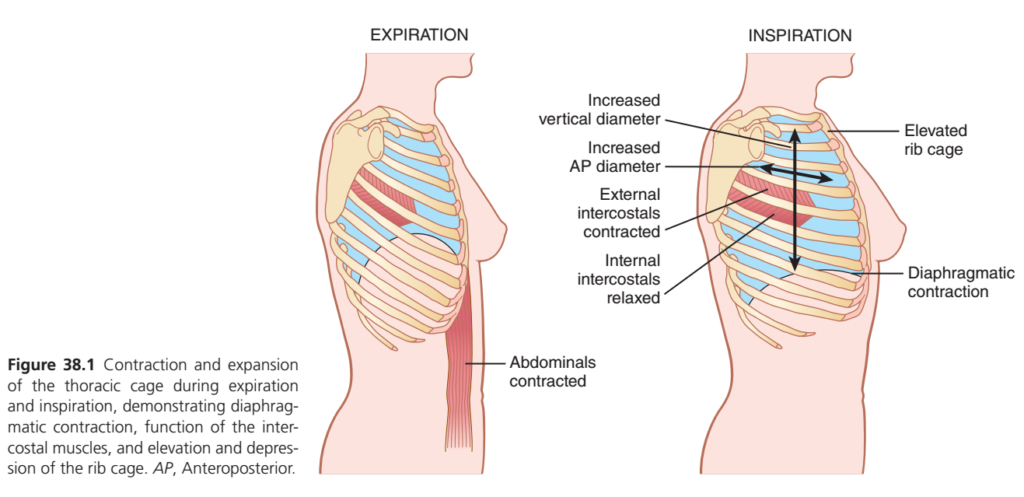
Figure 38.1: Mechanics of Breathing (Guyton)
🎯 One Golden Rule to Remember
Air always moves from HIGH pressure → LOW pressure.
- To breathe IN (Inspiration): Chest must become bigger → Lung pressure becomes lower → Air enters.
- To breathe OUT (Expiration): Chest becomes smaller → Lung pressure becomes higher → Air leaves.
🌬️ INSPIRATION (Breathing In)
Think of inflating a balloon 🎈
To inflate a balloon, you increase its space.
Exactly the same happens in the chest.
Step 1: Diaphragm contracts
- The diaphragm is dome-shaped at rest.
- When it contracts, it moves downward (flattens).
👉 This increases the vertical (up-down) diameter of the chest.
Image label
- Diaphragmatic contraction
- Increased vertical diameter
Step 2: External intercostal muscles contract
These muscles are located between the ribs.
When they contract,
➡️ They lift the ribs upward and outward.
This causes:
- Rib cage elevates
- Chest expands sideways
- Front-to-back diameter increases
This is called the:
↑ Anteroposterior (AP) diameter
AP Diameter = Distance from chest front → chest back
Step 3: Internal intercostal muscles relax
Since inspiration needs expansion,
the muscles that pull ribs downward are relaxed.
Image label
✔ Internal intercostals relaxed
Final Result of Inspiration
✅ Diaphragm moves down
✅ Ribs move up
✅ Chest cavity becomes larger
✅ Lung volume increases
✅ Lung pressure decreases
✅ Air enters lungs
Easy Memory
INSPIRATION = EVERYTHING GOES UP OR DOWN TO MAKE SPACE
- Diaphragm ↓
- Ribs ↑
- Chest ↑
- Lung volume ↑
- Air comes IN
🌬️ EXPIRATION (Breathing Out)
Think of deflating a balloon.
To let air out,
you simply reduce its size.
Step 1: Diaphragm relaxes
It moves back upward into its dome shape.
Chest becomes shorter.
Step 2: Rib cage falls
External intercostals relax.
The ribs move downward.
Chest becomes narrower.
Step 3: Abdominal muscles contract (especially during forceful expiration)
The image shows:
Abdominals contracted
These muscles:
- Push abdominal organs upward.
- Push the diaphragm upward.
- Force more air out.
This happens during:
- Coughing
- Sneezing
- Running
- Heavy exercise
Final Result of Expiration
✅ Chest cavity becomes smaller
✅ Lung volume decreases
✅ Lung pressure increases
✅ Air is pushed out
Easy Memory
EXPIRATION = EVERYTHING RETURNS TO REST
- Diaphragm ↑
- Ribs ↓
- Chest ↓
- Lung volume ↓
- Air goes OUT
📚 Understanding Every Label in the Figure
| Figure Label | Meaning in Simple Words |
|---|---|
| Diaphragmatic contraction | Diaphragm moves downward, making more room for lungs. |
| Elevated rib cage | Ribs move upward and outward. |
| External intercostals contracted | Muscles between ribs lift the ribs. |
| Internal intercostals relaxed | Downward-pulling muscles are inactive during inspiration. |
| Increased vertical diameter | Chest becomes taller because the diaphragm moves down. |
| Increased AP diameter | Chest becomes wider from front to back due to rib elevation. |
| Abdominals contracted | Help force air out during active/forced expiration. |
🧠 Why Two Different Diameters Increase?
① Vertical Diameter ↑
Caused by:
➡️ Diaphragm moving downward.
Think of stretching a room from floor to ceiling.
② AP Diameter ↑
Caused by:
➡️ Ribs moving upward and outward.
Think of opening a bucket handle upward—the sides move outward, increasing the front-to-back space.
🎯 Complete Sequence (Flow Chart)
Inspiration
Diaphragm contracts
↓
Moves downward
↓
External intercostals contract
↓
Ribs elevate
↓
Chest cavity expands
↓
Lung volume increases
↓
Lung pressure decreases
↓
Air enters lungsExpiration
Diaphragm relaxes
↓
Moves upward
↓
Ribs fall downward
↓
Chest cavity becomes smaller
↓
Lung volume decreases
↓
Lung pressure increases
↓
Air leaves lungs⭐ MBBS Exam High-Yield Points
- Main muscle of inspiration: ✅ Diaphragm
- Muscles assisting inspiration: ✅ External intercostals
- Muscles active in forced expiration: ✅ Abdominal muscles + Internal intercostals
- Normal quiet expiration: Mostly passive due to elastic recoil of the lungs.
- Inspiration increases:
- Vertical diameter
- Anteroposterior (AP) diameter
- Thoracic volume
- Expiration decreases:
- Thoracic volume
- Lung volume
- Air is expelled
🧠 One-Line Memory Trick
“IN = Diaphragm DOWN + Ribs UP = Chest BIGGER = Air IN.”
“OUT = Diaphragm UP + Ribs DOWN = Chest SMALLER = Air OUT.”
PRESSURES THAT CAUSE MOVEMENT OF AIR IN AND OUT OF THE LUNGS
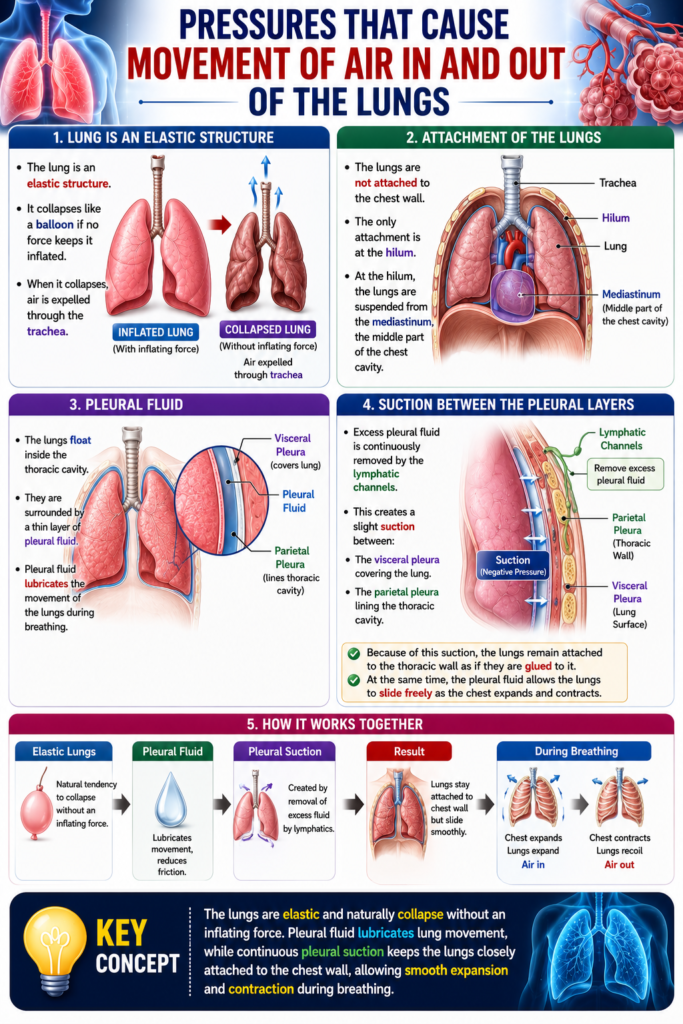
Lung is an Elastic Structure
- The lung is an elastic structure.
- It collapses like a balloon if no force keeps it inflated.
- When it collapses, air is expelled through the trachea.
Attachment of the Lungs
- The lungs are not attached to the chest wall.
- The only attachment is at the hilum.
- At the hilum, the lungs are suspended from the mediastinum, the middle part of the chest cavity.
Pleural Fluid
- The lungs float inside the thoracic cavity.
- They are surrounded by a thin layer of pleural fluid.
- Pleural fluid lubricates the movement of the lungs during breathing.
Suction Between the Pleural Layers
- Excess pleural fluid is continuously removed by the lymphatic channels.
- This creates a slight suction between:
- The visceral pleura covering the lung.
- The parietal pleura lining the thoracic cavity.
- Because of this suction, the lungs remain attached to the thoracic wall as if they are glued to it.
- At the same time, the pleural fluid allows the lungs to slide freely as the chest expands and contracts.
Key Concept
The lungs are elastic and naturally collapse without an inflating force. Pleural fluid lubricates lung movement, while continuous pleural suction keeps the lungs closely attached to the chest wall, allowing smooth expansion and contraction during breathing.mple rule explains almost the entire mechanism shown in Guyton Figure 38.1.
Pleural Pressure and Its Changes During Respiration
Figure Mentioned: Fig. 38.2 – Shows the relationship between pleural pressure and lung volume during inspiration and expiration.
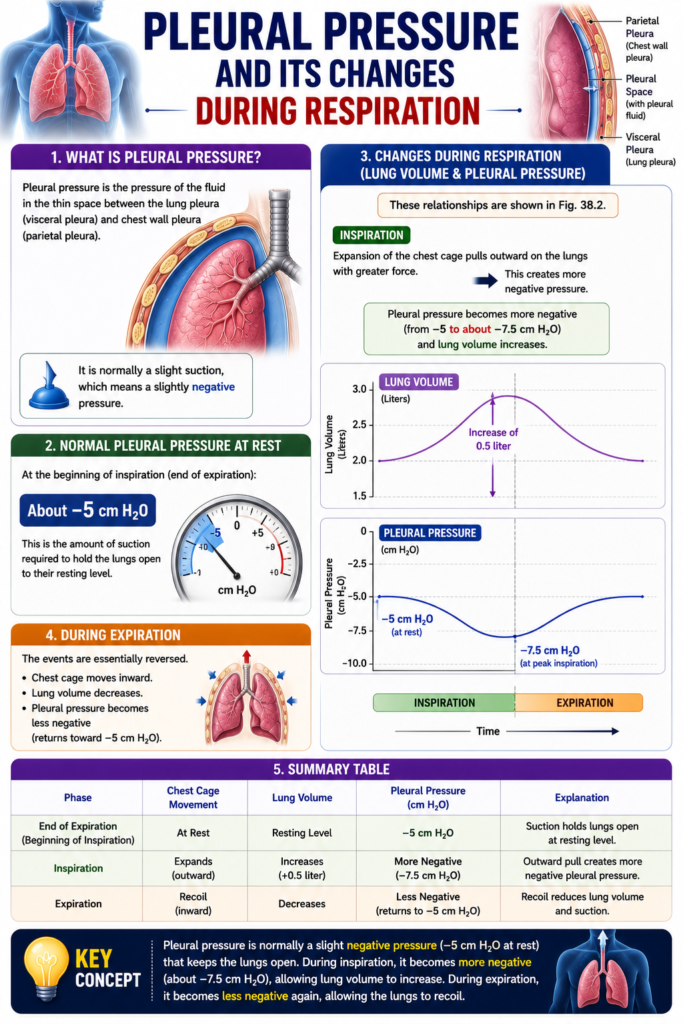
Pleural Pressure
- Pleural pressure is the pressure of the fluid in the thin space between:
- The lung (visceral) pleura
- The chest wall (parietal) pleura
- Pleural pressure is normally a slight suction.
- This means it is a slightly negative pressure.
Pleural Pressure at the Beginning of Inspiration
- At the beginning of inspiration, normal pleural pressure is about −5 cm H₂O.
- This negative pressure provides enough suction to keep the lungs open at their resting level.
Pleural Pressure During Inspiration
- During normal inspiration, the chest cage expands.
- Expansion of the chest cage pulls the lungs outward with greater force.
- As a result, pleural pressure becomes more negative.
- The average pleural pressure decreases to about −7.5 cm H₂O.
Relationship Between Pleural Pressure and Lung Volume
- Fig. 38.2 demonstrates this relationship.
- During inspiration:
- Pleural pressure changes from −5 cm H₂O to −7.5 cm H₂O.
- Lung volume increases by about 0.5 liter.
- During expiration:
- These changes occur in the opposite direction.
- Pleural pressure becomes less negative.
- Lung volume decreases.
Key Concept
- Pleural pressure is normally negative. It changes from about −5 cm H₂O to −7.5 cm H₂O during inspiration, creating greater suction that expands the lungs by about 0.5 liter. During expiration, these changes reverse.
Pleural Pressure and Its Changes During Respiration
Figure Mentioned: Fig. 38.2 – Shows the relationship between pleural pressure and lung volume during inspiration and expiration.
Pleural Pressure
- Pleural pressure is the pressure of the fluid in the thin space between:
- The lung (visceral) pleura
- The chest wall (parietal) pleura
- Pleural pressure is normally a slight suction.
- This means it is a slightly negative pressure.
Pleural Pressure at the Beginning of Inspiration
- At the beginning of inspiration, normal pleural pressure is about −5 cm H₂O.
- This negative pressure provides enough suction to keep the lungs open at their resting level.
Pleural Pressure During Inspiration
- During normal inspiration, the chest cage expands.
- Expansion of the chest cage pulls the lungs outward with greater force.
- As a result, pleural pressure becomes more negative.
- The average pleural pressure decreases to about −7.5 cm H₂O.
Relationship Between Pleural Pressure and Lung Volume
- Fig. 38.2 demonstrates this relationship.
- During inspiration:
- Pleural pressure changes from −5 cm H₂O to −7.5 cm H₂O.
- Lung volume increases by about 0.5 liter.
- During expiration:
- These changes occur in the opposite direction.
- Pleural pressure becomes less negative.
- Lung volume decreases.
Key Concept
- Pleural pressure is normally negative. It changes from about −5 cm H₂O to −7.5 cm H₂O during inspiration, creating greater suction that expands the lungs by about 0.5 liter. During expiration, these changes reverse.
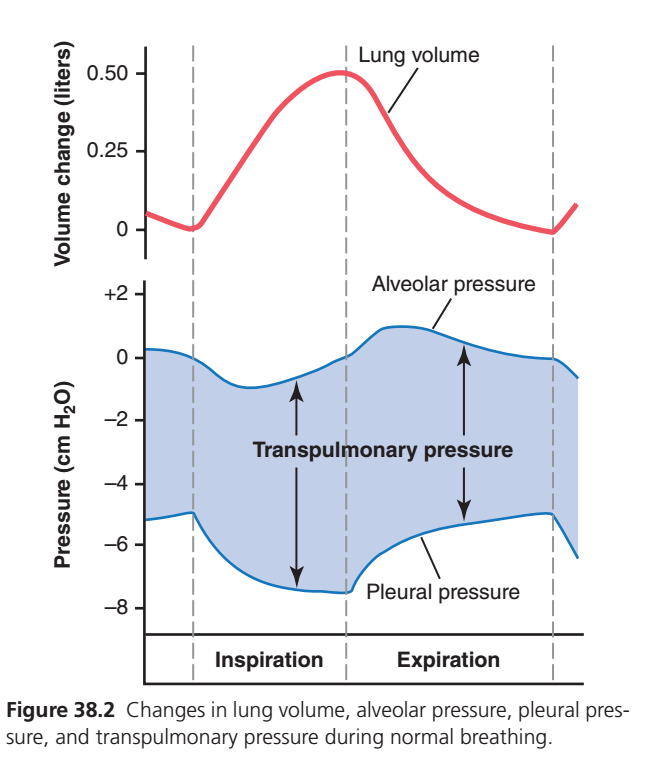
This is one of the most important graphs in Guyton Physiology because it explains how normal breathing occurs by showing the relationship between:
- Lung Volume (Red line)
- Alveolar Pressure (Upper Blue line)
- Pleural Pressure (Lower Blue line)
- Transpulmonary Pressure (Shaded Area)
First Understand the Big Picture
Think of the lungs as a balloon inside a sealed box.
- Balloon = Lung
- Box = Chest cavity
- Space between them = Pleural cavity
During breathing:
- Chest expands → pleural pressure becomes more negative → lungs expand.
- Lungs expand → alveolar pressure falls → air enters.
- Chest relaxes → lungs recoil → alveolar pressure rises → air leaves.
The graph shows this entire sequence.PART 1: Red Line (Lung Volume)
Top Graph
Question: What is changing?
👉 Amount of air inside the lungs.
![Concept]
More Air
▲
0.5L ───────── Peak Inspiration
/\
/ \
/ \
___/ \_________
Start EndA. Beginning
Lung volume is at its resting level.
No air is moving.
B. Inspiration
Red line rises.
Why?
Because air is entering the lungs.
The lungs gain about
500 mL (0.5 L)
This is the Tidal Volume.
Think:
Air In
↓↓↓↓↓
Lungs inflate
Volume ↑C. End of Inspiration
The red line reaches its highest point.
Lung volume is maximum.
No air is moving now because inspiration has just finished.
D. Expiration
Red line falls.
Why?
Air is leaving.
Lungs become smaller.
Air Out
↑↑↑↑↑
Volume ↓E. End of Expiration
Volume returns to normal resting level.
PART 2: Upper Blue Line (Alveolar Pressure)
This is the pressure inside the alveoli.
This pressure decides whether air moves in or out.
Rule to Remember
If Alveolar Pressure is Negative
Air enters.
If Alveolar Pressure is Positive
Air leaves.Beginning of Inspiration
Pressure = 0 cm H₂O
Why?
No pressure difference.
No airflow.
During Inspiration
Blue line falls to
−1 cm H₂O
Why?
Lungs expand.
Alveoli become larger.
Pressure inside drops.
Exactly like pulling a syringe.
Bigger Space
↓
Pressure Falls
↓
Air Rushes InThis small negative pressure is enough to pull about 500 mL of air into the lungs.
End of Inspiration
Pressure returns to
0 cm H₂O
Why?
The lungs are full.
Air has stopped moving.
During Expiration
Now lungs recoil.
They squeeze the air.
Pressure becomes
+1 cm H₂O
Positive pressure pushes air outside.
Smaller Lung
↓
Pressure Increases
↓
Air Moves OutEnd of Expiration
Pressure returns again to
0 cm H₂O
No airflow.
PART 3: Lower Blue Line (Pleural Pressure)
This is the pressure inside the pleural cavity, not inside the lung.
It is always negative during normal breathing.
Why?
Because the lungs naturally want to collapse inward, while the chest wall wants to spring outward. These opposite forces create a slight suction in the pleural space.
Beginning
Pleural pressure is about
−5 cm H₂O
This negative pressure keeps the lungs expanded.
Imagine:
Chest Wall ←
Pleural Space
→ Lung
Result:
Negative PressureDuring Inspiration
Chest expands.
Pleural cavity becomes larger.
Pressure becomes even more negative.
Approximately
−7.5 cm H₂O
Why?
Expansion increases the “suction” around the lungs, pulling them outward.
Think:
Chest Expands
↓
More Suction
↓
Pleural Pressure More NegativeDuring Expiration
Chest relaxes.
Pleural pressure becomes less negative.
Returns toward
−5 cm H₂O.
The suction decreases as the lungs recoil.
PART 4: Shaded Area (Transpulmonary Pressure)
This is the MOST IMPORTANT CONCEPT.
The shaded area represents the difference between alveolar pressure and pleural pressure.
Formula
Transpulmonary Pressure = Alveolar Pressure − Pleural Pressure
Example at rest:
Alveolar Pressure = 0
Pleural Pressure = -5
Transpulmonary Pressure
= 0 - (-5)
= +5 cm H₂OWhat Does Transpulmonary Pressure Do?
It is the distending pressure that keeps the lungs open.
It is the pressure trying to expand the lungs against their natural tendency to collapse.
More transpulmonary pressure = lungs expand more.
Less transpulmonary pressure = lungs expand less.
During Inspiration
Example:
Alveolar Pressure = -1
Pleural Pressure = -7.5
Difference
= (-1) - (-7.5)
= +6.5 cm H₂ONotice the difference becomes larger.
The shaded area widens.
This larger transpulmonary pressure stretches the lungs, increasing lung volume.
During Expiration
Pleural pressure becomes less negative.
The pressure difference decreases.
The shaded area narrows.
Less distending pressure allows the lungs to recoil, and air flows out.
Understanding All Four Together
| Phase | Lung Volume (Red) | Alveolar Pressure | Pleural Pressure | Transpulmonary Pressure |
|---|---|---|---|---|
| Start of inspiration | Normal | 0 | −5 | +5 |
| Inspiration | ↑ Increases | Slightly negative (≈−1) | More negative (≈−7.5) | ↑ Increases |
| End inspiration | Maximum | 0 | Most negative | Maximum |
| Expiration | ↓ Decreases | Slightly positive (≈+1) | Less negative | ↓ Decreases |
| End expiration | Normal | 0 | −5 | +5 |
One Complete Breathing Cycle (Story)
① Rest
- Lung volume is normal.
- Alveolar pressure = 0.
- Pleural pressure = −5 cm H₂O.
- Transpulmonary pressure keeps the lungs open.
⬇️
② Chest muscles contract
- Thoracic cavity expands.
- Pleural pressure becomes more negative.
- Transpulmonary pressure increases.
⬇️
③ Lungs expand
- Alveolar pressure falls to about −1 cm H₂O.
- Air flows into the lungs.
- Lung volume increases by about 500 mL.
⬇️
④ End inspiration
- Lung volume is maximum.
- Alveolar pressure returns to 0.
- Airflow stops.
⬇️
⑤ Chest muscles relax
- Lungs recoil because of their elastic tissue.
- Alveolar pressure rises to about +1 cm H₂O.
- Air is pushed out.
⬇️
⑥ End expiration
- Lung volume returns to resting level.
- Alveolar pressure returns to 0.
- Pleural pressure returns to about −5 cm H₂O.
- The cycle repeats.
High-Yield MBBS Viva Points
- Red line: Lung volume increases during inspiration and decreases during expiration.
- Upper blue line: Alveolar pressure becomes slightly negative (≈−1 cm H₂O) during inspiration to draw air in and slightly positive (≈+1 cm H₂O) during expiration to expel air.
- Lower blue line: Pleural pressure is always negative in normal breathing, becoming more negative during inspiration and less negative during expiration.
- Shaded area: Represents transpulmonary pressure (Alveolar Pressure − Pleural Pressure), the pressure that keeps the lungs expanded. It increases during inspiration (greater lung expansion) and decreases during expiration (elastic recoil).
Alveolar Pressure—Air Pressure Inside the Lung Alveoli
Figure Mentioned: Fig. 38.2 – Shows the changes in alveolar pressure, pleural pressure, and transpulmonary pressure during respiration.
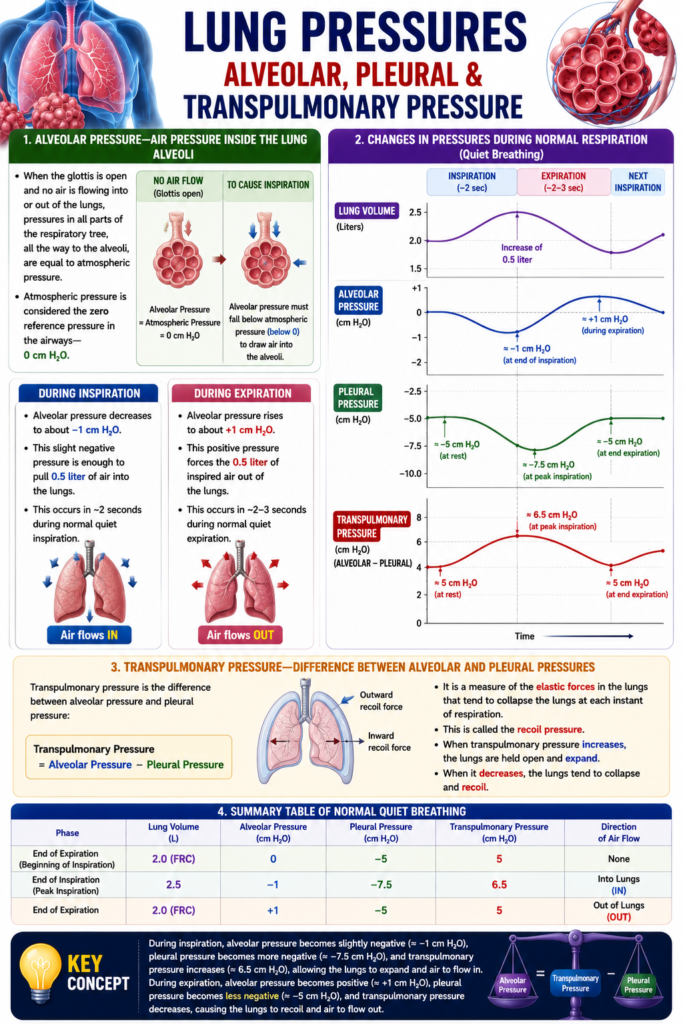
Alveolar Pressure
- Alveolar pressure is the air pressure inside the lung alveoli.
- When the glottis is open and no air is moving:
- The pressure throughout the respiratory tree, including the alveoli, is equal to atmospheric pressure.
- Atmospheric pressure is taken as the reference pressure.
- Therefore, alveolar pressure is 0 cm H₂O at rest.
Alveolar Pressure During Inspiration
- For air to enter the lungs, alveolar pressure must become slightly lower than atmospheric pressure.
- During normal inspiration, alveolar pressure falls to about −1 cm H₂O.
- This small negative pressure pulls about 0.5 liter of air into the lungs.
- Normal quiet inspiration takes about 2 seconds.
Alveolar Pressure During Expiration
- During expiration, alveolar pressure rises to about +1 cm H₂O.
- This positive pressure pushes 0.5 liter of inspired air out of the lungs.
- Normal expiration takes about 2–3 seconds.
Transpulmonary Pressure
- Transpulmonary pressure is the difference between:
- Alveolar pressure
- Pleural pressure
- Fig. 38.2 shows this relationship.
Function of Transpulmonary Pressure
- Transpulmonary pressure measures the elastic forces in the lungs.
- These elastic forces continuously tend to collapse the lungs.
- This collapsing force is called the recoil pressure.
Key Concept
- At rest, alveolar pressure is 0 cm H₂O. During inspiration it falls to −1 cm H₂O to draw 0.5 L of air into the lungs, and during expiration it rises to +1 cm H₂O to expel air. Transpulmonary pressure (alveolar pressure − pleural pressure) represents the lung’s elastic recoil pressure.
Transpulmonary Pressure—Difference Between Alveolar and Pleural Pressures
Figure Mentioned: Fig. 38.2 – Shows the relationship between alveolar pressure, pleural pressure, and transpulmonary pressure.
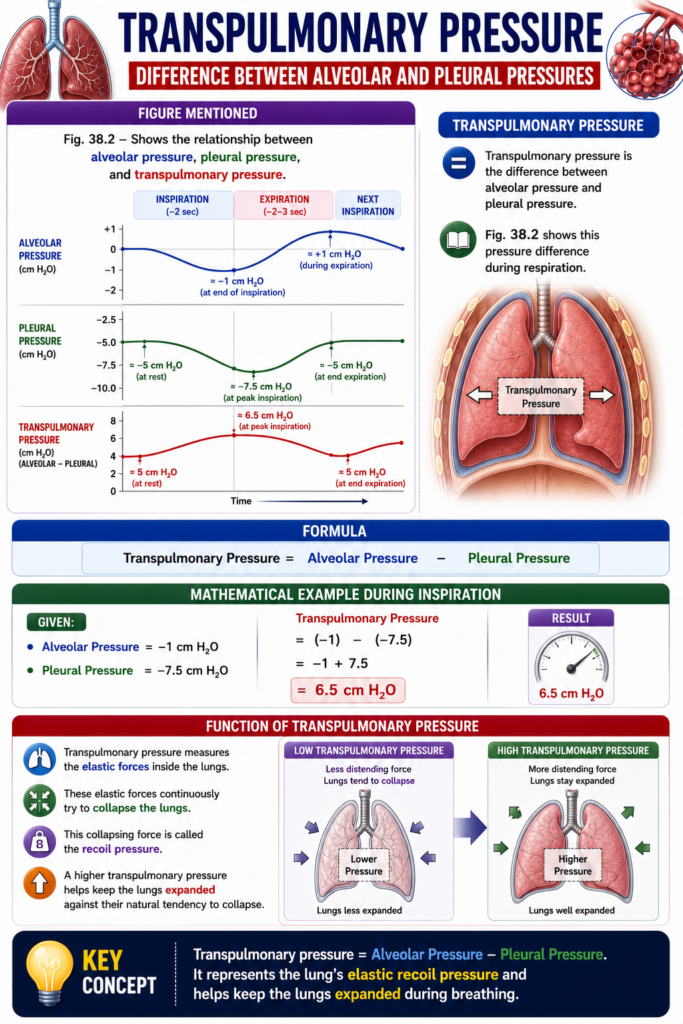
Transpulmonary Pressure
- Transpulmonary pressure is the difference between alveolar pressure and pleural pressure.
- Fig. 38.2 shows this pressure difference during respiration.
Formula
Transpulmonary Pressure=Alveolar Pressure−Pleural Pressure
Mathematical Example During Inspiration
Given:
- Alveolar Pressure = −1 cm H₂O
- Pleural Pressure = −7.5 cm H₂O
Transpulmonary Pressure=(−1)−(−7.5) =−1+7.5 =6.5 cm H2O
Function of Transpulmonary Pressure
- Transpulmonary pressure measures the elastic forces inside the lungs.
- These elastic forces continuously try to collapse the lungs.
- This collapsing force is called the recoil pressure.
- A higher transpulmonary pressure helps keep the lungs expanded against their natural tendency to collapse.
Key Concept
- Transpulmonary pressure = Alveolar Pressure − Pleural Pressure. It represents the lung’s elastic recoil pressure and helps keep the lungs expanded during breathing.
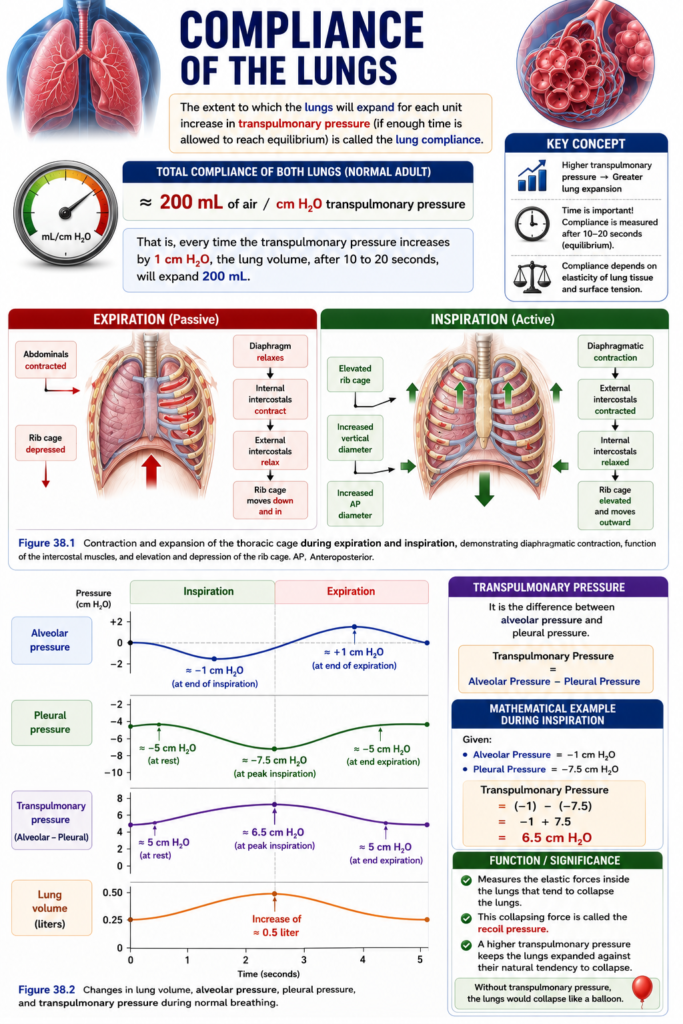
Compliance of the Lungs
Figure Mentioned:
- Fig. 38.1 – Contraction and expansion of the thoracic cage during inspiration and expiration.
- Fig. 38.2 – Changes in lung volume, alveolar pressure, pleural pressure, and transpulmonary pressure during normal breathing.
Compliance of the Lungs
- Lung compliance is the ability of the lungs to expand.
- It is measured by how much the lungs expand for each 1 cm H₂O increase in transpulmonary pressure.
- The lungs must be given enough time to reach equilibrium before measuring compliance.
Normal Lung Compliance
- The combined compliance of both lungs in a normal adult is about:
200 mL/cm H2O
- This means:
- If transpulmonary pressure increases by 1 cm H₂O,
- The lung volume increases by about 200 mL.
Time Required
- This lung expansion occurs after about 10–20 seconds, allowing the lungs to reach equilibrium.
Compliance Formula
Compliance=ΔTranspulmonary PressureΔLung Volume
Mathematical Calculation
Given:
- Compliance = 200 mL/cm H₂O
- Increase in transpulmonary pressure = 1 cm H₂O
Compliance=ΔPΔV
Substitute the values:200=1ΔV
Multiply both sides by 1:ΔV=200 mL
Answer:
A 1 cm H₂O increase in transpulmonary pressure causes the lungs to expand by 200 mL.
Another Example
If transpulmonary pressure increases by 3 cm H₂O:ΔV=200×3 ΔV=600 mL
Answer:
A 3 cm H₂O increase in transpulmonary pressure expands the lungs by 600 mL.
Key Concept
- Lung compliance = Change in Lung Volume ÷ Change in Transpulmonary Pressure. Normal lung compliance is about 200 mL/cm H₂O, meaning every 1 cm H₂O increase in transpulmonary pressure expands both lungs by approximately 200 mL after 10–20 seconds.
Compliance Diagram of the Lungs
Figure Mentioned:
- Fig. 38.3 – Compliance diagram of the lungs showing the inspiratory compliance curve and expiratory compliance curve.
- Fig. 38.4 – Comparison of the compliance of air-filled lungs and saline-filled lungs.
Compliance Diagram of the Lungs
- Fig. 38.3 shows the relationship between:
- Lung volume changes.
- Pleural pressure changes.
- Changes in pleural pressure also change the transpulmonary pressure.
- The relationship is different during inspiration and expiration.
- Each curve is obtained by:
- Changing pleural pressure in small steps.
- Allowing lung volume to reach a steady level before the next step.
- The two curves are:
- Inspiratory compliance curve
- Expiratory compliance curve
- Together, they form the compliance diagram of the lungs.
Factors Determining the Compliance Diagram
- The compliance diagram depends on the elastic forces of the lungs.
- These elastic forces have two components:
- Elastic forces of the lung tissue.
- Elastic forces produced by surface tension of the fluid lining the alveoli and other lung air spaces.
Elastic Forces of Lung Tissue
- Lung tissue elasticity depends mainly on:
- Elastin fibers
- Collagen fibers
- These fibers are interwoven throughout the lung parenchyma.
- In a deflated lung:
- The fibers are contracted and kinked.
- As the lungs expand:
- The fibers become stretched.
- The fibers become unkinked.
- They generate greater elastic force.
Elastic Forces Due to Surface Tension
- Surface tension forces are more complex.
- Fig. 38.4 compares:
- Air-filled lungs.
- Saline-filled lungs.
Air-Filled Lungs
- In air-filled lungs:
- There is an air–fluid interface inside the alveoli.
- This interface creates surface tension.
Saline-Filled Lungs
- In saline-filled lungs:
- There is no air–fluid interface.
- Therefore:
- Surface tension is absent.
- Only tissue elastic forces are present.
Comparison of Air-Filled and Saline-Filled Lungs
- Air-filled lungs require about three times more transpleural pressure to expand than saline-filled lungs.
- Therefore:
- Lung tissue elastic forces contribute about one-third (≈33%) of total lung elasticity.
- Surface tension contributes about two-thirds (≈67%) of total lung elasticity.
Effect of Surfactant
- Surface tension elastic forces increase greatly when surfactant is absent from the alveolar fluid.
Key Concept
- The compliance diagram (Fig. 38.3) shows different inspiratory and expiratory compliance curves. Total lung elasticity depends on lung tissue elasticity (≈1/3) and alveolar surface tension (≈2/3). Air-filled lungs require about three times more pressure to expand than saline-filled lungs, and absence of surfactant greatly increases surface tension.
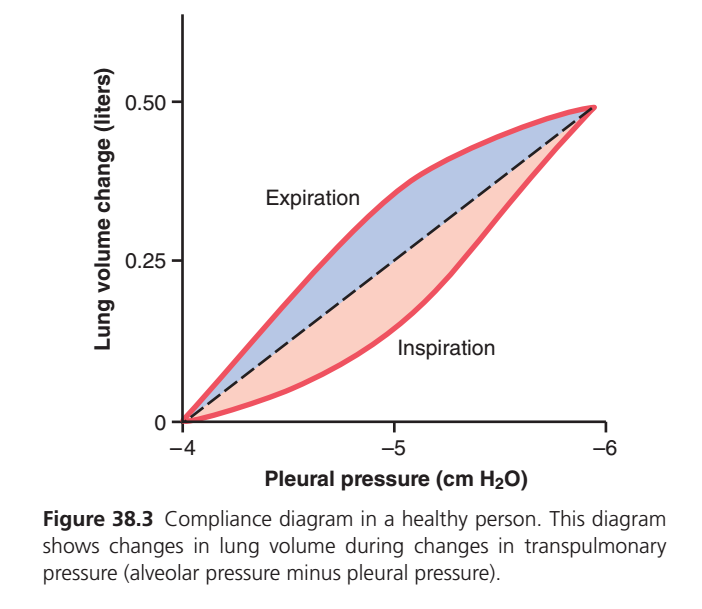
Guyton Figure 38.3 — Compliance Diagram of the Lungs
This is one of the highest-yield physiology graphs in MBBS because it explains:
- What lung compliance is
- Why inspiration and expiration follow different curves (hysteresis)
- Why the lungs do not inflate and deflate along the same path
- How surfactant reduces the work of breathing
- Why diseases like fibrosis and emphysema change compliance
Step 1. First Understand What This Graph Shows
This graph is NOT showing airflow.
It is showing:
How much the lung expands when the pressure across it changes.
Simply,
More pressure → More expansion
Exactly like inflating a balloon.
Step 2. Understand the Axes
X-axis (Horizontal)
Pleural Pressure (cm H₂O)
Left Right
-4 -5 -6Notice something unusual.
The numbers become more negative toward the right.
That means
Move Right
↓
Pleural pressure becomes MORE NEGATIVE
↓
Lungs are pulled outward more stronglyMore negative pleural pressure creates greater transpulmonary pressure, so the lungs expand.
Y-axis (Vertical)
Lung Volume Change (Liters)
Top
0.5 L
↑
More lung expansion
↓
Bottom
0 LHigher on the graph = lungs contain more air.
Step 3. What is Compliance?
Definition
Compliance is:
The ease with which the lungs expand.
Formula
Compliance=ΔPΔV
Where:
- ΔV = Change in lung volume
- ΔP = Change in transpulmonary pressure
Easy Balloon Analogy
Imagine two balloons.
Balloon A
Very soft.
Small pressure
↓
Big expansionHigh compliance.
Balloon B
Very stiff.
Large pressure
↓
Small expansionLow compliance.
The lungs behave exactly the same.
Step 4. The Red Curves
There are two red curves.
Many students think there should only be one.
But there are two because:
The lung behaves differently while filling and while emptying.
Lower Red Curve
Inspiration
Air entering
↓
Lung inflatingStarts here.
0 L
↓
0.5 LAs pleural pressure becomes more negative,
the lungs gradually expand.
Upper Red Curve
Expiration
Now lungs are already full.
Air leaves.
But surprisingly,
they do not return along the same path.
Instead,
they follow a different curve.
This phenomenon is called
Hysteresis
Step 5. What is Hysteresis?
The biggest concept in this graph.
Definition
The inspiratory and expiratory pressure-volume curves are different.
The lungs inflate and deflate by different paths.
Imagine opening a new balloon.
First inflation
Hard
↓
Needs extra pressureOnce inflated,
deflating is easier.
Exactly the same happens in the lungs.
Why Does This Happen?
Two major reasons.
Reason 1
Surfactant
When lungs inflate,
alveoli are initially small.
Surfactant molecules are crowded.
Surface tension changes during inflation.
As lungs expand,
surfactant spreads over a larger surface area.
On deflation,
surfactant becomes more concentrated again, reducing surface tension and making it easier to keep alveoli open.
Reason 2
Elastic Fibers
Elastic tissue behaves like a spring.
Stretching the spring requires more force than allowing it to recoil.
Therefore,
inflation requires more pressure,
while deflation occurs with less pressure.
Step 6. Why is the Expiratory Curve Higher?
Look carefully.
For the same pleural pressure, the expiratory curve lies above the inspiratory curve.
That means:
Same pressure
↓
Lung volume is larger during expirationExample
At
Pleural pressure = -5During inspiration
Volume may be
0.18 LDuring expiration
Volume may be
0.35 LWhy?
Because surfactant is more effective during deflation and alveoli remain open more easily.
Step 7. What is the Dashed Black Line?
This is an imaginary reference line.
It connects the start and end points.
It helps compare
- Inspiration
- Expiration
and clearly demonstrates hysteresis.
Step 8. What are the Colored Areas?
Pink Area
Represents the inspiratory path.
The lungs require extra pressure to open previously collapsed or smaller alveoli.
Blue Area
Represents the expiratory path.
The lungs retain more volume for the same pressure because alveoli stay open more easily during deflation.
Step 9. What Does the Area Between the Curves Mean?
This is extremely important.
The loop enclosed by the inspiratory and expiratory curves is called the hysteresis loop.
It represents:
Energy lost during one breathing cycle.
Why is energy lost?
Because some energy is used to overcome:
- Surface tension
- Elastic resistance
- Tissue friction
This energy cannot be fully recovered.
Easy Analogy
Rub your hands together.
Some movement becomes heat.
Similarly,
during breathing,
some muscular work is lost overcoming tissue and surface forces.
Step 10. Step-by-Step Story of the Graph
Stage 1
Beginning
Pleural Pressure
-4
↓
Volume = 0The lungs are at resting size.
Stage 2
Inspiration begins.
Diaphragm contracts.
Thoracic cavity expands
↓
Pleural pressure becomes more negative
↓
Transpulmonary pressure increases
↓
Lungs expandThe graph follows the lower (inspiratory) curve.
Stage 3
Maximum inspiration.
Pleural pressure
≈ -6
↓
Volume
≈0.5 LStage 4
Expiration begins.
Diaphragm relaxes.
Lungs recoil.
Instead of retracing the lower curve,
the graph follows the upper (expiratory) curve.
Stage 5
End expiration.
Returns to
Volume = 0Cycle repeats.
Step 11. Clinical Correlation
Pulmonary Fibrosis
Lungs become stiff.
Need more pressure
↓
Less expansionCompliance decreases.
The pressure-volume curve shifts downward and to the right.
Patients work harder to breathe.
Emphysema
Elastic fibers are destroyed.
Very easy expansion
↓
Poor recoilCompliance increases.
The curve shifts upward and to the left.
Patients can inflate lungs easily but have difficulty emptying them.
Surfactant Deficiency (e.g., Neonatal Respiratory Distress Syndrome)
Without surfactant:
- Surface tension increases.
- Alveoli collapse more easily.
- More pressure is required to inflate the lungs.
Compliance decreases and the hysteresis loop becomes larger.
Pneumothorax
Air enters the pleural cavity.
Pleural pressure rises toward atmospheric pressure.
Transpulmonary pressure falls.
The lung collapses because the expanding force is lost.
High-Yield Viva Questions
Q1. Define lung compliance.
Answer: Change in lung volume produced per unit change in transpulmonary pressure.
Q2. Normal lung compliance?
Approximately 200 mL/cm H₂O (0.2 L/cm H₂O) for both lungs together.
Q3. Why are there two curves?
Because of hysteresis—the inspiratory and expiratory pressure-volume relationships differ.
Q4. Why is the expiratory curve above the inspiratory curve?
Because surfactant is more effective during deflation, reducing surface tension and allowing the lungs to maintain a larger volume at the same pleural pressure.
Q5. Why is the inspiratory curve lower?
More pressure is needed to overcome surface tension and elastic resistance during inflation.
Q6. Which diseases increase compliance?
- Emphysema
- Aging (to some extent)
Q7. Which diseases decrease compliance?
- Pulmonary fibrosis
- Pulmonary edema
- Pneumonia
- ARDS
- Surfactant deficiency
MBBS Exam Pearls
- Compliance = ΔV / ΔP (change in volume per unit change in transpulmonary pressure).
- A steeper pressure-volume curve indicates higher compliance; a flatter curve indicates lower compliance.
- Two red curves represent inspiration (lower) and expiration (upper).
- The expiratory curve lies above the inspiratory curve because lungs retain more volume during deflation at the same pressure.
- The loop between the curves is the hysteresis loop, representing energy lost in overcoming elastic tissue resistance and surface tension during each breathing cycle.
- Surfactant reduces surface tension, increases compliance, decreases the work of breathing, and is a major reason for hysteresis.
- Pulmonary fibrosis decreases compliance (stiff lungs), whereas emphysema increases compliance (overly distensible lungs with poor recoil).
One-line memory trick:
“Compliance tells you how easily the lungs inflate; hysteresis tells you that inflating and deflating are not identical because surfactant and lung elasticity make expiration easier than inspiration.”
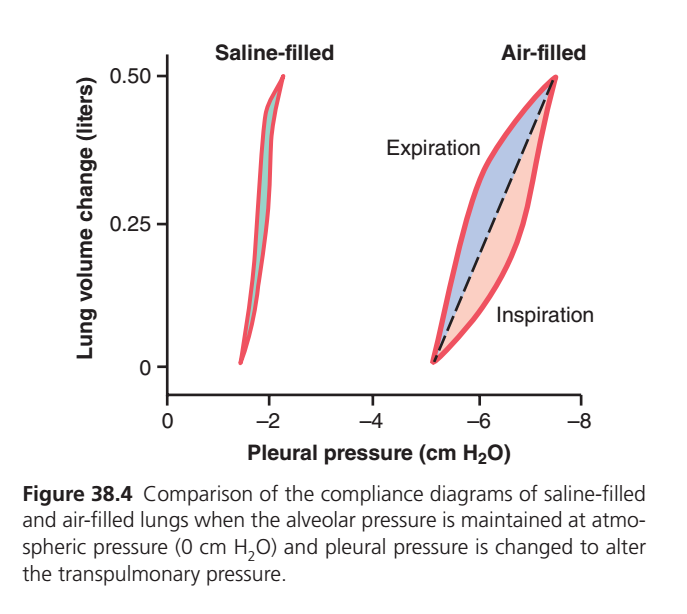
Guyton Figure 38.4 — Comparison of Compliance of Saline-Filled and Air-Filled Lungs
This figure is one of the most important graphs in respiratory physiology because it answers a fundamental question:
Why are lungs much easier to inflate when they are filled with saline instead of air?
The answer introduces the concept of surface tension, surfactant, and lung compliance.
BIG IDEA OF THIS GRAPH
This graph compares two identical lungs.
The only difference is:
| Lung | Filled With |
|---|---|
| Left Lung | Saline (water) |
| Right Lung | Air |
Everything else remains the same.
Then the pleural pressure is gradually changed, and the amount of lung expansion is measured.
Step 1. Understand the Axes
X-Axis
Pleural Pressure (cm H₂O)
0 ← -2 ← -4 ← -6 ← -8Moving toward the right means:
- Pleural pressure becomes more negative
- The lungs are pulled outward more strongly
- Lung expansion increases
Remember:
More negative pleural pressure = Greater transpulmonary pressure = More lung expansion
Y-Axis
Lung Volume Change (Liters)
0 L
│
│
0.25 L
│
│
0.50 LHigher on the graph means:
- More air (or saline) inside the lungs
- Greater lung expansion
Step 2. Look at the Left Side (Saline-Filled Lung)
This graph is very narrow.
It almost looks like one straight vertical line.
Volume ↑
0.5 │ │
│ │
│ │
0 └──────┘
-2Notice:
- Inspiration and expiration almost overlap.
- There is almost no hysteresis.
Why?
Because saline replaces the air inside the alveoli.
Now there is no air-water interface.
Since there is no interface,
there is no surface tension.
What normally creates surface tension?
Normally the alveolus looks like this.
Air
────────────
Water lining
────────────
Alveolar wallThe thin water layer tries to shrink.
This creates
Surface Tension
Surface tension pulls alveoli inward.
But in saline-filled lungs
Saline everywhere
██████████
██████████
██████████There is no air-water interface.
Therefore
Surface tension disappears.
Result
The lung becomes very easy to inflate.
Very little pressure produces a large increase in volume.
Therefore,
Compliance becomes very high.
Step 3. Why is There Almost No Hysteresis?
Remember
Hysteresis means
Inspiration and expiration follow different paths.
In saline lungs
Both curves almost overlap.
Why?
Because
There is almost no surface tension to overcome.
Only elastic fibers remain.
Elastic fibers behave similarly during inflation and deflation.
Therefore,
The inspiratory and expiratory curves become nearly identical.
Step 4. Look at the Right Side (Air-Filled Lung)
This is the normal lung.
Here you can clearly see
Two different curves.
Expiration
/
/
/
/
\
\
\
InspirationThis is called
Hysteresis
Why is the Air-Filled Lung Different?
Because now the alveoli contain
Air
↓
Water lining
↓
Surface tensionSurface tension resists expansion.
The lung becomes harder to inflate.
Step 5. Why Does Inspiration Need More Pressure?
During inspiration
The alveoli are initially small.
Surface tension tries to collapse them.
The inspiratory muscles must overcome
- Elastic tissue
- Surface tension
Therefore,
More negative pleural pressure is needed.
Step 6. Why is Expiration Easier?
During expiration
Surfactant becomes more concentrated as the alveoli become smaller.
Surface tension decreases.
The alveoli remain open more easily.
Thus,
The expiratory curve stays above the inspiratory curve.
Step 7. Compare Both Graphs
Saline-Filled Lung
No Air
↓
No Air-Water Interface
↓
No Surface Tension
↓
Only Elastic Fibers Resist Inflation
↓
Very Easy Expansion
↓
High ComplianceAir-Filled Lung
Air Present
↓
Air-Water Interface
↓
Surface Tension Present
↓
Elastic Tissue + Surface Tension Resist Inflation
↓
Harder Expansion
↓
Lower ComplianceStep 8. What Does This Teach Us?
The graph proves an important physiological fact.
The lungs do not resist expansion mainly because of elastic tissue.
Instead,
Surface tension is the major force opposing lung expansion.
Approximate contribution to elastic recoil:
- Surface tension: ~2/3 (≈65–70%)
- Elastic tissue: ~1/3 (≈30–35%)
This is why removing surface tension with saline dramatically increases compliance.
Step 9. Why Does Surfactant Matter?
Surfactant reduces surface tension.
Without surfactant,
the air-filled lung would behave much more stiffly.
Surfactant makes normal breathing possible by:
- Increasing lung compliance.
- Reducing the work of breathing.
- Preventing alveolar collapse (atelectasis), especially during expiration.
- Reducing hysteresis compared with what it would otherwise be.
Step 10. Clinical Correlations
1. Neonatal Respiratory Distress Syndrome (NRDS)
Premature infants have insufficient surfactant.
Result:
Less Surfactant
↓
More Surface Tension
↓
Very Low Compliance
↓
Lungs Hard to InflateThese infants must generate very high inspiratory pressures to breathe.
2. Acute Respiratory Distress Syndrome (ARDS)
Surfactant is damaged or inactivated.
Compliance falls.
Patients develop stiff lungs and require more pressure for ventilation.
3. Pulmonary Fibrosis
Compliance decreases because the lung tissue itself becomes stiff.
This is different from surfactant deficiency, where increased surface tension is the major problem.
4. Emphysema
Elastic fibers are destroyed.
Compliance increases because elastic recoil is reduced.
Patients inflate their lungs easily but have difficulty exhaling.
Step 11. Difference Between Elastic Tissue and Surface Tension
| Elastic Tissue | Surface Tension |
|---|---|
| Comes from elastin and collagen fibers | Comes from the air-water interface lining the alveoli |
| Present in both saline- and air-filled lungs | Present only in air-filled lungs |
| Provides about one-third of elastic recoil | Provides about two-thirds of elastic recoil |
| Cannot be removed by saline | Eliminated when alveoli are filled with saline |
Step 12. High-Yield Comparison Table
| Feature | Saline-Filled Lung | Air-Filled Lung |
|---|---|---|
| Air-water interface | ❌ Absent | ✅ Present |
| Surface tension | ❌ Absent | ✅ Present |
| Surfactant needed | ❌ No | ✅ Yes |
| Compliance | Very high | Lower (normal) |
| Pressure needed for inflation | Low | Higher |
| Hysteresis | Minimal/nearly absent | Prominent |
| Work of breathing | Low | Higher |
Complete Story of the Graph
SALINE LUNG
No Air
↓
No Air-Water Interface
↓
No Surface Tension
↓
Only Elastic Tissue Resists
↓
Very High Compliance
↓
Almost No Hysteresis
AIR-FILLED LUNG
Air Present
↓
Air-Water Interface
↓
Surface Tension Present
↓
Elastic Tissue + Surface Tension Resist Inflation
↓
Lower Compliance
↓
Large Hysteresis LoopMBBS Viva Questions
Q1. Why is compliance greater in a saline-filled lung?
Answer: Because filling the alveoli with saline eliminates the air-water interface, removing surface tension. Only the elastic tissue opposes expansion, so less pressure is needed to inflate the lungs.
Q2. Why is hysteresis minimal in saline-filled lungs?
Answer: Surface tension is absent, so inspiration and expiration are governed mainly by elastic tissue, causing the pressure-volume curves to nearly overlap.
Q3. Which force contributes most to the elastic recoil of normal lungs?
Answer: Surface tension at the alveolar air-water interface contributes about two-thirds of the elastic recoil, while elastic fibers contribute about one-third.
Q4. What is the role of surfactant in the air-filled lung?
Answer: Surfactant lowers alveolar surface tension, increases compliance, reduces the work of breathing, stabilizes alveoli, and helps prevent alveolar collapse during expiration.
One-Line Memory Trick
“Saline removes surface tension, making the lungs highly compliant with almost no hysteresis; air introduces surface tension, so more pressure is needed to inflate the lungs and a hysteresis loop appears.”
Hysteresis of the Lungs
Most MBBS students find hysteresis confusing because of its name. In reality, it is a very simple concept.
First Learn One Sentence
Hysteresis means the lungs do not inflate and deflate along the same path.
That’s all.
Balloon Analogy (The Easiest Way)
Imagine you buy a new balloon.
First Time You Inflate It
You try to blow air into it.
😮💨
Very Hard
Needs a lot of pressureWhy?
Because the balloon is tightly folded.
Now Deflate the Balloon
Air comes out.
Now inflate it again.
😮💨
Much EasierThe balloon is already stretched.
It opens much more easily.
This is exactly what happens in the lungs.
In the Lungs
During Inspiration
The alveoli are small.
They must be opened.
Surface tension tries to collapse them.
So the inspiratory muscles must work harder.
Small alveoli
↓
Need more pressure
↓
Lung expandsDuring Expiration
The alveoli are already open.
They don’t collapse immediately because surfactant keeps them open.
So,
Open alveoli
↓
Need less pressure
↓
Air comes out easilyThis Difference is Called
HYSTERESIS One-Line Definition
Hysteresis is the difference between the inspiratory and expiratory pressure-volume curves.
Or even simpler:
The lung follows one path while filling and another path while emptying.
See It Like a Road
Imagine two roads.
Going Up
↗
Coming Down
↘You reach the same destination,
but you use different roads.
The lungs behave the same way.
Why Doesn’t the Lung Use the Same Path?
Because during inspiration and expiration, the alveoli behave differently.
Inspiration
Alveoli Closed
↓
Need to Open Them
↓
More Pressure NeededExpiration
Alveoli Already Open
↓
Surfactant Prevents Collapse
↓
Less Pressure NeededTherefore,
the lung volume is greater during expiration than during inspiration at the same pleural pressure.
This creates two separate curves.
Simple Example
Suppose pleural pressure is −5 cm H₂O.
During Inspiration
Pressure = -5
↓
Volume = 200 mLDuring Expiration
Pressure = -5
↓
Volume = 350 mLNotice something.
Same pressure.
Different volume.
This difference is called
Hysteresisy Does Hysteresis Occur?
There are two reasons.
1. Surface Tension ⭐⭐⭐ (Most Important)
Inside every alveolus,
Air
↓
Thin Water Layer
↓
Surface TensionSurface tension wants to collapse the alveolus.
During inspiration,
extra pressure is needed to overcome this.
During expiration,
surfactant becomes relatively more concentrated as alveoli get smaller, reducing surface tension and helping alveoli stay open.
This is the main reason for hysteresis.2. Elastic Fibers
The lung contains elastic tissue.
Like stretching a spring,
Stretching
Hard
↓
Returning
EasyElastic fibers also contribute to hysteresis, but less than surface tension.
What Happens if We Fill the Lung with Saline?
This is exactly what Guyton Figure 38.4 demonstrates.
Saline
↓
No Air
↓
No Air-Water Interface
↓
No Surface Tension
↓
Almost No HysteresisNow the inspiration and expiration curves almost overlap.
This proves that surface tension is the major cause of hysteresis.mory Trick
Think of a Sticky Door
Imagine a door.
Opening It
Push Hard
🚪
Needs ForceClosing It
Very Easy
🚪The lungs behave like that door.
Opening (inspiration) is harder than closing (expiration).
That difference is called hysteresis.
One Complete Story
Start
↓
Alveoli Small
↓
Need More Pressure
↓
Inspiration
↓
Lung Becomes Full
↓
Surfactant Keeps Alveoli Open
↓
Expiration Needs Less Pressure
↓
Different Path
↓
HYSTERESISWhy is Hysteresis Important Clinically?BS Viva Answer (2 Lines)
Q: What is hysteresis?
Answer:
Hysteresis is the phenomenon in which the pressure-volume curve during inspiration is different from the pressure-volume curve during expiration. It occurs mainly because of changes in alveolar surface tension (modified by surfactant) and, to a lesser extent, the elastic properties of the lung tissue.
10-Second Memory Trick
“Opening a new balloon is harder than letting air out. The lungs behave the same way—more pressure is needed to inflate than to deflate. This difference is called hysteresis.”
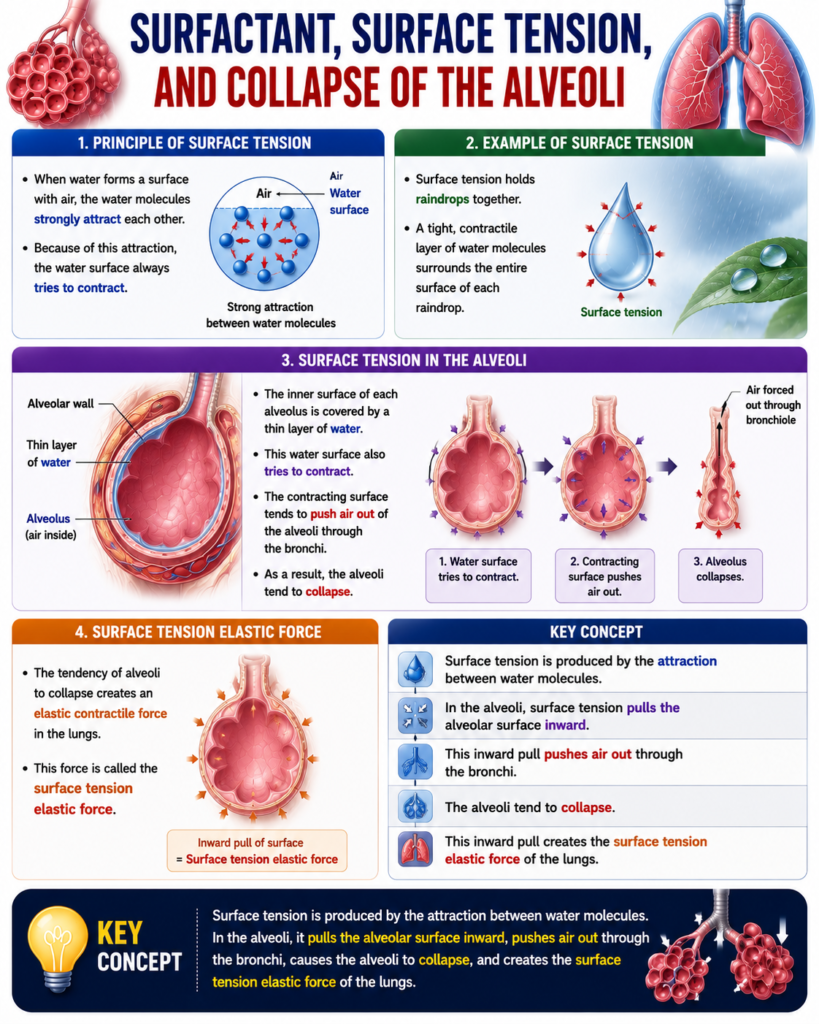
Surfactant, Surface Tension, and Collapse of the Alveoli
Principle of Surface Tension
- When water forms a surface with air, the water molecules strongly attract each other.
- Because of this attraction, the water surface always tries to contract.
Example of Surface Tension
- Surface tension holds raindrops together.
- A tight, contractile layer of water molecules surrounds the entire surface of each raindrop.
Surface Tension in the Alveoli
- The inner surface of each alveolus is covered by a thin layer of water.
- This water surface also tries to contract.
- The contracting surface tends to push air out of the alveoli through the bronchi.
- As a result, the alveoli tend to collapse.
Surface Tension Elastic Force
- The tendency of alveoli to collapse creates an elastic contractile force in the lungs.
- This force is called the surface tension elastic force.
Key Concept
- Surface tension is produced by the attraction between water molecules. In the alveoli, it pulls the alveolar surface inward, pushes air out through the bronchi, causes the alveoli to collapse, and creates the surface tension elastic force of the lungs.
Surfactant and Its Effect on Surface Tension
Figure Mentioned:
- Fig. 38.3 – Compliance diagram in a healthy person.
- Fig. 38.4 – Comparison of compliance diagrams of air-filled and saline-filled lungs.
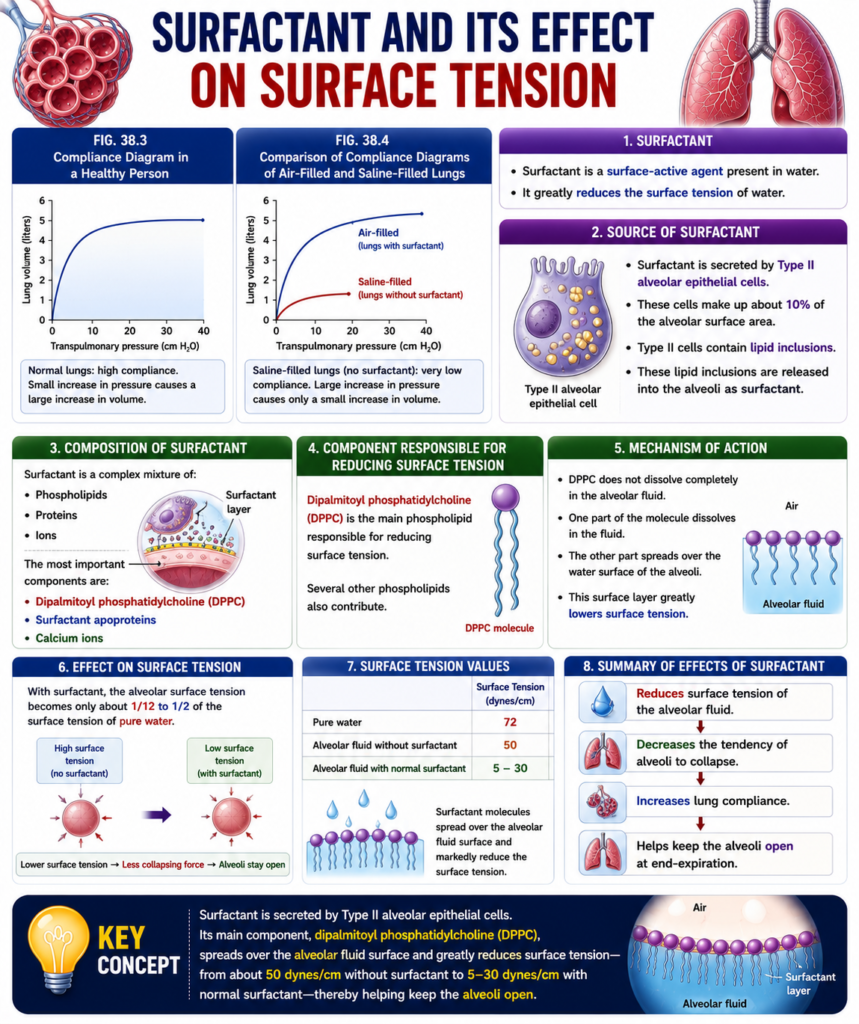
Surfactant
- Surfactant is a surface-active agent present in water.
- It greatly reduces the surface tension of water.
Source of Surfactant
- Surfactant is secreted by Type II alveolar epithelial cells.
- These cells make up about 10% of the alveolar surface area.
- Type II cells contain lipid inclusions.
- These lipid inclusions are released into the alveoli as surfactant.
Composition of Surfactant
- Surfactant is a complex mixture of:
- Phospholipids
- Proteins
- Ions
- The most important components are:
- Dipalmitoyl phosphatidylcholine (DPPC)
- Surfactant apoproteins
- Calcium ions
Component Responsible for Reducing Surface Tension
- Dipalmitoyl phosphatidylcholine (DPPC) is the main phospholipid responsible for reducing surface tension.
- Several other phospholipids also contribute.
Mechanism of Action
- DPPC does not dissolve completely in the alveolar fluid.
- One part of the molecule dissolves in the fluid.
- The other part spreads over the water surface of the alveoli.
- This surface layer greatly lowers surface tension.
Effect on Surface Tension
- With surfactant, the alveolar surface tension becomes only about 1/12 to 1/2 of the surface tension of pure water.
Surface Tension Values
- Pure water: 72 dynes/cm
- Alveolar fluid without surfactant: 50 dynes/cm
- Alveolar fluid with normal surfactant: 5–30 dynes/cm
Key Concept
- Surfactant is secreted by Type II alveolar epithelial cells. Its main component, dipalmitoyl phosphatidylcholine (DPPC), spreads over the alveolar fluid surface and greatly reduces surface tension—from about 50 dynes/cm without surfactant to 5–30 dynes/cm with normal surfactant—thereby helping keep the alveoli open.
Pressure in Occluded Alveoli Caused by Surface Tension
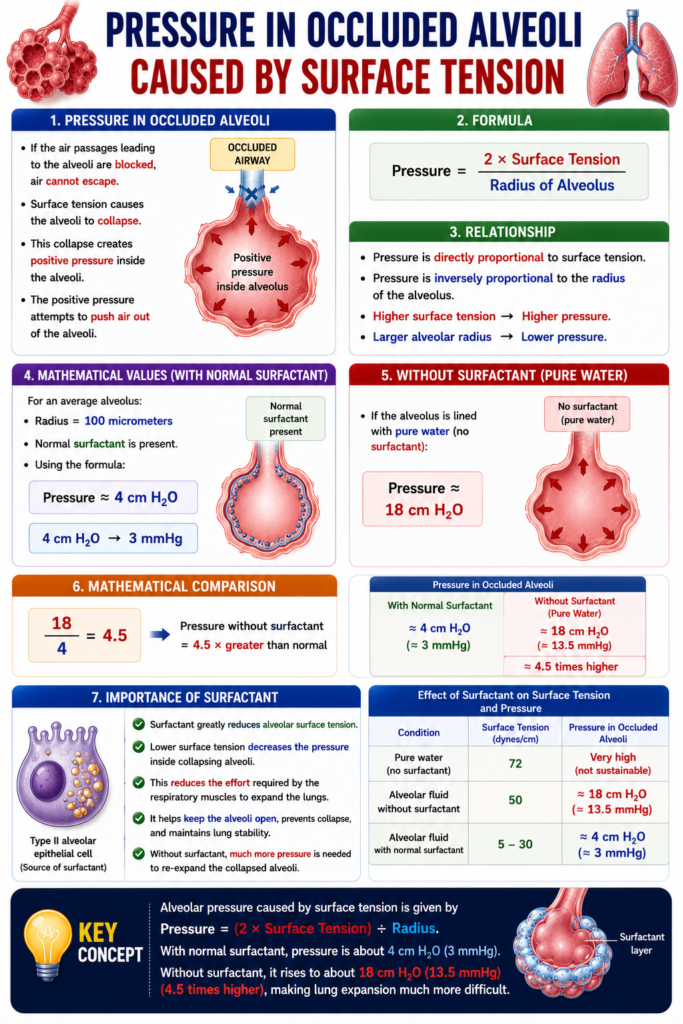
Pressure in Occluded Alveoli
- If the air passages leading to the alveoli are blocked, air cannot escape.
- Surface tension causes the alveoli to collapse.
- This collapse creates positive pressure inside the alveoli.
- The positive pressure attempts to push air out of the alveoli.
Formula
Pressure=Radius of Alveolus2×Surface Tension
Relationship
- Pressure is directly proportional to surface tension.
- Pressure is inversely proportional to the radius of the alveolus.
- Higher surface tension → Higher pressure.
- Larger alveolar radius → Lower pressure.
Mathematical Values
For an average alveolus:
- Radius = 100 micrometers
- Normal surfactant is present.
Using the formula:Pressure≈4 cm H2O 4 cm H2O≈3 mmHg
Without Surfactant
If the alveolus is lined with pure water (no surfactant):Pressure≈18 cm H2O
Mathematical Comparison
418=4.5 Pressure without surfactant=4.5×greater than normal
Importance of Surfactant
- Surfactant greatly reduces alveolar surface tension.
- Lower surface tension decreases the pressure inside collapsing alveoli.
- This reduces the effort required by the respiratory muscles to expand the lungs.
Key Concept
- Alveolar pressure caused by surface tension is given by Pressure = (2 × Surface Tension) ÷ Radius. With normal surfactant, pressure is about 4 cm H₂O (3 mmHg). Without surfactant, it rises to about 18 cm H₂O (4.5 times higher), making lung expansion much more difficult.
Pressure Caused by Surface Tension Is Inversely Related to Alveolar Radius
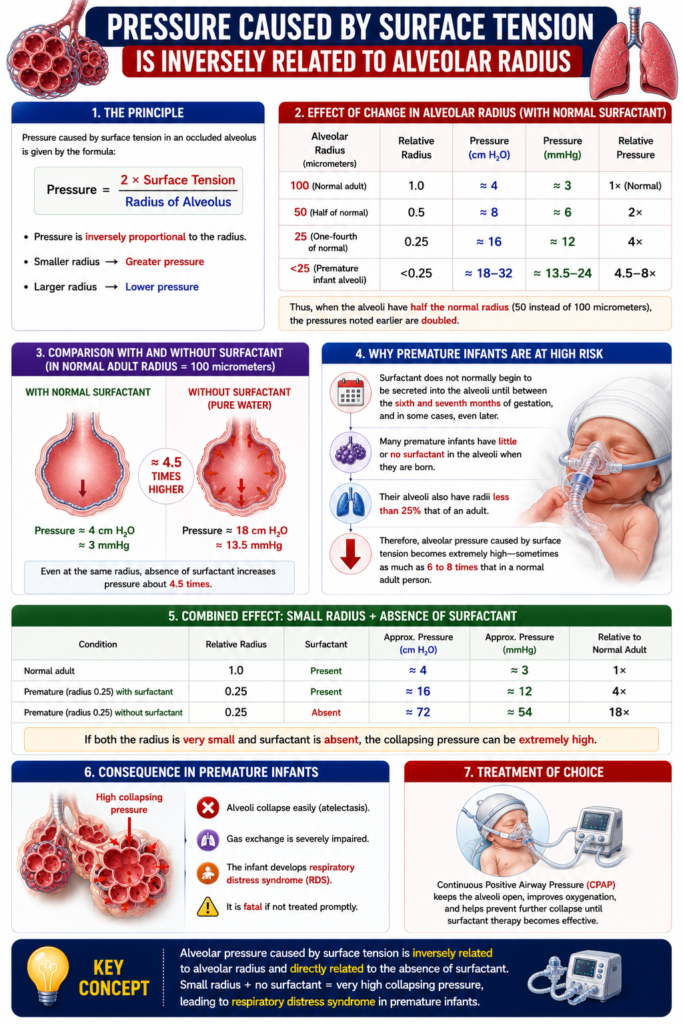
Relationship Between Pressure and Alveolar Radius
- From the previous formula:
Pressure=Radius of Alveolus2×Surface Tension
- Pressure is inversely related to alveolar radius.
- As the alveolar radius decreases, the pressure increases.
- As the alveolar radius increases, the pressure decreases.
Mathematical Calculation
Normal Alveolus
Given:
- Radius = 100 µm
- Pressure = 4 cm H₂O
Alveolus with Half the Radius
Given:
- Radius = 50 µm
Using the inverse relationship:P2=P1×R2R1
Substitute the values:P2=4×50100 P2=4×2 P2=8 cm H2O
Answer:
When the alveolar radius decreases from 100 µm to 50 µm, the pressure doubles from 4 cm H₂O to 8 cm H₂O.
Significance in Premature Infants
- This effect is especially important in small premature infants.
- Many premature infants have alveoli with a radius less than 25% of that of an adult.
Surfactant Secretion
- Surfactant normally begins to be secreted into the alveoli between the 6th and 7th months of gestation.
- In some cases, surfactant secretion begins even later.
- Therefore, many premature infants are born with little or no surfactant in their alveoli.
Effect of Surfactant Deficiency
- Without enough surfactant:
- The lungs have an extreme tendency to collapse.
- Lung collapse may be 6–8 times greater than in a normal adult.
Respiratory Distress Syndrome of the Newborn
- Severe alveolar collapse causes respiratory distress syndrome (RDS) of the newborn.
- RDS can be fatal if not treated.
- Treatment requires properly applied continuous positive pressure breathing.
Key Concept
- Pressure caused by surface tension is inversely proportional to alveolar radius. Halving the alveolar radius (100 µm → 50 µm) doubles alveolar pressure (4 → 8 cm H₂O). Premature infants have very small alveoli and little or no surfactant, causing severe lung collapse (6–8 times greater than normal) and respiratory distress syndrome of the newborn.
EFFECT OF THE THORACIC CAGE ON LUNG EXPANSIBILITY
Effect of the Thoracic Cage on Lung Expansibility
- So far, lung expansibility has been discussed without considering the thoracic cage.
- The thoracic cage has its own:
- Elastic properties
- Viscous properties
- The thoracic cage resists expansion because of these properties.
- Even if the lungs were absent, muscular effort would still be required to expand the thoracic cage.
Key Concept
- Lung expansion depends not only on the lungs but also on the thoracic cage. The thoracic cage has its own elastic and viscous properties, so muscular effort is required to expand it even without the lungs.
Compliance of Thorax and Lungs Together
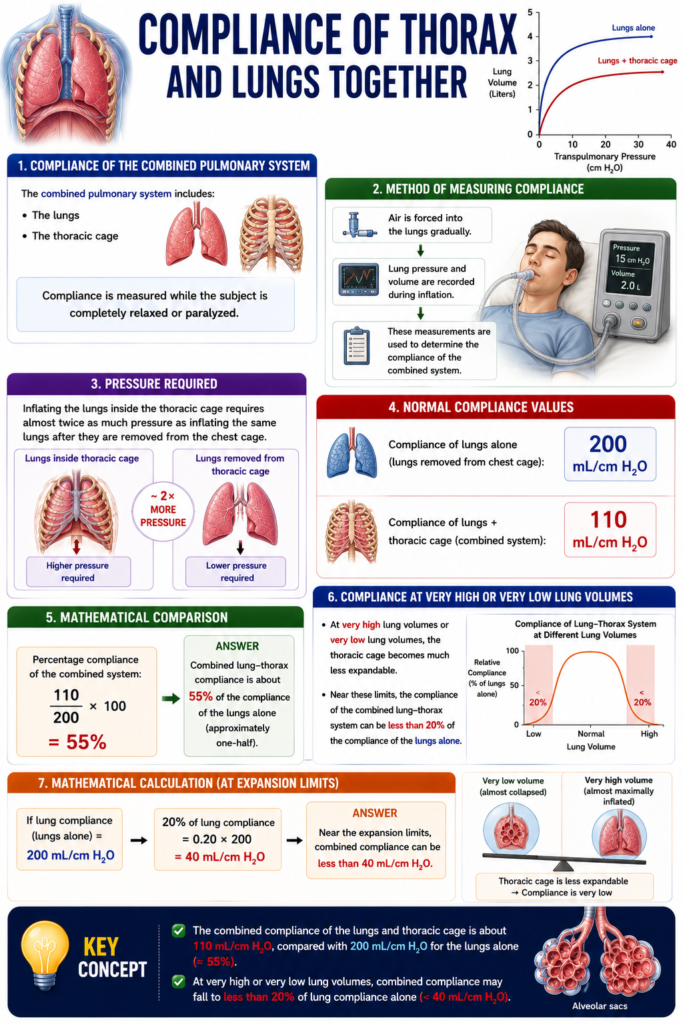
Compliance of the Combined Pulmonary System
- The combined pulmonary system includes:
- The lungs
- The thoracic cage
- Compliance is measured while the subject is completely relaxed or paralyzed.
Method of Measuring Compliance
- Air is forced into the lungs gradually.
- Lung pressure and volume are recorded during inflation.
- These measurements are used to determine the compliance of the combined system.
Pressure Required
- Inflating the lungs inside the thoracic cage requires almost twice as much pressure as inflating the same lungs after they are removed from the chest cage.
Normal Compliance Values
- Compliance of lungs alone:
200 mL/cm H2O
- Compliance of lungs + thoracic cage:
110 mL/cm H2O
Mathematical Comparison
Percentage compliance of the combined system:200110×100 =55%
Answer:
- Combined lung-thorax compliance is about 55% of the compliance of the lungs alone (approximately one-half).
Compliance at Very High or Very Low Lung Volumes
- At very high lung volumes or very low lung volumes, the thoracic cage becomes much less expandable.
- Near these limits, the compliance of the combined lung-thorax system can be less than 20% of the compliance of the lungs alone.
Mathematical Calculation
If lung compliance = 200 mL/cm H₂O20%×200 =0.20×200 =40 mL/cm H2O
Answer:
Near the expansion limits, combined compliance can be less than 40 mL/cm H₂O.
Key Concept
- The combined compliance of the lungs and thoracic cage is about 110 mL/cm H₂O, compared with 200 mL/cm H₂O for the lungs alone (≈55%). At very high or very low lung volumes, combined compliance may fall to less than 20% of lung compliance alone (<40 mL/cm H₂O).
Work of Breathing
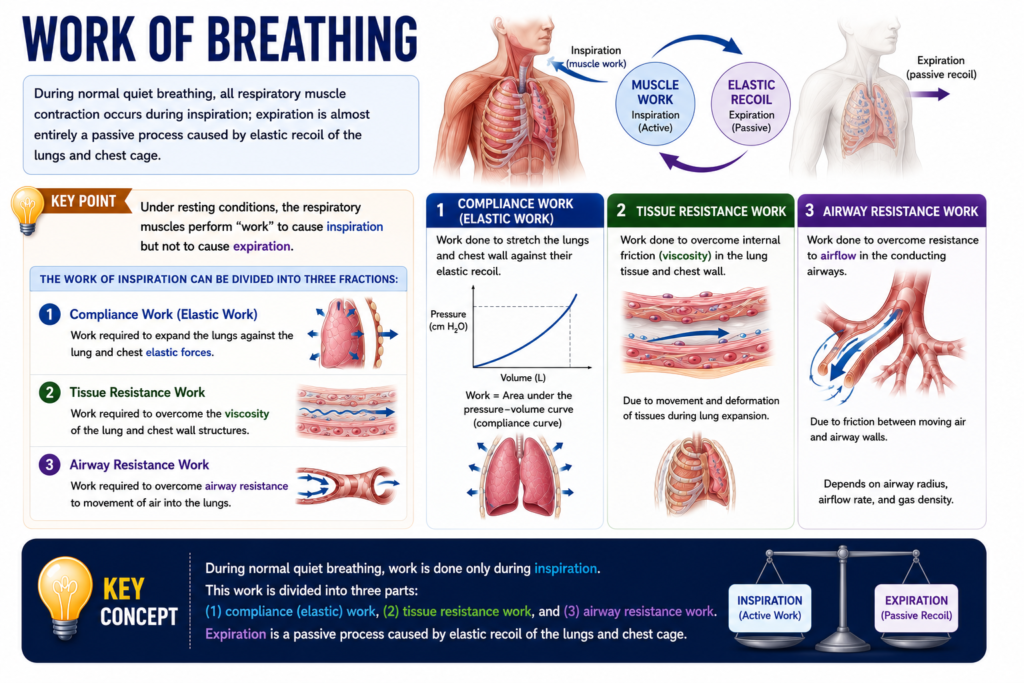
Work During Normal Quiet Breathing
- During normal quiet breathing, respiratory muscles contract only during inspiration.
- Expiration is almost entirely a passive process.
- Passive expiration occurs because of the elastic recoil of:
- The lungs.
- The chest cage.
- Therefore, under resting conditions:
- Respiratory muscles perform work during inspiration.
- Respiratory muscles do not normally perform work during expiration.
Three Types of Inspiratory Work
1. Compliance Work (Elastic Work)
- This is the work required to expand the lungs.
- It overcomes the elastic forces of:
- The lungs.
- The chest wall.
- It is also called elastic work.
2. Tissue Resistance Work
- This is the work required to overcome the viscosity of:
- The lung tissues.
- The chest wall structures.
3. Airway Resistance Work
- This is the work required to overcome the airway resistance.
- It allows air to move into the lungs during inspiration.
Key Concept
- During normal quiet breathing, respiratory muscles perform work only during inspiration, while expiration is passive due to elastic recoil. Inspiratory work has three components: compliance (elastic) work, tissue resistance work, and airway resistance work.
Energy Required for Respiration
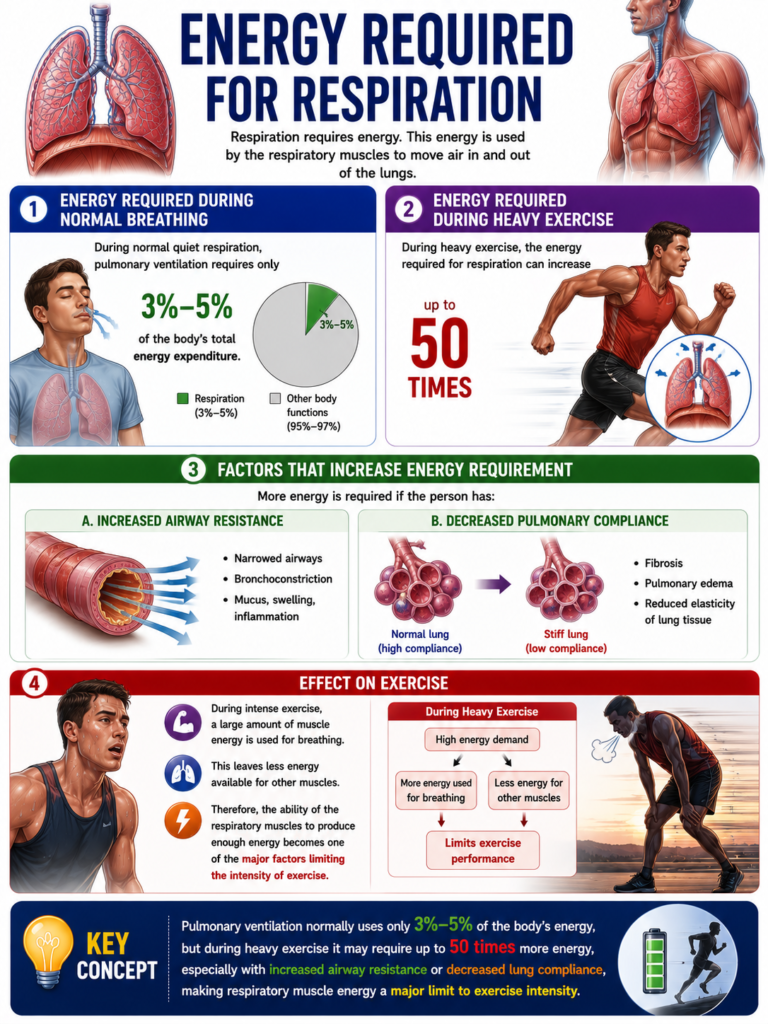
Energy Required During Normal Breathing
- During normal quiet respiration, pulmonary ventilation requires only 3%–5% of the body’s total energy expenditure.
Energy Required During Heavy Exercise
- During heavy exercise, the energy required for respiration can increase by up to 50 times.
Factors That Increase Energy Requirement
- More energy is required if the person has:
- Increased airway resistance
- Decreased pulmonary compliance
Effect on Exercise
- During intense exercise, a large amount of muscle energy is used for breathing.
- Therefore, the ability of the respiratory muscles to produce enough energy becomes one of the major factors limiting the intensity of exercise.
Key Concept
- Pulmonary ventilation normally uses only 3%–5% of the body’s energy, but during heavy exercise it may require up to 50 times more energy, especially with increased airway resistance or decreased lung compliance, making respiratory muscle energy a major limit to exercise intensity.