


- The countercurrent multiplier mechanism depends on the special arrangement of the loops of Henle and vasa recta.
- The vasa recta are specialized peritubular capillaries located in the renal medulla.
- In humans, about 25% of nephrons are juxtamedullary nephrons.
- These juxtamedullary nephrons have loops of Henle that extend deep into the medulla before returning to the cortex.
- These juxtamedullary nephrons also have vasa recta that extend deep into the medulla before returning to the cortex.
- Some loops of Henle extend all the way to the tips of the renal papillae.
- The renal papillae project from the medulla into the renal pelvis.
- The vasa recta run parallel to the long loops of Henle.
- The vasa recta also descend into the medulla before returning to the renal cortex.
- The collecting ducts carry urine through the hyperosmotic renal medulla before urine is excreted.
- The collecting ducts also play a critical role in the countercurrent mechanism.
KEY CONCEPT
- The countercurrent multiplier mechanism depends on:
- Loops of Henle
- Vasa recta
- Collecting ducts
- About 25% of nephrons are juxtamedullary nephrons.
- Long loops of Henle and vasa recta extend deep into the medulla.
- Collecting ducts pass through the hyperosmotic medulla before urine is excreted.
- All three structures are essential for the countercurrent mechanism.
COUNTERCURRENT MULTIPLIER PRODUCES HYPEROSMOTIC RENAL MEDULLARY INTERSTITIUM
- The osmolarity of interstitial fluid in most parts of the body is about 300 mOsm/L.
- This osmolarity is similar to plasma osmolarity.
- The corrected osmolar activity is about 282 mOsm/L.
- The osmolarity of the interstitial fluid in the renal medulla is much higher.
- The osmolarity in the renal medulla may gradually increase to about 1200–1400 mOsm/L at the pelvic tip of the medulla.
- This high osmolarity means that the renal medullary interstitium contains a large amount of solutes compared with water.
- Once a high solute concentration is established in the medulla, it is maintained.
- Maintenance occurs through a balanced inflow and outflow of solutes and water in the medulla.
- Several factors contribute to the buildup of solute concentration in the renal medulla.
- Active transport of sodium ions occurs from the thick ascending limb of the loop of Henle into the medullary interstitium.
- Potassium, chloride, and other ions are co-transported from the thick ascending limb into the medullary interstitium.
- Active transport of ions also occurs from the collecting ducts into the medullary interstitium.
- Urea moves from the inner medullary collecting ducts into the medullary interstitium by facilitated diffusion.
- Only small amounts of water diffuse from the medullary tubules into the medullary interstitium.
- Water diffusion is much less than the amount of solute reabsorbed into the medullary interstitium.
KEY CONCEPT
- Most body interstitial fluid has an osmolarity of about 300 mOsm/L.
- Renal medullary interstitial osmolarity increases up to 1200–1400 mOsm/L.
- The medulla becomes hyperosmotic because solutes accumulate in excess of water.
- Major contributors to medullary hyperosmolarity:
- Active transport of Na⁺, K⁺, Cl⁻, and other ions from the thick ascending limb.
- Active transport of ions from collecting ducts.
- Facilitated diffusion of urea from inner medullary collecting ducts.
- Very little water movement compared with solute reabsorption.
- The countercurrent multiplier mechanism creates and maintains the hyperosmotic renal medulla.
LOOP OF HENLE PUMPS SOLUTES INTO THE RENAL MEDULLA
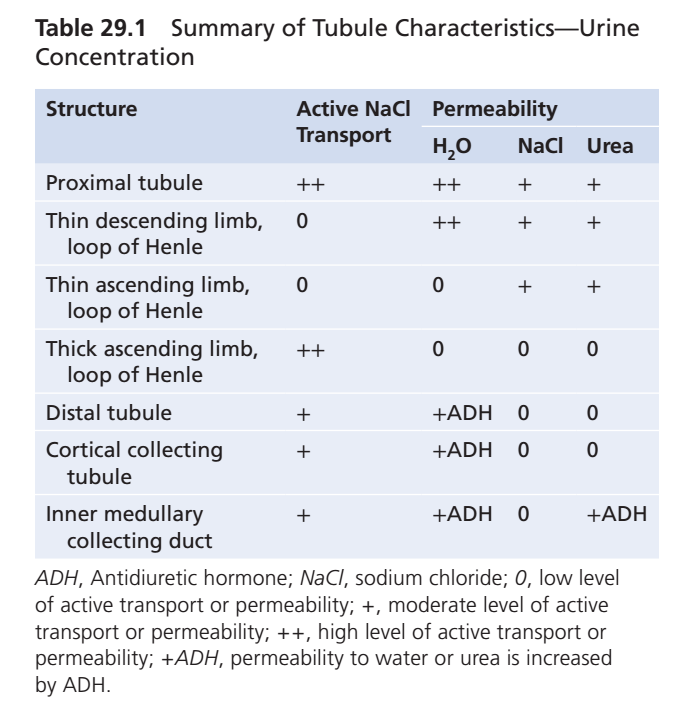
- The transport characteristics of the loops of Henle are summarized in Table 29.1.
- Table 29.1 also includes the properties of:
- Proximal tubules
- Distal tubules
- Cortical collecting tubules
- Inner medullary collecting ducts
- A major reason for the high osmolarity of the renal medulla is the active transport of sodium from the thick ascending limb of the loop of Henle into the interstitium.
- Potassium, chloride, and other ions are co-transported with sodium into the interstitium.
- This transport system can establish about a 200-mOsm/L concentration gradient between the tubular lumen and the interstitial fluid.
- The thick ascending limb is virtually impermeable to water.
- The solutes pumped out are not followed by osmotic movement of water into the interstitium.
- Active transport of sodium and other ions from the thick ascending limb adds solutes to the renal medullary interstitium without adding water.
- This adds solutes in excess of water to the renal medullary interstitium.
- Some sodium chloride is passively reabsorbed from the thin ascending limb of the loop of Henle.
- The thin ascending limb is also essentially impermeable to water.
- This passive sodium chloride reabsorption further increases the solute concentration of the renal medullary interstitium.
- The descending limb of the loop of Henle is very permeable to water.
- The descending limb differs from the ascending limb in its high water permeability.
- The osmolarity of the tubular fluid in the descending limb quickly becomes equal to the osmolarity of the renal medulla.
- Water diffuses out of the descending limb into the interstitium.
- As tubular fluid flows toward the tip of the loop of Henle, its osmolarity gradually increases.
KEY CONCEPT
- The thick ascending limb actively pumps Na⁺, K⁺, Cl⁻, and other ions into the medullary interstitium.
- The thick ascending limb is impermeable to water.
- Solutes leave the tubule, but water does not follow.
- The thin ascending limb passively reabsorbs NaCl and is also impermeable to water.
- The descending limb is highly permeable to water.
- Water leaves the descending limb and enters the medullary interstitium.
- As fluid moves down the descending limb, it becomes progressively more concentrated.
STEPS INVOLVED IN CAUSING HYPEROSMOTIC RENAL MEDULLARY INTERSTITIUM
- To understand how the renal medulla becomes hyperosmotic, consider the transport properties of the loop of Henle.
- First, assume that the loop of Henle contains fluid with an osmolarity of 300 mOsm/L.
- This is the same osmolarity as the fluid leaving the proximal tubule.
- Next, the active ion pump in the thick ascending limb transports ions out of the tubule.
- This decreases the electrolyte concentration inside the tubule.
- This increases the solute concentration in the interstitial fluid.
- The pump establishes about a 200-mOsm/L concentration gradient between the tubular fluid and interstitial fluid.
- The concentration gradient is limited to about 200 mOsm/L.
- Paracellular diffusion of ions back into the tubule eventually balances the transport of ions out of the tubule.
- In the next step, water moves out of the descending limb by osmosis.
- Because of water movement, the tubular fluid in the descending limb and the interstitial fluid quickly reach osmotic equilibrium.
- The interstitial osmolarity remains at 400 mOsm/L because ions continue to be transported out of the thick ascending limb.
- By itself, active transport of sodium chloride from the thick ascending limb can create only a 200-mOsm/L concentration gradient.
- This gradient is much smaller than the final gradient produced by the countercurrent multiplier system.
- Additional fluid then enters the loop of Henle from the proximal tubule.
- This pushes the previously concentrated fluid in the descending limb into the ascending limb.
- When this fluid enters the ascending limb, more ions are pumped into the interstitium.
- Water remains inside the tubular fluid.
- A new 200-mOsm/L gradient is established.
- The osmolarity of the interstitial fluid increases to 500 mOsm/L.
- Once again, fluid in the descending limb reaches equilibrium with the hyperosmotic medullary interstitial fluid.
- As concentrated fluid from the descending limb enters the ascending limb, more solute is pumped into the medullary interstitium.
- These steps continue repeatedly.
- The overall effect is the addition of more solute to the medulla than water.
- Over time, solutes gradually become concentrated in the renal medulla.
- The concentration gradient created by active ion pumping becomes progressively larger.
- Eventually, the osmolarity of the medullary interstitial fluid rises to about 1200–1400 mOsm/L.
- The repeated reabsorption of sodium chloride from the thick ascending limb and the continued delivery of new sodium chloride from the proximal tubule is called the countercurrent multiplier.
- Sodium chloride reabsorbed from the ascending limb is continuously added to newly arriving sodium chloride.
- This process multiplies the concentration of solutes in the medullary interstitium.
- After a high solute concentration is established in the renal medulla, the countercurrent multiplier reaches its limit.
- At this point, inflow and outflow of solutes and water become balanced.
- No further increase in medullary interstitial osmolarity occurs.
KEY CONCEPT
- Fluid enters the loop of Henle at 300 mOsm/L.
- The thick ascending limb actively pumps NaCl into the interstitium.
- This creates a maximum 200-mOsm/L gradient between tubular fluid and interstitial fluid.
- The descending limb is permeable to water, so water leaves until osmotic equilibrium is reached.
- Continuous flow of new fluid from the proximal tubule pushes concentrated fluid through the loop.
- Repeated cycles continuously add solutes to the medulla without adding equivalent water.
- This “multiplies” the medullary osmotic gradient.
- The countercurrent multiplier eventually increases medullary osmolarity to about 1200–1400 mOsm/L.
- Once maximum concentration is reached, solute and water inflow equal outflow, and no further increase occurs.
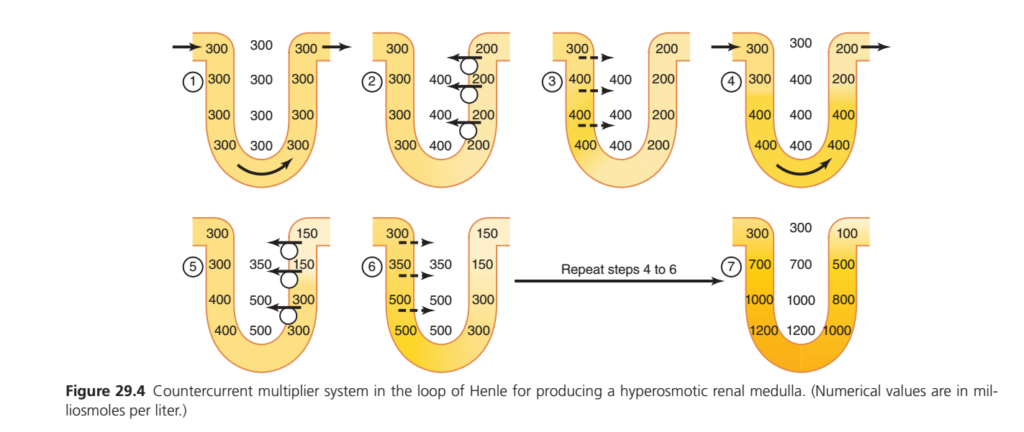
Countercurrent Multiplier System (Figure 29.4) – Easiest Concept Ever
🎯 Main Goal of This Figure
The kidney wants to create a very concentrated renal medulla so that later (when ADH is present) it can reabsorb water and make concentrated urine.
Final Result
The medulla becomes:
300 → 700 → 1000 → 1200 mOsm/L
This is achieved by the Countercurrent Multiplier of the Loop of Henle.
Golden Rule to Remember
Descending Limb
✅ Water leaves
❌ Salt cannot leave
Ascending Limb
✅ Salt leaves
❌ Water cannot leave
STEP 1 (Panel ①)
Initially everything is the same.
| Location | Osmolarity |
|---|---|
| Descending limb | 300 |
| Ascending limb | 300 |
| Interstitium | 300 |
Everything starts isotonic.
Simple Picture
Descending = 300
Interstitium = 300
Ascending = 300No gradient exists.
STEP 2 (Panel ②)
Thick Ascending Limb Pumps NaCl Out
Salt is actively pumped into the medulla.
Because water cannot follow:
Ascending limb becomes dilute.
New Situation
| Ascending Limb | 200 |
| Interstitium | 400 |
The ascending limb is now 200.
The interstitium becomes 400.
Key Concept
Salt leaves, water stays.
Therefore:
Ascending = 200
Interstitium = 400A 200 mOsm difference is created.
STEP 3 (Panel ③)
Water Leaves Descending Limb
Descending limb is permeable to water.
Water moves into the now concentrated medulla (400).
Fluid inside descending limb becomes concentrated too.
New Situation
| Descending Limb | 400 |
| Interstitium | 400 |
They become equal.
Easy Memory
Water follows osmolaritySo:
400 ↔ 400STEP 4 (Panel ④)
New 300 mOsm Fluid Enters From Proximal Tubule
Fresh fluid (300) enters the descending limb.
Older concentrated fluid is pushed downward.
Fluid moves around the loop.
Result
| Top Descending | 300 |
| Deep Descending | 400 |
| Ascending | 200–400 |
A concentration gradient begins to appear.
STEP 5 (Panel ⑤)
Ascending Limb Pumps More Salt Out
Again:
✅ Salt leaves
❌ Water cannot leave
The interstitium becomes even more concentrated.
Values Become
| Interstitium | 350–500 |
| Ascending Limb | 150–300 |
Now a stronger gradient exists.
STEP 6 (Panel ⑥)
Water Leaves Descending Limb Again
Because the interstitium is now even more concentrated:
More water leaves the descending limb.
Descending limb concentration rises.
Values
| Descending | 350–500 |
| Interstitium | 350–500 |
Again equilibrium is achieved.
Repeat Steps 4 → 6 Again and Again
The process continues thousands of times every day.
Each cycle:
- Salt pumped out of ascending limb
- Water leaves descending limb
- New fluid enters
- Flow pushes concentrated fluid deeper
STEP 7 (Final Result)
After repeated cycles:
A huge osmotic gradient develops.
Interstitial Osmolarity
| Cortex | 300 |
|---|---|
| Upper Medulla | 700 |
| Mid Medulla | 1000 |
| Deep Medulla | 1200 |
Final Concentrations in Figure
Descending Limb
| Level | Osmolarity |
|---|---|
| Top | 300 |
| Middle | 700 |
| Lower | 1000 |
| Bottom | 1200 |
Ascending Limb
| Level | Osmolarity |
|---|---|
| Bottom | 1000 |
| Middle | 800 |
| Upper | 500 |
| Top | 100 |
Notice:
👉 Ascending limb becomes progressively dilute because salt is continuously removed.
Why Is It Called a “Countercurrent Multiplier”?
Countercurrent
Fluid flows in opposite directions.
Descending ↓
Ascending ↑Multiplier
A small 200 mOsm difference created by the ascending limb gets multiplied into a huge vertical gradient.
200 difference
↓
700
↓
1000
↓
1200The loop multiplies the effect.
Super Easy Story
Descending Limb
💧 Water leaves
Fluid becomes concentrated.
Ascending Limb
🧂 Salt leaves
Fluid becomes dilute.
Repetition
Continuous flow + repeated salt pumping + water movement
creates:
Cortex = 300
↓
700
↓
1000
↓
1200This is the hyperosmotic renal medulla.
KEY CONCEPT
The thick ascending limb pumps NaCl into the medulla but cannot lose water, creating a 200 mOsm gradient. Water then leaves the descending limb until it matches the medulla. Continuous tubular flow repeats this process, multiplying the gradient and producing a hyperosmotic renal medulla (300 → 1200 mOsm/L). This is called the Countercurrent Multiplier System. 🔥🧂💧
ROLE OF DISTAL TUBULES AND COLLECTING DUCTS IN EXCRETING CONCENTRATED URINE
- Tubular fluid leaving the loop of Henle and entering the distal convoluted tubule is dilute.
- The osmolarity of this fluid is about 100–140 mOsm/L.
- The early distal tubule further dilutes the tubular fluid.
- The early distal tubule actively transports sodium chloride out of the tubule.
- The early distal tubule is relatively impermeable to water.
- Because solutes are removed without water, the tubular fluid becomes more dilute.
- As fluid enters the cortical collecting tubule, water reabsorption depends on the level of ADH.
- In the absence of ADH, the cortical collecting tubule is almost impermeable to water.
- Without ADH, little or no water is reabsorbed.
- Solute reabsorption continues.
- The urine becomes even more dilute.
- When ADH levels are high, the cortical collecting tubule becomes highly permeable to water.
- Large amounts of water are reabsorbed from the tubule into the cortical interstitium.
- The reabsorbed water is carried away by the peritubular capillaries.
- More water is reabsorbed in the cortex than in the renal medulla.
- This helps maintain the high osmolarity of the medullary interstitial fluid.
- As tubular fluid moves through the medullary collecting ducts, additional water is reabsorbed.
- Water moves from the tubular fluid into the medullary interstitium.
- The total amount of water reabsorbed in the medulla is relatively small compared with the amount reabsorbed in the cortex.
- The reabsorbed water is carried away by the vasa recta into the venous blood.
- When ADH levels are high, the collecting ducts become permeable to water.
- Under these conditions, the fluid at the end of the collecting ducts reaches nearly the same osmolarity as the renal medullary interstitium.
- This osmolarity is about 1200 mOsm/L.
- By reabsorbing the maximum possible amount of water, the kidneys produce highly concentrated urine.
- The kidneys continue to excrete normal amounts of solutes in the urine.
- At the same time, water is returned to the extracellular fluid.
- This helps compensate for deficits of body water.
KEY CONCEPT
- Fluid entering the distal tubule is already dilute (100–140 mOsm/L).
- The early distal tubule removes NaCl but not water, making the fluid even more dilute.
- Water reabsorption in the cortical collecting tubule depends on ADH.
- Without ADH → little water reabsorption → dilute urine.
- With high ADH → large water reabsorption → concentrated urine.
- Additional water is reabsorbed in the medullary collecting ducts.
- At high ADH levels, urine osmolarity can reach about 1200 mOsm/L.
- Distal tubules and collecting ducts help conserve water and produce concentrated urine.
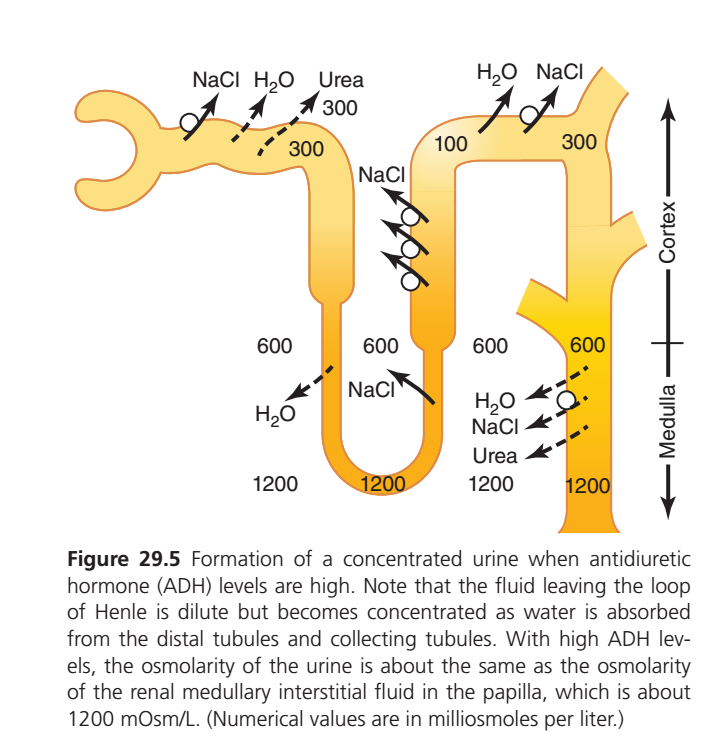
Formation of Concentrated Urine (When ADH is High) – Easiest Concept
🎯 Main Idea
When ADH (Antidiuretic Hormone) is high:
✅ Kidneys reabsorb a lot of water
✅ Urea recycling increases
✅ Urine becomes very concentrated
Final Result
Small volume of urine + Very concentrated urine (≈1200 mOsm/L)
Compare Low ADH vs High ADH
| Low ADH | High ADH |
|---|---|
| Water stays in tubule | Water leaves tubule |
| Large urine volume | Small urine volume |
| Dilute urine (50 mOsm/L) | Concentrated urine (1200 mOsm/L) |
Step 1: Proximal Tubule
What happens?
- NaCl reabsorbed
- Water reabsorbed
- Some urea reabsorbed
Osmolarity
Remains:
300 mOsm/L
Because water and solutes leave together.
Step 2: Descending Limb
What happens?
Descending limb is highly permeable to water.
💧 Water leaves the tubule.
Osmolarity Changes
| Level | Osmolarity |
|---|---|
| Cortex | 300 |
| Mid Medulla | 600 |
| Deep Medulla | 1200 |
As water leaves:
Tubular fluid becomes concentrated
300 → 600 → 1200Step 3: Ascending Limb
What happens?
✅ NaCl leaves
❌ Water cannot leave
Osmolarity Changes
1200 → 600 → 100Fluid becomes dilute.
Why?
Salt is removed but water remains.
Important Point
Fluid Leaving Loop of Henle
Is only:
100 mOsm/L
Very dilute.
This is exactly like the previous figure.
Step 4: Distal Tubule (High ADH Present)
Now ADH starts working.
ADH inserts Aquaporins
Water channels open.
What happens?
💧 Water leaves tubule
Because surrounding medulla is concentrated.
Step 5: Cortical Collecting Duct
What happens?
ADH continues to act.
Water moves out into the hyperosmotic interstitium.
Osmolarity
Tubular fluid becomes more concentrated:
100 → 300By the time fluid leaves cortex:
It becomes approximately isotonic.
Step 6: Medullary Collecting Duct
This is the most important area.
Under High ADH
The medullary collecting duct becomes highly permeable to:
✅ Water
✅ Urea
Water Reabsorption
Because medulla is very concentrated:
600
↓
1200Water is strongly pulled out.
Large amounts of water leave the collecting duct.
Urea Reabsorption
ADH also increases urea permeability.
Urea leaves collecting duct
Urea enters medullary interstitium.
This is called:
Urea Recycling
Why Is Urea Important?
Urea contributes nearly half of the deep medullary osmolarity.
Example
At papilla:
1200 mOsm/LApproximately:
600 from NaCl
+
600 from Urea
=
1200This helps pull even more water out.
Understanding the Numbers in Figure
Cortex
Interstitial Osmolarity
300Mid Medulla
600Deep Medulla (Papilla)
1200Tubular Fluid
Descending Limb
300 → 600 → 1200Concentrated because water leaves.
Ascending Limb
1200 → 600 → 100Diluted because salt leaves.
Collecting Duct
100 → 300 → 600 → 1200Concentrated again because water leaves under ADH.
Meaning of Each Arrow
H₂O Arrow
💧 Water leaving tubule
Occurs in:
- Descending limb
- Distal tubule
- Collecting duct
(when ADH is high)
NaCl Arrow
🧂 Salt leaving tubule
Occurs in:
- Ascending limb
- Distal tubule
- Collecting duct
Urea Arrow
Occurs mainly in:
Inner Medullary Collecting Duct
Urea diffuses into medulla.
This strengthens the medullary osmotic gradient.
Simple Story of the Whole Figure
Loop of Henle Creates the Gradient
300 → 600 → 1200ADH Uses the Gradient
ADH opens water channels.
Water leaves collecting ducts.
Urea Strengthens the Gradient
Urea enters medulla.
Medulla becomes even more concentrated.
Final Result
Very little water remains in tubule.
Urine concentration rises to:
≈1200 mOsm/L
Super Easy Memory Trick
Loop of Henle
Creates the gradient.
🧂 Salt mechanism
Urea
Strengthens the gradient.
📈 Osmotic booster
ADH
Uses the gradient.
💧 Water saver
KEY CONCEPT
The Loop of Henle creates a hyperosmotic medulla (300→1200 mOsm/L). When ADH is high, distal tubules and collecting ducts become permeable to water, allowing large amounts of water to leave the tubule. ADH also increases urea recycling, which further raises medullary osmolarity. As a result, the dilute fluid leaving the Loop of Henle (100 mOsm/L) becomes highly concentrated urine (≈1200 mOsm/L) with a very small volume. 🚰➡️💧➡️🔥1200 mOsm/L
UREA CONTRIBUTES TO HYPEROSMOTIC RENAL MEDULLARY INTERSTITIUM AND FORMATION OF CONCENTRATED URINE
- Urea contributes about 40%–50% of the osmolarity of the renal medullary interstitium during maximal urine concentration.
- Urea contributes about 500–600 mOsm/L to the osmolarity of the renal medulla.
- Unlike sodium chloride, urea is passively reabsorbed from the tubule.
- During water deficit, ADH levels become high.
- High ADH levels cause large amounts of urea to be passively reabsorbed from the inner medullary collecting ducts into the interstitium.
- As tubular fluid passes through the ascending loop of Henle, distal tubule, and cortical collecting tubule, little urea is reabsorbed.
- These segments have low permeability to urea.
- In the presence of high ADH, large amounts of water are reabsorbed from the cortical collecting tubule.
- Because urea permeability is low in this segment, urea remains in the tubular fluid.
- As water is removed, the concentration of urea in the tubular fluid increases rapidly.
- As tubular fluid enters the inner medullary collecting ducts, additional water reabsorption occurs.
- This further increases the concentration of urea in the tubular fluid.
- The high concentration of urea creates a gradient that causes urea to diffuse into the renal interstitial fluid.
- Urea diffusion is facilitated by specific urea transporters.
- UT-A1 is mainly present in the luminal (apical) membrane.
- UT-A3 is mainly present in the basolateral membrane.
- ADH stimulates the accumulation of these urea transporters.
- Increased urea transporters enhance the movement of urea out of the inner medullary collecting ducts.
- Water and urea leave the inner medullary collecting ducts simultaneously.
- This process maintains a high concentration of urea in the tubular fluid.
- Eventually, a high concentration of urea is also present in the urine.
- Urea plays a fundamental role in the kidney’s ability to concentrate urine.
- People who consume a high-protein diet produce larger amounts of urea.
- These individuals can concentrate their urine better.
- People with low protein intake produce less urea.
- Their urine-concentrating ability is reduced.
- Malnutrition is associated with a low concentration of urea in the medullary interstitium.
- Malnutrition is also associated with impaired urine-concentrating ability.
KEY CONCEPT
- Urea contributes 40%–50% of the osmolarity of the renal medulla.
- During dehydration, high ADH increases urea reabsorption from the inner medullary collecting ducts.
- Water reabsorption concentrates urea inside the tubules.
- High urea concentration drives diffusion of urea into the medullary interstitium.
- ADH increases UT-A1 and UT-A3 transporters, enhancing urea movement.
- Urea accumulation helps create the hyperosmotic renal medulla.
- A high-protein diet increases urea production and improves urine-concentrating ability.
- Low protein intake and malnutrition decrease medullary urea concentration and reduce the ability to concentrate urine.
RECIRCULATION OF UREA FROM COLLECTING DUCT TO LOOP OF HENLE CONTRIBUTES TO HYPEROSMOTIC RENAL MEDULLA
- A healthy person normally excretes about 20% to 60% of the filtered urea load.
- The percentage of urea excreted depends on urine flow rate and hydration status.
- The rate of urea excretion is mainly determined by:
- Plasma urea concentration
- Glomerular filtration rate (GFR)
- Renal tubular urea reabsorption
- In renal disease, a large reduction in GFR causes plasma urea concentration to increase markedly.
- The increased plasma urea concentration restores the filtered urea load and urea excretion rate toward normal.
- In the proximal tubule, about 40% to 50% of filtered urea is reabsorbed.
- Despite this reabsorption, urea concentration in the tubular fluid increases.
- Urea concentration increases because urea is less permeable than water.
- As tubular fluid enters the thin segments of the loop of Henle, urea concentration continues to rise.
- Water reabsorption from the descending limb contributes to this rise in urea concentration.
- Some urea is also secreted from the medullary interstitium into the thin loop of Henle.
- This passive secretion is facilitated by the urea transporter UT-A2.
- The thick ascending limb, distal tubule, and cortical collecting tubule have low permeability to urea.
- Therefore, only small amounts of urea are reabsorbed in these segments.
- During concentrated urine formation, ADH levels are high.
- High ADH increases water reabsorption from the distal tubule and cortical collecting tubule.
- Water reabsorption further increases the concentration of urea in the tubular fluid.
- As tubular fluid enters the inner medullary collecting duct, urea concentration becomes very high.
- UT-A1 and UT-A3 transporters facilitate diffusion of urea into the medullary interstitium.
- Some of the urea that enters the medullary interstitium diffuses back into the thin loop of Henle.
- This urea then travels through the ascending limb, distal tubule, and cortical collecting tubule.
- The urea eventually returns to the medullary collecting duct.
- In this way, urea recirculates through these parts of the nephron several times before being excreted.
- Each cycle of recirculation increases the concentration of urea.
- Urea recirculation provides an additional mechanism for producing a hyperosmotic renal medulla.
- Urea is one of the major waste products excreted by the kidneys.
- Concentrating urea before excretion helps conserve body water when water is limited.
- When excess water is present in the body, urine flow rate increases.
- Increased urine flow lowers the urea concentration in the inner medullary collecting ducts.
- Lower urea concentration reduces diffusion of urea into the medullary interstitium.
- ADH levels also decrease when excess body water is present.
- Reduced ADH decreases the permeability of the inner medullary collecting ducts to water.
- Reduced ADH also decreases permeability to urea.
- As a result, more urea is excreted in the urine.
KEY CONCEPT
- About 40%–50% of filtered urea is reabsorbed in the proximal tubule.
- Urea concentration increases as water is reabsorbed from the nephron.
- UT-A2 helps secrete urea into the thin loop of Henle.
- UT-A1 and UT-A3 help move urea from the inner medullary collecting duct into the medullary interstitium.
- Some urea recycles between the collecting duct and loop of Henle several times.
- This urea recirculation increases medullary urea concentration.
- Urea recirculation is an important contributor to the hyperosmotic renal medulla.
- High ADH promotes urea recycling and concentrated urine formation.
- Low ADH reduces urea recycling and increases urea excretion in dilute urine.
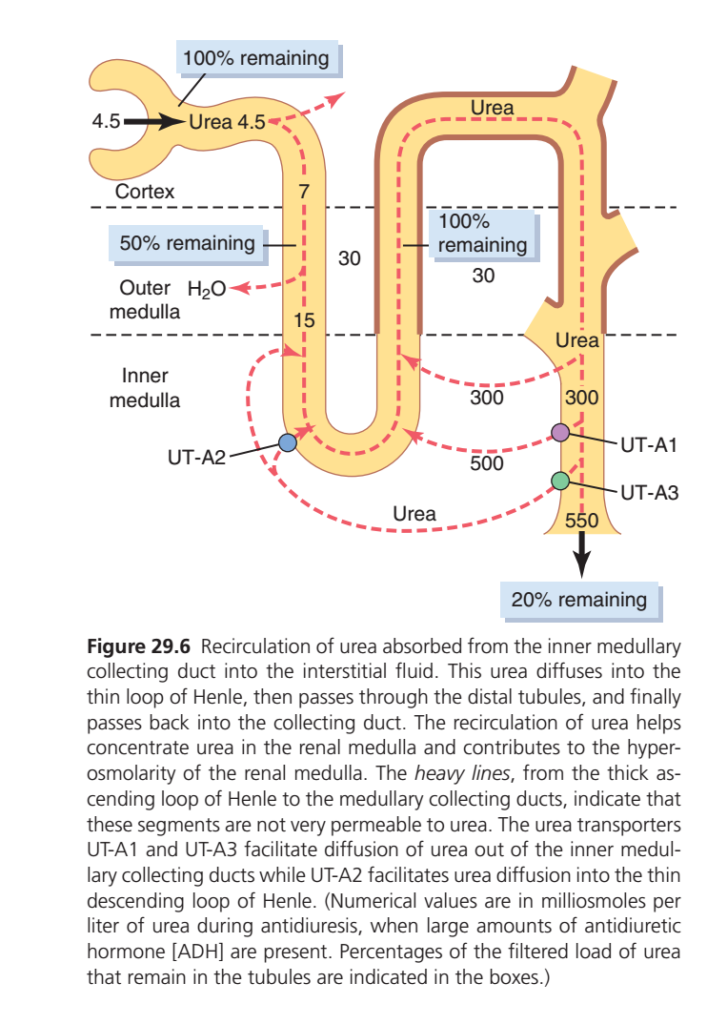
Figure 29.6 – Urea Recycling (Recirculation of Urea) Made Super Easy
🎯 Main Idea
The kidney does not waste all urea.
Instead:
✅ Some urea leaves the collecting duct
✅ Enters the medulla
✅ Enters the Loop of Henle again
✅ Travels through the nephron
✅ Returns to the collecting duct
This continuous cycle is called:
🔄 Urea Recycling
Why Does the Kidney Recycle Urea?
Because urea helps create a very concentrated medulla.
A concentrated medulla:
➡️ Pulls water out of collecting ducts
➡️ Helps ADH make concentrated urine
Step 1: Urea Is Filtered
At the glomerulus:
Filtered Urea = 100%
In the figure:
4.5 = Filtered amount of ureaThink of 4.5 as:
“100% of filtered urea”
Step 2: Proximal Tubule
What happens?
Water is reabsorbed.
Some urea is also reabsorbed.
But water is removed faster than urea.
Therefore:
Urea concentration inside the tubule rises.
Step 3: Thin Descending Loop
As water continues leaving:
💧 Water leaves
❌ Urea stays
Therefore urea concentration becomes even higher.
Values in Figure
7
↓
15Urea concentration increases.
Important Box
“50% Remaining”
Means:
After the proximal tubule,
only about:
50% of filtered urea
is still inside the nephron.
The other 50% has already been reabsorbed.
Step 4: Inner Medullary Collecting Duct
This is the most important part.
Under:
High ADH
special urea transporters open.
Urea Transporters
UT-A1
UT-A3
These transporters allow urea to leave the collecting duct.
What Happens?
Urea diffuses into:
Inner medullary interstitium
The concentration becomes very high.
Values in Figure
300
500
550These numbers show increasing urea concentration in the deep medulla.
Why Is This Important?
Urea now becomes trapped in the medulla.
This increases medullary osmolarity.
Remember
Deep medulla osmolarity:
1200 mOsm/Lcomes from approximately:
600 NaCl
+
600 Urea
=
1200So urea provides about half of the concentrating power.
Step 5: Urea Enters Thin Loop of Henle Again
Now the recycled urea moves from:
Medulla
↓
Thin Descending Limbthrough transporter:
UT-A2
UT-A2 Function
Facilitates urea movement:
Interstitium
↓
Thin Descending LimbStep 6: Urea Travels Through Nephron Again
Now urea flows through:
Thin Loop
↓
Ascending Limb
↓
Distal Tubule
↓
Collecting Duct
and returns to the collecting duct.
Why Is This Called Recycling?
Because urea keeps moving in a circle:
Collecting duct
↓
Medulla
↓
Loop of Henle
↓
Distal Tubule
↓
Collecting ductAgain and again.
Understanding the Dashed Red Arrows
The red dashed arrows show:
Path of Recycled Urea
Collecting duct
↓
Medullary interstitium
↓
Thin Loop of Henle
↓
Distal nephron
↓
Collecting ductThis is the recycling loop.
Meaning of Heavy Brown Lines
The thick brown nephron segments represent:
Thick Ascending Limb
Distal Tubule
Cortical Collecting Duct
These parts are:
❌ Not very permeable to urea
Therefore urea remains trapped inside until it reaches the inner medullary collecting duct.
What Do the Percentage Boxes Mean?
Box 1
100% Remaining
At filtration:
100% urea presentBox 2
50% Remaining
After proximal tubule:
50% remains
50% reabsorbedBox 3
100% Remaining
After urea is secreted back into the thin loop from the medulla,
the amount inside the tubule becomes nearly equal to the original filtered load again.
Box 4
20% Remaining
At the end:
Only about:
20% of filtered urea
is finally excreted in urine.
Simple Story of the Whole Figure
ADH High
↓
Urea leaves inner medullary collecting duct through UT-A1 and UT-A3
↓
Urea accumulates in medulla
↓
Urea enters thin loop through UT-A2
↓
Urea circulates through nephron
↓
Returns to collecting duct
↓
Repeats again and again
↓
Medulla becomes highly concentrated
↓
More water reabsorbed
↓
Concentrated urine formed
Super Easy Memory Trick
UT-A1 & UT-A3
👉 Urea OUT of Collecting Duct
Collecting Duct → MedullaUT-A2
👉 Urea INTO Loop of Henle
Medulla → Thin LoopKEY CONCEPT
Urea recycling is the movement of urea from the inner medullary collecting duct into the medullary interstitium and then back into the thin loop of Henle. UT-A1 and UT-A3 transport urea out of the collecting duct, while UT-A2 transports urea into the thin descending limb. This recycling traps urea in the medulla, contributes about half of the deep medullary osmolarity, strengthens the corticomedullary osmotic gradient, and allows ADH to produce highly concentrated urine. 🔄🧂💧🔥
COUNTERCURRENT EXCHANGE IN VASA RECTA PRESERVES HYPEROSMOLARITY OF RENAL MEDULLA
- Blood flow to the renal medulla is necessary to supply oxygen and nutrients to the cells.
- Without a special blood flow system, the solutes accumulated in the renal medulla would be rapidly washed away.
- Two special features of medullary blood flow help preserve the high solute concentration of the renal medulla.
- The first feature is low medullary blood flow.
- Medullary blood flow accounts for less than 5% of total renal blood flow.
- This slow blood flow is sufficient to meet the metabolic needs of the medullary tissues.
- Slow blood flow helps minimize the loss of solutes from the medullary interstitium.
- The second feature is the presence of the vasa recta.
- The vasa recta act as countercurrent exchangers.
- The vasa recta help prevent the washout of solutes from the medullary interstitium.
- Blood enters and leaves the medulla through the vasa recta at the corticomedullary junction.
- The vasa recta are highly permeable to most solutes.
- Plasma proteins do not readily cross the vasa recta.
- As blood descends into the medulla, it becomes progressively more concentrated.
- Solutes move from the interstitium into the blood.
- Water moves from the blood into the interstitium.
- By the time blood reaches the tip of the vasa recta, its osmolarity is about 1200 mOsm/L.
- This osmolarity is approximately equal to that of the medullary interstitium.
- As blood ascends toward the cortex, it becomes progressively less concentrated.
- Solutes diffuse from the blood back into the medullary interstitium.
- Water moves from the interstitium into the blood.
- Large amounts of water and solutes are exchanged across the vasa recta.
- Despite this exchange, there is little net dilution of the medullary interstitial fluid.
- The U-shaped structure of the vasa recta is responsible for this effect.
- The U-shaped vasa recta function as countercurrent exchangers.
- The vasa recta do not create medullary hyperosmolarity.
- The vasa recta help preserve the hyperosmolarity that has already been created.
- The U-shaped arrangement minimizes the loss of solutes from the medullary interstitium.
- The vasa recta do not prevent bulk reabsorption of fluid and solutes into the blood.
- Reabsorption occurs because of hydrostatic and colloid osmotic pressures in the capillaries.
- Under steady-state conditions, the vasa recta remove only the amount of water and solutes absorbed from the medullary tubules.
- Therefore, the high solute concentration established in the medulla is maintained.
KEY CONCEPT
- The vasa recta preserve the hyperosmotic renal medulla.
- Medullary blood flow is very low (<5% of total renal blood flow).
- Slow blood flow reduces solute washout.
- As blood descends:
- Solutes enter blood.
- Water leaves blood.
- As blood ascends:
- Solutes leave blood.
- Water enters blood.
- The U-shaped vasa recta act as countercurrent exchangers.
- Vasa recta do not create medullary hyperosmolarity.
- Vasa recta prevent loss of the osmotic gradient created by the countercurrent multiplier.
- This preservation of medullary hyperosmolarity is essential for forming concentrated urine.
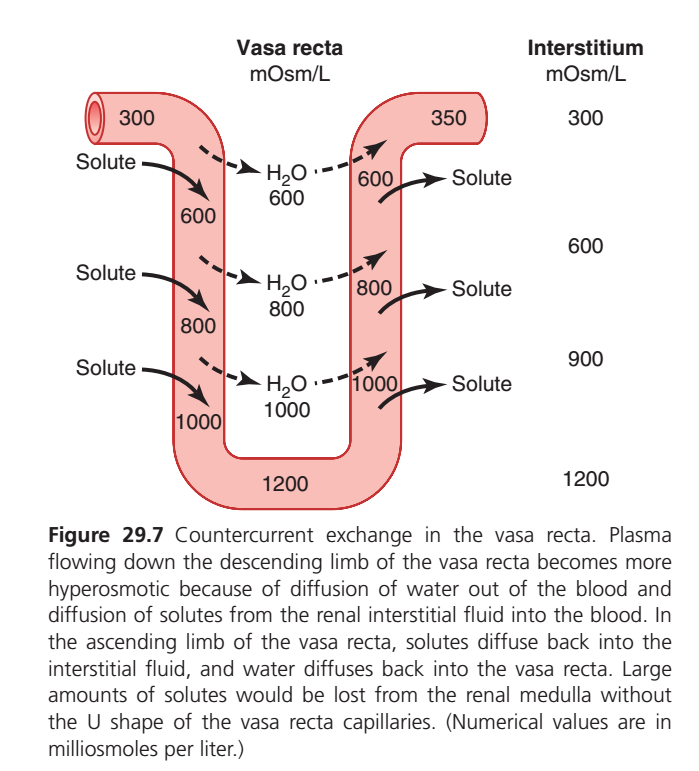
Figure 29.7 – Countercurrent Exchange in Vasa Recta (Easiest Concept)
🎯 Main Idea
The Loop of Henle creates the concentrated medulla.
The Vasa Recta preserves the concentrated medulla.
Easy Memory
🧂 Loop of Henle = Creates Gradient
🩸 Vasa Recta = Protects Gradient
Why Do We Need the Vasa Recta?
The medulla needs blood supply.
But there is a problem:
If ordinary blood vessels flowed through the medulla,
👉 They would wash away all the NaCl and urea.
👉 The medulla would lose its high osmolarity.
👉 Concentrated urine could not be formed.
Therefore the kidney uses a special capillary:
Vasa Recta
A U-shaped capillary.
Understanding the Figure
Right Side = Interstitial Osmolarity
| Region | Osmolarity |
|---|---|
| Cortex | 300 |
| Upper Medulla | 600 |
| Mid Medulla | 900 |
| Deep Medulla | 1200 |
The deeper you go:
300
↓
600
↓
900
↓
1200The medulla becomes progressively more concentrated.
Step 1: Blood Enters Descending Vasa Recta
Blood enters from cortex.
Osmolarity
300 mOsm/LBlood is normal.
Step 2: Blood Descends into Medulla
As blood moves downward:
The surrounding interstitium becomes more concentrated.
What Happens?
Water Leaves Blood
💧 Blood → Interstitium
Because medulla is hyperosmotic.
Solutes Enter Blood
🧂 NaCl and Urea
Interstitium → Blood
Result
Blood becomes progressively concentrated.
Osmolarity Changes
300
↓
600
↓
800
↓
1000
↓
1200At the tip:
Blood osmolarity = 1200
Why?
Because:
Water lost
Solute gained
makes blood concentrated.
Step 3: Blood Reaches Bottom
At the deepest medulla:
Blood = 1200 mOsm/L
Interstitium = 1200 mOsm/L
They become almost equal.
No major net movement occurs.
Step 4: Blood Ascends Back Toward Cortex
Now blood moves upward.
The surrounding interstitium becomes less concentrated.
What Happens?
Now the opposite occurs.
Solutes Leave Blood
🧂 Blood → Interstitium
NaCl and urea diffuse back out.
Water Enters Blood
💧 Interstitium → Blood
Water diffuses into blood.
Result
Blood gradually becomes dilute again.
Osmolarity Changes
1200
↓
1000
↓
800
↓
600
↓
350By the time blood leaves:
Blood ≈ 350 mOsm/L
Why Doesn’t the Vasa Recta Wash Away Solutes?
This is the most important concept.
Descending Limb
Takes solutes INTO blood.
Interstitium → BloodAscending Limb
Returns solutes BACK to medulla.
Blood → InterstitiumNet Effect
Most solutes that entered blood:
✅ Return to medulla
Most water entering blood:
✅ Leaves medulla circulation
Thus:
Solutes stay in medulla
Water is removed
Exactly what the kidney wants.
What Do the Arrows Mean?
Solid Arrows (Solute)
🧂 NaCl and Urea movement
Descending Side
Interstitium → BloodAscending Side
Blood → InterstitiumDashed Arrows (Water)
💧 Water movement
Descending Side
Blood → InterstitiumAscending Side
Interstitium → BloodWhy Is It Called Countercurrent Exchange?
Because blood flows in opposite directions.
Descending limb ↓
Ascending limb ↑Substances exchange passively between blood and interstitium.
No active transport required.
Countercurrent Multiplier vs Countercurrent Exchange
| Countercurrent Multiplier | Countercurrent Exchange |
|---|---|
| Loop of Henle | Vasa Recta |
| Creates gradient | Preserves gradient |
| Active NaCl transport | Passive diffusion |
| Produces 1200 mOsm medulla | Prevents washout |
Simple Story
Blood enters cortex
300↓
Water leaves blood
Solutes enter blood
↓
Blood becomes
600 → 800 → 1000 → 1200↓
Blood turns upward
↓
Solutes leave blood
Water enters blood
↓
Blood exits as
350↓
Medullary solutes remain preserved
↓
Kidney can continue producing concentrated urine
KEY CONCEPT
The Vasa Recta acts as a countercurrent exchanger. As blood descends, it loses water and gains NaCl and urea, becoming progressively concentrated (300→1200 mOsm/L). As blood ascends, it gains water and loses solutes, becoming dilute again (1200→350 mOsm/L). Because the solutes gained in the descending limb are returned to the medulla in the ascending limb, the Vasa Recta supplies blood to the medulla without washing away the corticomedullary osmotic gradient. 🩸🔄🧂💧
One-Line Memory Trick
Loop of Henle BUILDS the osmotic gradient; Vasa Recta PROTECTS the osmotic gradient. 🔥🧂🩸
INCREASED MEDULLARY BLOOD FLOW REDUCES URINE-CONCENTRATING ABILITY
- Certain vasodilator substances can greatly increase blood flow through the renal medulla.
- Increased medullary blood flow washes some solutes out of the renal medulla.
- Loss of medullary solutes reduces the hyperosmolarity of the renal medulla.
- As medullary hyperosmolarity decreases, the kidney’s maximum urine-concentrating ability decreases.
- Large increases in arterial pressure can also increase blood flow to the renal medulla.
- Medullary blood flow may increase more than blood flow in other regions of the kidney.
- Increased medullary blood flow tends to wash out the hyperosmotic interstitium.
- This washout reduces the ability of the kidneys to concentrate urine.
- Maximum urine-concentrating ability depends on the concentration of ADH.
- Maximum urine-concentrating ability also depends on the osmolarity of the renal medullary interstitial fluid.
- Even when ADH levels are maximal, urine-concentrating ability can still decrease.
- This decrease occurs if medullary blood flow becomes high enough to reduce medullary hyperosmolarity.
KEY CONCEPT
- High medullary blood flow washes solutes out of the renal medulla.
- Loss of solutes decreases medullary hyperosmolarity.
- Reduced medullary hyperosmolarity lowers the kidney’s ability to concentrate urine.
- Vasodilators and increased arterial pressure can increase medullary blood flow.
- Concentrated urine requires:
- High ADH levels
- A hyperosmotic renal medulla
- Even with maximum ADH, urine cannot become highly concentrated if the medullary osmotic gradient is washed out.
SUMMARY OF URINE-CONCENTRATING MECHANISM AND CHANGES IN OSMOLARITY IN DIFFERENT TUBULAR SEGMENTS
Proximal Tubule
- About 65% of most filtered electrolytes are reabsorbed in the proximal tubule.
- The proximal tubular membranes are highly permeable to water.
- Whenever solutes are reabsorbed, water also moves across the tubular membrane by osmosis.
- Water movement is aided by aquaporin-1 (AQP-1) channels.
- Therefore, the osmolarity of the tubular fluid remains about the same as the glomerular filtrate.
- The tubular fluid osmolarity remains about 300 mOsm/L.
Descending Loop of Henle
- As fluid flows down the descending loop of Henle, water is reabsorbed into the medulla.
- The descending limb contains aquaporin-1 (AQP-1).
- The descending limb is highly permeable to water.
- The descending limb is much less permeable to sodium chloride and urea.
- During antidiuretic conditions, passive urea secretion into the thin loops of Henle is facilitated by UT-A2.
- The osmolarity of the tubular fluid gradually increases as it flows through the descending loop.
- The tubular fluid osmolarity becomes nearly equal to the surrounding interstitial fluid.
- When ADH levels are high, the surrounding interstitial fluid osmolarity is about 1200 mOsm/L.
- During formation of dilute urine, ADH levels are low.
- When ADH levels are low, medullary interstitial osmolarity is less than 1200 mOsm/L.
- Therefore, the tubular fluid in the descending loop becomes less concentrated.
- This decrease in concentration occurs partly because less urea is reabsorbed into the medullary interstitium.
- Less urea is reabsorbed from the inner medullary collecting ducts when ADH levels are low.
- Under these conditions, the kidney forms a large volume of dilute urine.
Thin Ascending Loop of Henle
- The thin ascending limb is essentially impermeable to water.
- The thin ascending limb reabsorbs some sodium chloride.
- Water removal in the descending limb increases sodium chloride concentration in the tubular fluid.
- Sodium chloride passively diffuses from the thin ascending limb into the medullary interstitium.
- Tubular fluid becomes more dilute as sodium chloride leaves the tubule.
- Water remains in the tubule.
- Some urea absorbed into the medullary interstitium diffuses into the ascending limb.
- This returns urea to the tubular system.
- This process helps prevent washout of urea from the renal medulla.
- Urea recycling contributes to the hyperosmotic renal medulla.
Thick Ascending Loop of Henle
- The thick ascending limb is virtually impermeable to water.
- Large amounts of sodium, chloride, potassium, and other ions are actively transported into the medullary interstitium.
- Tubular fluid becomes very dilute in the thick ascending limb.
- Tubular fluid osmolarity falls to about 140 mOsm/L.
Early Distal Tubule
- The early distal tubule has properties similar to the thick ascending limb.
- Solutes are reabsorbed while water remains in the tubule.
- Further dilution of the tubular fluid occurs.
- Tubular fluid osmolarity decreases to about 100 mOsm/L.
Late Distal Tubule and Cortical Collecting Tubules
- The osmolarity of the tubular fluid depends on the level of ADH.
- With high ADH levels, these tubules become highly permeable to water.
- Significant amounts of water are reabsorbed.
- These segments are not very permeable to urea.
- Urea concentration increases as water is reabsorbed.
- Most of the urea delivered to these segments passes into the inner medullary collecting ducts.
- Urea is eventually reabsorbed or excreted in the urine.
- In the absence of ADH, little water is reabsorbed.
- Osmolarity decreases further because active ion reabsorption continues.
Inner Medullary Collecting Ducts
- The concentration of tubular fluid depends on ADH levels.
- The concentration of tubular fluid also depends on medullary interstitial osmolarity.
- Medullary interstitial osmolarity is established by the countercurrent mechanism and urea reabsorption.
- In the presence of high ADH levels, these ducts become highly permeable to water.
- Water diffuses from the tubule into the interstitial fluid.
- Water movement continues until osmotic equilibrium is reached.
- The tubular fluid reaches approximately the same concentration as the medullary interstitium.
- The concentration becomes about 1200–1400 mOsm/L.
- A small volume of concentrated urine is produced when ADH levels are high.
- Water reabsorption increases urea concentration in the tubular fluid.
- The inner medullary collecting ducts contain UT-A1 and UT-A3 urea transporters.
- These transporters facilitate urea diffusion.
- Much of the concentrated urea diffuses into the medullary interstitium.
- Urea absorption contributes to the high osmolarity of the medullary interstitium.
- Urea absorption contributes to the high urine-concentrating ability of the kidney.
Additional Important Points
- Sodium chloride is one of the major solutes contributing to medullary hyperosmolarity.
- The kidney can excrete highly concentrated urine containing little sodium chloride.
- In these circumstances, urine hyperosmolarity is mainly due to other solutes.
- Urea is especially important in producing this hyperosmolarity.
- One example is dehydration with low sodium intake.
- Low sodium intake stimulates formation of angiotensin II and aldosterone.
- Angiotensin II and aldosterone cause avid sodium reabsorption from the tubules.
- Urea and other solutes remain to maintain highly concentrated urine.
- Large volumes of dilute urine can be excreted without increasing sodium excretion.
- This occurs by decreasing ADH secretion.
- Reduced ADH decreases water reabsorption in distal tubular segments.
- Sodium reabsorption is not substantially altered.
- There is an obligatory urine volume determined by the kidney’s maximum concentrating ability.
- Obligatory urine volume is also determined by the amount of solute that must be excreted.
- Large amounts of solute require a minimum amount of water for excretion.
- If 600 mOsm of solute must be excreted each day, a minimum of 0.5 liter of urine is required.
- This calculation assumes a maximum urine concentration of 1200 mOsm/L.
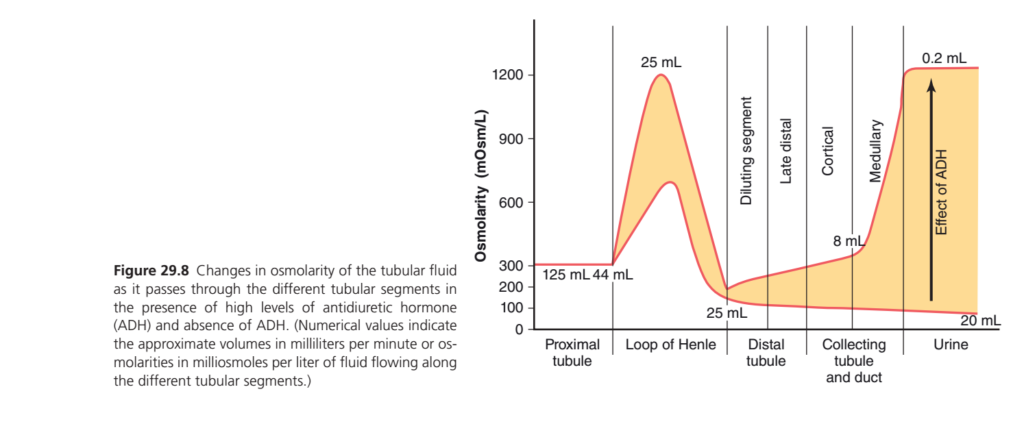
Figure 29.8 – Changes in Tubular Fluid Osmolarity With and Without ADH (Easiest Explanation)
🎯 What Is This Graph Showing?
This graph follows the tubular fluid from:
Proximal Tubule
↓
Loop of Henle
↓
Distal Tubule
↓
Collecting Duct
↓
Urineand shows:
Y-Axis (Vertical)
Osmolarity (mOsm/L)
How concentrated the tubular fluid is.
- 300 = Normal body fluid
- 1200 = Very concentrated
- 50–100 = Very dilute
X-Axis (Horizontal)
Different parts of the nephron.Understanding the Two Red Lines
There are actually two possible pathways.
🔴 Upper Red Line = HIGH ADH
When ADH is present
✅ Water is reabsorbed
✅ Urine becomes concentrated
🔴 Lower Red Line = NO ADH
When ADH is absent
❌ Water is not reabsorbed
✅ Urine becomes dilute
Understanding the Yellow Shaded Area
⭐ MOST IMPORTANT PART OF THE GRAPH
The yellow shaded area is the difference between:
High ADH
and
Low ADHIt represents:
“The Effect of ADH”
The larger the yellow area,
the greater ADH’s effect on concentrating urine.
Step-by-Step Journey Through the Graph
1. Proximal Tubule
Osmolarity
300 mOsm/Lfor BOTH lines.
Why?
In proximal tubule:
- Sodium reabsorbed
- Water reabsorbed
Both leave together.
Therefore concentration does not change.
Volume Changes
At beginning:
125 mL/min(GFR)
At end of proximal tubule:
44 mL/minbecause lots of water has already been reabsorbed.
Graph Interpretation
Both red lines stay flat at:
3002. Loop of Henle
Now the interesting part begins.
Descending Limb
Water leaves.
Fluid becomes concentrated.
Osmolarity Rises
300
↓
600
↓
1200Why?
Water leaves but salt remains.
On Graph
Both red lines rise sharply upward.
The peak reaches:
12003. Ascending Limb
Now NaCl leaves.
Water cannot leave.
Osmolarity Falls
1200
↓
600
↓
200Why?
Salt leaves but water stays.
This is the:
Diluting Segment
Graph
Both lines fall sharply downward.
End of Loop of Henle
Fluid becomes dilute.
Osmolarity
Around:
200 mOsm/LVolume
Only:
25 mL/minremains.IMPORTANT POINT
Up to this stage:
Both red lines are identical.
Because ADH has not yet acted.
4. Distal Tubule
Now ADH starts making a difference.
No ADH (Lower Red Line)
Water cannot leave.
Salt continues leaving.
Therefore:
Fluid becomes even more dilute.
Osmolarity
200
↓
100High ADH (Upper Red Line)
Water leaves.
Fluid becomes concentrated.
Osmolarity
200
↑
300This is Where the Yellow Area Starts
ADH begins separating the two curves.
5. Collecting Tubule & Collecting Duct
This is where ADH has its greatest effect.
Without ADH
Water cannot leave.
Tubular fluid becomes even more dilute.
Osmolarity
100
↓
50With High ADH
Water leaves rapidly.
Tubular fluid becomes concentrated.
Osmolarity
300
↑
400
↑
600
↑
1200Graph Interpretation
Upper line rises dramatically.
Lower line falls gradually.
The distance between them becomes huge.
Why Does Upper Line Rise to 1200?
Because:
ADH opens aquaporins
Water leaves collecting duct.
The remaining fluid becomes concentrated.
Eventually it matches:
Medullary Osmolarity
1200 mOsm/LFinal Urine
No ADH
Osmolarity
50–100 mOsm/LVery dilute urine.
Volume
20 mL/minLarge urine volume.
Easy Interpretation
No ADH
=
Water lost
=
Dilute urineHigh ADH
Osmolarity
1200 mOsm/LVery concentrated urine.
Volume
0.2 mL/minVery small urine volume.
Easy Interpretation
High ADH
=
Water saved
=
Concentrated urineUnderstanding the Numbers Written on Graph
125 mL
GFR entering nephron.
44 mL
Fluid remaining after proximal tubule.
25 mL
Fluid entering distal tubule.
8 mL
Fluid entering medullary collecting duct.
0.2 mL
Final urine with HIGH ADH.
Very little water lost.
20 mL
Final urine with NO ADH.
Large water loss.
What Does the Yellow Shaded Area Really Mean?
Think of the yellow area as:
“Water Saved by ADH”
Without ADH:
Urine = 20 mL/minWith ADH:
Urine = 0.2 mL/minADH dramatically reduces water loss.
The yellow region visually shows:
How much ADH changes urine concentration and urine volume.
Super Easy Story of the Entire Graph
Proximal Tubule
300 → 300No change.
Descending Loop
300 → 1200Water leaves.
Ascending Loop
1200 → 200Salt leaves.
Distal Tubule & Collecting Duct
Now pathways separate:
No ADH
200 → 100 → 50Dilute urine.
High ADH
200 → 300 → 600 → 1200Concentrated urine.
KEY CONCEPT
The graph compares tubular fluid osmolarity when ADH is absent versus when ADH is high. Up to the Loop of Henle both pathways are identical. The Loop of Henle first concentrates the fluid (300→1200 mOsm/L) and then dilutes it (1200→200 mOsm/L). In the distal tubule and collecting ducts, ADH becomes the deciding factor. Without ADH, water cannot be reabsorbed and dilute urine (50–100 mOsm/L, ~20 mL/min) is produced. With high ADH, large amounts of water are reabsorbed, producing a very small volume of highly concentrated urine (~1200 mOsm/L, ~0.2 mL/min). The yellow shaded area represents the effect of ADH on urine concentration and water conservation. 💧🔥🩺
QUANTIFYING RENAL URINE CONCENTRATION AND DILUTION: FREE WATER AND OSMOLAR CLEARANCES
Basic Concept
- The kidneys can excrete water and solutes independently.
- When urine is dilute, more water is excreted than solutes.
- When urine is concentrated, more solutes are excreted than water.
Osmolar Clearance (Cosm)
- Osmolar clearance represents the volume of plasma cleared of solutes each minute.
Formula
Cosm=PosmUosm×V
Where:
- Cosm = Osmolar clearance
- Uosm = Urine osmolarity
- V = Urine flow rate
- Posm = Plasma osmolarity
Given Example
- Plasma osmolarity (Posm) = 300 mOsm/L
- Urine osmolarity (Uosm) = 600 mOsm/L
- Urine flow rate (V) = 1 mL/min = 0.001 L/min
Step 1: Calculate Osmolar Excretion Rate
Uosm×V 600×0.001 =0.6mOsm/min
- The kidneys excrete 0.6 mOsm of solute per minute.
Step 2: Calculate Osmolar Clearance
Cosm=3000.6 =0.002L/min
Convert liters to milliliters:0.002×1000=2mL/min
Result
- Osmolar Clearance = 2 mL/min
MeaningFree Water Clearance (CH₂O)
- Free water clearance compares water excretion with solute excretion.
Formula
CH2O=V−Cosm
orCH2O=V−PosmUosm×V
Where:
- CH₂O = Free water clearance
- V = Urine flow rate
- Cosm = Osmolar clearance
Using the Same Example
- Urine flow rate = 1 mL/min
- Osmolar clearance = 2 mL/min
Calculation
CH2O=1−2 =−1mL/min
Result
- Free Water Clearance = –1 mL/min
Meaning
- The kidneys are not losing extra water.
- The kidneys are conserving water.
- Water is being returned to the blood.
- This occurs during dehydration or water deficit.
Interpretation of Free Water Clearance
When CH₂O is Negative
CH2O<0
- Urine osmolarity is greater than plasma osmolarity.
Uosm>Posm
- Urine is concentrated.
- Water is conserved.
- More solutes are excreted than water.
Example
- Plasma osmolarity = 300 mOsm/L
- Urine osmolarity = 600 mOsm/L
Since:600>300
When CH₂O is Positive
CH2O>0
- Urine osmolarity is less than plasma osmolarity.
Uosm<Posm
- Urine is dilute.
- Excess water is being excreted.
- More water is excreted than solutes.
Example
Suppose:
- Plasma osmolarity = 300 mOsm/L
- Urine osmolarity = 100 mOsm/L
Since:100<300
- Urine is dilute.
- Free water clearance becomes positive.
- Solute-free water is being removed from the body.
- Plasma becomes more concentrated.
KEY CONCEPT
- Osmolar Clearance (Cosm) = Volume of plasma cleared of solutes per minute.
Cosm=PosmUosm×V
- Free Water Clearance (CH₂O) = Difference between urine flow and osmolar clearance.
CH2O=V−Cosm
Negative Free Water Clearance
- Concentrated urine
- Urine osmolarity > Plasma osmolarity
- Water conserved
- Dehydration state
Positive Free Water Clearance
- Dilute urine
- Urine osmolarity < Plasma osmolarity
- Excess water excreted
- Water-loaded state
Easy Memory Trick
- CH₂O Positive = Peeing out extra water
- CH₂O Negative = Saving water in the body
DISORDERS OF URINARY CONCENTRATING ABILITY
General Causes of Impaired Urine Concentration and Dilution
- The kidneys may lose the ability to concentrate or dilute urine properly.
- This can occur because of inappropriate ADH secretion.
- Too much ADH can cause abnormal water excretion.
- Too little ADH can also cause abnormal water excretion.
- Impairment of the countercurrent mechanism can reduce urine-concentrating ability.
- A hyperosmotic renal medulla is necessary for maximal urine concentration.
- Even high ADH levels cannot produce maximally concentrated urine if medullary hyperosmolarity is reduced.
- Urine-concentrating ability is also impaired when distal tubules, collecting tubules, and collecting ducts cannot respond to ADH.
Central Diabetes Insipidus: Failure to Produce ADH
- Central diabetes insipidus occurs when ADH cannot be produced or released from the posterior pituitary.
- This condition may be caused by head injury.
- This condition may be caused by infections.
- This condition may be congenital.
- In the absence of ADH, distal nephron segments cannot effectively reabsorb water.
- As a result, a large volume of dilute urine is produced.
- In severe cases, urine volume may exceed 15 L/day.
- Excessive water loss activates the thirst mechanism.
- If adequate water is consumed, major body water deficits usually do not occur.
Clinical Features
- Large volumes of dilute urine are produced.
- Patients develop polydipsia.
- Polydipsia means increased thirst and increased water intake.
- Severe dehydration can occur if water intake is restricted.
- Hypernatremia can also develop rapidly when water intake is restricted.
- This may occur in hospitalized or unconscious patients.
Treatment
- Treatment is administration of desmopressin.
- Desmopressin is a synthetic analogue of ADH.
- Desmopressin acts selectively on V₂ receptors.
- Desmopressin increases water permeability in the late distal tubules and collecting tubules.
- Desmopressin can be given by injection.
- Desmopressin can be given as a nasal spray.
- Desmopressin can be given orally.
- Desmopressin rapidly restores urine output toward normal.
Nephrogenic Diabetes Insipidus: Inability of Kidneys to Respond to ADH
- In nephrogenic diabetes insipidus, ADH levels may be normal or elevated.
- The kidneys fail to respond appropriately to ADH.
- The defect is located in the kidneys.
- The condition is also called arginine vasopressin resistance.
- One cause is failure of the countercurrent mechanism to create a hyperosmotic medulla.
- Another cause is failure of distal tubules, collecting tubules, and collecting ducts to respond to ADH.
- Large volumes of dilute urine are produced.
- Increased urine output can cause dehydration.
- Fluid intake must increase to match urine losses.
Causes
- Renal diseases that damage the renal medulla can impair urine concentration.
- Impaired loop of Henle function can reduce concentrating ability.
- Diuretics such as furosemide can inhibit electrolyte reabsorption in the loop of Henle.
- Furosemide can therefore impair urine-concentrating ability.
- Lithium can impair the response of distal nephron segments to ADH.
- Tetracyclines can impair the response of distal nephron segments to ADH.
- Vasopressin V₂ receptor mutations can cause nephrogenic diabetes insipidus.
- Aquaporin-2 gene mutations can also cause nephrogenic diabetes insipidus.
Clinical Features
- Patients usually present with polyuria.
- Patients usually present with polydipsia.
Diagnosis
- Desmopressin is used to distinguish nephrogenic diabetes insipidus from central diabetes insipidus.
- In nephrogenic diabetes insipidus, desmopressin does not produce a prompt decrease in urine volume.
- Desmopressin does not produce a prompt increase in urine osmolarity.
- Lack of response within 2 hours strongly suggests nephrogenic diabetes insipidus.
Treatment
- The underlying renal disorder should be corrected if possible.
- Hypernatremia can be reduced with a low-sodium diet.
- Hypernatremia can also be reduced with a diuretic that increases sodium excretion.
- Thiazide diuretics can be used for this purpose.
KEY CONCEPT
Urine-concentrating defects occur because of:
- Abnormal ADH secretion
- Defective countercurrent mechanism
- Failure of renal tubules to respond to ADH
- Central Diabetes Insipidus
- ADH deficiency
- Large volume of dilute urine
- Polydipsia
- Responds to desmopressin
- Nephrogenic Diabetes Insipidus
- ADH present but kidneys do not respond
- Large volume of dilute urine
- Polydipsia
- Does not respond to desmopressin
- Central DI = No ADH
- Nephrogenic DI = No renal response to ADH
Z