

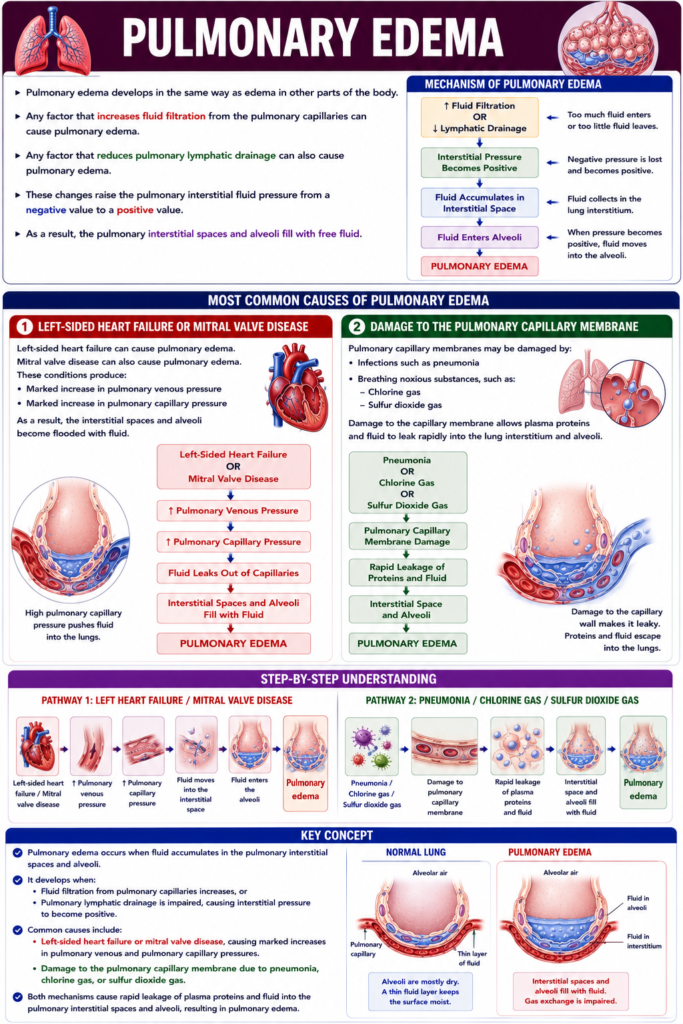
- Pulmonary edema develops in the same way as edema in other parts of the body.
- Any factor that increases fluid filtration from the pulmonary capillaries can cause pulmonary edema.
- Any factor that reduces pulmonary lymphatic drainage can also cause pulmonary edema.
- These changes raise the pulmonary interstitial fluid pressure from a negative value to a positive value.
- As a result, the pulmonary interstitial spaces and alveoli fill with free fluid.
Mechanism of Pulmonary Edema
- Increased fluid filtration or reduced lymphatic drainage causes fluid to accumulate in the pulmonary interstitium.
- When the interstitial pressure becomes positive, fluid enters the alveoli.
Easy Concept
↑ Fluid Filtration
OR
↓ Lymphatic Drainage
│
▼
Interstitial Pressure
Becomes Positive
│
▼
Fluid Accumulates
in Interstitial Space
│
▼
Fluid Enters Alveoli
│
▼
Pulmonary EdemaConcept:
- Too much fluid enters or too little fluid leaves.
- Therefore, fluid accumulates in the lungs.
Most Common Causes of Pulmonary Edema
1. Left-Sided Heart Failure or Mitral Valve Disease
- Left-sided heart failure can cause pulmonary edema.
- Mitral valve disease can also cause pulmonary edema.
- These conditions produce:
- Marked increase in pulmonary venous pressure
- Marked increase in pulmonary capillary pressure
- As a result, the interstitial spaces and alveoli become flooded with fluid.
Easy Concept
Left-Sided Heart Failure
OR
Mitral Valve Disease
│
▼
↑ Pulmonary Venous Pressure
│
▼
↑ Pulmonary Capillary Pressure
│
▼
Fluid Leaks Out
of Capillaries
│
▼
Interstitial Spaces
and Alveoli Fill
with Fluid
│
▼
Pulmonary EdemaConcept:
- High pulmonary capillary pressure pushes fluid into the lungs.
- This results in pulmonary edema.
2. Damage to the Pulmonary Capillary Membrane
Easy Concept
Pneumonia
OR
Chlorine Gas
OR
Sulfur Dioxide Gas
│
▼
Pulmonary Capillary
Membrane Damage
│
▼
Rapid Leakage of
Proteins and Fluid
│
▼
Interstitial Space
and Alveoli
│
▼
Pulmonary EdemaConcept:
- Damage to the capillary wall makes it leaky.
- Therefore, proteins and fluid escape into the lungs.
Step-by-Step Understanding
Pathway 1
Left-sided heart failure / Mitral valve disease
↓
↑ Pulmonary venous pressure
↓
↑ Pulmonary capillary pressure
↓
Fluid moves into the interstitial space
↓
Fluid enters the alveoli
↓
Pulmonary edema
Pathway 2
Pneumonia / Chlorine gas / Sulfur dioxide gas
↓
Damage to pulmonary capillary membrane
↓
Rapid leakage of plasma proteins and fluid
↓
Interstitial space and alveoli fill with fluid
↓
Pulmonary edema
Key Concept
- Pulmonary edema occurs when fluid accumulates in the pulmonary interstitial spaces and alveoli.
- It develops when:
- Fluid filtration from pulmonary capillaries increases, or
- Pulmonary lymphatic drainage is impaired, causing interstitial pressure to become positive.
- Common causes include:
- Left-sided heart failure or mitral valve disease, causing marked increases in pulmonary venous and pulmonary capillary pressures.
- Damage to the pulmonary capillary membrane due to pneumonia, chlorine gas, or sulfur dioxide gas.
- Both mechanisms cause rapid leakage of plasma proteins and fluid into the pulmonary interstitial spaces and alveoli, resulting in pulmonary edema.
Pulmonary Edema Safety Factor
Figure: Fig. 39.8
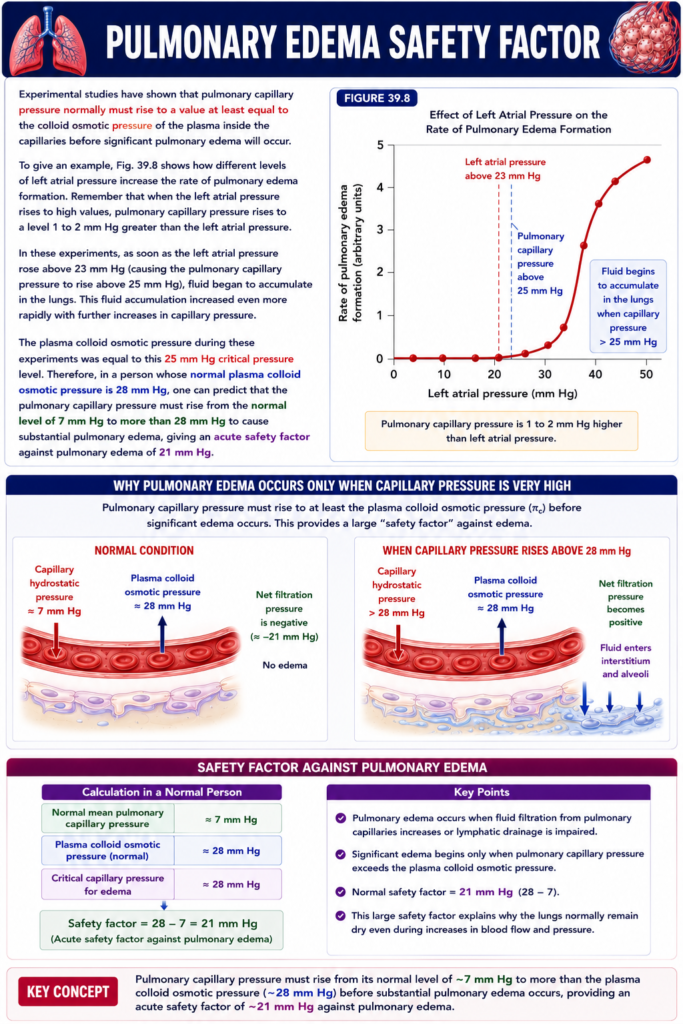
- Experimental studies show that pulmonary capillary pressure must rise to at least the plasma colloid osmotic pressure before significant pulmonary edema develops.
- Fig. 39.8 shows how different levels of left atrial pressure increase the rate of pulmonary edema formation.
- When the left atrial pressure rises, the pulmonary capillary pressure also rises.
- The pulmonary capillary pressure is usually 1–2 mm Hg higher than the left atrial pressure.
Easy Concept
Left Atrial Pressure Increases
│
▼
Pulmonary Capillary Pressure
Also Increases
(1–2 mm Hg Higher)
│
▼
Higher Chance of
Pulmonary EdemaConcept:
- Higher left atrial pressure → Higher pulmonary capillary pressure.
- Higher pulmonary capillary pressure → Greater risk of pulmonary edema.
Critical Pressure for Pulmonary Edema
- In these experiments, left atrial pressure increased above 23 mm Hg.
- This caused the pulmonary capillary pressure to rise above 25 mm Hg.
- At this point, fluid began to accumulate in the lungs.
- As the pulmonary capillary pressure increased further, fluid accumulated even more rapidly.
Step-by-Step Understanding
Step 1
Left Atrial Pressure = 23 mm Hg
↓
Step 2
Pulmonary Capillary Pressure = 25 mm Hg
(About 1–2 mm Hg higher)
↓
Step 3
Fluid Begins to Accumulate in the Lungs
↓
Step 4
Further Increase in Capillary Pressure
↓
Pulmonary Edema Develops More Rapidly
Easy Concept
Left Atrial Pressure
23 mm Hg
│
▼
Pulmonary Capillary Pressure
25 mm Hg
│
▼
Fluid Starts Entering
the Lungs
│
▼
Pulmonary Edema BeginsConcept:
- 25 mm Hg is the critical pulmonary capillary pressure in these experiments.
- Above this level, fluid begins to leak into the lungs.
Role of Plasma Colloid Osmotic Pressure
- During these experiments, the plasma colloid osmotic pressure was 25 mm Hg.
- This value was equal to the critical pulmonary capillary pressure at which pulmonary edema began.
Easy Concept
Pulmonary Capillary Pressure
25 mm Hg
=
Plasma Colloid Osmotic Pressure
25 mm Hg
│
▼
Pulmonary Edema BeginsConcept:
- When the outward capillary pressure equals the inward plasma colloid osmotic pressure, fluid starts leaking into the lungs.
Pulmonary Edema Safety Factor
- In a normal person, the plasma colloid osmotic pressure is about 28 mm Hg.
- The normal pulmonary capillary pressure is about 7 mm Hg.
- Therefore, the pulmonary capillary pressure must rise above 28 mm Hg before significant pulmonary edema develops.
Step-by-Step Calculation
Step 1
Normal Pulmonary Capillary Pressure = 7 mm Hg
↓
Step 2
Critical Pressure Needed for Pulmonary Edema = 28 mm Hg
↓
Step 3
Formula
Safety Factor
= Critical Pulmonary Capillary Pressure
− Normal Pulmonary Capillary PressureSubstitute the Values
= 28 − 7Solve
= 21 mm HgFinal Answer
Pulmonary Edema Safety Factor = 21 mm Hg
Easy Concept
Normal Pulmonary
Capillary Pressure
7 mm Hg
│
▼
Must Rise Above
28 mm Hg
│
▼
Difference
28 − 7
= 21 mm Hg
↓
Pulmonary Edema
Safety FactorConcept:
- The lungs can tolerate a 21 mm Hg increase in pulmonary capillary pressure before significant pulmonary edema develops.
Easy Memory Trick
Normal Pressure
7 mm Hg
↓
Critical Pressure
28 mm Hg
↓
Safety Margin
21 mm HgRemember:
7 → 28 → 21
(Normal → Critical → Safety Factor)
Key Concept
- Fig. 39.8 shows that higher left atrial pressure increases the rate of pulmonary edema formation.
- Pulmonary capillary pressure is usually 1–2 mm Hg higher than left atrial pressure.
- In the experiments:
- Left atrial pressure >23 mm Hg
- Pulmonary capillary pressure >25 mm Hg
- Fluid began to accumulate in the lungs.
- As pulmonary capillary pressure increased further, pulmonary edema developed more rapidly.
- The critical pulmonary capillary pressure was equal to the plasma colloid osmotic pressure (25 mm Hg) in these experiments.
- In a normal person:
- Normal pulmonary capillary pressure = 7 mm Hg
- Normal plasma colloid osmotic pressure = 28 mm Hg
- Safety Factor = 28 − 7 = 21 mm Hg.
- This 21 mm Hg safety factor protects the lungs from developing significant pulmonary edema under normal conditions.
Pulmonary Edema Safety Factor
Figure: Fig. 39.8
- Experimental studies show that pulmonary capillary pressure must rise to at least the plasma colloid osmotic pressure before significant pulmonary edema develops.
- Fig. 39.8 shows how different levels of left atrial pressure increase the rate of pulmonary edema formation.
- When the left atrial pressure rises, the pulmonary capillary pressure also rises.
- The pulmonary capillary pressure is usually 1–2 mm Hg higher than the left atrial pressure.
Easy Concept
Left Atrial Pressure Increases
│
▼
Pulmonary Capillary Pressure
Also Increases
(1–2 mm Hg Higher)
│
▼
Higher Chance of
Pulmonary EdemaConcept:
- Higher left atrial pressure → Higher pulmonary capillary pressure.
- Higher pulmonary capillary pressure → Greater risk of pulmonary edema.
Critical Pressure for Pulmonary Edema
Step-by-Step Understanding
Step 1
Left Atrial Pressure = 23 mm Hg
↓
Step 2
Pulmonary Capillary Pressure = 25 mm Hg
(About 1–2 mm Hg higher)
↓
Step 3
Fluid Begins to Accumulate in the Lungs
↓
Step 4
Further Increase in Capillary Pressure
↓
Pulmonary Edema Develops More Rapidly
Easy Concept
Left Atrial Pressure
23 mm Hg
│
▼
Pulmonary Capillary Pressure
25 mm Hg
│
▼
Fluid Starts Entering
the Lungs
│
▼
Pulmonary Edema BeginsConcept:
- 25 mm Hg is the critical pulmonary capillary pressure in these experiments.
- Above this level, fluid begins to leak into the lungs.
Role of Plasma Colloid Osmotic Pressure
- During these experiments, the plasma colloid osmotic pressure was 25 mm Hg.
- This value was equal to the critical pulmonary capillary pressure at which pulmonary edema began.
Easy Concept
Pulmonary Capillary Pressure
25 mm Hg
=
Plasma Colloid Osmotic Pressure
25 mm Hg
│
▼
Pulmonary Edema BeginsConcept:
Pulmonary Edema Safety Factor
- In a normal person, the plasma colloid osmotic pressure is about 28 mm Hg.
- The normal pulmonary capillary pressure is about 7 mm Hg.
- Therefore, the pulmonary capillary pressure must rise above 28 mm Hg before significant pulmonary edema develops.
Step-by-Step Calculation
Step 1
Normal Pulmonary Capillary Pressure = 7 mm Hg
↓
Step 2
Critical Pressure Needed for Pulmonary Edema = 28 mm Hg
↓
Step 3
Formula
Safety Factor
= Critical Pulmonary Capillary Pressure
− Normal Pulmonary Capillary PressureSubstitute the Values
= 28 − 7Solve
= 21 mm HgFinal Answer
Pulmonary Edema Safety Factor = 21 mm Hg
Easy Concept
Normal Pulmonary
Capillary Pressure
7 mm Hg
│
▼
Must Rise Above
28 mm Hg
│
▼
Difference
28 − 7
= 21 mm Hg
↓
Pulmonary Edema
Safety FactorConcept:
- The lungs can tolerate a 21 mm Hg increase in pulmonary capillary pressure before significant pulmonary edema develops.
Easy Memory Trick
Normal Pressure
7 mm Hg
↓
Critical Pressure
28 mm Hg
↓
Safety Margin
21 mm HgRemember:
7 → 28 → 21
(Normal → Critical → Safety Factor)
Key Concept
- Fig. 39.8 shows that higher left atrial pressure increases the rate of pulmonary edema formation.
- Pulmonary capillary pressure is usually 1–2 mm Hg higher than left atrial pressure.
- In the experiments:
- Left atrial pressure >23 mm Hg
- Pulmonary capillary pressure >25 mm Hg
- Fluid began to accumulate in the lungs.
- As pulmonary capillary pressure increased further, pulmonary edema developed more rapidly.
- The critical pulmonary capillary pressure was equal to the plasma colloid osmotic pressure (25 mm Hg) in these experiments.
- In a normal person:
- Normal pulmonary capillary pressure = 7 mm Hg
- Normal plasma colloid osmotic pressure = 28 mm Hg
- Safety Factor = 28 − 7 = 21 mm Hg.
- This 21 mm Hg safety factor protects the lungs from developing significant pulmonary edema under normal conditions.
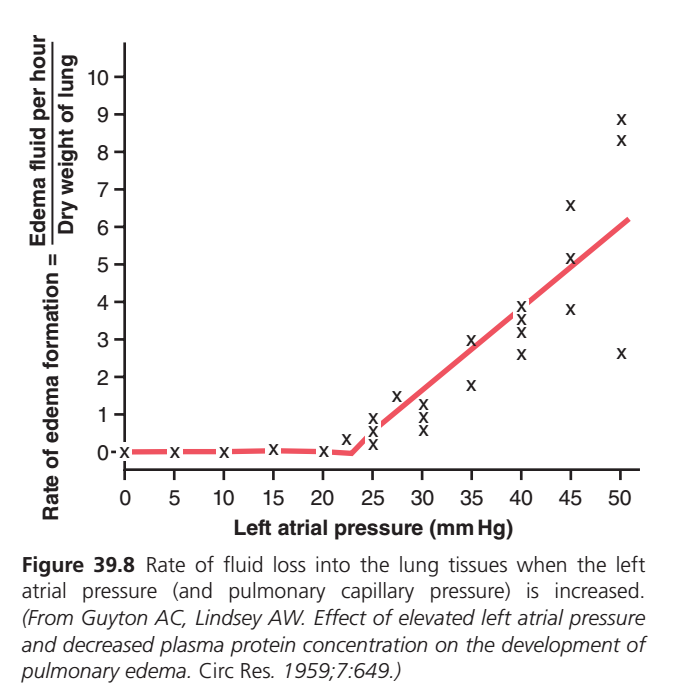
Figure 39.8: Effect of Left Atrial Pressure on Pulmonary Edema Formation (Guyton Physiology 15th Edition)
🎯 One-Line Core Concept
The lungs can tolerate an increase in left atrial pressure up to about 25 mmHg without significant pulmonary edema. Beyond this point, fluid rapidly leaks into the lungs, and pulmonary edema develops.
🧠 First Understand the Big Picture
Imagine your lungs are like a sponge.
Normally,
only a few drops of water enter the sponge.
The sponge stays almost dry because:
- Lymphatic vessels continuously remove the fluid.
- The alveoli remain dry.
Now imagine someone increases the pressure inside the water pipe.
More water begins leaking.
Initially, the drain (lymphatics) removes it.
But eventually,
the drain cannot keep up.
The sponge becomes soaked.
➡ This is pulmonary edema.
This graph shows exactly when that happens.
Step 1: Understanding the Axes
Y-axis (Vertical)
Rate of Edema Formation
(Edema fluid per hour per dry weight of lung)
This tells us
How fast fluid is accumulating inside the lungs.
Higher on the graph
↓
More pulmonary edema
Lower on the graph
↓
Little or no edema
X-axis (Horizontal)
Left Atrial Pressure (mmHg)
This tells us
Pressure inside the left atrium.
Normally,
Left atrial pressure is only about
2 mmHg
In disease,
it can increase to
- 20 mmHg
- 30 mmHg
- 40 mmHg
- 50 mmHg
What Is Left Atrial Pressure?
The left atrium receives blood from the lungs.
If pressure inside the left atrium increases,
blood cannot leave the lungs easily.
It begins backing up.
Pulmonary Capillary
↓
Pulmonary Vein
↓
Left AtriumIf the left atrium becomes crowded,
blood accumulates behind it.
This increases pulmonary capillary pressure.
More fluid leaks out.
Understanding the Red Line
The red line is the average trend.
It shows
How pulmonary edema increases as left atrial pressure increases.
Now let’s understand every part.
PART 1 — Flat Portion (0–24 mmHg)
Look at the beginning.
The red line is almost flat.
What does this mean?
Even though left atrial pressure is increasing,
almost no pulmonary edema forms.
Why?
Because the lungs have powerful safety mechanisms.
They include:
✅ Increased lymphatic drainage
✅ Low pulmonary capillary pressure
✅ Strong plasma proteins pulling fluid back
These mechanisms remove the tiny amount of leaked fluid.
Easy Memory
Pressure ↑
↓
Lymphatics work harder
↓
Lungs stay dryWhy Is This Called the Safety Factor?
The lungs can tolerate a fairly large rise in pressure
without becoming waterlogged.
This protective ability is called the
Pulmonary Edema Safety Factor
PART 2 — Around 25 mmHg
Look carefully.
Around
25 mmHg
the red line suddenly bends upward.
This is the critical point.
Why?
Now pulmonary capillary hydrostatic pressure becomes high enough that
large amounts of fluid leave the capillaries.
The lymphatics cannot remove all of it.
Fluid starts accumulating.
Pulmonary edema begins.
Easy Memory
25 mmHg = Danger Zone
Above this pressure,
pulmonary edema develops rapidly.
PART 3 — Steep Upward Line
Now look at the red line after
25 mmHg.
It rises almost straight upward.hat does this mean?
Every small increase in left atrial pressure now produces
a large increase in edema.
Example
25 mmHg
↓
Small edema
35 mmHg
↓
Much more edema
45 mmHg
↓
Severe edema
50 mmHg
↓
Massive pulmonary edema
Why?
The lymphatic system has reached its maximum capacity.
Now
every extra drop of filtered fluid remains inside the lung.Understanding the “X” Marks
Many students ask
“What are these X’s?”
These are individual experimental observations.
Each X represents
One measurement obtained from an experiment or one tested subject.
Researchers measured:
- Left atrial pressure
- Rate of pulmonary edema
for many experiments.
Each measurement is plotted as one X.
Why Are the X’s Not Exactly on the Red Line?
Biological systems are not identical.
Different animals or individuals have:
- Slightly different lymphatic drainage.
- Different plasma protein levels.
- Different pulmonary vascular resistance.
- Different measurement variability.
Therefore,
not every point is exactly the same.
The Red Line
The red line simply shows
the average trend through all the X’s.
Think of it as the “best-fit” line.
Example
Suppose five students score:
70
72
74
75
78Average = 74
The average represents the group,
even though no student scored exactly 74.
The red line works the same way.
Why Does Pulmonary Edema Occur?
Let’s follow the sequence.
Left Heart Failure
↓
↑ Left Atrial Pressure
↓
↑ Pulmonary Venous Pressure
↓
↑ Pulmonary Capillary Pressure
↓
Fluid leaks into interstitium
↓
Lymphatics become overloaded
↓
Fluid enters alveoli
↓
Pulmonary EdemaWhat Happens Inside the Lung?
Initially
Capillary
│
Small leak
│
Lymphatics remove fluidLater
Capillary
│
Large leak
│
Lymphatics overloaded
│
Fluid accumulates
│
Alveoli fill with waterClinical Importance
This graph explains why patients with:
- Left ventricular failure
- Mitral stenosis
- Severe hypertension
- Cardiomyopathy
develop
- Shortness of breath
- Orthopnea
- Pulmonary edema
Because
left atrial pressure rises,
fluid backs up into the lungs.
Easy Story to Remember
Imagine a sink with a drain.
- Water entering = Fluid leaking from pulmonary capillaries.
- Drain = Lymphatic vessels.
Normal Situation
The tap is opened slightly.
The drain removes all the water.
The sink stays empty.
Pressure Increases
The tap is opened more and more.
The drain works harder.
Still,
the sink remains almost empty.
Critical Point (~25 mmHg)
Now the tap is fully opened.
The drain cannot keep up.
Water begins collecting.
Soon,
the sink overflows.
➡ This overflowing sink is pulmonary edema.
Easy Flowchart
↑ Left Atrial Pressure
↓
↑ Pulmonary Capillary Pressure
↓
↑ Fluid Filtration
↓
Lymphatics Compensate (up to ~25 mmHg)
↓
Safety Factor Protects Lung
↓
Beyond ~25 mmHg
↓
Lymphatics Fail
↓
Rapid Pulmonary Edema📚 High-Yield MBBS Points
Normal Phase (0–24 mmHg)
- Very little or no pulmonary edema develops.
- Pulmonary lymphatics effectively remove filtered fluid.
- This protective ability is called the pulmonary edema safety factor.
Critical Threshold (~25 mmHg)
- Pulmonary capillary hydrostatic pressure becomes high enough to overwhelm lymphatic drainage.
- Pulmonary edema begins to develop.
Above 25 mmHg
- Small increases in left atrial pressure produce large increases in edema formation.
- Fluid accumulates in the lung interstitium and then floods the alveoli, severely impairing gas exchange.
Understanding the “X” Symbols
- Each X represents an individual experimental measurement of edema formation at a specific left atrial pressure.
- The red line represents the overall average (best-fit) relationship through all these measurements.
⭐ MBBS Viva Pearls
- Normal left atrial pressure: ~2 mmHg
- Mean pulmonary capillary pressure: ~7 mmHg
- Critical left atrial pressure for pulmonary edema: ≈25 mmHg
- Safety factor: The lungs can increase lymphatic drainage and limit edema formation until left atrial pressure reaches about 25 mmHg.
- Common causes of elevated left atrial pressure: Left ventricular failure, mitral valve disease (especially mitral stenosis), severe systemic hypertension, and cardiomyopathy.
Pulmonary Edema Safety Factor in Chronic Conditions
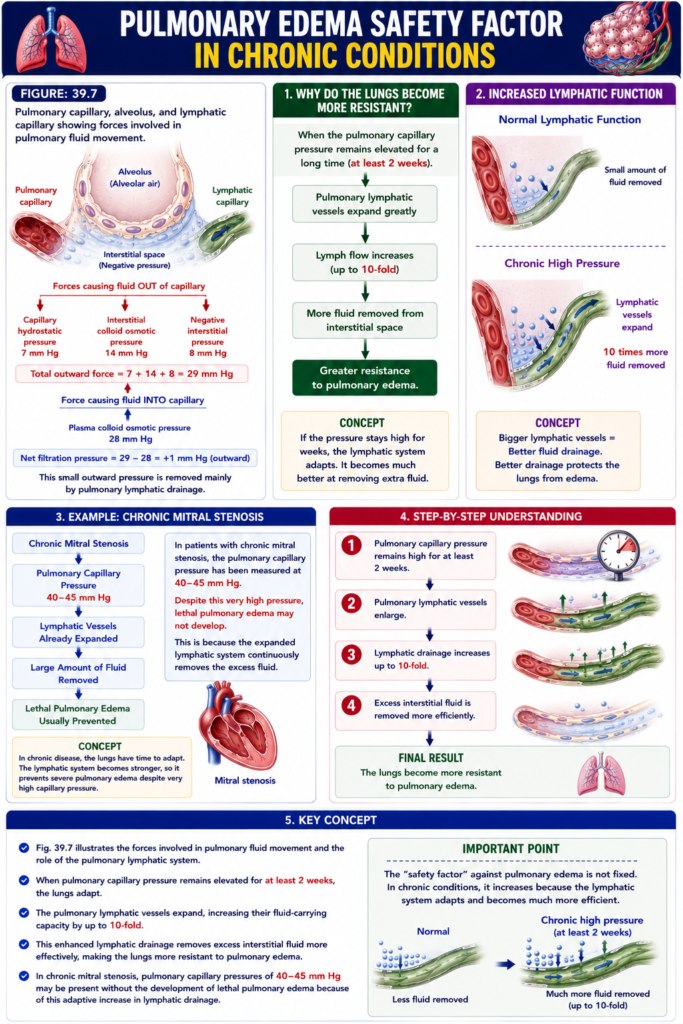
Figure: Fig. 39.7
- When the pulmonary capillary pressure remains elevated for a long time (at least 2 weeks), the lungs become more resistant to pulmonary edema.
Why Do the Lungs Become More Resistant?
- The pulmonary lymphatic vessels expand greatly.
- As they expand, their ability to remove fluid from the pulmonary interstitial spaces increases.
- The lymphatic system may increase its fluid-carrying capacity by as much as 10-fold.
Easy Concept
Chronic Increase in
Pulmonary Capillary Pressure
(At Least 2 Weeks)
│
▼
Pulmonary Lymphatic
Vessels Expand
│
▼
Lymph Flow Increases
Up to 10-Fold
│
▼
More Fluid Removed
from Interstitial Space
│
▼
Greater Resistance
to Pulmonary EdemaConcept:
- If the pressure stays high for weeks, the lymphatic system adapts.
- It becomes much better at removing extra fluid.
Increased Lymphatic Function
- The expanded lymphatic vessels remove much more interstitial fluid.
- This reduces fluid accumulation in the lungs.
- Therefore, the lungs can tolerate higher pulmonary capillary pressures without developing severe pulmonary edema.
Easy Concept
Normal Lymphatic Function
│
▼
Small Amount of
Fluid RemovedChronic High Pressure
│
▼
Lymphatic Vessels Expand
│
▼
10 Times More
Fluid RemovedConcept:
- Bigger lymphatic vessels = Better fluid drainage.
- Better drainage protects the lungs from edema.
Example: Chronic Mitral Stenosis
- In patients with chronic mitral stenosis, the pulmonary capillary pressure has been measured at 40–45 mm Hg.
- Despite this very high pressure, lethal pulmonary edema may not develop.
- This is because the expanded lymphatic system continuously removes the excess fluid.
Easy Concept
Chronic Mitral Stenosis
│
▼
Pulmonary Capillary Pressure
40–45 mm Hg
│
▼
Lymphatic Vessels
Already Expanded
│
▼
Large Amount of Fluid
Removed
│
▼
Lethal Pulmonary Edema
Usually PreventedConcept:
- In chronic disease, the lungs have time to adapt.
- The lymphatic system becomes stronger, so it prevents severe pulmonary edema despite very high capillary pressure.
Step-by-Step Understanding
Step 1
Pulmonary capillary pressure remains high for at least 2 weeks.
↓
Step 2
Pulmonary lymphatic vessels enlarge.
↓
Step 3
Lymphatic drainage increases up to 10-fold.
↓
Step 4
Excess interstitial fluid is removed more efficiently.
↓
Final Result
The lungs become more resistant to pulmonary edema.
Key Concept
- Fig. 39.7 illustrates the forces involved in pulmonary fluid movement and the role of the pulmonary lymphatic system.
- When pulmonary capillary pressure remains elevated for at least 2 weeks, the lungs adapt.
- The pulmonary lymphatic vessels expand, increasing their fluid-carrying capacity by up to 10-fold.
- This enhanced lymphatic drainage removes excess interstitial fluid more effectively, making the lungs more resistant to pulmonary edema.
- In chronic mitral stenosis, pulmonary capillary pressures of 40–45 mm Hg may be present without the development of lethal pulmonary edema because of this adaptive increase in lymphatic drainage.
Rapidity of Death in Persons With Acute Pulmonary Edema
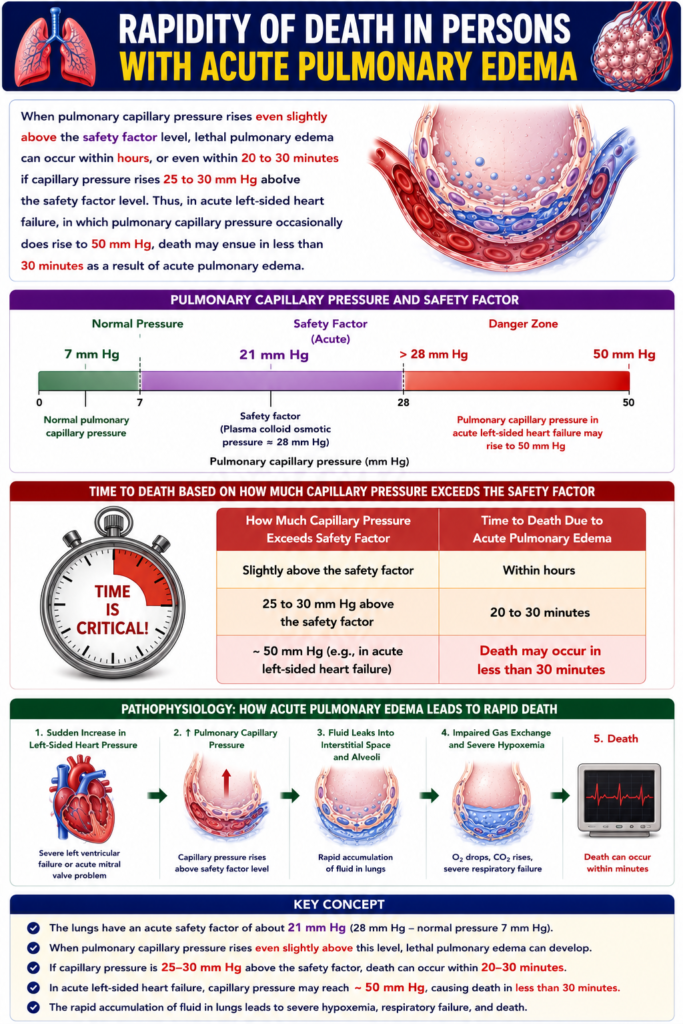
- When the pulmonary capillary pressure rises even slightly above the pulmonary edema safety factor, acute pulmonary edema can develop.
- Lethal pulmonary edema may occur within a few hours.
- If the pulmonary capillary pressure rises 25–30 mm Hg above the safety factor level, death may occur within 20–30 minutes.
Acute Left-Sided Heart Failure
- In acute left-sided heart failure, the pulmonary capillary pressure may rise to about 50 mm Hg.
- At this very high pressure, acute pulmonary edema develops rapidly.
- As a result, death may occur in less than 30 minutes.
Easy Concept
Acute Left-Sided
Heart Failure
│
▼
Pulmonary Capillary
Pressure Rises
(≈50 mm Hg)
│
▼
Massive Fluid Leakage
from Capillaries
│
▼
Alveoli Fill with Fluid
│
▼
Acute Pulmonary Edema
│
▼
Severe Impairment
of Gas Exchange
│
▼
Death May Occur
in Less Than
30 MinutesConcept:
- In acute left-sided heart failure, pulmonary capillary pressure rises suddenly.
- This causes rapid fluid leakage into the alveoli.
- The alveoli fill with fluid, making oxygen exchange extremely difficult.
- Therefore, acute pulmonary edema can become fatal very quickly.
Effect of Increasing Pulmonary Capillary Pressure
Pulmonary Capillary Pressure
Slightly Above
Safety Factor
│
▼
Pulmonary Edema
Develops Within HoursPulmonary Capillary Pressure
25–30 mm Hg Above
Safety Factor
│
▼
Massive Pulmonary Edema
│
▼
Death May Occur
Within 20–30 MinutesConcept:
- A small increase above the safety factor can produce pulmonary edema over hours.
- A much larger increase (25–30 mm Hg above the safety factor) causes very rapid pulmonary edema, which can become fatal within 20–30 minutes.
Step-by-Step Understanding
Step 1
Pulmonary capillary pressure rises above the safety factor.
↓
Step 2
Fluid leaks rapidly from the pulmonary capillaries.
↓
Step 3
Interstitial spaces and alveoli fill with fluid.
↓
Step 4
Gas exchange becomes severely impaired.
↓
Final Result
Acute pulmonary edema develops, and death may occur rapidly if the pressure continues to rise.Key Concept
- When pulmonary capillary pressure rises above the pulmonary edema safety factor, acute pulmonary edema can develop.
- Lethal pulmonary edema may occur within hours.
- If the pulmonary capillary pressure rises 25–30 mm Hg above the safety factor level, death may occur within 20–30 minutes.
- In acute left-sided heart failure, the pulmonary capillary pressure may rise to about 50 mm Hg, causing rapid fluid accumulation in the alveoli.
- Acute pulmonary edema may then lead to death in less than 30 minutes.
FLUID IN THE PLEURAL CAVITY
Figure: Fig. 39.9
- During normal breathing, the lungs continuously expand and contract.
- As the lungs move, they slide back and forth inside the pleural cavity.
- To make this movement smooth, a thin layer of mucoid fluid is present between the parietal pleura and the visceral pleura.
Pleural Fluid Formation
- Fig. 39.9 shows the movement of fluid in the pleural space.
- The pleural membrane is a porous, mesenchymal, serous membrane.
- Small amounts of interstitial fluid continuously pass (transude) through the pleural membrane into the pleural space.
- This fluid carries tissue proteins with it.
- Because of these proteins, the pleural fluid becomes mucoid.
- The mucoid pleural fluid allows the lungs to slide very easily during breathing.
Easy Concept
Parietal Pleura
│
▼
Small Amount of
Pleural Fluid
│
▼
Visceral Pleura
│
▼
Lungs Slide Smoothly
During BreathingConcept:
- The thin mucoid fluid acts like a lubricant.
- It reduces friction between the two pleural layers.
Normal Amount of Pleural Fluid
- Each pleural cavity normally contains only a few milliliters of pleural fluid.
Easy Concept
Pleural Cavity
│
▼
Only a Few mL
of Pleural Fluid
│
▼
Normal Smooth
Lung MovementConcept:
- Only a very small amount of pleural fluid is needed for normal lung movement.
Removal of Excess Pleural Fluid
- If the amount of pleural fluid becomes greater than normal, the excess fluid is removed by lymphatic vessels.
- These lymphatic vessels open directly into the pleural cavity.
The lymphatics drain the excess fluid into:
- The mediastinum
- The superior surface of the diaphragm
- The lateral surfaces of the parietal pleura
Easy Concept
Excess Pleural Fluid
│
▼
Lymphatic Vessels
│
├────────► Mediastinum
│
├────────► Superior Surface
│ of Diaphragm
│
└────────► Lateral Surface
of Parietal PleuraConcept:
- The lymphatic system continuously removes extra pleural fluid.
- This prevents fluid accumulation in the pleural cavity.
Pleural Space
- The pleural space is the space between the parietal pleura and the visceral pleura.
- Normally, this space is extremely narrow.
- Therefore, it is called a potential space.
- It is called a potential space because it normally is not an obvious physical space.
Easy Concept
Parietal Pleura
│
Thin Layer of
Pleural Fluid
│
Visceral PleuraConcept:
- Normally, the two pleural layers are almost touching.
- Only a thin film of pleural fluid separates them.
- Therefore, the pleural space is called a potential space.
Step-by-Step Understanding
Step 1
Lungs expand and contract during breathing.
↓
Step 2
A thin layer of mucoid pleural fluid reduces friction.
↓
Step 3
Small amounts of interstitial fluid continuously enter the pleural cavity.
↓
Step 4
If excess pleural fluid accumulates, lymphatic vessels remove it.
↓
Final Result
The pleural cavity remains a narrow potential space, allowing smooth lung movement during breathing.
Key Concept
- Fig. 39.9 shows the dynamics of pleural fluid exchange.
- During breathing, the lungs slide within the pleural cavity.
- A thin layer of mucoid pleural fluid between the parietal and visceral pleurae reduces friction.
- The pleural membrane continuously allows small amounts of interstitial fluid and tissue proteins to enter the pleural space, producing mucoid pleural fluid.
- Each pleural cavity normally contains only a few milliliters of fluid.
- Excess pleural fluid is removed by lymphatic vessels draining into:
- The mediastinum
- The superior surface of the diaphragm
- The lateral surfaces of the parietal pleura
- The pleural space is called a potential space because it is normally extremely narrow and not an obvious physical space.
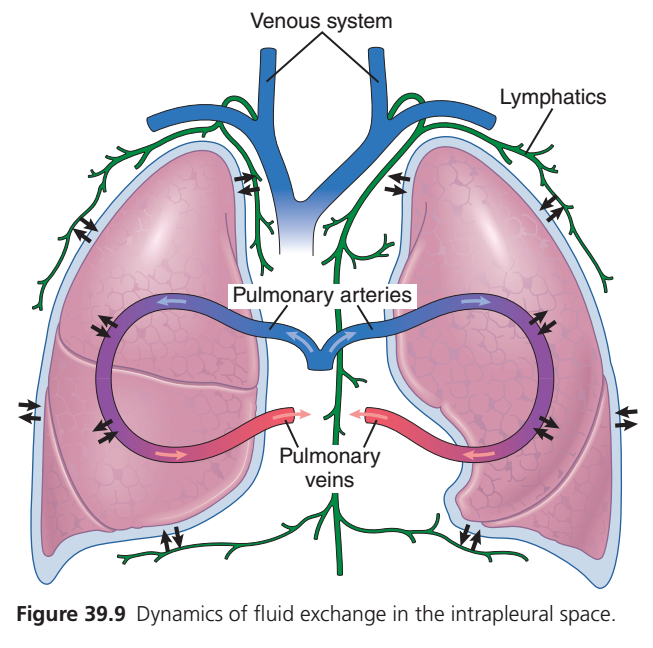
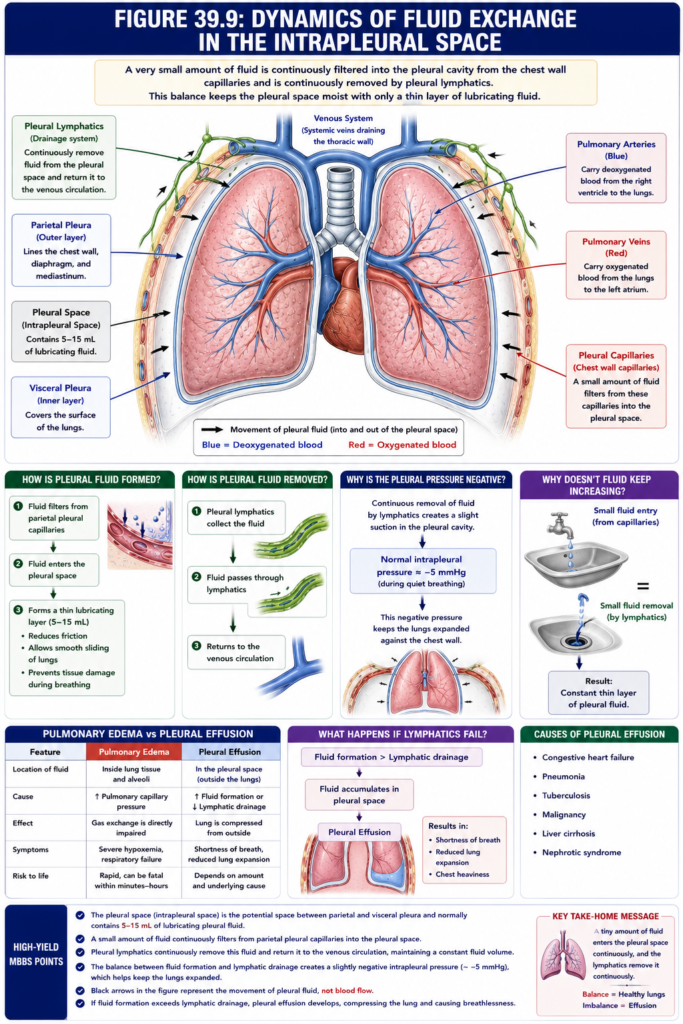
Figure 39.9: Dynamics of Fluid Exchange in the Intrapleural Space (Guyton Physiology 15th Edition)
🎯 One-Line Core Concept
A very small amount of fluid is continuously filtered into the pleural cavity from the chest wall capillaries and is continuously removed by pleural lymphatics. This balance keeps the pleural space moist with only a thin layer of lubricating fluid.
🧠 First Understand the Big Picture
Imagine your lungs are inside a plastic bag.
The lung is not directly attached to the chest wall.
Instead,
there is a very thin space between them called the
Pleural Space (Intrapleural Space)
Chest Wall
│
Parietal Pleura
│
Pleural Space
│
Visceral Pleura
│
LungThis space contains only
5–15 mL of pleural fluid.
This tiny amount acts like
Lubricating oil between two moving surfaces.
It allows the lungs to slide smoothly during breathing.
Let’s Understand Every Part of the Figure
Step 1 — The Pink Structures
These are the
Lungs
Both lungs are shown.
They expand and contract during breathing.
Step 2 — Blue Outer Border
This thin blue line represents the
Pleura
Remember,
the pleura has two layers.
Outer Layer
Parietal Pleura
Attached to:
- Chest wall
- Diaphragm
- Mediastinum
Inner Layer
Visceral Pleura
Attached directly to the lung surface.
Between them lies
Pleural Space
Step 3 — Green Network
The green vessels are
Lymphatics
These are the drainage system of the pleural cavity.
Think of them as
🧹 The cleaning system
or
🚰 The drainage pipes
Their Job
Whenever fluid enters the pleural cavity,
the lymphatics immediately remove it.
Without lymphatics,
fluid would accumulate around the lungs.
Step 4 — Black Arrows
The black arrows are extremely important.
Many students think they represent blood flow.
❌ They do not.
They represent
Movement of Pleural Fluid
Notice
Some arrows point
➡ Into the pleural space.
Others point
➡ Toward the lymphatics.
This shows
Fluid is
continuously
entering
and
leaving
the pleural cavity.
Step 5 — Pulmonary Arteries (Blue)
These large blue vessels are
Pulmonary Arteries
They carry
Deoxygenated blood
from the
Right Ventricle
↓
to the lungs.
Direction of Blood
Right Heart
↓
Pulmonary Artery
↓
LungsStep 6 — Pulmonary Veins (Red)
These vessels return
Oxygenated blood
back to the heart.
Lungs
↓
Pulmonary Veins
↓
Left AtriumStep 7 — Venous System
At the top,
the blue vessels are labeled
Venous System
These represent the
Systemic veins draining the thoracic wall.
They are important because
fluid entering the pleural space eventually returns to the bloodstream through the lymphatic system and venous circulation.
How Is Pleural Fluid Formed?
Now let’s understand the actual physiology.
Step 1
Tiny amounts of fluid filter from
Parietal Pleural Capillaries
↓
into
↓
Pleural Space
Why?
Because capillary hydrostatic pressure pushes a small amount of plasma outward.
Exactly like filtration in other capillaries.
Step 2
The pleural space now contains
a thin lubricating layer of fluid.
This fluid
Step 3
The lymphatics continuously remove this fluid.
The amount entering
≈
The amount leaving.
Therefore,
fluid never accumulates.
Easy Flowchart
Pleural Capillaries
↓
Small Fluid Filtration
↓
Pleural Space
↓
Lubrication
↓
Pleural Lymphatics
↓
Venous CirculationWhy Doesn’t Fluid Keep Increasing?
Imagine a kitchen sink.
The tap is slightly open.
Water enters continuously.
But the drain removes water at exactly the same rate.
Therefore,
the sink never overflows.
The pleural cavity works exactly like this.
Small Fluid Entry
=
Small Fluid RemovalResult
↓
Constant thin layer of pleural fluid.
Why Is Pleural Fluid Important?
Without pleural fluid,
every breath would cause
Lung rubbing against chest wall.
Imagine rubbing
Two dry glass plates together.
Very difficult.
Now add one drop of oil.
They slide easily.
Pleural fluid acts exactly like that oil.
Why Is the Pleural Pressure Negative?
The lymphatics continuously remove fluid.
This creates
a slight suction inside the pleural cavity.
Therefore,
Normal intrapleural pressure is about
−5 mmHg
during quiet breathing.
This negative pressure helps keep the lungs expanded against the chest wall.
Clinical Importance
What Happens if Lymphatics Fail?
Suppose lymphatic drainage becomes blocked.
Fluid continues entering
↓
but cannot leave.
Fluid accumulates.
↓
Pleural Effusion
The lungs become compressed.
The patient develops
- Shortness of breath
- Reduced lung expansion
- Chest heaviness
Causes of Pleural Effusion
Common causes include:
- Congestive heart failure
- Pneumonia
- Tuberculosis
- Malignancy
- Liver cirrhosis
- Nephrotic syndrome
Difference Between Pulmonary Edema and Pleural Effusion
| Pulmonary Edema | Pleural Effusion |
|---|---|
| Fluid inside lung tissue and alveoli | Fluid in the pleural space |
| Gas exchange is directly impaired | Lung is compressed from outside |
| Usually due to increased pulmonary capillary pressure | Usually due to excess pleural fluid formation or reduced lymphatic drainage |
Easy Story to Remember
Imagine your lungs are two balloons inside a thin plastic bag.
Between the balloon and the bag is
a tiny amount of oil.
Every second,
a few drops of oil leak in.
At the same time,
a small drain removes the same amount.
As long as the drain works,
the balloons move smoothly.
If the drain becomes blocked,
oil fills the bag and squeezes the balloons.
That squeezing is exactly what happens in pleural effusion.
High-Yield MBBS Points
- The pleural space is the potential space between the parietal and visceral pleura and normally contains 5–15 mL of lubricating pleural fluid.
- A small amount of fluid continuously filters from the parietal pleural capillaries into the pleural space.
- Pleural lymphatics continuously remove this fluid and return it to the venous circulation, maintaining a constant fluid volume.
- The balance between fluid formation and lymphatic drainage creates a slightly negative intrapleural pressure (~−5 mmHg), which helps keep the lungs expanded.
- Black arrows in the figure represent the movement of pleural fluid, not blood flow.
- If fluid formation exceeds lymphatic drainage, pleural effusion develops, compressing the lung and causing breathlessness.
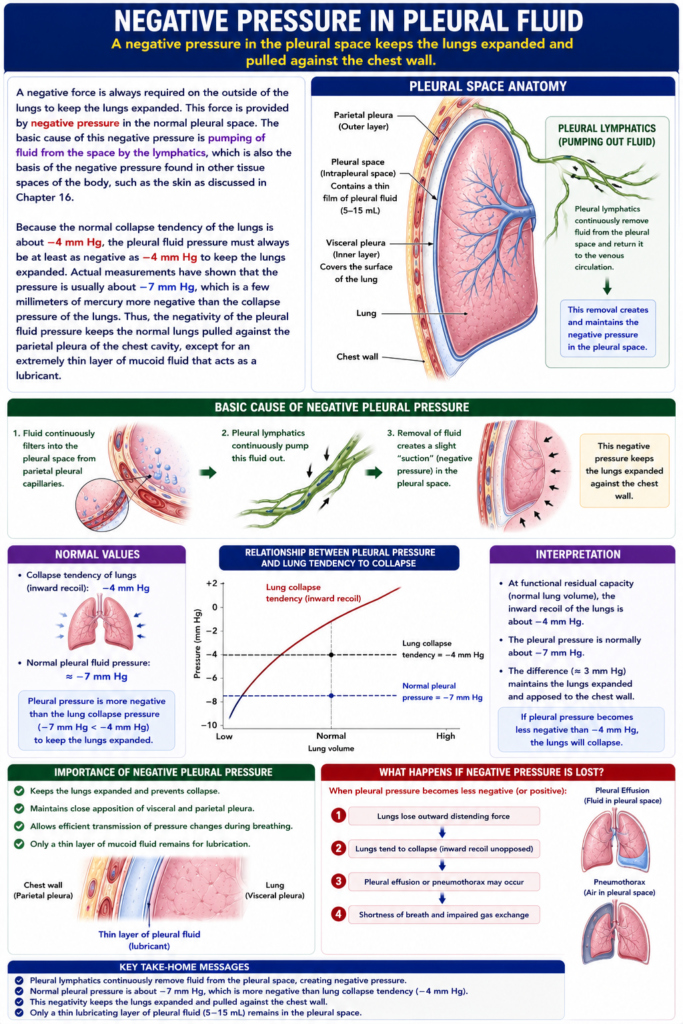
Negative Pressure in Pleural Fluid
- A negative pressure is always required outside the lungs to keep the lungs expanded.
- This force is provided by the negative pressure in the normal pleural space.
Cause of Negative Pleural Pressure
- The basic cause of negative pleural pressure is the continuous pumping of pleural fluid by the lymphatic vessels.
- The same mechanism also produces negative pressure in other tissue spaces of the body, such as the skin.
Easy Concept
Pleural Space
│
▼
Lymphatics Continuously
Remove Pleural Fluid
│
▼
Negative Pleural Pressure
Develops
│
▼
Lungs Remain ExpandedConcept:
- The lymphatic vessels continuously remove pleural fluid.
- This creates a negative pressure (suction) in the pleural cavity.
- This negative pressure keeps the lungs expanded.
Normal Collapse Tendency of the Lungs
- The lungs naturally tend to collapse.
- The normal collapse tendency of the lungs is about −4 mm Hg.
Easy Concept
Lungs Naturally
Want to Collapse
│
Collapse Force
≈ −4 mm HgConcept:
- The lungs have a natural inward elastic recoil.
- Therefore, an equal or greater negative pressure outside the lungs is needed to keep them open.
Required Pleural Pressure
- The pleural fluid pressure must be at least −4 mm Hg to prevent lung collapse.
- Actual measurements show that the normal pleural fluid pressure is about −7 mm Hg.
- This is a few mm Hg more negative than the lung collapse pressure.
Step-by-Step Understanding
Step 1
Normal lung collapse tendency = −4 mm Hg
↓
Step 2
Pleural pressure must be at least −4 mm Hg
↓
Step 3
Actual pleural pressure ≈ −7 mm Hg
↓
Final Result
The lungs remain fully expanded.
Easy Concept
Normal Lung
Collapse Force
−4 mm Hg
│
▼
Pleural Pressure
−7 mm Hg
(More Negative)
│
▼
Lungs Stay ExpandedConcept:
- Because −7 mm Hg is more negative than −4 mm Hg, it provides enough suction to keep the lungs expanded.
Effect of Negative Pleural Pressure
- The negative pleural pressure pulls the lungs outward.
- It keeps the lungs closely attached to the parietal pleura of the chest wall.
- Only an extremely thin layer of mucoid pleural fluid remains between the visceral pleura and the parietal pleura.
- This thin fluid layer acts as a lubricant, allowing smooth lung movement during breathing.
Easy Concept
Chest Wall
(Parietal Pleura)
│
▼
Negative Pleural Pressure
(−7 mm Hg)
│
▼
Lungs Pulled Outward
│
▼
Very Thin Layer
of Mucoid Fluid
│
▼
Smooth Sliding During
BreathingConcept:
- The negative pressure keeps the lungs attached to the chest wall.
- The thin pleural fluid layer reduces friction, allowing the lungs to slide smoothly during inspiration and expiration.
Step-by-Step Understanding
Step 1
Lymphatics continuously remove pleural fluid.
↓
Step 2
Negative pleural pressure develops.
↓
Step 3
Negative pressure (≈ −7 mm Hg) is greater than the lung collapse tendency (−4 mm Hg).
↓
Step 4
The lungs remain expanded and attached to the chest wall.
↓
Step 5
A thin layer of mucoid pleural fluid allows smooth movement during breathing.
Key Concept
- A negative pressure outside the lungs is essential to keep the lungs expanded.
- This negative pleural pressure is produced by the continuous removal of pleural fluid by the lymphatic vessels.
- The lungs normally tend to collapse with a force of about −4 mm Hg.
- Therefore, the pleural pressure must be at least −4 mm Hg to prevent lung collapse.
- The normal pleural pressure is about −7 mm Hg, which is more negative than the collapse tendency, keeping the lungs expanded and attached to the chest wall.
- Only a thin layer of mucoid pleural fluid remains between the pleural layers, acting as a lubricant for smooth lung movement during breathing.
Pleural Effusion—Collection of Excess Free Fluid in the Pleural Space
Figure: Fig. 39.8 and Fig. 39.9
- Pleural effusion is the collection of excess free fluid in the pleural space.
- Pleural effusion is similar to edema in the body tissues.
- Therefore, pleural effusion can be called edema of the pleural cavity.
Causes of Pleural Effusion
- The causes of pleural effusion are the same as the causes of edema in other tissues.
1. Blockage of Lymphatic Drainage
- Blockage of lymphatic drainage from the pleural cavity prevents the removal of pleural fluid.
- As a result, fluid accumulates in the pleural space.
Easy Concept
Lymphatic Drainage Blocked
│
▼
Pleural Fluid
Cannot Be Removed
│
▼
Fluid Accumulates
│
▼
Pleural EffusionConcept:
- If the lymphatic drainage stops, fluid builds up in the pleural cavity.
2. Cardiac Failure
Easy Concept
Cardiac Failure
│
▼
↑ Peripheral &
Pulmonary Capillary Pressure
│
▼
More Fluid Leaves
Capillaries
│
▼
Fluid Enters
Pleural Cavity
│
▼
Pleural EffusionConcept:
3. Reduced Plasma Colloid Osmotic Pressure
- Greatly reduced plasma colloid osmotic pressure allows excessive transudation of fluid.
- As a result, fluid accumulates in the pleural cavity.
Easy Concept
↓ Plasma Colloid
Osmotic Pressure
│
▼
Less Fluid Pulled
Back Into Blood
│
▼
More Fluid Moves Into
Pleural Cavity
│
▼
Pleural EffusionConcept:
- When plasma colloid osmotic pressure decreases, more fluid leaves the blood vessels.
4. Infection or Inflammation
- Infection or any other cause of inflammation of the pleural cavity increases the permeability of the capillary membranes.
- The increased permeability allows rapid leakage of plasma proteins and fluid into the pleural cavity.
Easy Concept
Infection
OR
Inflammation
│
▼
Capillary Permeability
Increases
│
▼
Proteins and Fluid
Leak Into
Pleural Cavity
│
▼
Pleural EffusionConcept:Step-by-Step Understanding
Pathway 1
Lymphatic drainage blocked
↓
Pleural fluid cannot be removed
↓
Pleural effusion develops
Pathway 2
Cardiac failure
↓
↑ Peripheral & pulmonary capillary pressure
↓
Excess fluid enters the pleural cavity
↓
Pleural effusion develops
Pathway 3
↓ Plasma colloid osmotic pressure
↓
Excess fluid leaves the capillaries
↓
Pleural effusion develops
Pathway 4
Infection or inflammation
↓
Capillary permeability increases
↓
Proteins and fluid leak into the pleural cavity
↓
Pleural effusion develops
Key Concept
- Fig. 39.8 shows the relationship between left atrial pressure and pulmonary edema formation.
- Fig. 39.9 illustrates the dynamics of pleural fluid exchange.
- Pleural effusion is the accumulation of excess free fluid in the pleural space and is analogous to edema of the pleural cavity.
- The major causes of pleural effusion are:
- Blockage of lymphatic drainage from the pleural cavity
- Cardiac failure, causing high peripheral and pulmonary capillary pressures and excessive transudation of fluid
- Greatly reduced plasma colloid osmotic pressure, allowing excessive transudation of fluid
- Infection or inflammation of the pleural cavity, increasing capillary permeability and causing rapid leakage of plasma proteins and fluid into the pleural cavity.