


- A precise balance between tubular reabsorption and glomerular filtration is essential.
- Multiple nervous mechanisms help regulate tubular reabsorption.
- Multiple hormonal mechanisms help regulate tubular reabsorption.
- Multiple local control mechanisms help regulate tubular reabsorption.
- Similar control mechanisms also regulate glomerular filtration.
- An important feature of tubular reabsorption is that some solutes can be regulated independently of others.
- Hormonal control mechanisms are especially important for this independent regulation.
KEY CONCEPT
- Tubular reabsorption must remain balanced with glomerular filtration.
- Nervous, hormonal, and local mechanisms regulate tubular reabsorption.
- Similar mechanisms also regulate glomerular filtration.
- Different solutes can be regulated independently.
- Hormones play a major role in selective control of tubular reabsorption.
GLOMERULOTUBULAR BALANCE—REABSORPTION RATE INCREASES IN RESPONSE TO INCREASED TUBULAR LOAD
- One of the basic mechanisms controlling tubular reabsorption is the ability of the tubules to increase reabsorption when tubular load increases.
- An increased tubular load means an increased flow of fluid into the tubules.
- This phenomenon is called glomerulotubular balance.
- If GFR increases from 125 mL/min to 150 mL/min, proximal tubular reabsorption also increases.
- Proximal tubular reabsorption may increase from about 81 mL/min to about 97.5 mL/min.
- The total rate of reabsorption increases when the filtered load increases.
- The percentage of GFR reabsorbed by the proximal tubule remains relatively constant at about 65%.
- Some degree of glomerulotubular balance also occurs in other nephron segments.
- This mechanism is especially important in the loop of Henle.
- The exact mechanisms responsible for glomerulotubular balance are not completely understood.
- It may be partly related to changes in physical forces within the tubules and surrounding renal interstitium.
- Higher flow rates in the proximal tubule may increase the availability of ion transporters on the luminal membrane.
- The sodium-hydrogen exchanger is one of the transporters that may become more available.
- Glomerulotubular balance occurs independently of hormonal control.
- This mechanism can be demonstrated in isolated kidneys.
- It can also be demonstrated in isolated proximal tubular segments.
- Glomerulotubular balance helps prevent overloading of the distal tubular segments when GFR increases.
- It acts as a protective mechanism against changes in urine output caused by changes in GFR.
- Renal autoregulatory mechanisms provide another protective mechanism.
- Tubuloglomerular feedback is an important renal autoregulatory mechanism.
- Renal autoregulation helps prevent large changes in GFR.
- Glomerulotubular balance and renal autoregulation work together.
- Together, they prevent large changes in fluid flow reaching the distal tubules.
- These mechanisms help maintain sodium balance and body fluid volume.
- They also protect against disturbances caused by changes in arterial pressure and other factors.
KEY CONCEPT
- Glomerulotubular balance means tubular reabsorption increases when filtered load increases.
- The proximal tubule continues to reabsorb about 65% of the filtered load even when GFR rises.
- This mechanism also occurs in other nephron segments, especially the loop of Henle.
- Glomerulotubular balance works independently of hormones.
- It prevents overload of distal tubules when GFR increases.
- Renal autoregulation and glomerulotubular balance work together to maintain sodium and fluid homeostasis.
PERITUBULAR CAPILLARY AND RENAL INTERSTITIAL FLUID PHYSICAL FORCES
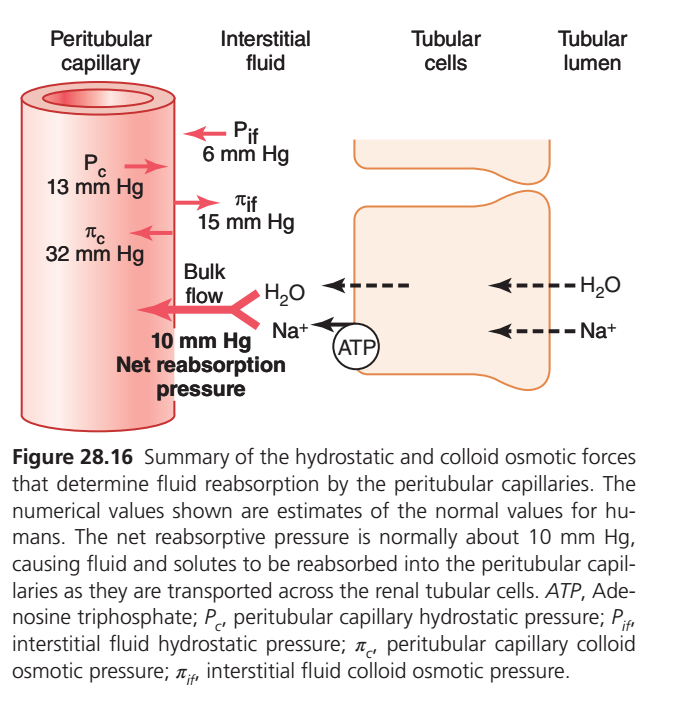
- The final step of tubular reabsorption is the movement of water and solutes from the renal interstitium into the peritubular capillaries.
- This movement occurs by bulk flow through the wall of the peritubular capillaries.
- Hydrostatic forces influence the rate of reabsorption across the peritubular capillaries.
- Colloid osmotic forces also influence the rate of reabsorption across the peritubular capillaries.
- These forces control peritubular capillary reabsorption in the same way they influence filtration in other capillaries.
- These forces also control filtration in the glomerular capillaries.
- Changes in peritubular capillary reabsorption can affect the hydrostatic pressure of the renal interstitium.
- Changes in peritubular capillary reabsorption can also affect the colloid osmotic pressure of the renal interstitium.
- These changes ultimately influence the reabsorption of water and solutes from the renal tubules.
KEY CONCEPT
- The final step of tubular reabsorption occurs from the renal interstitium into the peritubular capillaries.
- Bulk flow carries water and solutes into the blood.
- Hydrostatic and colloid osmotic forces regulate this reabsorption.
- Changes in peritubular capillary reabsorption alter renal interstitial pressures.
- These changes influence tubular reabsorption of water and solutes.
PERITUBULAR CAPILLARY AND RENAL INTERSTITIAL FLUID PHYSICAL FORCES
- The final step of tubular reabsorption is the movement of water and solutes from the renal interstitium into the peritubular capillaries.
- Water and solutes enter the blood through the walls of the peritubular capillaries.
- Hydrostatic forces help determine the rate of reabsorption across the peritubular capillaries.
- Colloid osmotic forces also help determine the rate of reabsorption across the peritubular capillaries.
- These forces control reabsorption in the same way that they control filtration in other capillaries.
- These forces also influence filtration in the glomerular capillaries.
- Changes in peritubular capillary reabsorption can change the hydrostatic pressure of the renal interstitium.
- Changes in peritubular capillary reabsorption can also change the colloid osmotic pressure of the renal interstitium.
- These changes ultimately affect tubular reabsorption of water and solutes.
- Normally, more than 99% of filtered water is reabsorbed as filtrate passes through the renal tubules.
- Most filtered solutes are also reabsorbed.
- Fluid and electrolytes move from the tubules into the renal interstitium.
- From the renal interstitium, they move into the peritubular capillaries.
- The normal rate of peritubular capillary reabsorption is about 124 mL/min.
- Reabsorption across the peritubular capillaries can be calculated using the formula:
- Reabsorption = Kf × Net Reabsorptive Force
- The net reabsorptive force is determined by the combined effects of hydrostatic and colloid osmotic forces.
- Peritubular capillary hydrostatic pressure (Pc) opposes reabsorption.
- Renal interstitial hydrostatic pressure (Pif) favors reabsorption.
- Peritubular capillary plasma colloid osmotic pressure (πc) favors reabsorption.
- Renal interstitial colloid osmotic pressure (πif) opposes reabsorption.
- The normal peritubular capillary hydrostatic pressure is about 13 mm Hg.
- The normal renal interstitial hydrostatic pressure is about 6 mm Hg.
- This creates a hydrostatic pressure gradient of about 7 mm Hg opposing reabsorption.
- The plasma colloid osmotic pressure is about 32 mm Hg.
- The renal interstitial colloid osmotic pressure is about 15 mm Hg.
- This creates a net colloid osmotic force of about 17 mm Hg favoring reabsorption.
- The net colloid osmotic force is greater than the opposing hydrostatic force.
- Therefore, there is an overall net force favoring reabsorption.
- The net reabsorptive force is about 10 mm Hg.
- This force is similar in magnitude to the force in glomerular capillaries but acts in the opposite direction.
- A high filtration coefficient (Kf) also contributes to the high rate of reabsorption.
- The high Kf results from high hydraulic conductivity of the capillaries.
- The large surface area of the capillaries also contributes to a high Kf.
- The normal reabsorption rate is about 124 mL/min.
- The normal net reabsorptive pressure is about 10 mm Hg.
- Therefore, Kf is about 12.4 mL/min per mm Hg.
EASY CALCULATION
- Hydrostatic Force Opposing Reabsorption = Pc − Pif = 13 − 6 = 7 mm Hg
- Colloid Osmotic Force Favoring Reabsorption = πc − πif = 32 − 15 = 17 mm Hg
- Net Reabsorptive Force = Colloid Osmotic Force − Hydrostatic Force = 17 − 7 = 10 mm Hg
- Filtration Coefficient (Kf) Kf = Reabsorption ÷ Net Reabsorptive Force = 124 ÷ 10 = 12.4 mL/min/mm Hg
KEY CONCEPT
- Peritubular capillaries are the final site of tubular reabsorption into the blood.
- Hydrostatic pressure opposes reabsorption.
- Colloid osmotic pressure favors reabsorption.
- Net Hydrostatic Force = 13 − 6 = 7 mm Hg.
- Net Colloid Osmotic Force = 32 − 15 = 17 mm Hg.
- Net Reabsorptive Force = 17 − 7 = 10 mm Hg.
- Reabsorption = Kf × Net Reabsorptive Force.
- Normal Kf = 124 ÷ 10 = 12.4 mL/min/mm Hg.
- Strong reabsorptive forces allow more than 99% of filtered water to be reabsorbed.
This figure explains:
Why water and solutes move from the kidney tubules back into the blood (reabsorption).
The answer is:
✅ The peritubular capillaries are “pulling” much harder than they are “pushing.”
Therefore fluid moves:
Tubular Lumen → Tubular Cell → Interstitial Fluid → Peritubular Capillary (Blood)
STEP 1: FOLLOW THE JOURNEY OF WATER
Water starts in:
🟡 Tubular lumen (future urine)
↓
🟠 Tubular cells
↓
⚪ Interstitial fluid
↓
🔴 Peritubular capillary
↓
Blood circulation
This process is called:
REABSORPTION
STEP 2: WHAT PULLS WATER INTO THE CAPILLARY?
There are 4 Starling Forces.
Think of a Tug-of-War.
Some forces:
✅ Pull water INTO capillary
Some forces:
❌ Push water OUT of capillary
FORCE 1
Pc = 13 mmHg
Peritubular Capillary Hydrostatic Pressure
Think:
💧 Blood pressure inside capillary
It pushes fluid:
➡️ OUT of capillary
Memory
Pc = PUSHES OUT
FORCE 2
πc = 32 mmHg
Capillary Colloid Osmotic Pressure
Created by plasma proteins.
Proteins cannot leave capillary.
They pull water toward themselves.
Effect
⬅️ Pulls fluid INTO capillary
Memory
Proteins PULL
FORCE 3
Pif = 6 mmHg
Interstitial Hydrostatic Pressure
Pressure in tissue space.
It pushes fluid:
⬅️ INTO capillary
Memory
Interstitial pressure PUSHES fluid into capillary
FORCE 4
πif = 15 mmHg
Interstitial Colloid Osmotic Pressure
Proteins in interstitial fluid attract water.
Effect
➡️ Pulls water OUT of capillary
Memory
Interstitial proteins pull water outward
STEP 3: WHO WINS THE TUG OF WAR?
Forces FAVORING REABSORPTION
(Into capillary)
πc = 32
PLUS
Pif = 6
Total:
32 + 6
= 38 mmHg
✅ Pulling into capillary
Forces OPPOSING REABSORPTION
(Out of capillary)
Pc = 13
PLUS
πif = 15
Total:
13 + 15
= 28 mmHg
❌ Pulling out of capillary
NET REABSORPTIVE PRESSURE
38 − 28
= 10 mmHg
✅ Net Reabsorption Pressure
WHAT DOES THIS MEAN?
The capillary is pulling with:
10 mmHg more force
than it is pushing.
Therefore:
💧 Water enters capillary
🧂 Sodium enters capillary
🍬 Glucose enters capillary
🧪 Amino acids enter capillary
STEP 4: WHY IS Na⁺ IMPORTANT?
Look at ATP pump.
The Na⁺/K⁺ ATPase pump is continuously pumping:
Na⁺ OUT of tubular cell
↓
Into interstitial fluid
↓
Toward capillary
Result
Tubular cell Na⁺ stays low.
This causes:
Na⁺ from lumen → cell
to move continuously.
Water follows sodium.
EASY STORY
Imagine:
🏠 Tubule = House
🌳 Interstitial fluid = Yard
🚛 Capillary = Truck
Sodium Pump
Worker carries boxes from house to yard.
Capillary
Truck strongly sucks boxes from yard.
Water
Follows the boxes.
Result:
House becomes empty.
Truck becomes full.
This is reabsorption.
WHY ARE PERITUBULAR CAPILLARIES SO GOOD AT REABSORPTION?
Because they have:
LOW Hydrostatic Pressure
Pc = 13 mmHg
(weak pushing force)
AND
HIGH Protein Osmotic Pressure
πc = 32 mmHg
(strong pulling force)
Therefore:
✅ Perfect design for reabsorption.
SUPER-FAST EXAM MEMORY TABLE
| Force | Value | Action |
|---|---|---|
| Pc | 13 mmHg | Pushes fluid OUT |
| πc | 32 mmHg | Pulls fluid IN |
| Pif | 6 mmHg | Pushes fluid IN |
| πif | 15 mmHg | Pulls fluid OUT |
| Net Reabsorption | 10 mmHg | Fluid enters capillary |
10-SECOND GUYTON EXAM CONCEPT
Peritubular Capillaries = “Fluid Vacuum Cleaner”
🩸 High protein pressure (32 mmHg)
+
🩸 Low capillary pressure (13 mmHg)
⬇️
Create a net reabsorptive force of 10 mmHg
⬇️
Water and solutes move:
Tubule → Interstitium → Peritubular Capillary
⬇️
Reabsorption occurs. ✅
REGULATION OF PERITUBULAR CAPILLARY PHYSICAL FORCES
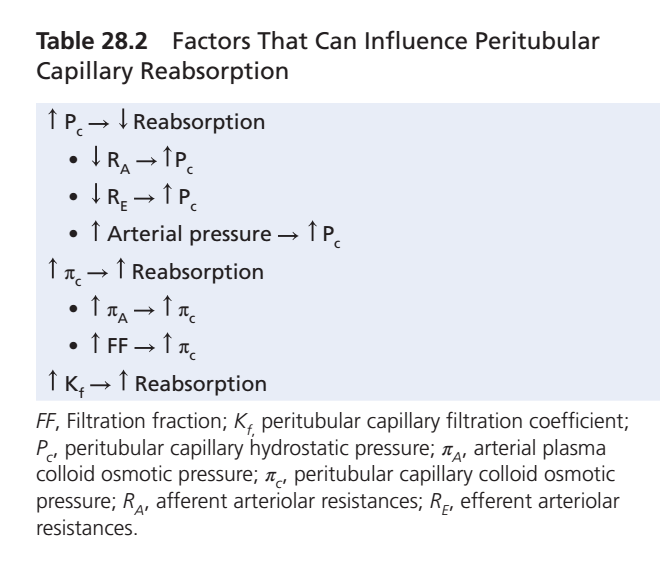
- The two main factors that directly affect peritubular capillary reabsorption are hydrostatic pressure and colloid osmotic pressure in the peritubular capillaries.
- Peritubular capillary hydrostatic pressure is influenced by arterial pressure.
- Peritubular capillary hydrostatic pressure is also influenced by the resistance of blood vessels before the peritubular capillaries.
- The afferent and efferent arterioles are especially important in controlling this pressure.
- An increase in arterial pressure tends to increase peritubular capillary hydrostatic pressure.
- Increased peritubular capillary hydrostatic pressure decreases reabsorption.
- This effect is partially buffered by renal autoregulatory mechanisms.
- Autoregulatory mechanisms help maintain relatively constant renal blood flow.
- Autoregulatory mechanisms also help maintain relatively constant hydrostatic pressures in renal blood vessels.
- An increase in resistance of blood vessels before the peritubular capillaries decreases peritubular capillary hydrostatic pressure.
- A decrease in peritubular capillary hydrostatic pressure tends to increase reabsorption.
- The afferent and efferent arterioles provide much of the pre-peritubular vascular resistance.
- The interlobar, arcuate, and interlobular arteries also contribute to vascular resistance.
- Constriction of the efferent arteriole increases glomerular capillary hydrostatic pressure.
- Constriction of the efferent arteriole decreases peritubular capillary hydrostatic pressure.
- The second major determinant of peritubular capillary reabsorption is plasma colloid osmotic pressure.
- Increasing colloid osmotic pressure increases peritubular capillary reabsorption.
- Peritubular capillary colloid osmotic pressure depends on systemic plasma colloid osmotic pressure.
- An increase in plasma protein concentration increases peritubular capillary colloid osmotic pressure.
- Increased plasma protein concentration increases reabsorption.
- Peritubular capillary colloid osmotic pressure also depends on the filtration fraction.
- A higher filtration fraction increases plasma protein concentration in the peritubular capillaries.
- A higher filtration fraction increases peritubular capillary reabsorption.
- Filtration fraction is defined as GFR divided by RPF.
EASY CALCULATION
- Filtration Fraction (FF) FF = GFR ÷ RPF
- Example: FF = 125 mL/min ÷ 625 mL/min FF = 0.20 = 20%
- Increased GFR increases FF.
- Decreased RPF also increases FF.
- Increased FF increases peritubular capillary colloid osmotic pressure.
- Increased FF increases peritubular capillary reabsorption.
- Some renal vasoconstrictors, such as angiotensin II, increase peritubular capillary reabsorption.
- Angiotensin II decreases renal plasma flow.
- Angiotensin II increases filtration fraction.
- Changes in peritubular capillary Kf can also affect reabsorption.
- Kf represents capillary permeability and surface area.
- An increase in Kf increases reabsorption.
- A decrease in Kf decreases reabsorption.
- Kf remains relatively constant under most physiological conditions.
- Changes in peritubular capillary reabsorption alter the hydrostatic pressure of the renal interstitium.
- Changes in peritubular capillary reabsorption also alter the colloid osmotic pressure of the renal interstitium.
- Reduced peritubular capillary reabsorption increases interstitial hydrostatic pressure.
- Reduced peritubular capillary reabsorption decreases interstitial colloid osmotic pressure.
- These changes reduce reabsorption from the renal tubules into the interstitium.
- Solutes enter the intercellular channels and renal interstitium by active transport or passive diffusion.
- Water follows the solutes into the interstitium by osmosis.
- Water and solutes in the interstitium can enter the peritubular capillaries.
- Water and solutes can also leak back into the tubular lumen.
- Tight junctions of the proximal tubule are somewhat leaky.
- Sodium can move in both directions through these junctions.
- Under normal conditions, high peritubular capillary reabsorption causes net movement of fluid and solutes into the capillaries.
- Under normal conditions, only a small amount leaks back into the tubular lumen.
- Reduced peritubular capillary reabsorption increases interstitial hydrostatic pressure.
- Increased interstitial hydrostatic pressure promotes backleak of water and solutes into the tubular lumen.
- This reduces net tubular reabsorption.
- Increased peritubular capillary reabsorption lowers interstitial hydrostatic pressure.
- Increased peritubular capillary reabsorption raises interstitial colloid osmotic pressure.
- Both effects favor movement of water and solutes from the tubular lumen into the interstitium.
- Backleak into the tubular lumen decreases.
- Net tubular reabsorption increases.
- Uptake of water and solutes by peritubular capillaries is closely matched with tubular reabsorption.
- Factors that increase peritubular capillary reabsorption also increase tubular reabsorption.
- Factors that decrease peritubular capillary reabsorption also decrease tubular reabsorption.
KEY CONCEPT
- Peritubular capillary reabsorption is mainly controlled by hydrostatic pressure, colloid osmotic pressure, and Kf.
- ↑ Arterial Pressure → ↑ Pc → ↓ Reabsorption.
- ↑ Afferent/Efferent Resistance → ↓ Pc → ↑ Reabsorption.
- ↑ Plasma Proteins → ↑ πc → ↑ Reabsorption.
- ↑ Filtration Fraction → ↑ πc → ↑ Reabsorption.
- FF = GFR ÷ RPF.
- ↑ Kf → ↑ Reabsorption.
- ↓ Peritubular Reabsorption → ↑ Interstitial Hydrostatic Pressure → ↑ Backleak → ↓ Tubular Reabsorption.
- ↑ Peritubular Reabsorption → ↓ Backleak → ↑ Tubular Reabsorption.
- In general, factors that increase peritubular capillary reabsorption also increase tubular reabsorption.
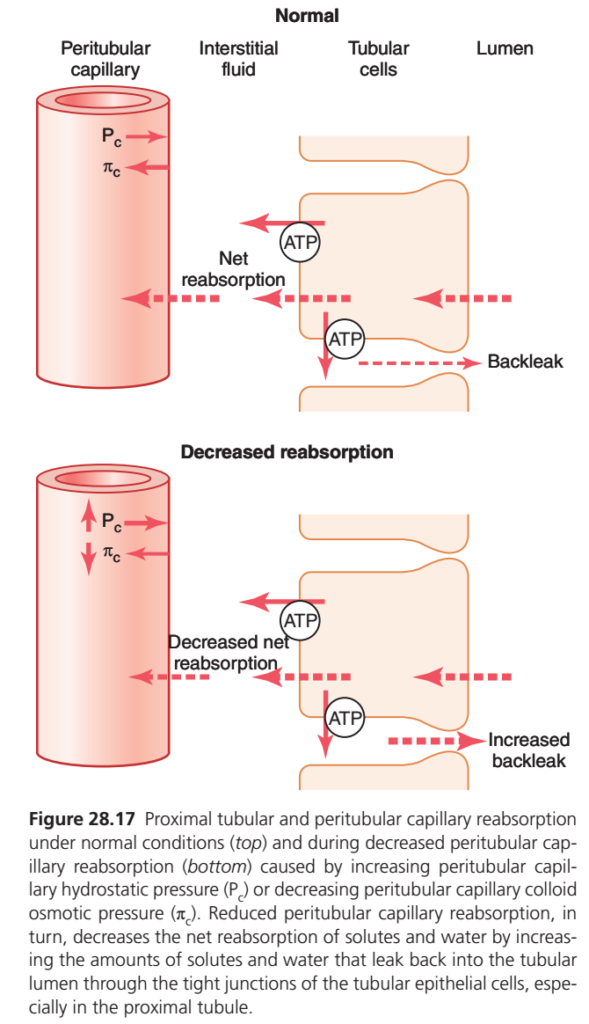
his figure shows:
When peritubular capillaries pull less fluid from the kidney tissue, tubular reabsorption decreases because more water and solutes leak back into the tubule (backleak).
NORMAL SITUATION (TOP FIGURE)
Think of the peritubular capillary as a:
🧲 Powerful Vacuum Cleaner
Normally:
✅ Capillary hydrostatic pressure (Pc) is LOW
✅ Capillary colloid osmotic pressure (πc) is HIGH
Therefore the capillary strongly pulls fluid from the interstitial space.
What Happens?
Step 1
Tubular cells actively pump Na⁺ outward using ATP.
Tubule → Cell → Interstitial Fluid
Step 2
Water follows sodium.
💧 follows 🧂
Step 3
Peritubular capillary immediately removes this fluid.
Interstitial Fluid → Blood
Result
✅ Strong net reabsorption
✅ Little backleak
✅ Efficient fluid recovery
WHAT IS BACKLEAK?
Backleak means:
Some reabsorbed fluid leaks back into the tubular lumen through spaces between tubular cells.
Think of it as:
🚰 Fixing a water leak but some water leaks back through cracks.
Normally:
Only a small amount leaks back.
DECREASED REABSORPTION (BOTTOM FIGURE)
Now imagine the vacuum cleaner becomes weak.
The capillary no longer pulls fluid effectively.
WHY DOES THIS HAPPEN?
Two changes occur:
1. Pc INCREASES
Capillary Hydrostatic Pressure ↑
Normally:
Pc = low
Now:
Pc becomes higher.
Higher pressure pushes fluid outward.
Memory
High Pc = Less Reabsorption
2. πc DECREASES
Capillary Colloid Osmotic Pressure ↓
Normally:
Blood proteins pull water inward.
Now:
Protein pull becomes weaker.
Memory
Low πc = Weak Suction
WHAT HAPPENS NEXT?
The tubular cells are still pumping sodium.
ATP pumps are still working.
But the capillary is no longer removing fluid efficiently.
Interstitial Fluid Starts Accumulating
Fluid collects around the tubules.
Like water accumulating around a drain.
Backleak Increases
Because interstitial fluid builds up:
More fluid leaks back into the tubule.
⬅️ Reabsorbed Fluid
➡️ Back into Tubule
FINAL RESULT
Normal
Reabsorbed = Mostly reaches blood
Decreased Capillary Reabsorption
Reabsorbed = More leaks back
Therefore:
✅ Net reabsorption decreases
EASY STORY
Imagine:
Tubular Cell = Worker 👷
Moves boxes (Na⁺ and water) outside.
Peritubular Capillary = Truck 🚚
Normally:
Truck immediately picks up boxes.
No pile forms.
When Truck Becomes Slow
Boxes accumulate outside.
The pile becomes larger.
Some boxes roll back into the building.
This is:
Backleak
Result:
Less delivery to the blood.
Less reabsorption.
WHY IS THIS IMPORTANT CLINICALLY?
Conditions that increase Pc or decrease πc reduce reabsorption.
Examples:
Increased Pc
- Renal venous congestion
- Heart failure
Decreased πc
- Low plasma proteins
- Liver disease
- Nephrotic syndrome
- Severe malnutrition
SMART EXAM CONCEPT
Normal
Low Pc + High πc
⬇️
Strong capillary suction
⬇️
Strong reabsorption
⬇️
Minimal backleak
Abnormal
High Pc + Low πc
⬇️
Weak capillary suction
⬇️
Interstitial fluid accumulation
⬇️
Increased backleak
⬇️
Decreased net reabsorption
KEY CONCEPT
The tubular cells may continue pumping sodium normally, but if the peritubular capillaries lose their suction power (↑Pc or ↓πc), fluid accumulates in the interstitial space and leaks back into the tubule. As a result, overall reabsorption falls despite normal tubular transport activity. 🎯
EFFECT OF ARTERIAL PRESSURE ON URINE OUTPUT—PRESSURE NATRIURESIS AND PRESSURE DIURESIS
- Even small increases in arterial pressure can greatly increase urinary excretion of sodium.
- Even small increases in arterial pressure can greatly increase urinary excretion of water.
- Increased sodium excretion due to increased arterial pressure is called pressure natriuresis.
- Increased water excretion due to increased arterial pressure is called pressure diuresis.
- Renal autoregulatory mechanisms help maintain relatively stable renal blood flow.
- Renal autoregulatory mechanisms also help maintain relatively stable GFR.
- Therefore, increasing arterial pressure between 75 and 160 mm Hg usually causes only a small change in renal blood flow.
- Increasing arterial pressure between 75 and 160 mm Hg usually causes only a small change in GFR.
- The slight increase in GFR contributes to the increase in urine output.
- When GFR autoregulation is impaired, increases in arterial pressure can produce much larger increases in GFR.
- Increased arterial pressure also decreases the percentage of filtered sodium that is reabsorbed by the tubules.
- Increased arterial pressure decreases the percentage of filtered water that is reabsorbed by the tubules.
- This reduction in tubular reabsorption further increases urine output.
- The exact mechanisms responsible for this effect are not completely understood.
- Both physical factors and hormonal factors contribute to this effect.
- Increased arterial pressure causes a slight increase in peritubular capillary hydrostatic pressure.
- This increase is especially important in the vasa recta of the renal medulla.
- Increased peritubular capillary hydrostatic pressure raises renal interstitial fluid hydrostatic pressure.
- Increased renal interstitial hydrostatic pressure promotes backleak of sodium into the tubular lumen.
- Increased sodium backleak reduces net sodium reabsorption.
- Reduced sodium reabsorption decreases water reabsorption.
- Reduced sodium and water reabsorption increase urine output.
- Reduced angiotensin II formation is another factor that contributes to pressure natriuresis and pressure diuresis.
- Angiotensin II normally increases sodium reabsorption by the renal tubules.
- Angiotensin II also stimulates aldosterone secretion.
- Aldosterone further increases sodium reabsorption.
- Therefore, decreased angiotensin II formation reduces sodium reabsorption.
- Reduced sodium reabsorption contributes to increased sodium and water excretion.
- Internalization of sodium transporter proteins is another factor that may contribute to pressure natriuresis.
- Increased arterial pressure can cause sodium transporters to move from the apical membrane into the cytoplasm.
- This reduces the number of sodium transporters available on the cell membrane.
- Fewer sodium transporters reduce sodium transport across tubular cells.
- Reduced sodium transport decreases sodium reabsorption.
- This effect may be partly caused by decreased angiotensin II formation.
- Other local autacoid and paracrine signals may also contribute to this effect.
KEY CONCEPT
- ↑ Arterial Pressure → ↑ Sodium Excretion = Pressure Natriuresis.
- ↑ Arterial Pressure → ↑ Water Excretion = Pressure Diuresis.
- GFR changes only slightly because of renal autoregulation.
- ↑ Arterial Pressure → ↑ Peritubular Hydrostatic Pressure → ↑ Interstitial Hydrostatic Pressure.
- ↑ Interstitial Hydrostatic Pressure → ↑ Sodium Backleak → ↓ Tubular Reabsorption.
- ↑ Arterial Pressure → ↓ Angiotensin II → ↓ Aldosterone → ↓ Sodium Reabsorption.
- ↑ Arterial Pressure → Internalization of Sodium Transporters → ↓ Sodium Transport.
- Net Effect: ↓ Sodium and Water Reabsorption → ↑ Urine Output.
HORMONAL CONTROL OF TUBULAR REABSORPTION
- Precise regulation of body fluid volumes and solute concentrations requires the kidneys to excrete water and different solutes at variable rates.
- The kidneys can regulate the excretion of water and solutes independently when needed.
- When potassium intake increases, the kidneys must excrete more potassium.
- During increased potassium excretion, normal excretion of sodium and other electrolytes must be maintained.
- When sodium intake changes, the kidneys must adjust sodium excretion accordingly.
- Changes in sodium excretion should occur without major changes in the excretion of other electrolytes.
- Several hormones provide specific control of tubular reabsorption of different electrolytes and water.
- These hormones help the kidneys selectively regulate the excretion and reabsorption of different substances.
- Some hormones act on specific parts of the renal tubule.
- Different hormones produce different effects on solute and water excretion.
- The major hormones involved in regulating tubular reabsorption have specific sites of action in the nephron.
- These hormones help maintain normal body fluid volume and electrolyte balance.
- Some of these hormones are discussed in greater detail in later chapters.
- Their renal tubular actions are briefly reviewed here.
KEY CONCEPT
- Hormones provide precise control of tubular reabsorption.
- Different solutes can be regulated independently.
- Increased potassium intake requires increased potassium excretion.
- Changes in sodium intake require appropriate changes in sodium excretion.
- Hormones act on specific nephron segments.
- Hormonal regulation helps maintain fluid, electrolyte, and volume balance.
- Different hormones selectively control the reabsorption and excretion of water and electrolytes.
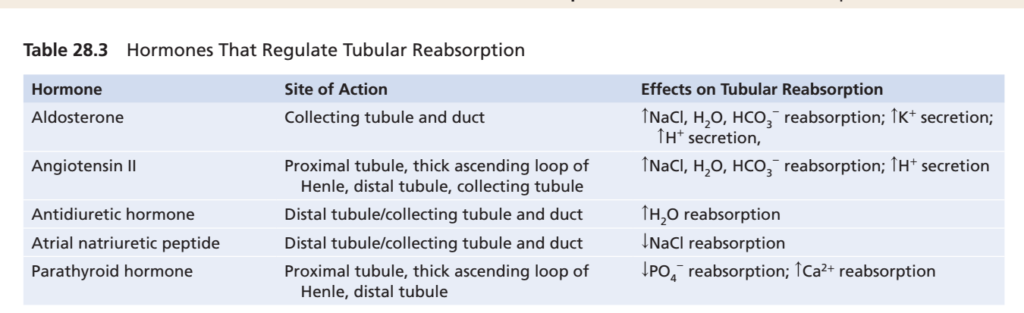
ANGIOTENSIN II INCREASES RENAL SODIUM AND WATER REABSORPTION
- Angiotensin II is one of the most powerful sodium-retaining hormones in the body.
- Angiotensin II formation increases when blood pressure is low.
- Angiotensin II formation also increases when extracellular fluid volume is low.
- Conditions such as hemorrhage increase angiotensin II formation.
- Excessive sweating can increase angiotensin II formation.
- Severe diarrhea can also increase angiotensin II formation.
- Increased angiotensin II helps restore blood pressure toward normal.
- Increased angiotensin II helps restore extracellular fluid volume toward normal.
- Angiotensin II increases sodium and water reabsorption by the renal tubules.
- Angiotensin II stimulates aldosterone secretion.
- Aldosterone increases sodium reabsorption.
- Angiotensin II constricts the efferent arterioles.
- Efferent arteriolar constriction decreases peritubular capillary hydrostatic pressure.
- Reduced peritubular capillary hydrostatic pressure increases tubular reabsorption.
- This effect is especially important in the proximal tubules.
- Efferent arteriolar constriction also reduces renal blood flow.
- Reduced renal blood flow increases the filtration fraction.
EASY CALCULATION
- Filtration Fraction (FF) FF = GFR ÷ RPF
- If RPF decreases while GFR is maintained: FF increases
- ↑ FF → ↑ Plasma Protein Concentration in Peritubular Capillaries
- ↑ FF → ↑ Peritubular Colloid Osmotic Pressure
- ↑ Peritubular Colloid Osmotic Pressure → ↑ Sodium and Water Reabsorption
- Increased filtration fraction increases protein concentration in the peritubular capillaries.
- Increased protein concentration raises peritubular capillary colloid osmotic pressure.
- Increased colloid osmotic pressure increases the reabsorptive force of the peritubular capillaries.
- This further increases sodium and water reabsorption.
- Angiotensin II directly stimulates sodium reabsorption in the proximal tubules.
- Angiotensin II directly stimulates sodium reabsorption in the loop of Henle.
- Angiotensin II directly stimulates sodium reabsorption in the distal tubules.
- Angiotensin II directly stimulates sodium reabsorption in the collecting tubules.
- Angiotensin II stimulates the Na⁺-K⁺ ATPase pump in the basolateral membrane.
- Angiotensin II stimulates sodium-hydrogen exchange in the luminal membrane.
- This effect is especially important in the proximal tubule.
- Angiotensin II also stimulates sodium-bicarbonate co-transport in the basolateral membrane.
- Angiotensin II increases sodium transport across both luminal and basolateral membranes.
- Angiotensin II acts in most renal tubular segments.
- Increased angiotensin II levels cause marked sodium retention.
- Increased angiotensin II levels also cause marked water retention.
- These effects help the body adapt to large changes in sodium intake.
- These adaptations occur without major changes in extracellular fluid volume.
- These adaptations also occur without major changes in blood pressure.
- While increasing sodium reabsorption, angiotensin II also constricts efferent arterioles.
- Efferent arteriolar constriction helps maintain an adequate GFR.
- Maintaining GFR helps preserve excretion of metabolic waste products.
- Urea excretion depends largely on adequate GFR.
- Creatinine excretion also depends largely on adequate GFR.
- During reduced sodium intake, increased angiotensin II helps retain sodium and water.
- At the same time, metabolic waste products continue to be excreted normally.
KEY CONCEPT
- Angiotensin II is a powerful sodium- and water-retaining hormone.
- It increases during low blood pressure and low extracellular fluid volume.
- Angiotensin II increases sodium reabsorption by three mechanisms:
- ↑ Aldosterone secretion.
- ↑ Efferent arteriolar constriction → ↑ Peritubular Reabsorption.
- ↑ Direct tubular sodium transport.
- It stimulates Na⁺-K⁺ ATPase, Na⁺-H⁺ exchange, and Na⁺-HCO₃⁻ co-transport.
- ↑ Angiotensin II → ↑ Sodium Retention + ↑ Water Retention.
- Efferent constriction helps maintain GFR and waste excretion.
- Net Effect: Restore blood pressure and extracellular fluid volume while maintaining excretion of urea and creatinine.
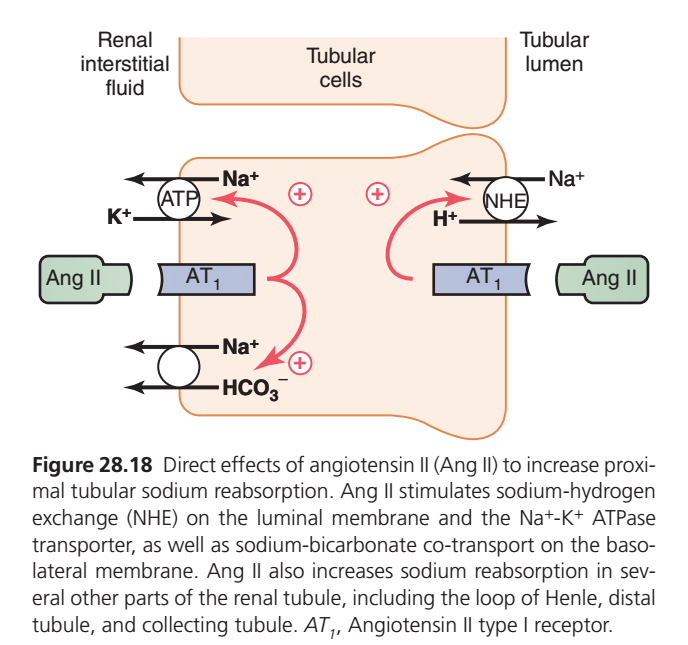
This figure shows:
How Angiotensin II tells the proximal tubule to reabsorb more sodium, bicarbonate, and water, helping the body conserve salt and increase blood volume and blood pressure.
THE EASY STORY
Imagine the body is losing blood or becoming dehydrated.
The body responds by producing:
Angiotensin II (Ang II)
Angiotensin II’s message to the kidney is:
🗣️ “Do not waste salt and water—save them!”WHERE DOES ANGIOTENSIN II ACT?
It acts on:
AT₁ Receptors
located on proximal tubular cells.
Think:
🔑 Angiotensin II = Key
🚪 AT₁ Receptor = Lock
WHAT HAPPENS AFTER ANG II BINDS?
Angiotensin II stimulates three important transporters.
1. Na⁺/H⁺ EXCHANGER (NHE)
Located on the luminal side.
What does it do?
It exchanges:
Na⁺ enters the cell
⬅️
H⁺ leaves the cell
➡️
Result
More sodium is reabsorbed from the tubular fluid.
Easy Memory
Ang II opens the front door for sodium.
2. Na⁺/K⁺ ATPase Pump
Located on the basolateral side.
Uses ATP energy.
What does it do?
Moves:
Na⁺ out of the cell
➡️ Blood
K⁺ into the cell
⬅️Why is this important?
By continuously removing sodium from the cell:
Cellular sodium remains low.
This allows more sodium to enter from the lumen.
Easy Memory
Na⁺/K⁺ ATPase is the engine that keeps sodium moving toward the blood.
3. Na⁺–HCO₃⁻ Cotransporter
Located on the basolateral membrane.
What does it do?
Moves:
Na⁺ + HCO₃⁻
➡️ Into blood
Result
More bicarbonate is reabsorbed.
Easy Memory
Ang II saves bicarbonate together with sodium.
WHAT IS THE OVERALL EFFECT?
Step 1
More Na⁺ enters tubular cells.
⬇️
Step 2
More Na⁺ leaves cells into blood.
⬇️
Step 3
More HCO₃⁻ enters blood.
⬇️
Step 4
Water follows sodium by osmosis.
⬇️
Increased Reabsorption
of:
✅ Sodium
✅ Bicarbonate
✅ Water
WHY DOES WATER FOLLOW?
Water always follows sodium.
When sodium is reabsorbed:
🧂 Na⁺ moves into blood
⬇️
💧 Water follows
⬇️
Blood volume increasesY IS THIS IMPORTANT?
During:
- Dehydration
- Blood loss
- Low blood pressure
the body needs to conserve fluid.
Angiotensin II helps by:
Saving Salt
🧂
Saving Water
💧
Increasing Blood Volume
🩸
Raising Blood Pressure
📈
EASY FLOWCHART
Low Blood Pressure
⬇️
Renin Release
⬇️
Angiotensin II Formation
⬇️
AT₁ Receptor Activation
⬇️
↑ Na⁺/H⁺ Exchanger (NHE)
⬇️
↑ Na⁺/K⁺ ATPase
⬇️
↑ Na⁺–HCO₃⁻ Cotransporter
⬇️
↑ Sodium Reabsorption
⬇️
↑ Water Reabsorption
⬇️
↑ Blood Volume
⬇️
↑ Blood Pressure
IMPORTANT EXAM POINT
Angiotensin II does not act only in the proximal tubule.
It also increases sodium reabsorption in:
- Loop of Henle
- Distal Tubule
- Collecting Tubule
However,
The proximal tubule is its major site of action.
SMARTEST CONCEPTUAL SUMMARY (ESSAY STYLE)
Angiotensin II is one of the body’s most powerful sodium-conserving hormones. When blood pressure or blood volume falls, Angiotensin II levels rise and bind to AT₁ receptors on proximal tubular cells. This stimulates the Na⁺/H⁺ exchanger on the luminal membrane, the Na⁺/K⁺ ATPase pump on the basolateral membrane, and the Na⁺–HCO₃⁻ cotransporter. Together, these transporters greatly increase the reabsorption of sodium and bicarbonate from the tubular fluid into the blood. Because water follows sodium osmotically, water reabsorption also increases. The overall result is conservation of salt and water, expansion of blood volume, and restoration of arterial blood pressure. Thus, Angiotensin II acts as the kidney’s “salt- and water-saving hormone”, helping the body maintain circulatory stability during dehydration, hemorrhage, or hypotension.
KEY CONCEPT
🧠 Angiotensin II tells the kidney: “Save sodium.” When sodium is saved, water automatically follows, leading to increased blood volume and increased blood pressure.
ANTIDIURETIC HORMONE (ADH) INCREASES RENAL WATER REABSORPTION
- The most important renal action of ADH is to increase water reabsorption.
- ADH increases water permeability of the distal tubule.
- ADH increases water permeability of the collecting tubule.
- ADH increases water permeability of the collecting duct.
- This effect helps the body conserve water.
- ADH is especially important during dehydration.
- In the absence of ADH, the distal tubules have low permeability to water.
- In the absence of ADH, the collecting ducts also have low permeability to water.
- Low water permeability causes the kidneys to excrete large amounts of dilute urine.
- This condition is called diabetes insipidus.
- ADH plays a key role in controlling urine concentration and urine dilution.
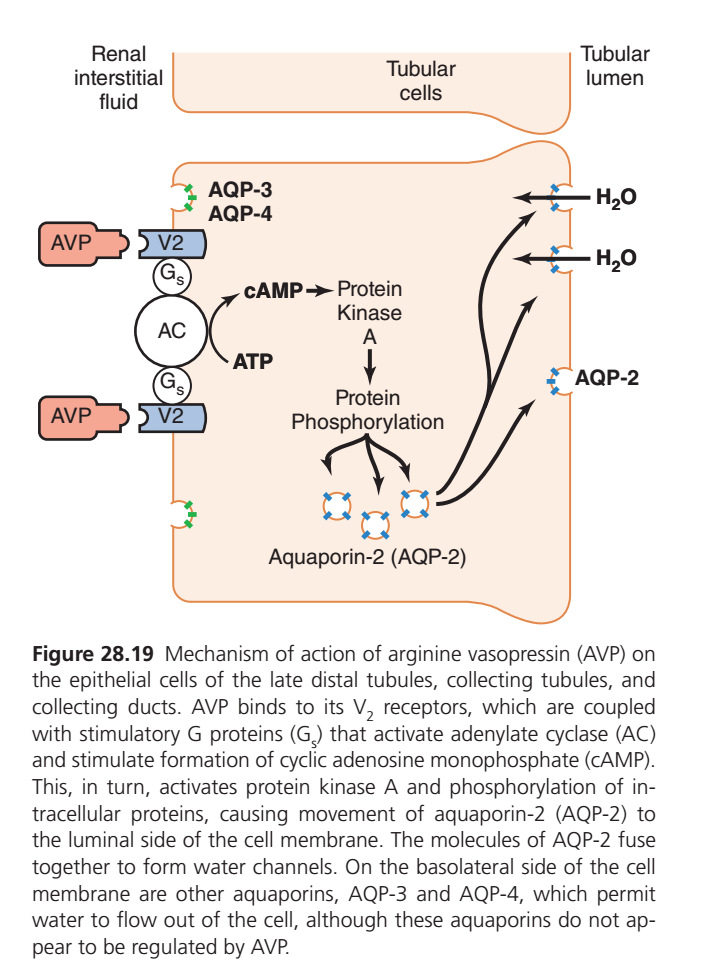
- ADH binds to V₂ receptors in the late distal tubules.
- ADH also binds to V₂ receptors in the collecting tubules.
- ADH also binds to V₂ receptors in the collecting ducts.
- Binding of ADH increases the formation of cyclic adenosine monophosphate (cAMP).
- Increased cAMP activates protein kinases.
- Protein kinases stimulate movement of AQP-2 water channels to the luminal membrane.
- AQP-2 molecules cluster together in the cell membrane.
- AQP-2 molecules fuse with the luminal membrane by exocytosis.
- AQP-2 channels allow rapid diffusion of water through the cells.
- AQP-3 water channels are present in the basolateral membrane.
- AQP-4 water channels are also present in the basolateral membrane.
- AQP-3 and AQP-4 provide a pathway for water to leave the cells.
- AQP-3 and AQP-4 are not regulated by ADH.
- Chronic increases in ADH stimulate the production of more AQP-2 proteins.
- ADH increases AQP-2 formation by stimulating AQP-2 gene transcription.
- When ADH levels decrease, AQP-2 molecules are removed from the luminal membrane.
- AQP-2 molecules return to the cell cytoplasm.
- Removal of AQP-2 channels decreases water permeability.
- Reduced water permeability decreases water reabsorption.
KEY CONCEPT
- ADH is the major hormone controlling water reabsorption.
- ADH increases water permeability in the distal tubule, collecting tubule, and collecting duct.
- Absence of ADH causes excretion of large amounts of dilute urine (diabetes insipidus).
- ADH binds to V₂ receptors.
- ADH → ↑ cAMP → ↑ Protein Kinases.
- Protein kinases move AQP-2 channels to the luminal membrane.
- AQP-2 allows water to enter tubular cells.
- AQP-3 and AQP-4 allow water to leave the cells through the basolateral membrane.
- High ADH → More AQP-2 → More Water Reabsorption.
- Low ADH → Removal of AQP-2 → Less Water Reabsorption.
🎯
This figure explains:
How ADH (AVP, Vasopressin) tells kidney cells to insert water channels (Aquaporin-2) so more water is reabsorbed and urine becomes concentrated.
THE EASY STORY
Imagine the collecting duct cell is a house.
🚪 The wall facing the urine (tubular lumen) normally has very few doors for water.
Therefore:
💧 Water cannot easily enter the cell.
As a result:
➡️ Water stays in urine.
➡️ Large volume of dilute urine is produced.
WHAT HAPPENS WHEN THE BODY NEEDS WATER?
The brain releases:
ADH (Antidiuretic Hormone)
Also called:
AVP (Arginine Vasopressin)
ADH travels in the blood and reaches the kidney.
STEP 1: ADH BINDS TO V2 RECEPTORS
ADH attaches to:
V2 Receptor
located on the blood side (basolateral membrane) of collecting duct cells.
Think:
🔑 ADH = Key
🚪 V2 receptor = Lock
STEP 2: Gs PROTEIN IS ACTIVATED
When ADH binds:
V2 receptor activates:
Gs Protein
Think of Gs as:
📞 A messenger
that carries the signal inside the cell.
STEP 3: ADENYLATE CYCLASE (AC) IS ACTIVATED
Gs stimulates:
Adenylate Cyclase (AC)
This enzyme acts like a factory.
STEP 4: cAMP IS PRODUCED
Adenylate cyclase converts:
ATP
➡️
cAMP
Think:
cAMP = Text Message Inside the Cell
It tells the cell:
📢 “We need to save water!”
STEP 5: PROTEIN KINASE A (PKA) IS ACTIVATED
cAMP activates:
Protein Kinase A (PKA)
PKA is the cell’s worker.
STEP 6: PROTEIN PHOSPHORYLATION
PKA phosphorylates proteins.
This switches on the machinery that moves water channels.
STEP 7: AQUAPORIN-2 (AQP-2) CHANNELS MOVE TO THE MEMBRANE
Inside the cell are stored vesicles containing:
Aquaporin-2 (AQP-2)
PKA causes these vesicles to move and fuse with the luminal membrane.
Before ADH
🚪 Few water doors
↓
Water cannot enter.
After ADH
🚪🚪🚪🚪 Many AQP-2 water doors
↓
Water enters easily.
STEP 8: WATER ENTERS THE CELL
Now water moves:
Tubular Lumen
➡️ AQP-2
➡️ Cell
because the kidney medulla is highly concentrated.
STEP 9: WATER LEAVES THE CELL
On the opposite side of the cell are:
AQP-3
AQP-4
These channels are always present.
They allow water to leave the cell and enter:
Renal Interstitial Fluid
and then the blood.
IMPORTANT DIFFERENCE
AQP-2
✅ Controlled by ADH
✅ Inserted when ADH is present
✅ Located on luminal side
AQP-3 & AQP-4
✅ Always present
✅ Not significantly regulated by ADH
✅ Located on basolateral sideASY MEMORY TRICK
Think of a water tunnel.
AQP-2
Front Door 🚪
Water enters cell.AQP-3 & AQP-4
Back Door 🚪
Water exits cell.
WHAT IS THE FINAL RESULT?
ADH
⬇️
V2 receptor
⬇️
Gs protein
⬇️
Adenylate cyclase
⬇️
cAMP
⬇️
Protein Kinase A
⬇️
AQP-2 inserted
⬇️
More water reabsorption
⬇️
Less water lost in urine
⬇️
Small volume of concentrated urineCLINICAL IMPORTANCE
High ADH
Examples:
- Dehydration
- Blood loss
Results:
✅ More AQP-2
✅ More water reabsorption
✅ Concentrated urineLow ADH
Examples:
- Diabetes Insipidus
Results:
❌ Few AQP-2 channels
❌ Poor water reabsorption
❌ Large volume of dilute urine
SMART EXAM CONCEPT
ADH does not directly move water.
Instead, it:
“Installs Water Channels”
(Aquaporin-2)
and allows water to move by osmosis.
SUPER-SHORT SUMMARY
ADH (AVP) binds to V2 receptors on collecting duct cells and activates the Gs → Adenylate Cyclase → cAMP → Protein Kinase A pathway. This causes Aquaporin-2 channels to be inserted into the luminal membrane, allowing water to enter the cell. Water then exits through Aquaporin-3 and Aquaporin-4 into the blood. The result is increased water reabsorption and production of a small volume of concentrated urine. 🎯
KEY CONCEPT
ADH is the kidney’s “water-saving hormone.” It does not pull water itself; it simply places Aquaporin-2 water doors in the collecting duct so water can move from urine back into the blood. 💧🧲
NATRIURETIC PEPTIDES SECRETED BY THE HEART DECREASE RENAL SODIUM AND WATER REABSORPTION
- Stretch of the cardiac atrial and ventricular muscle cells occurs when plasma volume increases.
- Stretch of the cardiac atrial and ventricular muscle cells also occurs when atrial pressure increases.
- Stretch of these cells stimulates secretion of atrial natriuretic peptide (ANP).
- ANP directly inhibits sodium reabsorption by the renal tubules.
- ANP directly inhibits water reabsorption by the renal tubules.
- This effect is especially important in the collecting ducts.
- ANP causes renal vasodilation.
- ANP decreases renin secretion.
- Reduced renin secretion decreases angiotensin II formation.
- Reduced angiotensin II formation decreases renal tubular reabsorption.
- ANP decreases aldosterone secretion from the adrenal gland.
- ANP acts directly on adrenal glomerulosa cells to reduce aldosterone secretion.
- Reduced angiotensin II formation also contributes to decreased aldosterone secretion.
- All of these effects reduce sodium reabsorption.
- All of these effects reduce water reabsorption.
- These effects increase urinary sodium excretion.
- These effects increase urinary water excretion.
- Increased sodium and water excretion help return blood volume toward normal.
- Stretch of ventricular muscle cells stimulates release of brain natriuretic peptide (BNP).
- BNP has renal effects similar to ANP.
- BNP was first isolated from porcine brain.
- BNP is produced mainly by the cardiac ventricles.
- The main stimulus for BNP release is ventricular stretch.
- Ventricular stretch occurs when ventricular volume increases.
- ANP and BNP act on the same natriuretic peptide receptors (NPRs).
- NPRs are guanylyl cyclase receptors.
- Activation of NPRs increases cyclic guanosine monophosphate (cGMP).
- Increased cGMP activates downstream kinases.
- These kinases mediate the actions of ANP and BNP.
- ANP levels are greatly increased in congestive heart failure.
- BNP levels are also greatly increased in congestive heart failure.
- In heart failure, the atria and ventricles are stretched because of impaired ventricular pumping.
- Increased ANP and BNP help reduce sodium retention in heart failure.
- Increased ANP and BNP help reduce water retention in heart failure.
KEY CONCEPT
- Increased atrial and ventricular stretch stimulates release of ANP and BNP.
- ANP and BNP decrease sodium and water reabsorption.
- ANP causes renal vasodilation.
- ANP decreases renin, angiotensin II, and aldosterone levels.
- ↓ Renin → ↓ Angiotensin II → ↓ Aldosterone → ↓ Sodium Reabsorption.
- ANP and BNP increase urinary sodium and water excretion.
- ANP and BNP act through NPR receptors and cGMP.
- ANP and BNP are elevated in congestive heart failure.
- Net Effect: ↓ Blood Volume, ↓ Sodium Retention, and ↑ Sodium & Water Excretion.
PARATHYROID HORMONE INCREASES RENAL CALCIUM REABSORPTION
- Parathyroid hormone (PTH) is one of the most important hormones regulating calcium in the body.
- The main renal action of PTH is to increase calcium reabsorption by the renal tubules.
- PTH especially increases calcium reabsorption in the distal tubules.
- PTH also increases calcium reabsorption in the connecting tubules.
- The connecting tubule links the distal tubule to the cortical collecting duct.
- PTH inhibits phosphate reabsorption in the proximal tubule.
- PTH stimulates magnesium reabsorption in the loop of Henle.
KEY CONCEPT
- PTH is a major calcium-regulating hormone.
- PTH increases calcium reabsorption in the distal and connecting tubules.
- PTH decreases phosphate reabsorption in the proximal tubule.
- PTH increases magnesium reabsorption in the loop of Henle.
- Net Effect: ↑ Calcium Reabsorption, ↓ Phosphate Reabsorption, and ↑ Magnesium Reabsorption.
SYMPATHETIC NERVOUS SYSTEM ACTIVATION INCREASES SODIUM REABSORPTION
- Severe activation of the sympathetic nervous system can decrease sodium excretion.
- Severe sympathetic activation can also decrease water excretion.
- This occurs by constricting the renal arterioles.
- Renal arteriolar constriction reduces GFR.
- Even low levels of sympathetic activation decrease sodium excretion.
- Even low levels of sympathetic activation decrease water excretion.
- Low levels of sympathetic activation increase sodium reabsorption in the proximal tubule.
- Low levels of sympathetic activation increase sodium reabsorption in the thick ascending limb of the loop of Henle.
- Low levels of sympathetic activation may also increase sodium reabsorption in more distal parts of the renal tubule.
- This effect occurs through activation of α-adrenergic receptors on renal tubular epithelial cells.
- Sympathetic nervous system stimulation increases renin release.
- Increased renin release increases angiotensin II formation.
- Increased angiotensin II further increases tubular reabsorption.
- Increased angiotensin II further decreases renal sodium excretion.
KEY CONCEPT
- Sympathetic nervous system activation increases sodium reabsorption.
- Severe sympathetic activation constricts renal arterioles and decreases GFR.
- Low levels of sympathetic activation directly increase tubular sodium reabsorption.
- This effect occurs through α-adrenergic receptors.
- Sympathetic stimulation increases renin release.
- ↑ Renin → ↑ Angiotensin II → ↑ Tubular Reabsorption.
- Net Effect: ↓ Sodium Excretion and ↓ Water Excretion.