Skip to content
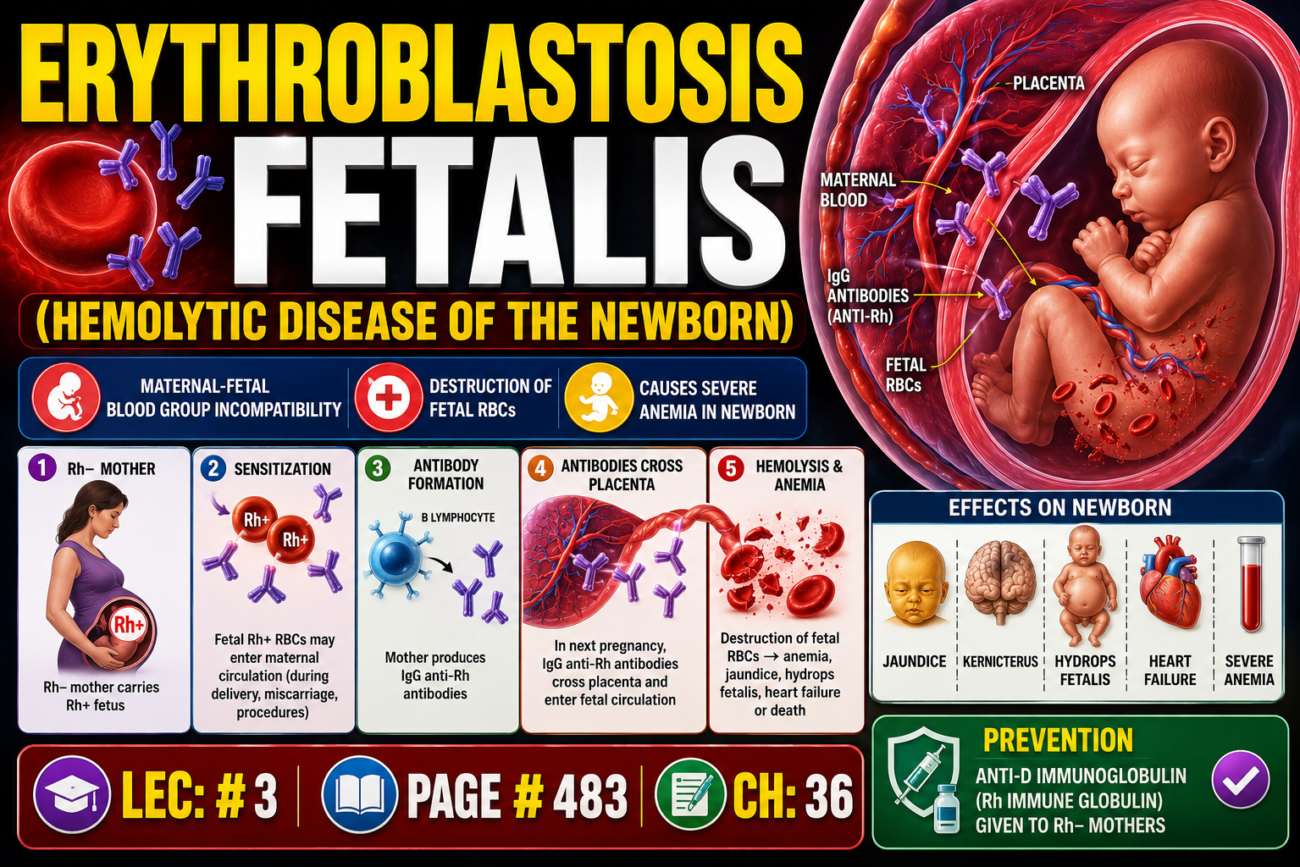
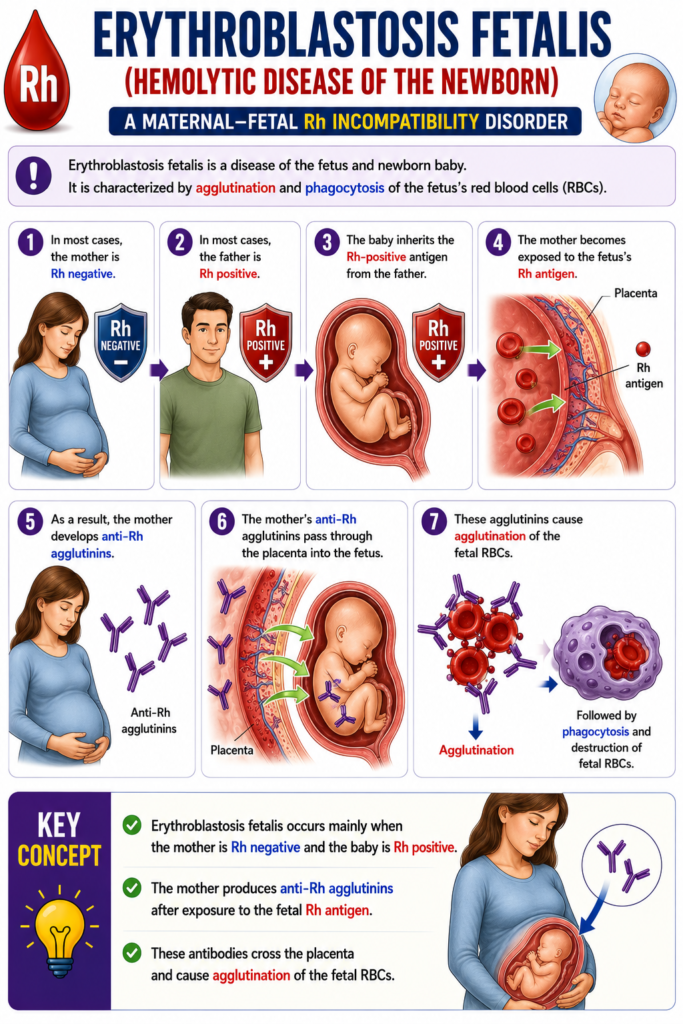
- Erythroblastosis fetalis is a disease of the fetus and newborn baby.
- It is characterized by agglutination and phagocytosis of the fetus’s red blood cells (RBCs).
- In most cases, the mother is Rh negative.
- In most cases, the father is Rh positive.
- The baby inherits the Rh-positive antigen from the father.
- The mother becomes exposed to the fetus’s Rh antigen.
- As a result, the mother develops anti-Rh agglutinins.
- The mother’s anti-Rh agglutinins pass through the placenta into the fetus.
- These agglutinins cause agglutination of the fetal RBCs.
Key Concept
- Erythroblastosis fetalis occurs mainly when the mother is Rh negative and the baby is Rh positive.
- The mother produces anti-Rh agglutinins after exposure to the fetal Rh antigen.
- These antibodies cross the placenta and cause agglutination of the fetal RBCs.
Incidence of Erythroblastosis Fetalis
- An Rh-negative mother having her first Rh-positive baby usually does not produce enough anti-Rh agglutinins to cause harm.
- About 3% of second Rh-positive babies show signs of erythroblastosis fetalis.
- About 10% of third Rh-positive babies develop erythroblastosis fetalis.
- The incidence increases progressively with each subsequent Rh-positive pregnancy.
Key Concept
- The first Rh-positive pregnancy is usually not affected because the mother produces few anti-Rh agglutinins.
- The risk of erythroblastosis fetalis increases with each subsequent Rh-positive pregnancy.
- Second Rh-positive baby: 3% affected.
- Third Rh-positive baby: 10% affected.
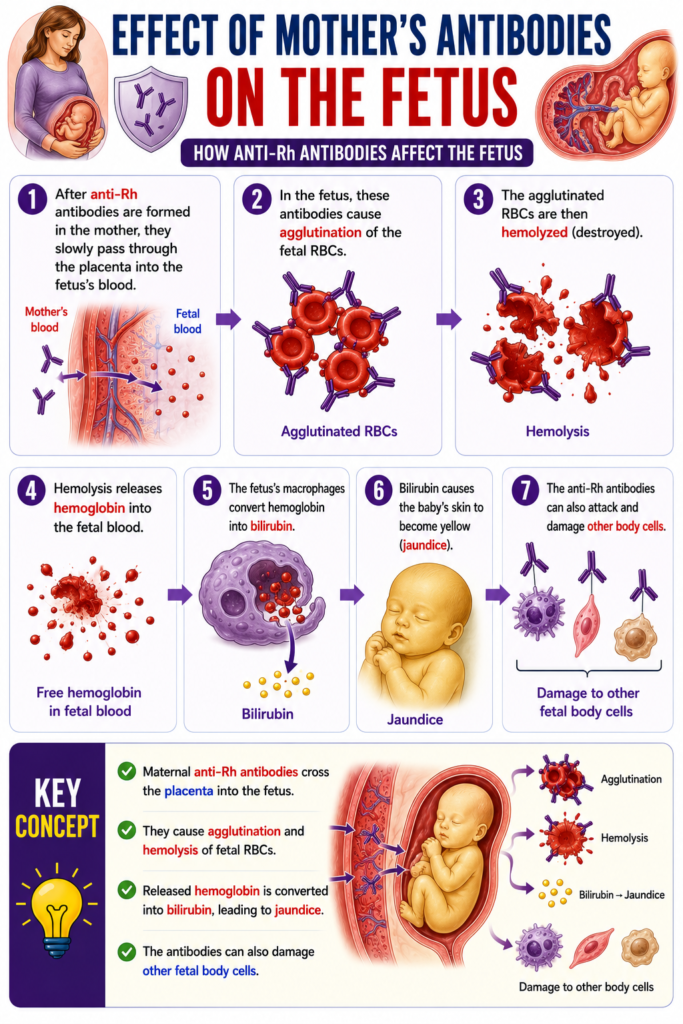
Effect of Mother’s Antibodies on the Fetus
- After anti-Rh antibodies are formed in the mother, they slowly pass through the placenta into the fetus’s blood.
- In the fetus, these antibodies cause agglutination of the fetal RBCs.
- The agglutinated RBCs are then hemolyzed (destroyed).
- Hemolysis releases hemoglobin into the fetal blood.
- The fetus’s macrophages convert hemoglobin into bilirubin.
- Bilirubin causes the baby’s skin to become yellow (jaundice).
- The anti-Rh antibodies can also attack and damage other body cells.
Key Concept
- Maternal anti-Rh antibodies cross the placenta into the fetus.
- They cause agglutination and hemolysis of fetal RBCs.
- Released hemoglobin is converted into bilirubin, leading to jaundice.
- The antibodies can also damage other fetal body cells.
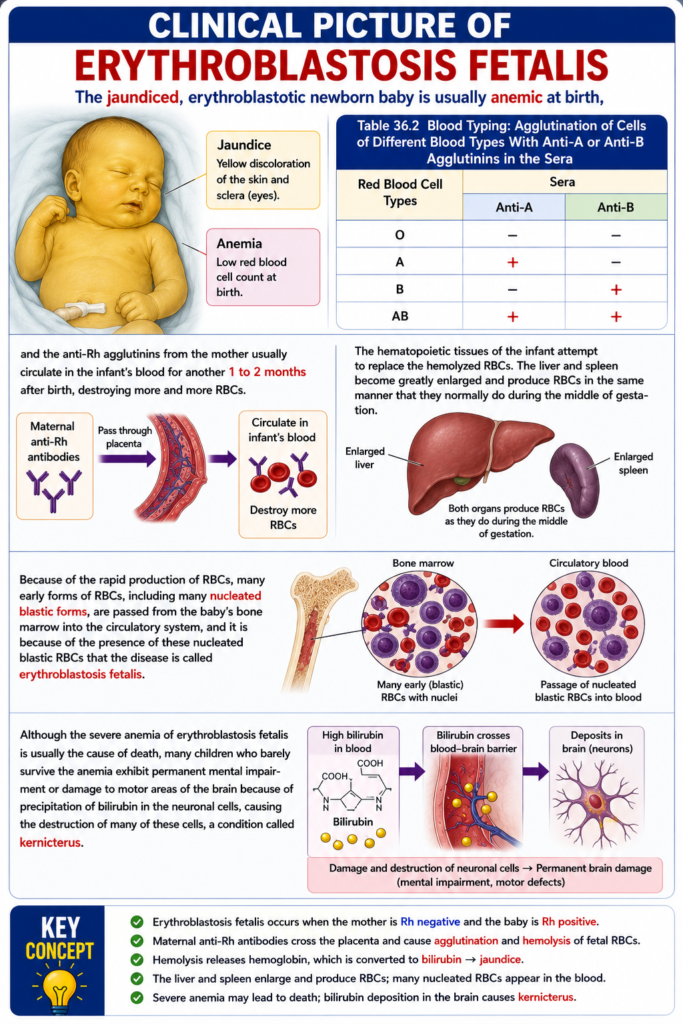
Clinical Picture of Erythroblastosis
- The jaundiced newborn with erythroblastosis fetalis is usually anemic at birth.
- The mother’s anti-Rh agglutinins continue to circulate in the infant’s blood for 1 to 2 months after birth.
- During this time, these antibodies continue destroying more RBCs.
- The infant’s hematopoietic tissues try to replace the hemolyzed RBCs.
- The liver becomes greatly enlarged and starts producing RBCs.
- The spleen also becomes greatly enlarged and produces RBCs.
- The liver and spleen produce RBCs in the same way they normally do during the middle of gestation.
- Because RBC production is very rapid, many early RBC forms are released into the circulation.
- Many nucleated blastic RBCs are released from the bone marrow into the bloodstream.
- The presence of these nucleated blastic RBCs is why the disease is called erythroblastosis fetalis.
- Severe anemia is usually the main cause of death in erythroblastosis fetalis.
- Some babies who survive severe anemia develop permanent mental impairment.
- Some survivors also develop damage to the motor areas of the brain.
- This damage occurs because bilirubin is deposited in neuronal cells.
- Bilirubin destroys many neuronal cells.
- This condition is called kernicterus.
- Table 36.2 shows the blood typing results with anti-A and anti-B agglutinins:
| Red Blood Cell Type | Anti-A | Anti-B |
|---|
| O | − | − |
| A | + | − |
| B | − | + |
| AB | + | + |
Key Concept
- Babies with erythroblastosis fetalis are usually anemic and jaundiced at birth.
- Maternal anti-Rh antibodies continue destroying fetal RBCs for 1–2 months after birth.
- The liver, spleen, and bone marrow increase RBC production, releasing nucleated blastic RBCs.
- Severe anemia may cause death, while bilirubin deposition in the brain can cause kernicterus with permanent neurological damage.
- Table 36.2 Blood Typing:
- O: Anti-A (−), Anti-B (−)
- A: Anti-A (+), Anti-B (−)
- B: Anti-A (−), Anti-B (+)
- AB: Anti-A (+), Anti-B (+)
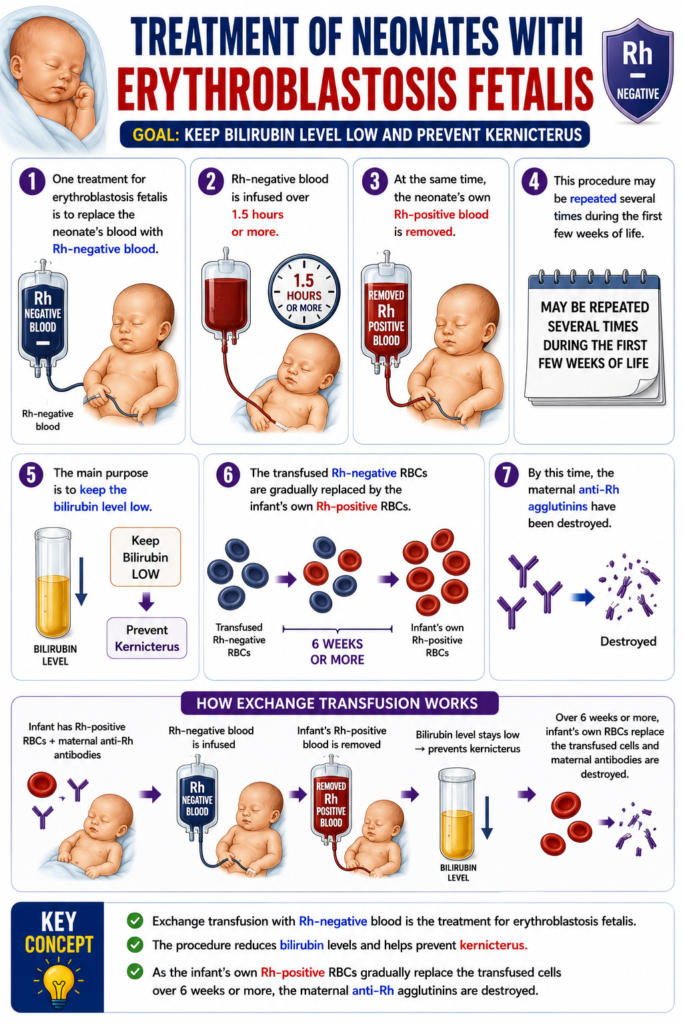
Treatment of Neonates With Erythroblastosis Fetalis
- One treatment for erythroblastosis fetalis is to replace the neonate’s blood with Rh-negative blood.
- Rh-negative blood is infused over 1.5 hours or more.
- At the same time, the neonate’s own Rh-positive blood is removed.
- This procedure may be repeated several times during the first few weeks of life.
- The main purpose is to keep the bilirubin level low.
- Keeping bilirubin low helps prevent kernicterus.
- The transfused Rh-negative RBCs are gradually replaced by the infant’s own Rh-positive RBCs.
- This replacement takes 6 weeks or more.
- By this time, the maternal anti-Rh agglutinins have been destroyed.
Key Concept
- Exchange transfusion with Rh-negative blood is the treatment for erythroblastosis fetalis.
- The procedure reduces bilirubin levels and helps prevent kernicterus.
- As the infant’s own Rh-positive RBCs gradually replace the transfused cells over 6 weeks or more, the maternal anti-Rh agglutinins are destroyed.
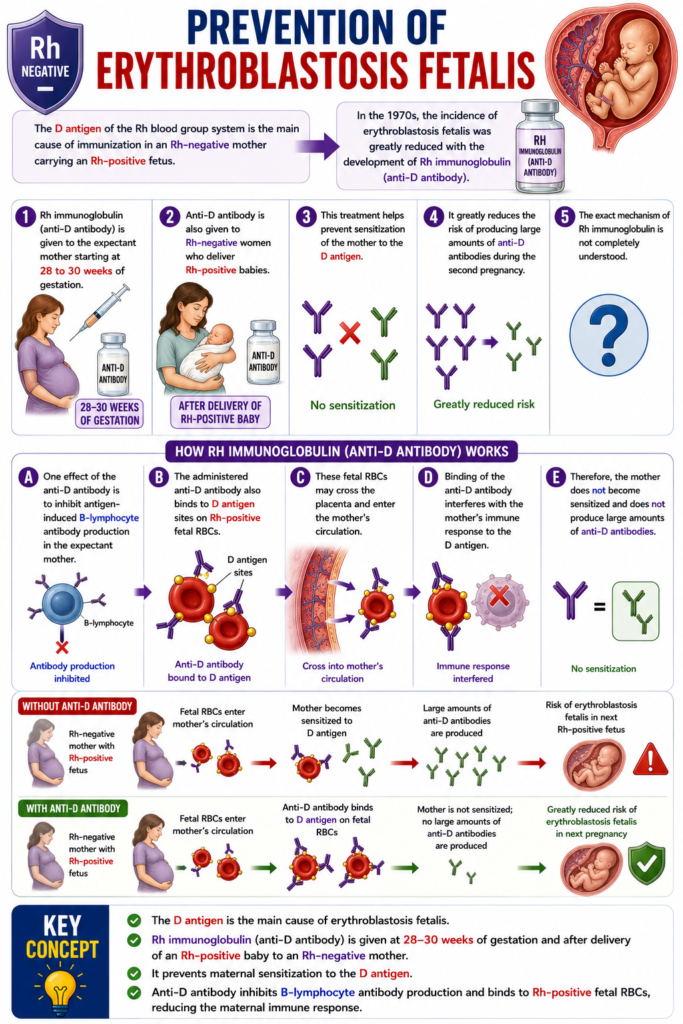
Prevention of Erythroblastosis Fetalis
- The D antigen of the Rh blood group system is the main cause of immunization in an Rh-negative mother carrying an Rh-positive fetus.
- In the 1970s, the incidence of erythroblastosis fetalis was greatly reduced with the development of Rh immunoglobulin (anti-D antibody).
- Rh immunoglobulin (anti-D antibody) is given to the expectant mother starting at 28 to 30 weeks of gestation.
- Anti-D antibody is also given to Rh-negative women who deliver Rh-positive babies.
- This treatment helps prevent sensitization of the mother to the D antigen.
- It greatly reduces the risk of producing large amounts of anti-D antibodies during the second pregnancy.
- The exact mechanism of Rh immunoglobulin is not completely understood.
- One effect of the anti-D antibody is to inhibit antigen-induced B-lymphocyte antibody production in the expectant mother.
- The administered anti-D antibody also binds to D antigen sites on Rh-positive fetal RBCs.
- These fetal RBCs may cross the placenta and enter the mother’s circulation.
- Binding of the anti-D antibody interferes with the mother’s immune response to the D antigen.
Key Concept
- The D antigen is the main cause of erythroblastosis fetalis.
- Rh immunoglobulin (anti-D antibody) is given at 28–30 weeks of gestation and after delivery of an Rh-positive baby to an Rh-negative mother.
- It prevents maternal sensitization to the D antigen.
- Anti-D antibody inhibits B-lymphocyte antibody production and binds to Rh-positive fetal RBCs, reducing the maternal immune response.