


- Extracellular fluid osmolarity and sodium concentration are controlled together.
- Sodium is the most abundant ion in the extracellular fluid.
- Normal plasma sodium concentration = 135–145 mEq/L.
- Average plasma sodium concentration = 142 mEq/L.
- Average osmolarity = 300 mOsm/L.
- Corrected osmolarity = 282 mOsm/L.
- Osmolarity usually changes by only ±2% to 3%.
- These values must be kept very precise.
- They control fluid distribution between intracellular and extracellular compartments.
Estimating Plasma Osmolarity From Plasma Sodium Concentration
- Plasma osmolarity is not routinely measured in most clinical laboratories.
- Sodium and its associated anions make up about 94% of extracellular solutes.
- Plasma osmolarity can be estimated from plasma sodium concentration.
Formula:
- Plasma Osmolarity = 2.1 × Plasma Sodium Concentration
Example:
- Plasma Sodium = 142 mEq/L
- Plasma Osmolarity = 2.1 × 142
- Plasma Osmolarity = 298 mOsm/L
- For greater accuracy, glucose and urea concentrations are also included.
- Plasma Osmolarity = (2 × Plasma Sodium) + Glucose + Urea
- These estimates are usually within a few percent of directly measured osmolarity.
- Sodium and associated anions normally contribute about 94% of extracellular osmoles.
- Glucose and urea contribute about 3% to 5% of total osmoles.
- Urea crosses most cell membranes easily.
- Urea produces little effective osmotic pressure under steady-state conditions.
- Sodium and its associated anions are the main determinants of fluid movement across cell membranes.
- Control of osmolarity and control of sodium concentration can be discussed together.
- Many mechanisms regulate sodium and water excretion by the kidneys.
- Two major systems regulate extracellular fluid sodium concentration and osmolarity.
- Osmoreceptor–ADH System
- Thirst Mechanism
KEY CONCEPT
- Sodium is the main extracellular ion.
- Normal plasma sodium = 135–145 mEq/L.
- Average plasma sodium = 142 mEq/L.
- Estimated Plasma Osmolarity = 2.1 × Plasma Sodium.
- Example: 142 × 2.1 = 298 mOsm/L.
- Sodium and associated anions determine most extracellular osmolarity.
- The two main regulators are ADH and Thirst.
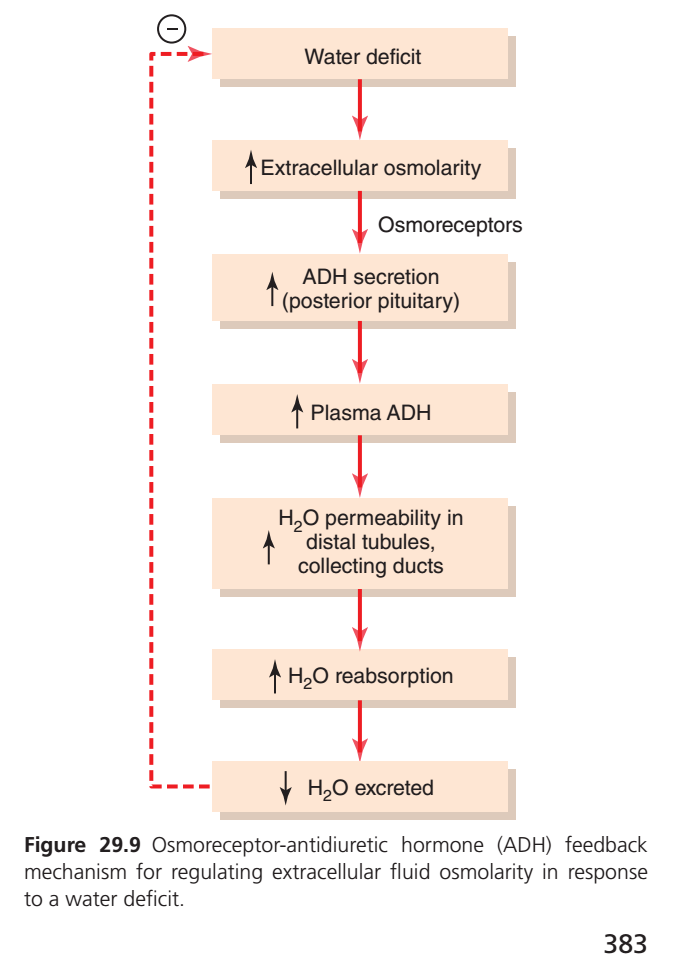
OSMORECEPTOR-ADH FEEDBACK SYSTEM
- The osmoreceptor-ADH feedback system controls extracellular fluid sodium concentration and osmolarity.
- This system becomes active when extracellular fluid osmolarity rises above normal.
- A water deficit can increase extracellular fluid osmolarity.
Step 1
- Extracellular fluid osmolarity increases.
- In practical terms, plasma sodium concentration increases.
- Special nerve cells called osmoreceptors detect this change.
- Osmoreceptor cells are located in the anterior hypothalamus.
- They are located near the supraoptic nuclei.
- Increased osmolarity causes osmoreceptor cells to shrink.
Step 2
- Shrinkage stimulates the osmoreceptor cells.
- Osmoreceptor cells begin firing nerve signals.
- These signals are sent to nerve cells in the supraoptic nuclei.
- The supraoptic nuclei relay the signals down the pituitary stalk.
- The signals reach the posterior pituitary gland.
Step 3
- Action potentials arrive at the posterior pituitary.
- The posterior pituitary releases ADH.
- ADH is stored in secretory granules (vesicles) in nerve endings.
Step 4
- ADH enters the bloodstream.
- ADH is transported to the kidneys.
- ADH increases water permeability of the late distal tubules.
- ADH increases water permeability of the cortical collecting tubules.
- ADH increases water permeability of the medullary collecting ducts.
Step 5
- Increased water permeability occurs in distal nephron segments.
- More water is reabsorbed.
- A smaller volume of urine is excreted.
- The urine becomes more concentrated.
Result
- Water is conserved in the body.
- Sodium continues to be excreted in urine.
- Other solutes continue to be excreted in urine.
- Extracellular fluid becomes diluted.
- The initial high osmolarity is corrected.
When Extracellular Fluid Becomes Too Dilute
- The opposite sequence occurs when extracellular fluid becomes hypo-osmotic.
- Excess water intake decreases extracellular fluid osmolarity.
- Less ADH is produced.
- Renal tubules become less permeable to water.
- Less water is reabsorbed.
- A larger volume of urine is excreted.
- The urine becomes dilute.
- Body fluids become more concentrated.
- Plasma osmolarity returns toward normal.
KEY CONCEPT
- ↑ Extracellular Osmolarity → Osmoreceptor Shrinkage
- Osmoreceptor Shrinkage → ↑ ADH Release
- ↑ ADH → ↑ Water Permeability in Distal Tubules & Collecting Ducts
- ↑ Water Reabsorption → ↓ Urine Volume
- Water Conservation → ↓ Extracellular Osmolarity
Easy Flow
Water Deficit → ↑ Osmolarity → Osmoreceptors Shrink → ↑ ADH → ↑ Water Reabsorption → Concentrated Urine → Osmolarity Returns Toward Normal
Excess Water Intake → ↓ Osmolarity → ↓ ADH → ↓ Water Reabsorption → Dilute Urine → Osmolarity Returns Toward Normal
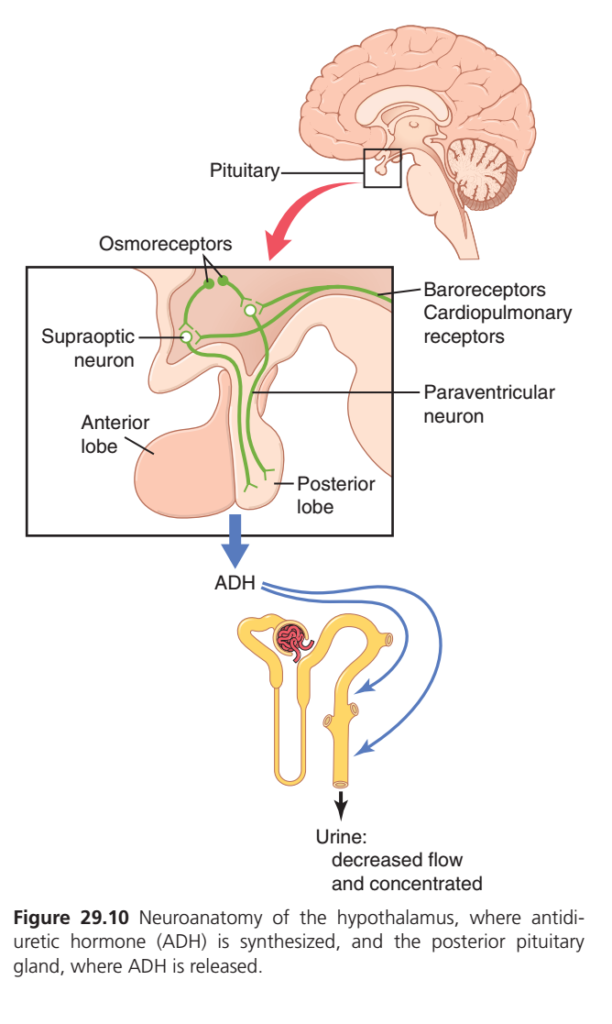
ADH Is Synthesized in Supraoptic and Paraventricular Nuclei of Hypothalamus and Released From the Posterior Pituitary
- ADH is synthesized in the hypothalamus.
- ADH is released from the posterior pituitary gland.
- The hypothalamus contains two types of magnocellular (large) neurons.
- These neurons synthesize ADH in the supraoptic and paraventricular nuclei.
Sites of ADH Production
- About 5/6 (≈83%) of ADH is synthesized in the supraoptic nuclei.
- About 1/6 (≈17%) of ADH is synthesized in the paraventricular nuclei.
- Both nuclei send axons to the posterior pituitary.
Transport of ADH
- After synthesis, ADH is transported down the axons.
- ADH moves to the nerve endings in the posterior pituitary gland.
Release of ADH
- Increased osmolarity stimulates the supraoptic and paraventricular nuclei.
- Other factors can also stimulate these nuclei.
- Nerve impulses travel down the axons to the nerve endings.
- Membrane permeability of the nerve endings changes.
- Calcium entry into the nerve endings increases.
- ADH is stored in secretory granules (vesicles).
- Increased calcium entry triggers ADH release.
- Released ADH enters the capillary blood of the posterior pituitary.
- ADH then enters the systemic circulation.
Response to Osmotic Stimulus
- ADH secretion occurs rapidly.
- Plasma ADH levels can increase severalfold within minutes.
- This provides a rapid way to alter renal water excretion.
AV3V Region
- Another important area for osmolarity and ADH control is the AV3V region.
- The AV3V region is located along the anteroventral region of the third ventricle.
Components of the AV3V Region
- The upper part contains the subfornical organ.
- The lower part contains the organum vasculosum of the lamina terminalis.
- Between them is the median preoptic nucleus.
Connections of the Median Preoptic Nucleus
- It has multiple nerve connections with the subfornical organ.
- It has multiple nerve connections with the organum vasculosum.
- It connects with the supraoptic nuclei.
- It connects with blood pressure control centers in the medulla.
Functions of the AV3V Region
- Damage to the AV3V region causes defects in ADH secretion control.
- Damage to the AV3V region causes defects in thirst control.
- Damage to the AV3V region causes defects in sodium appetite control.
- Damage to the AV3V region causes defects in blood pressure regulation.
Stimulation of the AV3V Region
- Electrical stimulation of the AV3V region increases ADH secretion.
- Electrical stimulation increases thirst.
- Electrical stimulation increases sodium appetite.
- Angiotensin II stimulation also increases ADH secretion.
- Angiotensin II stimulation also increases thirst.
- Angiotensin II stimulation also increases sodium appetite.
Osmoreceptors
- Neurons near the AV3V region and supraoptic nuclei act as osmoreceptors.
- These neurons are stimulated by small increases in extracellular fluid osmolarity.
- Osmoreceptors send nerve signals to the supraoptic nuclei.
- These signals regulate firing of the supraoptic nuclei.
- These signals regulate ADH secretion.
- Osmoreceptors likely stimulate thirst when extracellular fluid osmolarity increases.
Special Feature of the Subfornical Organ and Organum Vasculosum
- Their blood vessels lack the typical blood-brain barrier.
- Ions and other solutes can move easily between blood and local interstitial fluid.
- Osmoreceptors rapidly detect changes in extracellular fluid osmolarity.
- Osmoreceptors strongly control ADH secretion.
- Osmoreceptors strongly control thirst.
KEY CONCEPT
- ADH is synthesized in the hypothalamus.
- ADH is released from the posterior pituitary.
- Supraoptic nuclei produce ≈83% of ADH.
- Paraventricular nuclei produce ≈17% of ADH.
- ↑ Osmolarity → ↑ Nerve Activity → ↑ Calcium Entry → ↑ ADH Release.
- AV3V region helps control ADH, thirst, sodium appetite, and blood pressure.
- Osmoreceptors detect osmolarity changes and stimulate ADH secretion and thirst.
Easy Flow
↑ Osmolarity → Osmoreceptors Activated → Supraoptic & Paraventricular Nuclei Stimulated → ↑ Calcium Entry → ADH Released from Posterior Pituitary → Bloodstream → Kidneys → Water Conservation
ADH (Antidiuretic Hormone) Regulation — Simplest Concept
🎯 Main Idea
The body constantly checks:
- How concentrated the blood is (osmolarity)
- How much blood volume/pressure is present
If the body senses dehydration, high osmolarity, or low blood volume, it releases ADH.
ADH tells the kidneys:
➡️ “Save water, don’t lose it in urine.”
Step 1: Sensors Detect a Problem
A. Osmoreceptors (Most Important)
📍 Located in the hypothalamus
They monitor blood concentration.
When activated?
- Water loss (sweating)
- Dehydration
- High plasma osmolarity
- High sodium concentration
Message:
🗣️ “Blood is too concentrated! Save water!”
B. Baroreceptors & Cardiopulmonary Receptors
📍 Located in:
- Large blood vessels
- Heart
They monitor:
- Blood pressure
- Blood volume
When activated?
- Hemorrhage (blood loss)
- Severe dehydration
- Low blood pressure
Message:
🗣️ “Blood volume is falling! Save water!”
Step 2: Hypothalamus Produces ADH
Two special neurons in the hypothalamus make ADH:
1. Supraoptic Nucleus
⭐ Major source of ADH
2. Paraventricular Nucleus
⭐ Also produces ADH
Think:
Osmoreceptors/Baroreceptors → Hypothalamic Neurons → ADH Production
Step 3: ADH Travels to Posterior Pituitary
ADH is:
✅ Synthesized in hypothalamic neurons
❌ Not synthesized in pituitary
It travels down nerve fibers to the:
📍 Posterior Pituitary
where it is stored and released into blood.
Step 4: ADH Acts on Kidneys
ADH reaches:
📍 Distal Tubules
📍 Collecting Ducts
Effect:
More water channels (Aquaporins) are inserted.
Result:
💧 More water reabsorbed into blood
💧 Less water lost in urine
Final Result
With ADH
✅ Water retained in body
✅ Blood volume increases
✅ Plasma osmolarity decreases
✅ Blood pressure improves
Urine becomes:
❌ Small volume
✅ Highly concentrated
Easy Flow Chart
Dehydration / ↑ Osmolarity / ↓ Blood Volume
↓
Osmoreceptors & Baroreceptors
↓
Hypothalamus
(Supraoptic + Paraventricular Nuclei)
↓
ADH Produced
↓
Posterior Pituitary
↓
ADH Released
↓
Kidneys
↓
↑ Water Reabsorption
↓
↓ Urine Volume + ↑ ConcentrationKEY CONCEPT
ADH is synthesized in the supraoptic and paraventricular nuclei of the hypothalamus, stored and released from the posterior pituitary, and acts on the distal tubules and collecting ducts of the kidneys to increase water reabsorption, producing a small volume of concentrated urine.
Stimulation of ADH Release By Decreased Arterial Pressure and/or Decreased Blood Volume
- ADH release is also controlled by cardiovascular reflexes.
- These reflexes respond to decreases in blood pressure.
- These reflexes respond to decreases in blood volume.
Types of Reflexes Involved
- Arterial Baroreceptor Reflexes
- Cardiopulmonary Reflexes
Origin of These Reflexes
- These reflex pathways begin in high-pressure areas of the circulation.
- High-pressure areas include the aortic arch.
- High-pressure areas include the carotid sinus.
- These reflex pathways also begin in low-pressure areas of the circulation.
- Low-pressure areas are mainly located in the cardiac atria.
Nerve Pathway
- Sensory (afferent) signals travel through the vagus nerve.
- Sensory (afferent) signals also travel through the glossopharyngeal nerve.
- These signals synapse in the nuclei of the tractus solitarius.
- Signals are then relayed to hypothalamic nuclei.
- These hypothalamic nuclei control ADH synthesis.
- These hypothalamic nuclei control ADH secretion.
Stimuli That Increase ADH Secretion
- Increased osmolarity increases ADH secretion.
- Decreased arterial pressure increases ADH secretion.
- Decreased blood volume increases ADH secretion.
During Hemorrhage
- Hemorrhage decreases blood pressure.
- Hemorrhage decreases blood volume.
- ADH secretion increases.
- Increased ADH causes more water reabsorption by the kidneys.
- More water is retained in the body.
- Blood pressure moves back toward normal.
- Blood volume moves back toward normal.
KEY CONCEPT
Three Major Stimuli for ADH Release
- ↑ Osmolarity
- ↓ Arterial Pressure
- ↓ Blood Volume
Easy Flow
Hemorrhage → ↓ Blood Pressure + ↓ Blood Volume → Cardiovascular Reflexes Activated → Hypothalamus Stimulated → ↑ ADH Release → ↑ Water Reabsorption by Kidneys → Blood Pressure & Blood Volume Return Toward Normal
Quantitative Importance of Osmolarity and Cardiovascular Reflexes in Stimulating ADH Secretion
- A decrease in effective blood volume stimulates ADH secretion.
- An increase in extracellular fluid osmolarity stimulates ADH secretion.
Sensitivity of ADH Secretion
- ADH is much more sensitive to changes in osmolarity than to changes in blood volume.
- Even a small change in osmolarity can increase ADH secretion.
Effect of Osmolarity
- A 1% increase in plasma osmolarity is enough to increase ADH levels.
Effect of Blood Volume
- After blood loss, ADH levels do not increase significantly at first.
- Blood volume must decrease by about 10% before ADH levels rise appreciably.
Severe Blood Volume Loss
- When blood volume decreases further, ADH levels rise rapidly.
- In severe blood volume depletion, cardiovascular reflexes become very important for ADH secretion.
Daily Regulation of ADH
- During simple dehydration, ADH secretion is controlled mainly by changes in plasma osmolarity.
- Osmolarity is the major day-to-day regulator of ADH release.
Combined Effect
- Decreased blood volume enhances the ADH response to increased osmolarity.
- Decreased blood pressure enhances the ADH response to increased osmolarity.
KEY CONCEPT
ADH Sensitivity Comparison
- 1% ↑ Plasma Osmolarity → ↑ ADH Secretion
- 10% ↓ Blood Volume → Significant ↑ ADH Secretion
Main Controller in Daily Life
- Simple Dehydration → Osmolarity is the main stimulus for ADH release
During Severe Blood Loss
- Severe ↓ Blood Volume → Cardiovascular Reflexes become the major stimulus for ADH release
Easy Comparison
| Stimulus | ADH Response |
|---|---|
| 1% ↑ Osmolarity | ADH increases |
| 10% ↓ Blood Volume | ADH begins to increase significantly |
| Severe ↓ Blood Volume | Rapid and marked ADH increase |
Easy Flow
Simple Dehydration → ↑ Osmolarity → ↑ ADH
Severe Hemorrhage → Large ↓ Blood Volume → Cardiovascular Reflexes Activated → Marked ↑ ADH
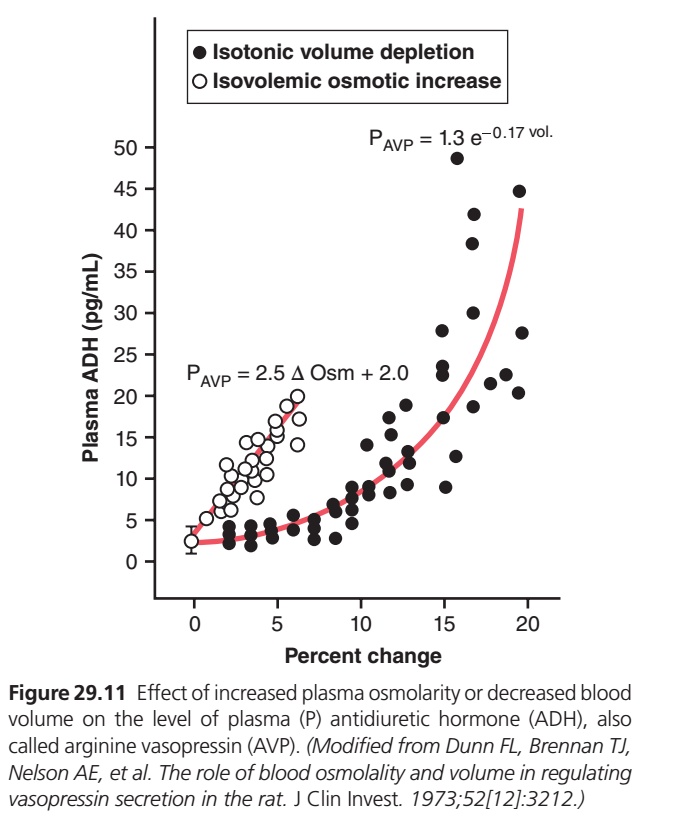
Figure 29.11 — ADH Secretion: Osmolarity vs Blood Volume Regulation (Simplest Explanation)
🎯 What Is This Graph Showing?
This graph compares two different stimuli that increase ADH secretion:
⚪ White Circles
Increase in Plasma Osmolarity
- Blood becomes more concentrated.
- Water is lost but blood volume remains nearly normal.
- Called Isovolemic Osmotic Increase.
⚫ Black Circles
Decrease in Blood Volume
- Blood volume falls.
- Example: hemorrhage, severe dehydration.
- Called Isotonic Volume Depletion.
The graph shows how much ADH (AVP) is released in each situation.
Understanding the Axes
X-Axis (Horizontal)
Percent Change
This shows how much the stimulus changes.
For example:
| Value | Meaning |
|---|---|
| 0% | Normal condition |
| 5% | Small increase/decrease |
| 10% | Moderate change |
| 20% | Large change |
Y-Axis (Vertical)
Plasma ADH (pg/mL)
Shows the amount of ADH in blood.
| ADH Level | Meaning |
|---|---|
| Low | Little water conservation |
| High | Strong water conservation |
| Very High | Emergency water conservation |
⚪ WHITE CIRCLES
Effect of Increased Osmolarity
What do the white circles represent?
Each white circle is an experimental measurement showing:
➡️ How much ADH was released when plasma osmolarity increased.
What happens?
As osmolarity increases:
- Blood becomes more concentrated.
- Osmoreceptors detect it.
- ADH secretion increases.
The increase is:
📈 Almost a straight-line increase
White Line Equation
PAVP=2.5ΔOsm+2.0
What does this mean?
PAVP
Amount of ADH in blood.
Δ Osm
Change in osmolarity.
2.5
For every 1-unit increase in osmolarity:
ADH increases by approximately 2.5 pg/mL.
+2.0
Even at normal osmolarity there is a small baseline ADH secretion.
Easy Concept
↑ Osmolarity
↓
Osmoreceptors stimulated
↓
ADH increases steadilyKey Point
Small changes in osmolarity produce noticeable increases in ADH.
⚫ BLACK CIRCLES
Effect of Decreased Blood Volume
What do black circles represent?
Each black circle is an experimental measurement showing:
➡️ How much ADH was released when blood volume decreased.
What happens initially?
Look at the left side of black circles.
Even when blood volume decreases slightly:
- ADH changes very little.
Example:
0–5% volume loss
ADH remains around:
2–5 pg/mL
Why?
Baroreceptors are not very sensitive to small volume changes.
The body can tolerate minor volume loss.
What Happens After Significant Volume Loss?
When volume loss becomes larger:
- Around 10–15%
- Baroreceptors fire strongly
- Hypothalamus becomes highly stimulated
ADH secretion rises dramatically.
Look at the Red Curved Line
The red curve through the black circles represents the average response.
Notice:
First Part
Almost flat.
Small volume loss
↓
Little ADH increaseLater Part
Very steep.
Large volume loss
↓
Massive ADH increaseBlack Line Equation
PAVP=1.3e−0.17(vol)
(Demonstrates an exponential relationship.)
What does exponential mean?
ADH does NOT increase evenly.
Instead:
5% volume loss
↓
Small ADH rise
10% volume loss
↓
Moderate ADH rise
15–20% volume loss
↓
Huge ADH riseThe response becomes increasingly steep.
Why Does This Happen?
The body considers:
Increased Osmolarity
Important
But
Severe Blood Volume Loss
Life-threatening
Because:
- Blood pressure may collapse.
- Organs may not receive blood.
- Shock can occur.
Therefore:
When volume loss becomes severe,
🚨 ADH secretion skyrockets.
Comparison of White Circles vs Black Circles
| Feature | ⚪ White Circles | ⚫ Black Circles |
|---|---|---|
| Stimulus | Increased Osmolarity | Decreased Blood Volume |
| Receptors | Osmoreceptors | Baroreceptors |
| Pattern | Linear | Exponential |
| Sensitivity | Very High | Low initially |
| Small Changes Cause ADH Release? | Yes | No |
| Large Changes Cause Huge ADH Release? | Moderate | Yes |
| Main Function | Control Osmolarity | Emergency Volume Preservation |
Most Important Guyton Concept
ADH is more sensitive to osmolarity than blood volume.
A tiny increase in osmolarity (1–2%) can increase ADH secretion.
However, blood volume usually must fall by about 10% or more before ADH rises dramatically.
Final Exam Point
↑ Plasma Osmolarity
↓
Small change produces ADH release
↓
Linear increase (White Circles)
↓ Blood Volume
↓
Small losses cause little effect
↓
Large losses (>10–15%)
↓
Explosive ADH secretion
↓
Exponential increase (Black Circles)KEY CONCEPT
White circles show that ADH secretion increases almost linearly with small increases in plasma osmolarity, demonstrating very high sensitivity of osmoreceptors. Black circles show that ADH changes little with small blood volume losses but rises exponentially during severe volume depletion, demonstrating the powerful emergency response of baroreceptors to protect blood pressure and circulation.
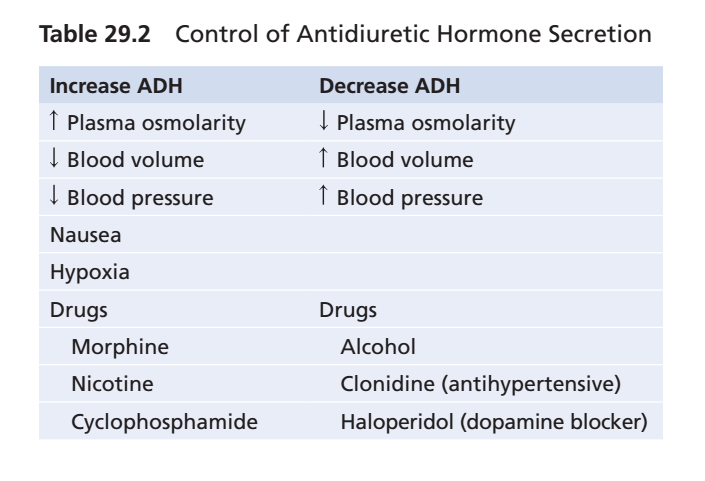
Other Stimuli for ADH Secretion
- ADH secretion can be increased by other stimuli acting on the central nervous system.
- ADH secretion can also be decreased by other stimuli acting on the central nervous system.
- Various drugs can increase or decrease ADH secretion.
- Various hormones can increase or decrease ADH secretion.
- Nausea is a powerful stimulus for ADH release.
- After vomiting, ADH levels may increase up to 100 times the normal level.
- Nicotine stimulates ADH release.
- Morphine stimulates ADH release.
- Alcohol inhibits ADH release.
- Marked diuresis can occur after alcohol ingestion.
- This increased urine production is partly due to inhibition of ADH release.
KEY CONCEPT
- Central nervous system stimuli can alter ADH secretion.
- Nausea → Strong increase in ADH release.
- Vomiting → ADH may increase up to 100× normal.
- Nicotine → ↑ ADH release.
- Morphine → ↑ ADH release.
- Alcohol → ↓ ADH release.
- Alcohol ingestion → Increased urine output (diuresis).
IMPORTANCE OF THIRST IN CONTROLLING EXTRACELLULAR FLUID OSMOLARITY AND SODIUM CONCENTRATION
- During water deficit, the kidneys minimize fluid loss through the osmoreceptor-ADH feedback system.
- Adequate fluid intake is also necessary.
- Fluid intake replaces fluid lost through sweating.
- Fluid intake replaces fluid lost through breathing.
- Fluid intake replaces fluid lost through the gastrointestinal tract.
- Fluid intake is regulated by the thirst mechanism.
- The thirst mechanism works together with the osmoreceptor-ADH mechanism.
- Together they maintain precise control of extracellular fluid osmolarity.
- Together they maintain precise control of sodium concentration.
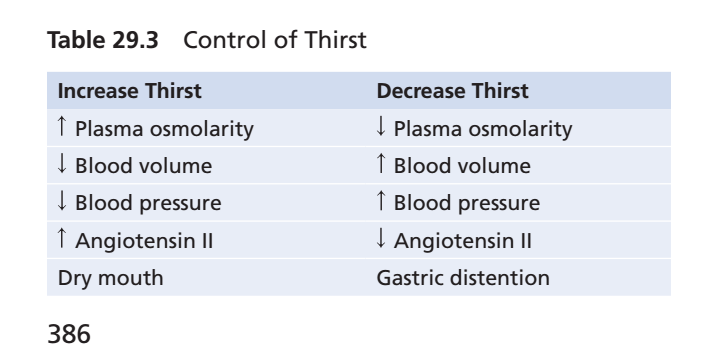
- Many of the same factors that stimulate ADH secretion also stimulate thirst.
- Thirst is the conscious desire for water.
Central Nervous System Centers for Thirst
- The same area along the anteroventral wall of the third ventricle that promotes ADH release also stimulates thirst.
- Another small area is located anterolaterally in the preoptic nucleus.
- Electrical stimulation of this area causes immediate drinking.
- Drinking continues as long as the stimulation continues.
- All these areas together are called the thirst center.
- Neurons in the thirst center respond to increased extracellular fluid sodium concentration.
- These neurons stimulate drinking behavior.
- These neurons likely function as osmoreceptors.
- They stimulate thirst in the same way that osmoreceptors stimulate ADH release.
- Increased osmolarity of the cerebrospinal fluid in the third ventricle promotes drinking.
- The organum vasculosum of the lamina terminalis is likely involved in this response.
- This structure lies beneath the ventricular surface.
- It is located at the inferior end of the AV3V region.
Stimuli for Thirst
1. Increased Extracellular Fluid Osmolarity
- Increased extracellular fluid osmolarity causes intracellular dehydration in the thirst centers.
- Intracellular dehydration stimulates the sensation of thirst.
- This response helps dilute extracellular fluid.
- This response helps return osmolarity toward normal.
2. Decreased Extracellular Fluid Volume and Arterial Pressure
- Decreased extracellular fluid volume stimulates thirst.
- Decreased arterial pressure stimulates thirst.
- This pathway is different from the pathway activated by increased plasma osmolarity.
- Blood loss due to hemorrhage stimulates thirst.
- Thirst can occur even when plasma osmolarity does not change.
- This stimulation probably occurs through neural input from cardiopulmonary baroreceptors.
- This stimulation probably occurs through neural input from systemic arterial baroreceptors.
3. Angiotensin II
- Angiotensin II is an important stimulus for thirst.
- Angiotensin II acts on the subfornical organ.
- Angiotensin II acts on the organum vasculosum of the lamina terminalis.
- These regions are outside the blood-brain barrier.
- Angiotensin II can diffuse into these tissues.
- Angiotensin II is stimulated by factors associated with hypovolemia.
- Angiotensin II is stimulated by factors associated with low blood pressure.
- Its effect on thirst helps restore blood volume toward normal.
- Its effect on thirst helps restore blood pressure toward normal.
- Angiotensin II also acts on the kidneys to decrease fluid excretion.
4. Dryness of the Mouth and Esophagus
- Dryness of the mouth can cause the sensation of thirst.
- Dryness of the esophageal mucous membranes can cause the sensation of thirst.
- A thirsty person may feel relief immediately after drinking water.
- This relief occurs before water is absorbed from the gastrointestinal tract.
- This relief occurs before extracellular fluid osmolarity changes.
5. Gastrointestinal and Pharyngeal Stimuli
- Gastrointestinal stimuli influence thirst.
- Pharyngeal stimuli influence thirst.
- In animals with an esophageal opening to the exterior, water is not absorbed into the blood.
- Partial relief of thirst still occurs after drinking.
- This relief is only temporary.
- Gastrointestinal distention may partially reduce thirst.
- Inflation of a balloon in the stomach can relieve thirst.
- Relief of thirst through gastrointestinal mechanisms is short-lived.
- Relief of thirst through pharyngeal mechanisms is short-lived.
- Thirst is completely satisfied only when plasma osmolarity returns to normal.
- Thirst is completely satisfied only when blood volume returns to normal.
- Animals and humans can accurately regulate fluid intake.
- This ability prevents overhydration.
- After drinking water, 30 to 60 minutes may be required for absorption and distribution throughout the body.
- If thirst were not temporarily relieved after drinking, excessive drinking could continue.
- Excessive drinking could lead to overhydration.
- Excessive drinking could cause excessive dilution of body fluids.
KEY CONCEPT
- Thirst works with the osmoreceptor-ADH system to regulate body fluid balance.
- The thirst center is located near the anteroventral wall of the third ventricle.
- Increased osmolarity is the most important stimulus for thirst.
- Decreased blood volume and blood pressure stimulate thirst.
- Angiotensin II stimulates thirst.
- Dry mouth stimulates thirst.
- Gastrointestinal and pharyngeal signals provide temporary relief of thirst.
- Thirst is completely satisfied only when osmolarity and/or blood volume return to normal.
- Temporary relief of thirst helps prevent overhydration.
Threshold for Osmolar Stimulus of Drinking
- The kidneys must continuously excrete a minimum amount of water.
- This occurs even in a dehydrated person.
- Water is needed to remove excess solutes taken in through food.
- Water is needed to remove excess solutes produced by metabolism.
- Water is lost by evaporation from the lungs.
- Water is lost through the gastrointestinal tract.
- Water is lost by evaporation from the skin.
- Water is lost through sweating.
- Therefore, the body always has a tendency toward dehydration.
- Dehydration increases extracellular fluid sodium concentration.
- Dehydration increases extracellular fluid osmolarity.
- The thirst mechanism is activated when sodium concentration rises about 2 mEq/L above normal.
- Activation of the thirst mechanism creates a desire to drink water.
- This level is called the threshold for drinking.
- Even small increases in plasma osmolarity stimulate drinking.
- Drinking helps restore extracellular fluid osmolarity toward normal.
- Drinking helps restore extracellular fluid volume toward normal.
- In this way, extracellular fluid osmolarity is precisely controlled.
- In this way, extracellular fluid sodium concentration is precisely controlled.
KEY CONCEPT
- The body continuously loses water through the kidneys, lungs, gastrointestinal tract, skin, and sweating.
- This creates a constant tendency toward dehydration.
- A rise in plasma sodium of about 2 mEq/L above normal activates the thirst mechanism.
- This level is called the threshold for drinking.
- Drinking restores extracellular fluid osmolarity and volume toward normal.
- Thirst helps maintain precise control of osmolarity and sodium concentration.
Disorders of Thirst and Water Intake
- Increased thirst occurs in various medical disorders.
- These disorders are often associated with increased urine volume (polyuria).
- These disorders are often associated with reduced extracellular fluid volume.
- Poorly controlled diabetes mellitus can cause increased thirst.
- Diabetes insipidus can cause increased thirst.
- Increased water intake acts as a compensatory response.
- Increased water intake helps correct increased plasma osmolarity.
- Increased water intake helps correct extracellular fluid volume depletion.
- Polydipsia means excessive thirst.
- Polydipsia can occur without known physiological stimuli for thirst.
- Psychogenic polydipsia is one type of excessive thirst.
- Psychogenic polydipsia may be caused by mental illnesses.
- Schizophrenia may cause psychogenic polydipsia.
- Obsessive-compulsive disorders may cause psychogenic polydipsia.
- Psychogenic polydipsia can lead to significant hyponatremia.
- Adipsia means absence of thirst.
- Adipsia can occur even when hypernatremia is present.
- Adipsia can occur even when volume depletion is present.
- Adipsia is rare.
- Adipsia usually results from lesions of the hypothalamic thirst centers.
- These lesions may be caused by trauma.
- These lesions may be caused by infection.
- These lesions may be caused by surgery.
- Partial deficiency of the thirst mechanism is called hypodipsia.
- Hypodipsia causes inadequate water intake.
- Inability to access water may also reduce water intake.
- Hypodipsia may occur in patients who have had a stroke.
- Hypodipsia may occur in older patients with dementia.
- Hypodipsia may occur in critically ill patients.
- Inadequate water intake leads to dehydration.
- Inadequate water intake leads to hypernatremia.
- Dehydration and hypernatremia occur despite large increases in ADH levels.
KEY CONCEPT
- Polyuria and extracellular fluid volume depletion → Increased thirst.
- Diabetes mellitus and diabetes insipidus → Increased thirst and water intake.
- Polydipsia = Excessive thirst.
- Psychogenic polydipsia → May occur in schizophrenia or obsessive-compulsive disorders.
- Psychogenic polydipsia → Can cause hyponatremia.
- Adipsia = Absence of thirst.
- Hypodipsia = Reduced thirst causing inadequate water intake.
- Hypothalamic lesions can cause adipsia.
- Inadequate water intake → Dehydration + Hypernatremia despite high ADH levels.
INTEGRATED RESPONSES OF OSMORECEPTOR-ADH AND THIRST MECHANISMS
- In a healthy person, the osmoreceptor-ADH mechanism and thirst mechanism work together.
- These mechanisms regulate extracellular fluid osmolarity precisely.
- These mechanisms regulate sodium concentration precisely.
- They continue to function despite constant dehydration challenges.
- These feedback systems can also handle additional challenges.
- High salt intake is one example of an additional challenge.
- These systems usually keep plasma osmolarity reasonably constant.
- Sodium intake can increase up to six times the normal amount.
- This causes only a small change in plasma sodium concentration.
- This occurs when both the ADH and thirst mechanisms are functioning normally.
- If the ADH mechanism fails, the thirst mechanism can still help control extracellular osmolarity.
- If the thirst mechanism fails, the ADH mechanism can still help control extracellular osmolarity.
- Either mechanism alone can control sodium concentration with reasonable effectiveness.
- Adequate fluid intake must be available.
- Fluid intake must replace the obligatory daily urine volume.
- Fluid intake must replace water lost through respiration.
- Fluid intake must replace water lost through sweating.
- Fluid intake must replace water lost through the gastrointestinal tract.
- Plasma sodium concentration becomes poorly controlled if both mechanisms fail at the same time.
- Plasma osmolarity becomes poorly controlled if both mechanisms fail at the same time.
- Increased sodium intake causes large changes in plasma sodium concentration when the ADH-thirst system is blocked.
- Without the ADH-thirst system, plasma sodium concentration cannot be adequately regulated.
- Without the ADH-thirst system, plasma osmolarity cannot be adequately regulated.
- No other feedback mechanism can adequately control plasma sodium concentration and osmolarity in the absence of both mechanisms.
KEY CONCEPT
- Osmoreceptor-ADH mechanism and thirst mechanism work together to control osmolarity and sodium concentration.
- These systems maintain near-normal plasma osmolarity even during high salt intake.
- If one mechanism fails, the other can still provide reasonable control.
- Adequate water intake is required for effective regulation.
- If both ADH and thirst mechanisms fail, plasma sodium concentration and osmolarity become poorly controlled.
- No other feedback system can adequately replace the combined ADH-thirst mechanisms.
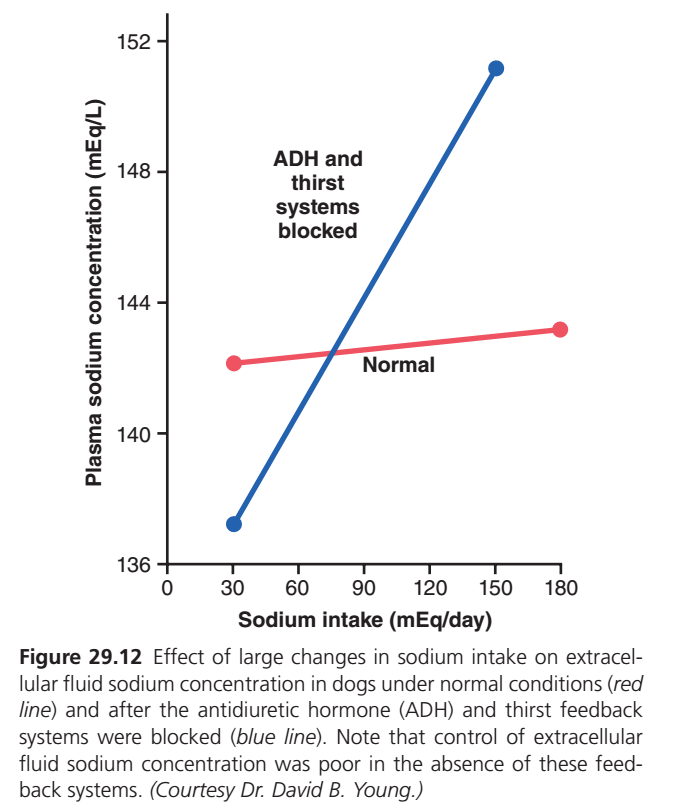
Figure 29.12 — Why ADH and Thirst Keep Plasma Sodium Almost Constant
🎯 Main Message of This Graph
This graph demonstrates:
Even when sodium intake changes enormously, plasma sodium concentration changes very little because the ADH and thirst mechanisms automatically maintain water balance.
Without ADH and thirst, plasma sodium concentration becomes poorly controlled.
Understanding the Axes
X-Axis (Horizontal)
Sodium Intake (mEq/day)
This shows how much sodium is consumed each day.
Left Side
30 mEq/day
- Low sodium intake
Right Side
180 mEq/day
- High sodium intake
So moving from left to right means:
➡️ Eating much more salt.
Y-Axis (Vertical)
Plasma Sodium Concentration (mEq/L)
This shows sodium concentration in extracellular fluid (blood plasma).
Normal range:
✅ About 135–145 mEq/L
Higher values mean:
- More concentrated body fluids
- Higher osmolarity
🔴 RED LINE = NORMAL PERSON
What does the red line represent?
A person with:
✅ Normal ADH system
AND
✅ Normal thirst mechanism
First Red Point
Sodium Intake = 30 mEq/day
Plasma sodium ≈ 142 mEq/L
This is normal.
Second Red Point
Sodium Intake = 180 mEq/day
Plasma sodium ≈ 143 mEq/L
Still normal.
What Happened?
Sodium intake increased:
30 → 180 mEq/dayThat is about:
6 times more sodiumYet plasma sodium changed only:
142 → 143 mEq/LAlmost no change!
Why Did Sodium Stay Constant?
When extra sodium is eaten:
Step 1
Plasma osmolarity rises slightly.
More sodium
↓
Higher osmolarityStep 2
Osmoreceptors detect it.
↑ Osmolarity
↓
Osmoreceptors stimulatedStep 3
ADH secretion increases.
↑ ADH
↓
Kidneys retain more waterStep 4
Thirst increases.
Person drinks more waterStep 5
Added water dilutes sodium.
More water retained
+
More water consumed
↓
Sodium concentration returns toward normal🔵 BLUE LINE = ADH and Thirst Blocked
What does the blue line represent?
Scientists experimentally blocked:
❌ ADH system
AND
❌ Thirst mechanism
The body could no longer correct sodium concentration.
First Blue Point
Sodium Intake = 30 mEq/day
Plasma sodium ≈ 137 mEq/L
Slightly lower than normal.
Second Blue Point
Sodium Intake = 150–180 mEq/day
Plasma sodium ≈ 151–152 mEq/L
Very high.
This represents:
⚠️ Hypernatremia
⚠️ Increased osmolarity
⚠️ Dehydrated cells
Why Did Sodium Rise So Much?
Normally:
Extra sodium
↓
ADH released
↓
Water retainedBut now:
Extra sodium
↓
No ADH response
↓
No extra water retainedAnd normally:
Extra sodium
↓
Thirst stimulated
↓
Drink waterBut now:
Extra sodium
↓
No thirst
↓
No extra water intakeResult
Sodium accumulates.
Water does not increase.
Therefore:
More sodium
+
Less water compensation
↓
Plasma sodium rises sharplyWhy Is the Blue Line So Steep?
Because there is no feedback control.
Normally:
↑ Sodium
↓
ADH + Thirst Activated
↓
Problem CorrectedBlocked condition:
↑ Sodium
↓
No ADH
No Thirst
↓
No Correction
↓
Sodium Keeps RisingTherefore the blue line climbs steeply.
Comparison of the Two Lines
| Feature | 🔴 Normal | 🔵 ADH & Thirst Blocked |
|---|---|---|
| ADH Present | Yes | No |
| Thirst Present | Yes | No |
| Water Retention | Yes | No |
| Water Drinking | Yes | No |
| Plasma Sodium Control | Excellent | Poor |
| Change in Sodium Concentration | Very Small | Very Large |
| Homeostasis | Maintained | Lost |
The Most Important Guyton Concept
The body does not primarily control sodium concentration by controlling sodium intake.
Instead, it controls sodium concentration by controlling water balance.
ADH Controls Water Output
ADH
↓
Water ReabsorptionThirst Controls Water Input
Thirst
↓
Water IntakeTogether they keep plasma sodium nearly constant.
Easy Flowchart
↑ Sodium Intake
↓
Slight ↑ Plasma Osmolarity
↓
Osmoreceptors Activated
↓
↑ ADH + ↑ Thirst
↓
More Water Retained
+
More Water Drunk
↓
Plasma Sodium Returns Near NormalKEY CONCEPT
The red line shows that even a sixfold increase in sodium intake causes only a tiny change in plasma sodium concentration because ADH and thirst mechanisms automatically increase water retention and water intake. The blue line shows that when ADH and thirst are blocked, plasma sodium rises dramatically, proving that these two feedback systems are the body’s most important regulators of extracellular fluid osmolarity and sodium concentration.
Role of Angiotensin II and Aldosterone in Controlling Extracellular Fluid Osmolarity and Sodium Concentration
- Angiotensin II and aldosterone play important roles in regulating sodium reabsorption by the renal tubules.
- Low sodium intake increases levels of angiotensin II and aldosterone.
- Increased levels of these hormones stimulate sodium reabsorption by the kidneys.
- This prevents large sodium losses.
- Sodium intake may decrease to as low as 10% of normal.
- Even then, sodium losses are minimized.
- High sodium intake decreases formation of angiotensin II and aldosterone.
- Reduced hormone levels allow the kidneys to excrete large amounts of sodium.
- Angiotensin II and aldosterone are important in regulating sodium excretion.
- They do not play a major role in regulating extracellular fluid sodium concentration.
- These hormones increase the amount of sodium in the extracellular fluid.
- They also increase extracellular fluid volume.
- They increase water reabsorption along with sodium reabsorption.
- Therefore, sodium concentration changes very little.
- Angiotensin II and aldosterone have little effect on sodium concentration under normal conditions.
- Plasma sodium concentration remains well regulated even when the aldosterone feedback system is blocked.
- Increasing sodium intake more than 6-fold changes plasma sodium concentration by only about 1% to 2%.
- This occurs under normal conditions.
- This also occurs when the aldosterone feedback system is blocked.
- Plasma sodium concentration can remain well regulated without a functional aldosterone feedback system.
- Similar results occur when angiotensin II formation is blocked.
- There are two main reasons why angiotensin II and aldosterone have little effect on plasma sodium concentration.
First Reason
- Angiotensin II and aldosterone increase sodium reabsorption.
- Angiotensin II and aldosterone increase water reabsorption.
- Extracellular fluid volume increases.
- Total body sodium increases.
- Sodium concentration changes very little.
Second Reason
- The ADH-thirst mechanism remains functional.
- Any tendency for plasma sodium concentration to increase stimulates compensation.
- Water intake increases.
- ADH secretion increases.
- Extracellular fluid becomes diluted.
- Plasma sodium concentration moves back toward normal.
- The ADH-thirst system is much more important than the angiotensin II and aldosterone systems for regulating sodium concentration under normal conditions.
- Patients with primary aldosteronism have very high aldosterone levels.
- Plasma sodium concentration usually increases only about 3 to 5 mEq/L above normal.
- Complete loss of aldosterone secretion can occur after adrenalectomy.
- Complete loss of aldosterone secretion can occur in Addison disease.
- These conditions cause tremendous sodium loss by the kidneys.
- Large sodium losses can markedly reduce plasma sodium concentration.
- Large sodium losses eventually cause severe volume depletion.
- Large sodium losses eventually cause decreased blood pressure.
- These changes activate the thirst mechanism through cardiovascular reflexes.
- Activation of thirst increases water intake.
- Increased water intake causes further dilution of plasma sodium concentration.
- Increased water intake helps reduce the decrease in body fluid volume.
- Under extreme conditions, plasma sodium concentration may change significantly.
- This can occur even when the ADH-thirst mechanism is functioning.
- The ADH-thirst mechanism is the most powerful feedback system for controlling extracellular fluid osmolarity.
- The ADH-thirst mechanism is the most powerful feedback system for controlling sodium concentration.
KEY CONCEPT
- Angiotensin II and aldosterone regulate sodium reabsorption by the kidneys.
- Low sodium intake → ↑ Angiotensin II + ↑ Aldosterone → ↑ Sodium reabsorption.
- High sodium intake → ↓ Angiotensin II + ↓ Aldosterone → ↑ Sodium excretion.
- These hormones increase both sodium and water reabsorption.
- Therefore, extracellular fluid volume increases but sodium concentration changes very little.
- The ADH-thirst system is the main regulator of plasma osmolarity and sodium concentration.
- Primary aldosteronism usually increases plasma sodium by only 3–5 mEq/L.
- Loss of aldosterone can cause severe sodium loss and decreased plasma sodium concentration.
- The ADH-thirst mechanism is the most powerful system controlling extracellular fluid osmolarity and sodium concentration.
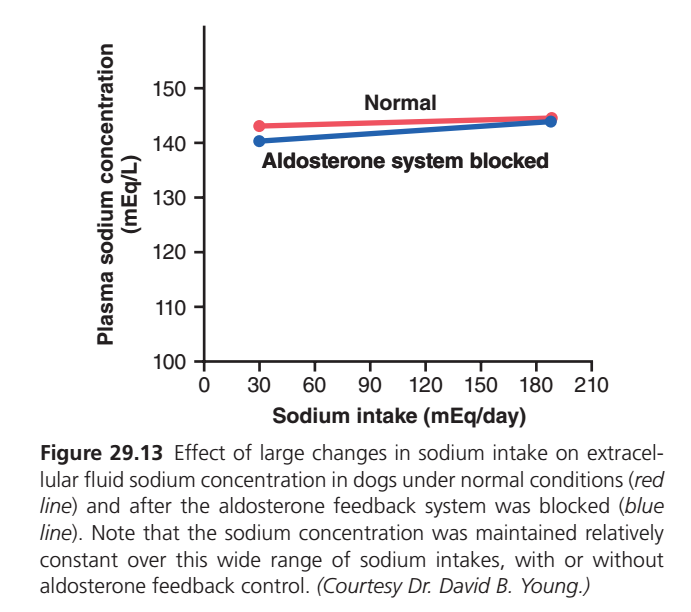
Figure 29.13 — Aldosterone vs Plasma Sodium Concentration (Easiest Concept)
🎯 Main Message of This Graph
This graph shows:
Even if the aldosterone system is completely blocked, plasma sodium concentration remains almost normal.
This means:
✅ Aldosterone is NOT the main regulator of plasma sodium concentration.
Instead:
✅ ADH and thirst are the major regulators of plasma sodium concentration and osmolarity.nderstanding the Axes
X-Axis (Horizontal)
Sodium Intake (mEq/day)
Shows how much sodium is eaten each day.
Left Side
30 mEq/day
Low sodium intake
Right Side
180 mEq/day
High sodium intake
So moving from left to right means:
➡️ Eating much more salt.
Y-Axis (Vertical)
Plasma Sodium Concentration (mEq/L)
Shows sodium concentration in blood plasma.
Normal value:
135–145 mEq/LThe body tries to keep this constant.
🔴 RED LINE = Normal Person
This line represents:
✅ Normal aldosterone system
✅ Normal kidneys
First Red Dot
Sodium Intake = 30 mEq/day
Plasma sodium ≈ 143 mEq/L
Normal.d Red Dot
Sodium Intake = 180 mEq/day
Plasma sodium ≈ 145 mEq/L
Still normal.
What Does This Mean?
Even though sodium intake increased about:
30 → 180 mEq/day(about 6 times higher)
Plasma sodium changed only:
143 → 145 mEq/LVery little change.
🔵 BLUE LINE = Aldosterone System Blocked
This line represents:
❌ No aldosterone feedback
The kidneys cannot use aldosterone to regulate sodium reabsorption normally.
First Blue Dot
Sodium Intake = 30 mEq/day
Plasma sodium ≈ 140–141 mEq/L
Slightly lower.
Second Blue Dot
Sodium Intake = 180 mEq/day
Plasma sodium ≈ 144–145 mEq/L
Still almost normal.
What Is Surprising?
Even without aldosterone:
Low sodium intake
↓
Plasma sodium ≈ Normal
High sodium intake
↓
Plasma sodium ≈ NormalThe blue line stays almost flat.
Compare the Two Lines
Notice:
Red Line (Normal)
143 → 145 mEq/LSmall change.
Blue Line (No Aldosterone)
140 → 144 mEq/LAlso a small change.
The two lines are very close together.
This means:
➡️ Aldosterone has only a small effect on plasma sodium concentration.
Why Doesn’t Plasma Sodium Change Much?
Many students think:
More aldosterone
↓
More sodium retained
↓
Huge rise in plasma sodiumThis is WRONG.hat Actually Happens?
When aldosterone retains sodium:
Na+ retained
↓
Water follows sodium
↓
Both increase togetherSo:
Sodium amount ↑
Water amount ↑Because both increase together:
Concentration changes very littleEasy Example
Imagine:
Before
100 sodium particles
100 water moleculesConcentration remains balanced.
After Aldosterone
120 sodium particles
120 water moleculesBoth increased together.
Result:
Concentration nearly unchangedThen What Does Aldosterone Actually Control?
Aldosterone mainly controls:
Total Body Sodium Content
Aldosterone
↓
Na+ retentionExtracellular Fluid Volume
Na+ retained
↓
Water retained
↓
ECF volume increasesBlood Volume
ECF volume ↑
↓
Blood volume ↑Blood Pressure
Blood volume ↑
↓
Blood pressure ↑What Controls Sodium Concentration?
The major regulators are:
ADH
Controls:
Water outputThirst
Controls:
Water intakeTogether they determine:
Plasma osmolarity
Plasma sodium concentrationComparison: Aldosterone vs ADH
| Feature | Aldosterone | ADH |
|---|---|---|
| Main Action | Retains Sodium | Retains Water |
| Controls Plasma Sodium Concentration? | Very Little | Major Control |
| Controls ECF Volume? | Yes | Slightly |
| Controls Blood Volume? | Yes | Yes |
| Controls Osmolarity? | Minimal | Major |
| Controls Sodium Content? | Major | Minimal |
Important Guyton Concept
Aldosterone regulates:
Total body sodium
↓
ECF volume
↓
Blood volume
↓
Blood pressureADH regulates:
Water balance
↓
Plasma osmolarity
↓
Plasma sodium concentrationEasy Flowchart
Aldosterone ↑
↓
Na+ Reabsorption ↑
↓
Water Follows Na+
↓
ECF Volume ↑
↓
Blood Volume ↑
↓
Blood Pressure ↑But
Na+ and Water increase together
↓
Plasma Sodium Concentration
Changes Very LittleKEY CONCEPT
This graph shows that plasma sodium concentration remains nearly constant whether the aldosterone system is functioning or blocked. Aldosterone primarily regulates total body sodium content, extracellular fluid volume, blood volume, and blood pressure—not plasma sodium concentration. Plasma sodium concentration is mainly controlled by ADH and the thirst mechanism through regulation of body water.
Salt-Appetite Mechanism for Controlling Extracellular Fluid Sodium Concentration and Volume
- Maintenance of normal extracellular fluid volume requires a balance between sodium intake and sodium excretion.
- Maintenance of normal extracellular fluid sodium concentration requires a balance between sodium intake and sodium excretion.
- In most people, sodium intake is much greater than required for homeostasis.
- People in industrialized societies usually consume processed foods.
- Average sodium intake is usually 100–200 mEq/day.
- Humans can survive normally while consuming only 10–20 mEq/day of sodium.
- High sodium intake may contribute to cardiovascular disorders.
- High sodium intake may contribute to hypertension.
- Salt appetite occurs partly because humans and animals naturally like salt.
- Salt may be consumed even when there is no sodium deficiency.
- Salt appetite also has a regulatory component.
- A sodium deficiency creates a behavioral drive to obtain salt.
- This behavioral drive is especially important in herbivores.
- Herbivores naturally consume a low-sodium diet.
- Salt craving may also be important in humans.
- Salt craving is especially important during severe sodium deficiency.
- Severe sodium deficiency occurs in Addison disease.
- Addison disease causes deficiency of aldosterone secretion.
- Aldosterone deficiency causes excessive sodium loss in urine.
- Excessive sodium loss decreases extracellular fluid volume.
- Excessive sodium loss decreases sodium concentration.
- Both changes stimulate the desire for salt.
- The main stimuli for increased salt appetite are associated with sodium deficiency.
- Decreased blood volume increases salt appetite.
- Decreased blood pressure increases salt appetite.
- Circulatory insufficiency increases salt appetite.
- The neuronal mechanism for salt appetite is similar to the thirst mechanism.
- Some neuronal centers in the AV3V region are involved in salt appetite.
- Lesions in the AV3V region often affect thirst and salt appetite together.
- Low blood pressure activates circulatory reflexes.
- Decreased blood volume activates circulatory reflexes.
- These reflexes influence thirst and salt appetite simultaneously.
KEY CONCEPT
- Normal sodium balance requires sodium intake = sodium excretion.
- Average sodium intake = 100–200 mEq/day.
- Humans can survive on 10–20 mEq/day of sodium.
- High sodium intake may contribute to hypertension.
- Salt appetite increases when sodium deficiency occurs.
- Addison disease → ↓ Aldosterone → ↑ Sodium loss → ↓ ECF Volume + ↓ Sodium Concentration → ↑ Salt Craving.
- Major stimuli for salt appetite:
- Sodium deficiency
- ↓ Blood volume
- ↓ Blood pressure
- Circulatory insufficiency
- Salt appetite and thirst share similar brain mechanisms in the AV3V region.