

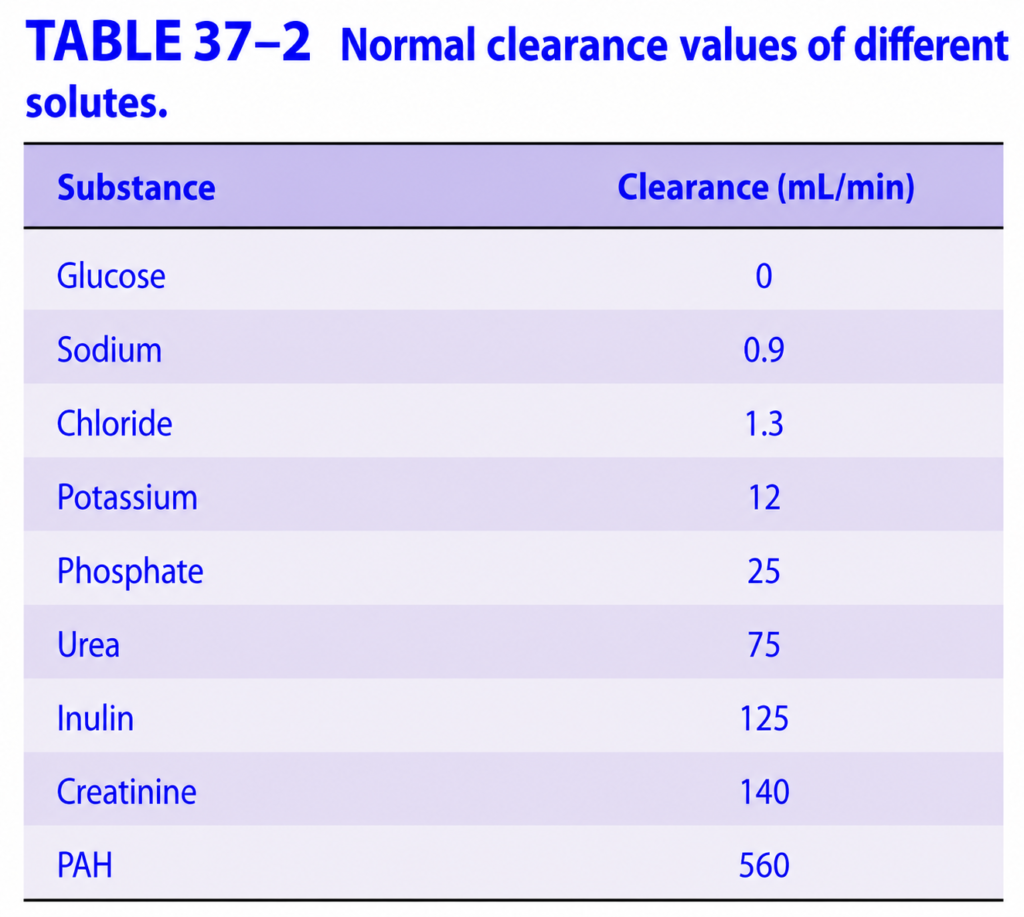
MEASURING GFR
- Glomerular Filtration Rate (GFR) is the amount of plasma ultrafiltrate formed by the kidneys each minute.
- GFR is measured by:
- Measuring the plasma concentration of a substance.
- Measuring the amount of that substance excreted in the urine.
- A substance used to measure GFR must have these properties:
- Freely filtered through the glomerulus.
- Not reabsorbed by the renal tubules.
- Not secreted by the renal tubules.
- Non-toxic.
- Not metabolized by the body.
- Inulin satisfies all of these requirements.
- Inulin is:
- A polymer of fructose.
- Has a molecular weight of about 5200.
- Therefore, inulin is the ideal substance for measuring GFR.
- Renal plasma clearance is the:
- Volume of plasma completely cleared of a substance by the kidneys per minute.
- Both GFR and clearance are expressed in mL/min.
- If the test substance is represented by X, then:
GFR (Clearance Formula)
GFR=CX=PXUX×V˙
Where:
- Uₓ = Concentration of substance X in urine
- V̇ = Urine flow rate (mL/min)
- Pₓ = Plasma concentration of substance X
- Cₓ = Clearance of substance X = GFR
Solving the Given Example
Given:
- Urine inulin concentration (UIN) = 35 mg/mL
- Urine flow (V̇) = 0.9 mL/min
- Plasma inulin concentration (PIN) = 0.25 mg/mL
Step 1
GFR=0.2535×0.9
Step 2
Multiply the numerator:35×0.9=31.5
Step 3
Divide by plasma concentration:0.2531.5=126
Final Answer
GFR=126 mL/min
Concept:
- The kidneys completely cleared 126 mL of plasma of inulin every minute.
- Therefore:
Inulin clearance = GFR
- In practice:
- A loading dose of inulin is given intravenously.
- This is followed by a continuous infusion to maintain a constant plasma concentration.
- After inulin is evenly distributed in body fluids:
- A timed urine sample is collected.
- A blood sample is taken during the urine collection.
- Plasma and urine inulin concentrations are measured.
- GFR is then calculated using the clearance formula.
- Creatinine clearance (CCr) can also be used to estimate GFR.
- However:
- A small amount of creatinine is secreted by the renal tubules.
- Therefore, creatinine clearance is slightly higher than true GFR.
- Despite this, endogenous creatinine clearance provides a good estimate of GFR because it closely matches the values obtained with inulin.
- In clinical practice:
- Plasma creatinine (PCr) is commonly used as an indicator of kidney function.
- Normal plasma creatinine ≈ 1 mg/dL.
Easy Concept
Think of GFR as the kidney’s filtering speed.
Blood enters Kidney
↓
Glomerulus filters plasma
↓
Inulin enters urine only
(No secretion, No reabsorption)
↓
Measure:
• Urine concentration
• Plasma concentration
• Urine flow
↓
Calculate GFREasy Formula Memory
Urine Concentration × Urine Flow
GFR = -----------------------------------------
Plasma ConcentrationOr simply:
GFR = U × V
-----
PEasy Memory Trick
Ideal GFR Marker
✔ Freely Filtered
✔ No Reabsorption
✔ No Secretion
✔ Non-toxic
✔ Not Metabolized
= INULINClinical Marker
Creatinine
↓
Easy to measure
↓
Slightly overestimates GFR
↓
Good clinical estimateKEY CONCEPT
- Glomerular Filtration Rate (GFR) is the volume of plasma filtered by the glomeruli each minute. The ideal marker is inulin because it is freely filtered and neither reabsorbed nor secreted. GFR is calculated as: GFR = (Urine concentration × Urine flow) ÷ Plasma concentration. In the given example, GFR = 126 mL/min. Although creatinine clearance slightly overestimates GFR due to tubular secretion, it is widely used clinically because it closely reflects true GFR.
NORMAL GFR
- The normal Glomerular Filtration Rate (GFR) in a healthy average adult is approximately 125 mL/min.
- GFR is related to body surface area.
- However, women have a GFR about 10% lower than men, even after correcting for body surface area.
- A GFR of 125 mL/min is equal to:
- 7.5 L/hour
- 180 L/day
- Although the kidneys filter about 180 L of fluid each day, the normal urine output is only about 1 L/day.
- This means that 99% or more of the filtered fluid is reabsorbed back into the blood.
- Only about 1% or less remains as urine.
- At a filtration rate of 125 mL/min, the kidneys filter in one day:
- About 4 times the total body water
- About 15 times the extracellular fluid (ECF) volume
- About 60 times the plasma volume
Easy Concept
Think of the kidneys as a high-speed water filter.
Blood
↓
Glomerulus filters
180 L/day
↓
Tubules reabsorb
179 L/day
↓
Only about 1 L/day
becomes urineEasy Numbers to Remember
Normal GFR
125 mL/min
↓
7.5 L/hour
↓
180 L/day180 L Filtered
↓
99% Reabsorbed
↓
≈1 L UrineEasy Memory Trick
Kidney Filters
180 L/day
BUT
Keeps 99%
Throws away only ~1%KEY CONCEPT
- The normal GFR is about 125 mL/min (7.5 L/hour or 180 L/day). Although the kidneys filter approximately 180 L of plasma each day, more than 99% of this filtrate is reabsorbed, producing only about 1 L of urine daily. In one day, the kidneys filter fluid equal to about 4 times the total body water, 15 times the extracellular fluid volume, and 60 times the plasma volume.
CONTROL OF GFR
- Glomerular Filtration Rate (GFR) is controlled by the same factors that control filtration in all body capillaries.
- These factors are:
- Size of the glomerular capillary bed
- Permeability of the glomerular capillaries
- Hydrostatic pressure across the capillary wall
- Osmotic (oncotic) pressure across the capillary wall
- For each nephron, GFR is calculated by the following equation:
GFR Equation
GFR=Kf[(PGC−PT)−(πGC−πT)]
Understanding the Equation Step by Step
Kf (Glomerular Ultrafiltration Coefficient)
- Kf represents the kidney’s filtering ability.
- It depends on:
- Hydraulic conductivity (permeability) of the glomerular capillary wall
- Effective filtration surface area
Easy Concept:
- Higher Kf = Better filtration = Higher GFR
- Lower Kf = Poor filtration = Lower GFR
PGC (Glomerular Capillary Hydrostatic Pressure)
- PGC is the blood pressure inside the glomerular capillaries.
- It pushes fluid out of the capillaries into Bowman’s space.
Effect on GFR
↑ PGC
↓
More filtration
↓
↑ GFRPT (Hydrostatic Pressure in Bowman’s Space)
- PT is the pressure of fluid already present in Bowman’s space.
- It pushes back against filtration.
Effect on GFR
↑ PT
↓
Less filtration
↓
↓ GFRπGC (Plasma Oncotic Pressure in Glomerular Capillaries)
- πGC is produced by plasma proteins.
- It pulls water back into the glomerular capillaries.
- Therefore, it opposes filtration.
Effect on GFR
↑ πGC
↓
More water pulled back
↓
↓ GFRπT (Oncotic Pressure in Bowman’s Space)
- πT is the oncotic pressure of the filtrate in Bowman’s space.
- It pulls water into Bowman’s space, helping filtration.
- Normally:
- Very little or no protein is filtered
- Therefore:
πT ≈ 0- So, under normal conditions, πT has almost no effect on GFR.
Solving the Equation Conceptually
Forces Helping Filtration
PGC
(Blood pressure in glomerulus)
↓
Forces Opposing Filtration
PT + πGC
↓
Net Filtration Pressure
↓
Multiply by Kf
↓
GFROr simply:
GFR
=
Filtering Ability (Kf)
×
(Pressure pushing fluid out)
−
(Pressure pushing/pulling fluid back)Easy Concept
Think of the glomerulus as a water filter.
Blood Pressure
(PGC)
↓
Pushes water OUT
✔ Helps filtrationBowman's Pressure
(PT)
↓
Pushes water BACK
✖ Reduces filtrationPlasma Proteins
(πGC)
↓
Pull water BACK
✖ Reduce filtrationFilter Quality
(Kf)
↓
Determines how easily water passesEasy Memory Trick
Things That Increase GFR
✔ ↑ Kf
✔ ↑ PGC
✔ ↑ Filtration Surface AreaThings That Decrease GFR
✔ ↑ PT
✔ ↑ πGC
✔ ↓ KfKEY CONCEPT
- GFR depends on the glomerular ultrafiltration coefficient (Kf) and the balance between forces that favor and oppose filtration. Glomerular capillary hydrostatic pressure (PGC) promotes filtration, whereas Bowman’s space hydrostatic pressure (PT) and plasma oncotic pressure (πGC) oppose filtration. Bowman’s space oncotic pressure (πT) is normally negligible because almost no protein enters the filtrate. Thus, GFR is determined by the kidney’s filtering capacity (Kf) and the net filtration pressure across the glomerular capillaries.
GFR Equation (SUPERFAST SOLVE )
The GFR equation simply means:
GFR depends on two things:
- How good the kidney filter is (Kf)
- The net pressure pushing fluid out of the glomerulus
Original Equation
GFR = Kf [(PGC − PT) − (πGC − πT)]
Step 1: Understand the Four Pressures
1. PGC = Glomerular Capillary Hydrostatic Pressure
- Blood pressure inside the glomerular capillaries.
- It pushes fluid out into Bowman’s space.
✅ Helps filtration
✅ Increases GFR
Blood Pressure
↓↓↓
Glomerulus
↓
Fluid pushed into Bowman's capsule2. PT = Bowman’s Space Hydrostatic Pressure
- Pressure of the fluid already present inside Bowman’s capsule.
- It pushes back against the incoming filtrate.
❌ Opposes filtration
❌ Decreases GFR
Bowman's Capsule
Fluid Pressure
↑↑
Pushes back3. πGC = Plasma Oncotic Pressure
- Produced by plasma proteins inside the glomerular capillaries.
- Proteins pull water back into the blood.
❌ Opposes filtration
❌ Decreases GFR
Proteins
↑
Pull water back
into blood4. πT = Bowman’s Space Oncotic Pressure
- Oncotic pressure in Bowman’s space.
- Normally almost zero because proteins are not filtered.
✔ Very little effect on GFR.
Normally
πT ≈ 0Step 2: Solve the Equation Conceptually
First solve the hydrostatic pressures:
(PGC − PT)
=
Pressure pushing OUT
−
Pressure pushing BACKExample:
PGC = 60
PT = 15
60 −15
=45 mmHgThis gives the net pushing force.
Now solve the oncotic pressures:
(πGC − πT)
=
Pressure pulling BACK
−
Pressure pulling OUTExample:
πGC = 30
πT = 0
30−0
=30 mmHgThis gives the net pulling-back force.
Now subtract both results:
Net Filtration Pressure
=
45 −30
=
15 mmHgFinally multiply by Kf
GFR
=
Kf ×15If Kf increases, GFR increases.
If Kf decreases, GFR decreases.
Entire Equation in One Easy Flow
STEP 1
Pressure pushing OUT
PGC − PT
↓
STEP 2
Pressure pulling BACK
πGC − πT
↓
STEP 3
Subtract both pressures
↓
Net Filtration Pressure
↓
STEP 4
Multiply by Kf
↓
GFRSuper Easy Memory Formula
GFR
=
Filter Quality
×
(Pushing Force
−
Pulling Force)OR
GFR
=
Kf
×
(Net Filtration Pressure)One-Line Concept
More PUSHING Pressure
↑
↑ GFR
More PULLING Pressure
↓
↓ GFRQuick Table
| Factor | Action | Effect on GFR |
|---|---|---|
| ↑ PGC | Pushes fluid out | ↑ GFR |
| ↑ PT | Pushes back | ↓ GFR |
| ↑ πGC | Pulls fluid into blood | ↓ GFR |
| ↑ πT | Pulls fluid into Bowman’s space | ↑ GFR (normally negligible) |
| ↑ Kf | Better filtration | ↑ GFR |
KEY CONCEPT
- The GFR equation is easiest to remember as: “GFR = Filter Quality (Kf) × Net Filtration Pressure.” Glomerular capillary hydrostatic pressure (PGC) pushes fluid out and increases GFR, while Bowman’s space pressure (PT) and plasma oncotic pressure (πGC) oppose filtration and decrease GFR. Bowman’s space oncotic pressure (πT) is normally almost zero, so it has little effect. The balance of these forces determines how much filtrate the kidneys produce each minute.
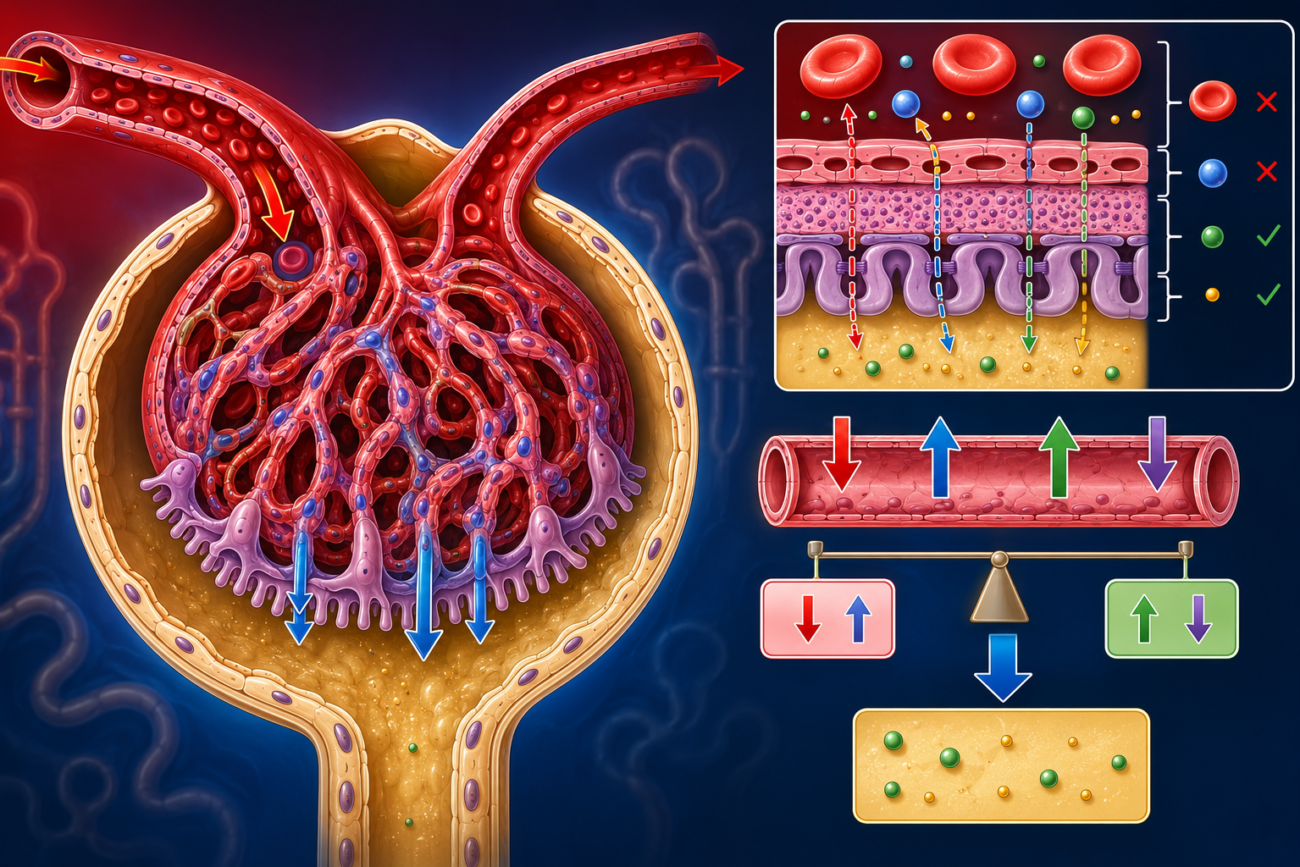
PERMEABILITY
- The glomerular capillaries are about 50 times more permeable than the capillaries in skeletal muscle.
- This high permeability allows the kidneys to filter large amounts of plasma efficiently.
- Neutral substances with an effective molecular diameter less than 4 nm are freely filtered.
- Neutral substances with a diameter greater than 8 nm are almost not filtered at all.
- For substances with a diameter between 4 and 8 nm:
- The larger the molecule, the less it is filtered.
- Thus, filtration decreases as molecular size increases.
- The glomerular capillary wall contains negatively charged sialoproteins.
- These negative charges repel negatively charged (anionic) substances in the blood.
- Therefore:
- A negatively charged molecule (anion) with a diameter of 4 nm is filtered less than half as much as a neutral molecule of the same size.
- Albumin is an example of a negatively charged protein.
- Although albumin has an effective diameter of about 7 nm, its filtration is much lower than expected based on size alone.
- Normally, the albumin concentration in the glomerular filtrate is only about 0.2% of its plasma concentration.
- This is because the negative charge of the glomerular membrane repels negatively charged albumin.
- In contrast, positively charged (cationic) substances are filtered more easily than neutral substances.
- Normally, urine contains less than 100 mg of protein per day.
- Most of this protein does not come from filtration.
- Instead, it comes from shed tubular cells.
- The presence of significant amounts of albumin in urine is called albuminuria.
- In nephritis:
- The negative charges of the glomerular filtration barrier are lost.
- As a result, albumin can pass into the urine more easily.
- This can occur even without an increase in the size of the filtration pores.
Easy Concept
Think of the glomerular filtration membrane as a security gate with both size and charge filters.
Step 1: Size Filter
Molecule Size
< 4 nm
↓
Freely Filtered
4–8 nm
↓
Partially Filtered
(Size ↑ → Filtration ↓)
> 8 nm
↓
Almost Not FilteredStep 2: Charge Filter
Glomerular Membrane
Negative Charge
↓
Repels Negative Molecules
(Albumin)
↓
Less FiltrationAlbumin Example
Albumin
Diameter ≈ 7 nm
Negative Charge
↓
Repelled by
Negative Membrane
↓
Very Little Filtered
↓
Only 0.2% enters filtrateNephritis
Nephritis
↓
Negative Charges Lost
↓
Albumin No Longer Repelled
↓
Albumin Passes Into Urine
↓
AlbuminuriaEasy Memory Trick
Filtration depends on:
SIZE
+
CHARGESmall + Neutral
↓↓
Easy FiltrationLarge + Negative
↓↓
Poor FiltrationPositive Charge
↓↓
Best FiltrationKEY CONCEPT
- Glomerular permeability depends on both molecular size and electrical charge. Neutral molecules smaller than 4 nm are freely filtered, whereas molecules larger than 8 nm are almost completely excluded. The negatively charged glomerular membrane repels negatively charged proteins such as albumin, so very little albumin is filtered despite its size. In nephritis, loss of these negative charges allows albumin to enter the urine, causing albuminuria even without enlargement of the filtration pores.
SIZE OF THE CAPILLARY BED
- The size of the glomerular capillary bed affects the glomerular ultrafiltration coefficient (Kf).
- Mesangial cells can change Kf by changing the filtration surface area.
- When mesangial cells contract:
- Kf decreases.
- This happens mainly because the surface area available for filtration becomes smaller.
- Mesangial cell contraction also:
- Narrows (distorts) some capillary loops.
- Reduces the area through which filtration can occur.
- At the branching points (bifurcations) of the capillary loops:
- Contraction can divert blood flow away from some capillary loops.
- As a result, fewer capillaries participate in filtration.
- In other parts of the glomerulus:
- Contracted mesangial cells press into the capillary lumen.
- This further reduces the filtration area.
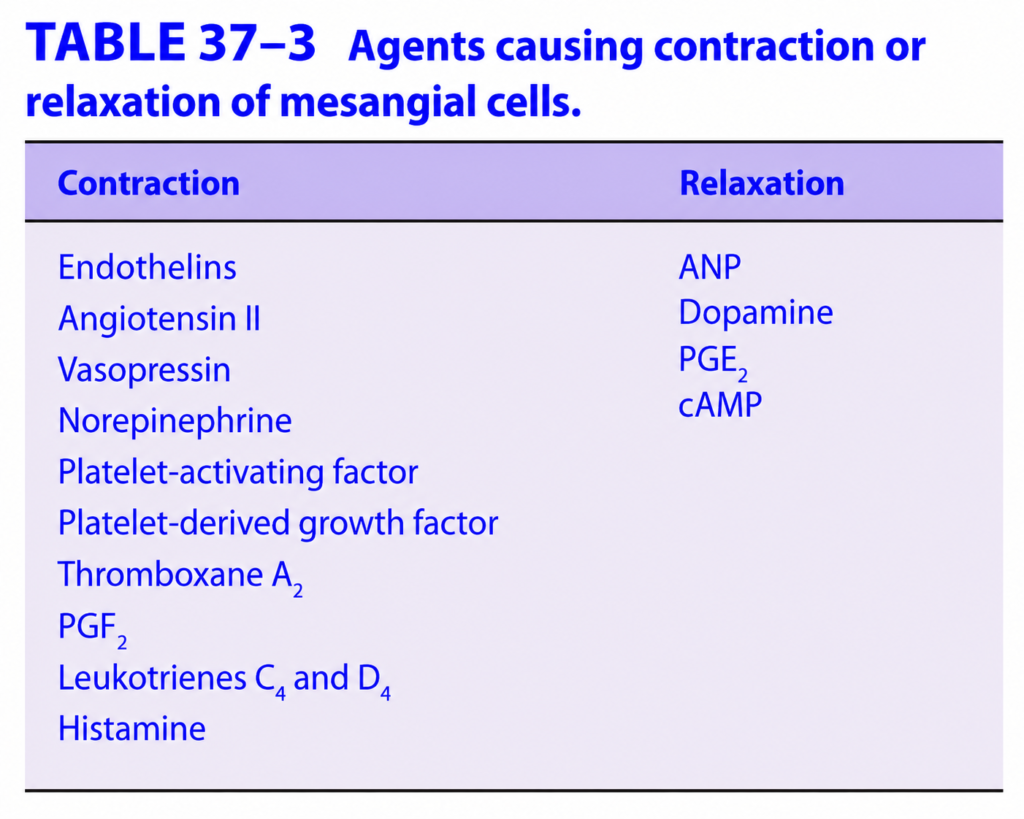
- Various chemical agents can affect mesangial cell contraction (listed in Table 37–3).
- Angiotensin II is an important regulator of mesangial cell contraction.
- Angiotensin II receptors are present in the glomeruli.
- Some evidence also suggests that mesangial cells may produce renin.
Easy Concept
Think of mesangial cells as adjustable “hands” around the glomerular capillaries.
Relaxed Mesangial Cells
Mesangial Cells Relax
↓
Capillary loops open
↓
Large Filtration Surface Area
↓
↑ Kf
↓
↑ GFRContracted Mesangial Cells
Mesangial Cells Contract
↓
Capillary loops become smaller
↓
Filtration Surface Area decreases
↓
↓ Kf
↓
↓ GFREffect of Angiotensin II
Angiotensin II
↓
Mesangial Cell Contraction
↓
↓ Filtration Surface Area
↓
↓ Kf
↓
↓ GFREasy Memory Trick
Mesangial Cells
Relax
↓↓
Large Filter
↓↓
↑ KfMesangial Cells
Contract
↓↓
Small Filter
↓↓
↓ KfKEY CONCEPT
- Mesangial cells regulate the size of the glomerular capillary filtration surface. When they contract, the filtration surface area decreases, reducing the glomerular ultrafiltration coefficient (Kf) and lowering GFR. Angiotensin II is an important stimulus for mesangial cell contraction, and mesangial cells may also produce renin.
HYDROSTATIC & OSMOTIC PRESSURE
- GFR is strongly influenced by hydrostatic pressure and osmotic (oncotic) pressure across the glomerular capillaries.
- The hydrostatic pressure in the glomerular capillaries is higher than in most other capillary beds.
- This high pressure occurs because:
- The afferent arterioles are short, straight branches of the interlobular arteries.
- The efferent arterioles have relatively high resistance, which maintains a high pressure inside the glomerular capillaries.
- The high glomerular capillary hydrostatic pressure pushes fluid from the blood into Bowman’s capsule, promoting filtration.
- This filtration pressure is opposed by:
- Hydrostatic pressure in Bowman’s capsule (PT).
- Oncotic pressure gradient across the glomerular capillaries (πGC − πT).
- Normally:
- πT (oncotic pressure in Bowman’s space) is almost zero.
- Therefore, the oncotic pressure gradient is essentially equal to the plasma oncotic pressure (πGC).
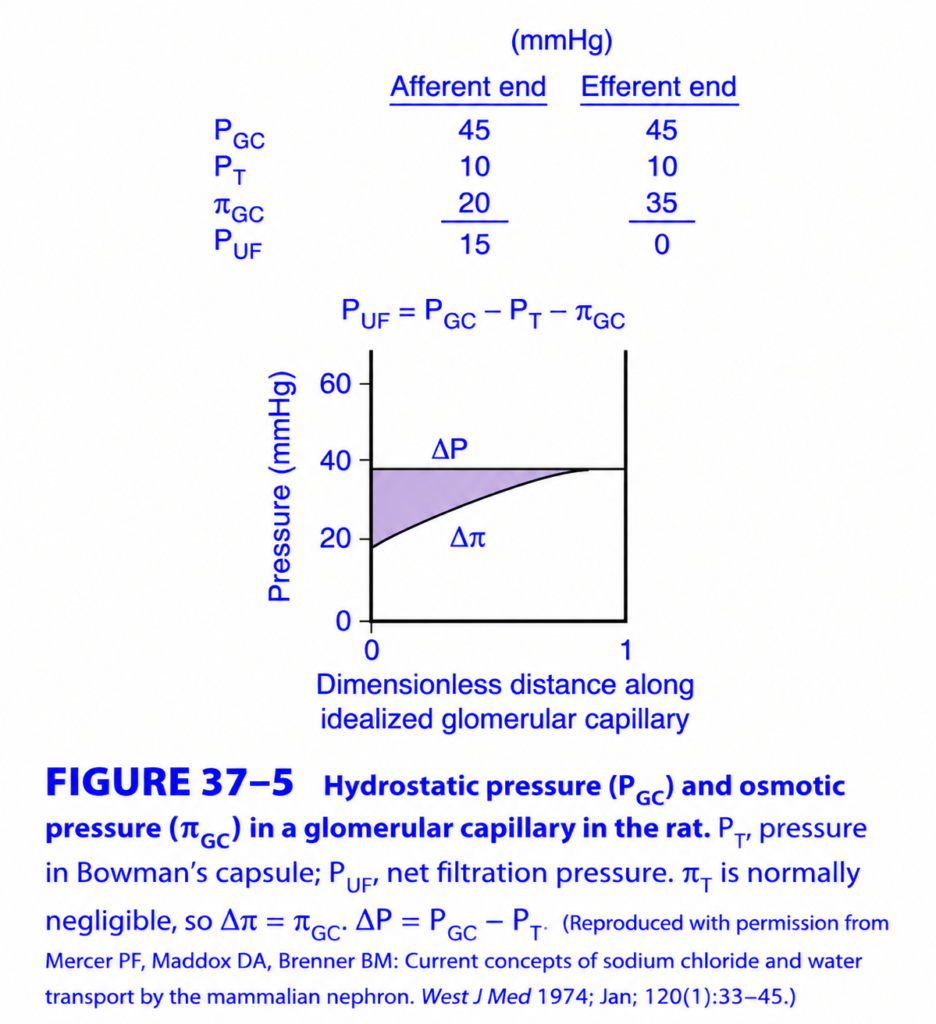
Figure 37–5
- At the afferent end of the glomerular capillaries:
- Net Filtration Pressure (PUF) = 15 mmHg.
- Therefore, filtration is maximal.
- As blood flows through the glomerular capillaries:
- Fluid leaves the plasma.
- Plasma proteins become more concentrated.
- Therefore, plasma oncotic pressure (πGC) gradually increases.
- As πGC increases:
- The net filtration pressure gradually decreases.
- Near the efferent end of the glomerular capillaries:
- Net filtration pressure falls to zero.
- This is called filtration equilibrium.
- At this point, filtration stops.
- Figure 37–5 also shows the calculated increase in oncotic pressure (Δπ) along the glomerular capillary.
- Because filtration stops before blood reaches the end of the capillary:
- Some portions of the glomerular capillaries normally do not participate in filtration.
- Therefore, glomerular filtration is flow-limited rather than diffusion-limited.
- If renal plasma flow (RPF) increases:
- The rise in plasma oncotic pressure becomes slower.
- Filtration continues along a greater length of the capillary.
- Therefore, GFR increases.
- There is considerable variation among different species regarding whether filtration equilibrium is reached.
- It is not certain whether filtration equilibrium occurs in humans.
Easy Concept
Think of the glomerular capillary as a water pipe with increasing protein concentration.
Beginning of the Capillary
High Blood Pressure
↓
Strong Filtration
↓
Net Filtration Pressure
≈ 15 mmHgMiddle of the Capillary
Fluid leaves blood
↓
Proteins become concentrated
↓
Plasma Oncotic Pressure rises
↓
Filtration gradually decreasesEnd of the Capillary
High Plasma Protein
↓
Strong Pulling Force
↓
Net Filtration Pressure = 0
↓
Filtration Stops
(Filtration Equilibrium)Effect of Increased Renal Plasma Flow (RPF)
↑ Renal Plasma Flow
↓
Proteins concentrate more slowly
↓
Oncotic Pressure rises slowly
↓
Filtration continues longer
↓
↑ GFREasy Memory Trick
Start of Capillary
High Push
↓
High FiltrationEnd of Capillary
High Protein
↓
High Pull
↓
Filtration StopsKEY CONCEPT
- The high hydrostatic pressure in the glomerular capillaries promotes filtration, whereas Bowman’s capsule hydrostatic pressure and plasma oncotic pressure oppose it. At the afferent end of the glomerular capillary, the net filtration pressure is about 15 mmHg. As plasma proteins become concentrated along the capillary, oncotic pressure rises, causing the net filtration pressure to fall to zero near the efferent end (filtration equilibrium). Increasing renal plasma flow slows the rise in oncotic pressure, prolongs filtration along the capillary, and increases GFR. Figure 37–5 illustrates these pressure changes.
Forces Governing Glomerular Filtration (GANONG Fig. 37-5) – Easiest & Most Conceptual Explanation
🎯 One-Line Concept
Glomerular filtration depends on the balance between forces that push fluid out of the glomerular capillary and forces that oppose filtration.
Think of filtration like water passing through a filter.
- 💪 Some forces push water out.
- 🛑 Other forces pull or push water back, opposing filtration.
The final result is called the Net Filtration Pressure (PUF).
The Three Important Pressures
Only three major forces determine glomerular filtration in this figure.
1. PGC = Glomerular Capillary Hydrostatic Pressure
2. PT = Bowman's Capsule Hydrostatic Pressure
3. πGC = Plasma Colloid Osmotic Pressure1. Glomerular Capillary Hydrostatic Pressure (PGC)
Value
45 mm Hg
This is the blood pressure inside the glomerular capillaries.
Function
It pushes water out of the capillary into Bowman’s capsule.
Blood Pressure
↓
Pushes Filtrate OutIt is the ONLY pressure that favors filtration.
Think of it as
🚰 Water pressure inside a garden hose pushing water outward.
2. Bowman’s Capsule Hydrostatic Pressure (PT)
Value
10 mm Hg
Once filtrate enters Bowman’s capsule,
it creates pressure that pushes back toward the capillary.
Bowman's Capsule
↑
Pushes BackThis pressure opposes filtration.
Think of it like
If a bucket under a tap becomes full,
the water inside the bucket pushes upward, making it harder for more water to enter.
3. Plasma Colloid Osmotic Pressure (πGC)
Value
Afferent End = 20 mm Hg
Efferent End = 35 mm Hg
This pressure is produced by plasma proteins (mainly albumin).
Proteins cannot leave the capillary,
so they pull water back into the blood.
Albumin
↓
Pulls Water BackThis pressure also opposes filtration.
Why Does πGC Increase Along the Capillary?
This is the most important concept in the graph.
At the beginning,
blood contains
Water + Proteins
As filtration continues,
water leaves,
but proteins remain.
Beginning
Water + Protein
↓
Water leaves
↓
Protein concentration increases
↓
Osmotic pressure increasesTherefore,
πGC increases
from
20 mm Hg → 35 mm Hg
Net Filtration Pressure (PUF)
The figure gives the formula.
Formula
PUF = PGC − PT − πGCSimply remember:
Pushing Force
−
Opposing Force
=
Net FiltrationAt the Afferent End
Values
PGC = 45
PT = 10
πGC = 20
Calculation
45 −10 −20
=15 mm HgNet Filtration Pressure
15 mm Hg
Filtration is strong.
At the Efferent End
Values
PGC = 45
PT = 10
πGC = 35
Calculation
45 −10 −35
=0Net Filtration Pressure
0 mm Hg
Filtration has essentially stopped by the end of the capillary in this idealized example.
Understanding the Graph
The graph shows pressure changes along the glomerular capillary.
Horizontal Line
This represents
PGC − PT
45
−10
-----
35 mm HgThis value remains almost constant.
Rising Curved Line
This is
πGC
At the beginning
20 mm Hg
↓
Gradually increases
↓
35 mm Hg
because proteins become more concentrated.
Purple Shaded Area
This represents
Net Filtration Pressure
At the start,
the shaded area is large,
meaning filtration is high.
As proteins become concentrated,
the shaded area becomes smaller.
At the end,
the shaded area disappears,
meaning
Net filtration pressure = 0.
Complete Pressure Story
Beginning
PGC = 45
PT =10
πGC=20
Net Pressure
15 mm Hg
↓↓↓↓↓↓↓↓
Filtration occurs
↓
Water leaves blood
↓
Protein concentration increases
↓
πGC rises
↓
Net pressure decreases
↓
Filtration slows
↓
End of capillary
Net Pressure = 0Easy Analogy
Imagine washing rice in a sieve.
Tap Water Pressure
Pushes water through.
Equivalent to
PGC
Rice Already in the Bowl
Pushes back slightly.
Equivalent to
PT
Sponge Pulling Water Back
Equivalent to
Plasma proteins
(πGC)
Only when
Water pressure >
Opposing pressures
does water continue flowing.
Easy Memory Trick
PGC
Pushes Out
PT
Pushes Back
πGC
Pulls Back
Which Forces Favor and Oppose Filtration?
| Force | Direction | Effect |
|---|---|---|
| PGC (Glomerular hydrostatic pressure) | Out of capillary | ✅ Favors filtration |
| PT (Bowman’s capsule hydrostatic pressure) | Into capillary | ❌ Opposes filtration |
| πGC (Plasma colloid osmotic pressure) | Into capillary | ❌ Opposes filtration |
Why Is PGC So High?
The glomerular capillary has:
- A wide afferent arteriole bringing blood in.
- A narrower efferent arteriole carrying blood out.
This maintains a relatively high hydrostatic pressure, which is essential for efficient filtration.
MBBS High-Yield Concepts
⭐ Formula
PUF = PGC − PT − πGC⭐ Normal Values (Figure)
| Pressure | Afferent End | Efferent End |
|---|---|---|
| PGC | 45 mm Hg | 45 mm Hg |
| PT | 10 mm Hg | 10 mm Hg |
| πGC | 20 mm Hg | 35 mm Hg |
| PUF | 15 mm Hg | 0 mm Hg |
⭐ Why does πGC increase?
Because:
- Water is filtered out.
- Proteins remain inside the capillary.
- Protein concentration increases.
- Osmotic pressure rises.
⭐ Why does filtration decrease along the capillary?
Because the opposing plasma colloid osmotic pressure (πGC) progressively increases, reducing the net filtration pressure.
Complete Flow Chart
Blood Enters Glomerulus
│
▼
PGC = 45
(Pushes Out)
│
▼
Filtration Begins
│
▼
Water Leaves Blood
│
▼
Protein Concentration ↑
│
▼
πGC ↑
(Pulls Water Back)
│
▼
Net Filtration Pressure ↓
│
▼
End of Capillary
PUF = 0🌟 Super Memory Summary
FORCES IN GLOMERULUS
PGC = 45
(Pushes OUT) ✅
PT = 10
(Pushes IN) ❌
πGC = 20 → 35
(Pulls IN) ❌
Formula
PUF = PGC − PT − πGC
Beginning
45 −10 −20 =15
⭐⭐ Strong Filtration
End
45 −10 −35 =0
⭐⭐ Filtration Stops🧠 Easy Mnemonic
“Push – Push Back – Pull Back”
- PGC → Pushes filtrate out.
- PT → Pushes filtrate back.
- πGC → Pulls water back into blood.
💎 Golden Rule
Glomerular filtration occurs because the glomerular hydrostatic pressure (PGC) exceeds the opposing forces of Bowman’s capsule hydrostatic pressure (PT) and plasma colloid osmotic pressure (πGC). As filtration proceeds, proteins become more concentrated within the capillary, causing πGC to rise, which progressively reduces the net filtration pressure along the glomerular capillary.
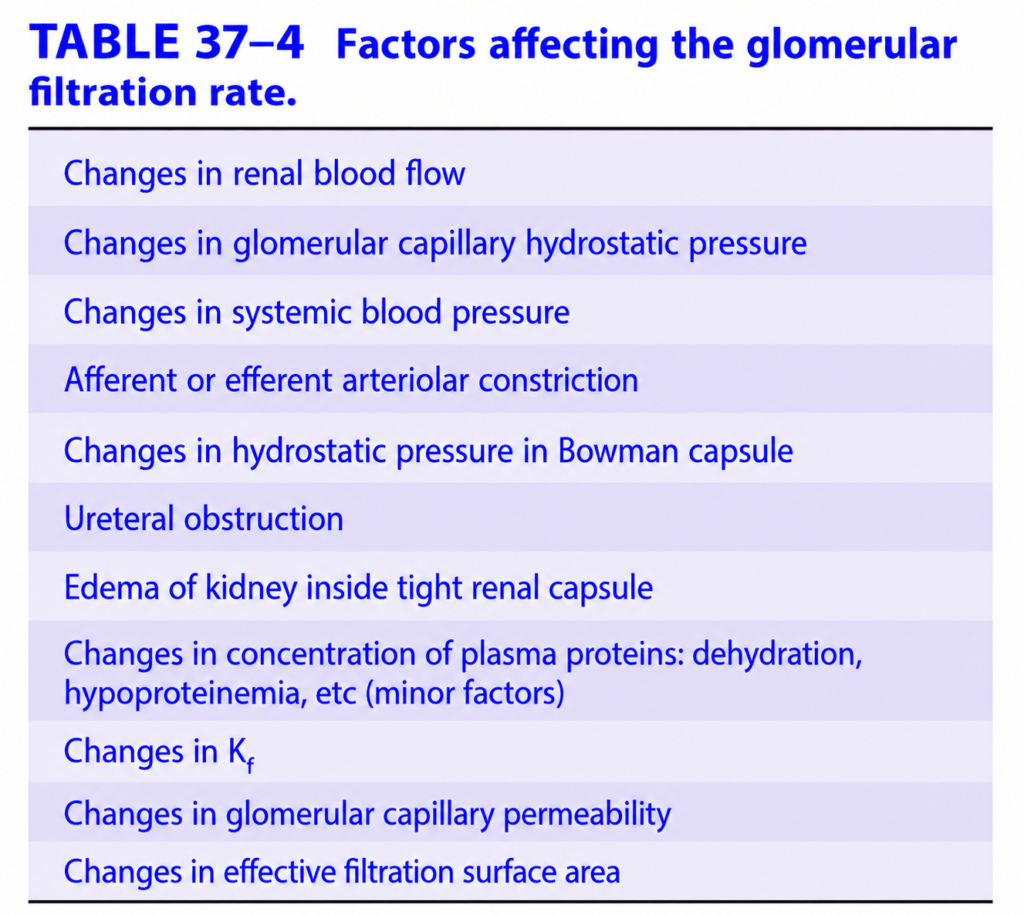
CHANGES IN GFR
- Changes in the factors that control filtration produce predictable changes in GFR (listed in Table 37–4).
- Renal vascular resistance changes because of autoregulation.
- Autoregulation helps keep the filtration pressure stable, even when blood pressure changes within the normal autoregulatory range.
- However, if the mean systemic arterial pressure falls below the autoregulatory range (Figure 37–4):
- Autoregulation can no longer maintain filtration pressure.
- As a result, GFR decreases sharply.
- Constriction of the efferent arteriole helps maintain GFR better than constriction of the afferent arteriole.
- This is because efferent arteriolar constriction increases pressure inside the glomerular capillaries, helping to sustain filtration.
- However:
- Both afferent and efferent arteriolar constriction decrease blood flow to the renal tubules.
Figure 37–4
Shows that:
- Within the autoregulatory blood pressure range, renal blood flow and GFR remain relatively constant.
- Below the autoregulatory range, GFR falls rapidly.
Easy Concept
Think of the kidney as an automatic water filter.
Normal Blood Pressure
Normal Blood Pressure
↓
Autoregulation Works
↓
Filtration Pressure Maintained
↓
Normal GFRLow Blood Pressure
Blood Pressure Falls
Below Autoregulatory Range
↓
Autoregulation Fails
↓
Filtration Pressure Falls
↓
GFR Drops SharplyEffect of Arteriolar Constriction
Efferent Arteriole Constriction
↓
↑ Glomerular Pressure
↓
Helps Maintain GFRAfferent or Efferent
Constriction
↓
↓ Renal Blood Flow
↓
Less Blood Reaches TubulesEasy Memory Trick
Autoregulation
↓↓
Keeps GFR StableBlood Pressure Too Low
↓↓
Autoregulation Stops
↓↓
GFR Falls QuicklyEfferent Constriction
↓↓
Maintains GFR Better
BUT
↓↓
Still Reduces Renal Blood FlowKEY CONCEPT
- GFR is normally stabilized by renal autoregulation. When systemic arterial pressure falls below the autoregulatory range (Figure 37–4), GFR decreases sharply. Efferent arteriolar constriction helps maintain glomerular filtration pressure better than afferent constriction, but both types of constriction reduce blood flow to the renal tubules.
FILTRATION FRACTION
- Filtration Fraction (FF) is the fraction (percentage) of renal plasma flow (RPF) that is filtered into Bowman’s capsule.
Formula
Filtration Fraction (FF)=RPFGFR
Easy Concept of the Formula
Renal Plasma Flow (RPF)
↓
Some plasma is filtered
↓
Glomerular Filtration Rate (GFR)
FF = Filtered Plasma
-------------------
Total Plasma Entering KidneyNormal Value
- Normal Filtration Fraction = 0.16–0.20
- This means 16–20% of the plasma entering the kidneys is filtered.
- The remaining 80–84% continues into the efferent arteriole.
Example (Conceptual)
If:
- GFR = 125 mL/min
- RPF = 625 mL/min
Then:
Step 1
FF=625125
Step 2
FF=0.20
Final Answer
FF=0.20=20%
Easy meaning:
- Out of 625 mL of plasma entering the kidneys every minute, only 125 mL is filtered.
- The remaining 500 mL is not filtered.
- Normally, GFR changes less than RPF.
- This means GFR is better maintained than renal plasma flow.
- When systemic blood pressure falls:
- RPF decreases.
- GFR also decreases, but to a lesser extent.
- This happens because:
- The efferent arteriole constricts.
- This helps maintain glomerular capillary pressure and supports filtration.
- Since RPF decreases more than GFR:
Filtration Fraction increases
Easy Concept
Think of RPF as the total water entering a filter.
625 mL Plasma
Enters Kidney
↓
125 mL Filtered
↓
FF = 20%During Low Blood Pressure
↓ Blood Pressure
↓
↓ Renal Plasma Flow
↓
Efferent Arteriole Constricts
↓
GFR Falls Only Slightly
↓
FF IncreasesEasy Memory Trick
FF
=
Filtered Plasma
÷
Total Plasma Entering KidneyNormal FF
=
16–20%
≈ 20%Low Blood Pressure
↓
RPF decreases more than GFR
↓
FF increasesKEY CONCEPT
- Filtration Fraction (FF) is the ratio of GFR to renal plasma flow (FF = GFR ÷ RPF). Normally, FF is 0.16–0.20 (16–20%), meaning that about one-fifth of the plasma entering the kidneys is filtered. During a fall in systemic blood pressure, efferent arteriolar constriction helps preserve GFR more than RPF, causing the filtration fraction to increase.