


- Kidney diseases are one of the most common causes of death and disability in many countries around the world.
- In 2023, more than 14% of adults in the United States had Chronic Kidney Disease (CKD).
- This means more than 35.5 million people were estimated to have CKD.
- In addition, millions of other people have Acute Kidney Injury (AKI) or milder forms of kidney dysfunction.
- Severe kidney diseases are divided into two main categories.
1. Acute Kidney Injury (AKI)
- Acute Kidney Injury (AKI) means there is a sudden (abrupt) loss of kidney function.
- This loss of kidney function usually develops within a few days.
- The term Acute Renal Failure is generally used for severe AKI.
- In severe AKI, the kidneys may stop working completely or almost completely.
- In these severe cases, the patient may need renal replacement therapy, such as dialysis.
- Dialysis is discussed later in this chapter.
- Some patients with AKI may recover and regain nearly normal kidney function.
2. Chronic Kidney Disease (CKD)
- Chronic Kidney Disease (CKD) means there is a progressive (gradual) loss of kidney function.
- More and more nephrons gradually stop functioning.
- As the number of working nephrons decreases, overall kidney function also gradually decreases.
Other Kidney Diseases
- Within these two main categories, many specific kidney diseases are present.
- These diseases can affect the kidney blood vessels.
- They can affect the glomeruli.
- They can affect the renal tubules.
- They can affect the renal interstitium.
- They can also affect parts of the urinary tract outside the kidney.
- These parts include the ureters and the bladder.
- This chapter discusses the physiological abnormalities that occur in some of the more common kidney diseases.
KEY CONCEPT
- Kidney diseases are a major cause of illness and death worldwide.
- Severe kidney diseases are classified into Acute Kidney Injury (AKI) and Chronic Kidney Disease (CKD).
- AKI develops suddenly over a few days and may recover.
- CKD develops gradually because of progressive nephron loss.
- Kidney diseases can involve the blood vessels, glomeruli, tubules, renal interstitium, ureters, and bladder.
ACUTE KIDNEY INJURY
- The causes of Acute Kidney Injury (AKI) are divided into three main categories.
1. Prerenal AKI
- Prerenal AKI occurs because of decreased blood supply to the kidneys.
- The cause of reduced blood flow originates outside the kidneys.
- One example is heart failure, where cardiac output decreases.
- Reduced cardiac output leads to low blood pressure.
- Low blood pressure decreases blood flow to the kidneys.
- Another example is severe hemorrhage (heavy bleeding).
- Severe hemorrhage reduces blood volume.
- Reduced blood volume also causes low blood pressure.
- This decreased blood supply can lead to Prerenal AKI.
2. Intrarenal AKI
- Intrarenal AKI results from abnormalities inside the kidney.
- These abnormalities may affect the kidney blood vessels.
- They may affect the glomeruli.
- They may also affect the renal tubules.
3. Postrenal AKI
- Postrenal AKI occurs because of obstruction of the urinary collecting system.
- The blockage can occur anywhere from the calyces to the outflow of the bladder.
- The most common cause of urinary tract obstruction outside the kidney is kidney stones.
- Kidney stones are formed by precipitation of calcium.
- They may also form from urate.
- They may also form from cystine.
Simultaneous Causes of AKI
- In some major causes of AKI, such as sepsis, Prerenal AKI and Intrarenal AKI may occur at the same time.
- Prerenal abnormalities include reduced blood pressure.
- Intrarenal abnormalities include endothelial injury.
- Intrarenal abnormalities also include tubular injury.
PRERENAL ACUTE KIDNEY INJURY CAUSED BY DECREASED BLOOD FLOW TO THE KIDNEY
- The kidneys normally receive about 1100 mL of blood per minute.
- This is about 20% to 25% of the cardiac output.
- The purpose of this high blood flow is to provide enough plasma for glomerular filtration.
- High glomerular filtration is necessary for effective regulation of body fluid volume.
- It is also necessary for regulation of solute concentrations.
- When renal blood flow decreases, GFR also decreases.
- As GFR decreases, urine output of water decreases.
- Urine output of solutes also decreases.
- Conditions that suddenly reduce renal blood flow often cause oliguria.
- Oliguria means urine output is lower than the intake of water and solutes.
- Oliguria causes water to accumulate in the body fluids.
- It also causes solutes to accumulate in the body fluids.
- If renal blood flow is markedly reduced, urine production may stop completely.
- Complete absence of urine production is called anuria.
- If renal blood flow remains above about 20% to 25% of normal, AKI is usually reversible.
- Reversal is possible if the cause of ischemia is corrected before kidney cell damage occurs.
- Compared with many other tissues, the kidney can tolerate a large reduction in blood flow before major cell damage develops.
- When renal blood flow decreases, GFR decreases.
- The amount of sodium chloride filtered by the glomeruli also decreases.
- Filtration of water and other electrolytes also decreases.
- Because less sodium chloride is filtered, less sodium chloride needs to be reabsorbed by the tubules.
- Tubular reabsorption normally uses most of the kidney’s energy and oxygen.
- Therefore, when renal blood flow and GFR decrease, renal oxygen consumption also decreases.
- As GFR approaches zero, kidney oxygen consumption falls to the minimum level needed to keep renal tubular cells alive.
- At this stage, the tubular cells are not reabsorbing sodium.
- If renal blood flow falls below this minimum requirement, the renal cells become hypoxic.
- This minimum blood flow is usually less than 20% to 25% of normal renal blood flow.
- If blood flow continues to decrease for a prolonged period, renal cells become damaged.
- Severe and prolonged reduction in blood flow may even cause death of renal cells.
- The tubular epithelial cells are especially affected.
- If the cause of Prerenal AKI is not corrected, kidney ischemia continues.
- If ischemia lasts longer than a few hours, Prerenal AKI may progress to Intrarenal AKI.
- This progression is discussed later in the chapter.
- Acute reduction in renal blood flow is a common cause of AKI in hospitalized patients.
- It is especially common in patients with severe injuries.
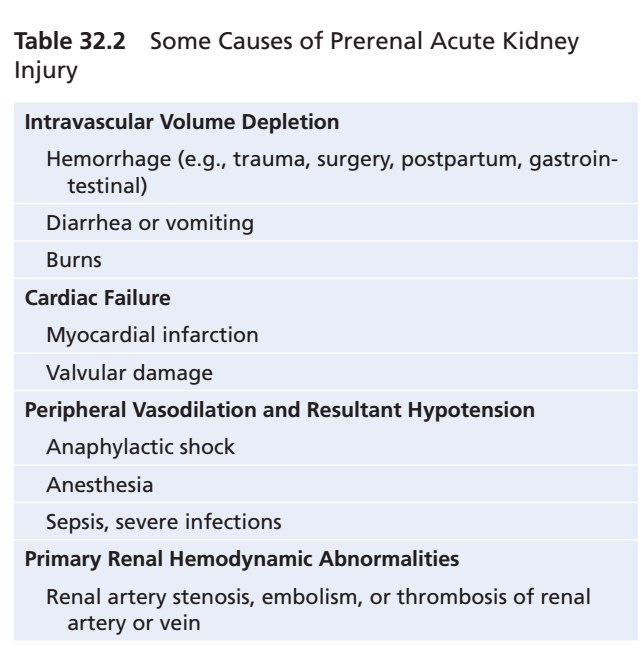
- Table 32.2 shows the common causes of decreased renal blood flow and Prerenal AKI.
KEY CONCEPT
- AKI has three major types: Prerenal, Intrarenal, and Postrenal.
- Prerenal AKI is caused by decreased blood flow to the kidneys.
- Intrarenal AKI is caused by damage within the kidney.
- Postrenal AKI is caused by obstruction of urine flow.
- Normal renal blood flow is about 1100 mL/min (20–25% of cardiac output).
- Decreased renal blood flow causes decreased GFR, oliguria, and, if severe, anuria.
- AKI is usually reversible if renal blood flow stays above 20–25% of normal and ischemia is corrected before cell damage occurs.
- Prolonged severe ischemia can progress from Prerenal AKI to Intrarenal AKI.
- Table Mentioned: Table 32.2
INTRARENAL AKI CAUSED BY ABNORMALITIES IN THE KIDNEY
- Intrarenal AKI occurs because of abnormalities that originate inside the kidney.
- These abnormalities cause a sudden decrease in urine output.
Intrarenal AKI
- Intrarenal AKI is divided into three main types.
- Type 1: Conditions that injure the glomerular capillaries or other small renal blood vessels.
- Type 2: Conditions that damage the renal tubular epithelium.
- Type 3: Conditions that damage the renal interstitium.
- This classification is based on the primary site of injury.
- The renal blood vessels and renal tubules are functionally interdependent.
- Damage to the renal blood vessels can lead to tubular damage.
- Primary tubular damage can also lead to damage of the renal blood vessels.
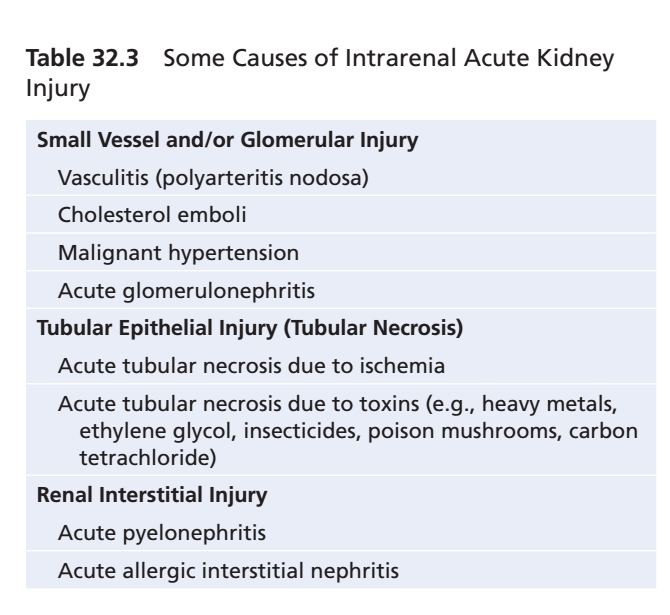
- Table 32.3 lists some causes of Intrarenal AKI.
AKI Caused By Glomerulonephritis
- Acute glomerulonephritis is a type of Intrarenal AKI.
- It is usually caused by an abnormal immune reaction.
- This immune reaction damages the glomeruli.
- In about 95% of patients, glomerular damage develops 1 to 3 weeks after an infection elsewhere in the body.
- The infection is often caused by certain types of group A beta streptococci.
- The previous infection may be a streptococcal sore throat.
- It may be streptococcal tonsillitis.
- It may also be a streptococcal skin infection.
- The infection itself does not damage the kidneys.
- Over the next few weeks, the body produces antibodies against streptococcal antigens.
- The antibodies combine with the antigens.
- This forms an insoluble immune complex.
- The immune complex becomes trapped in the glomeruli.
- It is especially trapped in the glomerular basement membrane.
- After the immune complex is deposited, many glomerular cells begin to proliferate.
- The mesangial cells proliferate the most.
- Mesangial cells are located between the endothelium and epithelium.
- Large numbers of white blood cells become trapped in the glomeruli.
- Many glomeruli become blocked by the inflammatory reaction.
- Glomeruli that are not blocked become excessively permeable.
- This increased permeability allows proteins to leak into the glomerular filtrate.
- It also allows red blood cells to leak into the glomerular filtrate.
- In severe cases, complete or almost complete renal shutdown may occur.
- Acute inflammation of the glomeruli usually subsides within about 2 weeks.
- In most patients, kidney function returns to almost normal.
- Recovery usually occurs within the next few weeks to a few months.
- Sometimes, many glomeruli are permanently destroyed.
- In a small percentage of patients, kidney function continues to deteriorate.
- Progressive deterioration eventually leads to Chronic Kidney Disease (CKD).
- This is discussed later in the chapter.
Tubular Necrosis as a Cause of AKI
- Another cause of Intrarenal AKI is tubular necrosis.
- Tubular necrosis means destruction of the epithelial cells of the renal tubules.
- Two common causes of tubular necrosis are:
- Severe ischemia with inadequate oxygen and nutrient supply to tubular epithelial cells.
- Poisons, toxins, or medications that destroy tubular epithelial cells.
Acute Tubular Necrosis Caused By Severe Renal Ischemia
- Severe renal ischemia can occur because of circulatory shock.
- It can also result from other conditions that greatly reduce kidney blood supply.
- If ischemia becomes severe, delivery of oxygen and nutrients to tubular epithelial cells decreases greatly.
- If the ischemia continues for a prolonged period, tubular epithelial cells become damaged or destroyed.
- When the damage is severe, tubular epithelial cells slough off.
- These detached cells plug many nephrons.
- Blocked nephrons produce no urine.
- Even if renal blood flow returns to normal, the affected nephrons may still fail to excrete urine.
- This continues as long as the tubules remain plugged.
- The most common cause of ischemic tubular damage is Prerenal AKI associated with circulatory shock.
- This was discussed earlier in the chapter.
Acute Tubular Necrosis Caused By Toxins or Medications
- Many poisons and medications can damage the renal tubular epithelium.
- This damage can cause Acute Kidney Injury (AKI).
- Examples include carbon tetrachloride.
- Examples also include heavy metals, such as mercury and lead.
- Another example is ethylene glycol, a major component of antifreeze.
- Various insecticides can also cause damage.
- Some antibiotics, such as tetracyclines, can damage the tubules.
- Cis-platinum, used to treat certain cancers, can also damage the tubules.
- Each of these substances has a specific toxic effect on renal tubular epithelial cells.
- They cause death of many tubular epithelial cells.
- Dead epithelial cells slough off from the basement membrane.
- These cells plug the renal tubules.
- In some cases, the basement membrane is also destroyed.
- If the basement membrane remains intact, new tubular epithelial cells can grow along its surface.
- The damaged tubule may repair itself within 10 to 20 days.
KEY CONCEPT
- Intrarenal AKI is caused by damage within the kidney.
- It mainly affects the glomeruli, renal blood vessels, renal tubules, or renal interstitium.
- Glomerulonephritis is usually caused by an immune reaction, not by the infection itself.
- Immune complexes become trapped in the glomerular basement membrane, causing inflammation and increased permeability.
- Severe glomerular injury may cause renal shutdown or progress to CKD.
- Tubular necrosis results from severe ischemia or toxic substances/medications.
- Sloughed tubular epithelial cells can block nephrons and stop urine formation.
- If the basement membrane remains intact, tubular repair can occur within 10–20 days.
- Table Mentioned: Table 32.3
POSTRENAL AKI CAUSED BY ABNORMALITIES OF THE LOWER URINARY TRACT
- Multiple abnormalities of the lower urinary tract can block or partially block urine flow.
- These abnormalities can cause Acute Kidney Injury (AKI).
- This can occur even when the kidneys initially have a normal blood supply and normal function.
- If only one kidney has reduced urine output, major changes in body fluid composition usually do not occur.
- The opposite (contralateral) kidney increases its urine output.
- This helps maintain normal extracellular electrolyte levels.
- It also maintains normal extracellular solute concentrations.
- It also helps maintain normal extracellular fluid volume.
- In Postrenal AKI, normal kidney function can be restored if the underlying cause is corrected within a few hours.
- If urinary tract obstruction continues for several days or weeks, it can cause irreversible kidney damage.
- Some causes of Postrenal AKI include:
- Bilateral obstruction of the ureters or renal pelvises caused by large stones or blood clots.
- Bladder obstruction caused by cancer.
- Urethral obstruction caused by scar tissue, prostate hypertrophy, or cancer.
PHYSIOLOGICAL EFFECTS OF AKI
- A major physiological effect of AKI is the retention of water in the body.
- AKI also causes retention of metabolic waste products.
- It also causes retention of electrolytes in the blood and extracellular fluid.
- Retention of water and salt can cause fluid overload.
- Fluid overload can lead to edema.
- Fluid overload can also lead to hypertension.
- Retention of potassium is often a more serious problem in patients with AKI.
- Increased plasma potassium concentration is called hyperkalemia.
- Hyperkalemia above 8 mEq/L (about twice the normal level) can be fatal.
- The kidneys are also unable to excrete enough hydrogen ions.
- As a result, patients with AKI may develop metabolic acidosis.
- Metabolic acidosis can be life-threatening.
- It can also worsen hyperkalemia.
- In the most severe cases of AKI, complete anuria occurs.
- Anuria means complete absence of urine production.
- Without restoration of kidney function or treatment, the patient may die within 8 to 14 days.
- Survival requires either recovery of kidney function or use of an artificial kidney.
- An artificial kidney removes:
- Excess water.
- Excess electrolytes.
- Excess metabolic waste products.
- Other effects of decreased urine output and treatment with an artificial kidney are discussed later in relation to Chronic Kidney Disease (CKD).
KEY CONCEPT
- Postrenal AKI is caused by obstruction of urine flow in the lower urinary tract.
- If one kidney is obstructed, the contralateral kidney can usually maintain normal body fluid balance.
- Early removal of the obstruction can restore normal kidney function.
- Prolonged obstruction for several days or weeks can cause irreversible kidney damage.
- AKI causes retention of water, electrolytes, and metabolic waste products.
- Water and salt retention lead to edema and hypertension.
- Hyperkalemia (>8 mEq/L) and metabolic acidosis are life-threatening complications.
- Complete anuria without treatment may cause death within 8–14 days.
CKD IS OFTEN ASSOCIATED WITH IRREVERSIBLE LOSS OF FUNCTIONAL NEPHRONS
- Chronic Kidney Disease (CKD) is usually defined as kidney damage or decreased kidney function that lasts for at least 3 months.
- CKD is often associated with progressive and irreversible loss of functioning nephrons.
- Serious clinical symptoms usually do not appear until the number of functional nephrons decreases by about 70% to 75% below normal.
- Blood concentrations of most electrolytes can still remain relatively normal until the number of functioning nephrons falls below 20% to 25% of normal.
- Body fluid volume can also remain normal until functioning nephrons decrease to less than 20% to 25% of normal.
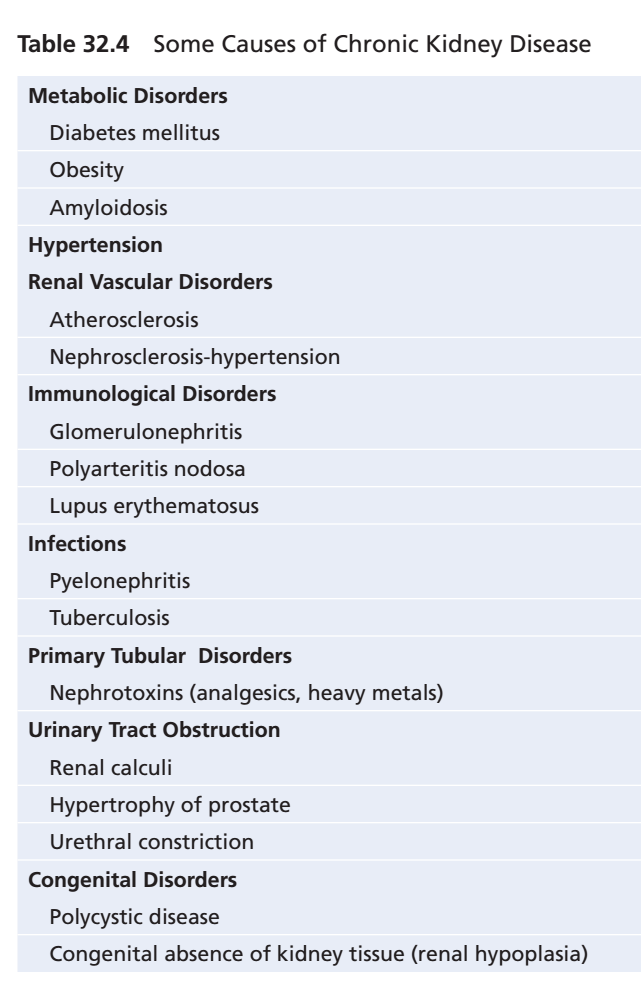
- Table 32.4 lists some of the most important causes of CKD.
- Like Acute Kidney Injury (AKI), CKD can occur because of disorders affecting:
- Renal blood vessels
- Glomeruli
- Renal tubules
- Renal interstitium
- Lower urinary tract
- Although many different disorders can cause CKD, the final outcome is the same.
- The final result is a decrease in the number of functional nephrons.
VICIOUS CYCLE OF CKD LEADING TO END-STAGE RENAL DISEASE
- In some patients, an initial kidney injury causes progressive deterioration of kidney function.
- Progressive deterioration causes continuous loss of nephrons.
- Eventually, kidney function becomes so poor that the patient requires dialysis or kidney transplantation to survive.
- This condition is called End-Stage Renal Disease (ESRD).
- Experimental studies show that surgical removal of a large portion of the kidney causes adaptive changes in the remaining nephrons.
- These adaptive changes increase:
- Renal blood flow
- Glomerular Filtration Rate (GFR)
- Urine output of the surviving nephrons
- The exact mechanisms of these adaptive changes are not completely understood.
- The adaptive changes include hypertrophy (growth) of structures in the surviving nephrons.
- They also include functional changes that:
- Decrease vascular resistance
- Decrease tubular reabsorption in the surviving nephrons
- These adaptive changes allow a person to excrete normal amounts of water and solutes.
- This is possible even when kidney mass is reduced to 20% to 25% of normal.
- After several years, these adaptive changes may begin to damage the remaining nephrons.
- The glomeruli are especially affected.
- Progressive injury may be partly caused by increased pressure or stretching of the remaining glomeruli.
- This increased pressure occurs because of:
- Functional vasodilation of the afferent arterioles
- Increased blood pressure
- Chronic increases in pressure and stretch damage the small arterioles and glomeruli.
- This causes sclerosis.
- Sclerosis means replacement of normal tissue with connective tissue.
- These sclerotic lesions may eventually destroy (obliterate) the glomerulus.
- This causes a further decrease in kidney function.
- Loss of kidney function causes more adaptive changes in the remaining nephrons.
- These adaptive changes produce a slowly progressing vicious cycle.
- This vicious cycle eventually leads to End-Stage Renal Disease (ESRD).
- Figure 32.2 illustrates this vicious cycle leading to ESRD.
- One effective way to slow the progression of CKD is to reduce arterial pressure.
- It is also important to reduce glomerular hydrostatic pressure.
- This can be achieved by using:
- Angiotensin-Converting Enzyme (ACE) inhibitors
- Angiotensin II (Ang II) receptor antagonists
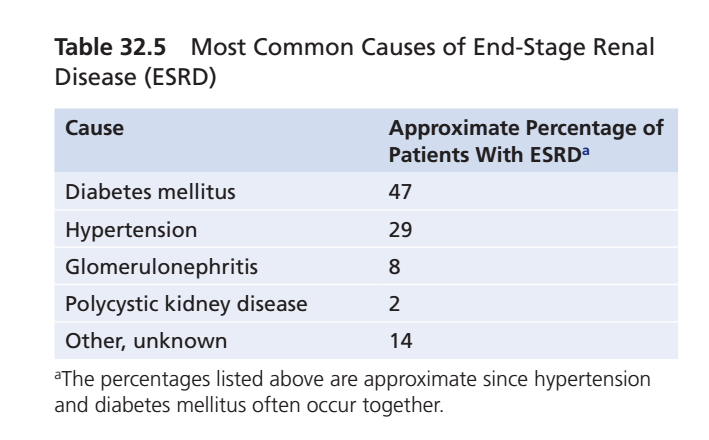
- Table 32.5 lists the most common causes of ESRD.
- In the early 1980s, glomerulonephritis was believed to be the most common initiating cause of ESRD.
- More recently, diabetes mellitus and hypertension have become the leading causes of ESRD.
- Together, they account for more than 75% of all ESRD cases.
- Obesity (excessive weight gain) appears to be the most important risk factor for diabetes and hypertension.
- Diabetes and hypertension often occur together.
- They also interact synergistically to cause kidney damage.
- As discussed in Chapter 79, Type 2 diabetes is closely linked to obesity.
- Type 2 diabetes accounts for 90% to 95% of all cases of diabetes mellitus.
- Excess body weight is also a major cause of essential hypertension.
- It accounts for 65% to 75% of the risk of developing hypertension in adults.
- Besides causing kidney damage through diabetes and hypertension, obesity may also have additive or synergistic effects.
- These effects can further worsen kidney function in patients who already have preexisting kidney disease.
KEY CONCEPT
- CKD is defined as kidney damage or reduced kidney function lasting at least 3 months.
- CKD causes progressive and irreversible loss of functional nephrons.
- Clinical symptoms usually appear after 70–75% nephron loss.
- Normal body fluid balance can often be maintained until nephron function falls below 20–25% of normal.
- Remaining nephrons initially adapt by increasing blood flow, GFR, and urine output.
- Long-term adaptation increases glomerular pressure, leading to glomerular sclerosis and further nephron loss.
- This creates a vicious cycle that eventually progresses to End-Stage Renal Disease (ESRD).
- ACE inhibitors and Ang II receptor antagonists help slow CKD progression by reducing arterial and glomerular pressure.
- Diabetes mellitus and hypertension are the leading causes of ESRD, accounting for more than 75% of cases.
- Obesity is the major risk factor for both diabetes and hypertension, and can further worsen existing kidney disease.
- Figure Mentioned: Figure 32.2
- Tables Mentioned: Table 32.4, Table 32.5
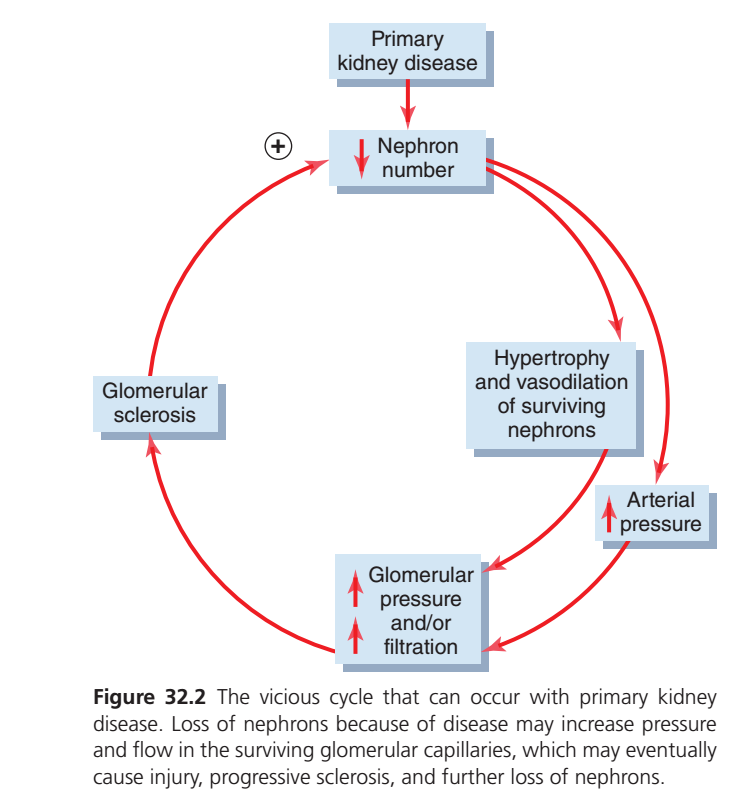
This figure explains one of the most important concepts in Chronic Kidney Disease (CKD) called the “Vicious Cycle of Progressive Kidney Damage.”
The easiest way to understand it is:
When some nephrons die, the remaining nephrons have to work much harder. At first, this helps the kidneys, but over time this extra workload damages the remaining nephrons, causing even more nephron loss. This cycle continues until chronic kidney disease progressively worsens.
Let’s explain every box, every arrow, every symbol, and every pathway in the easiest conceptual way.
Overall Idea of the Figure
Imagine a factory with 100 workers.
One day, 30 workers become sick and leave.
Now only 70 workers remain.
Will the work stop?
No.
The remaining 70 workers have to do the work of 100 workers.
Initially, they manage by working overtime.
But after months,
they become exhausted,
start getting injured,
and more workers leave.
Now only 50 workers remain.
The remaining 50 work even harder.
Eventually almost everyone becomes exhausted.
That is exactly what happens in the kidneys.
Here,
Workers = Nephrons
First Box
Primary Kidney Disease
This is the starting point.
Examples include
- Diabetes
- High blood pressure
- Glomerulonephritis
- Polycystic kidney disease
- Lupus nephritis
These diseases damage the kidneys first.
Think of this as
Healthy kidney
↓
Disease attacks kidneyRed Arrow Downward
The arrow means
The kidney disease causes
↓
loss of nephrons.
Second Box
↓ Nephron Number
The downward arrow means
The number of functioning nephrons decreases.
Suppose
Initially
1 million nephronsDisease destroys
300,000Now only
700,000remain.
These surviving nephrons are still alive.
Question
Does the body simply accept less kidney function?
No.
The body tries to compensate.
Red Arrow Toward the Right
Because fewer nephrons remain,
each surviving nephron has to do more work.
Third Box
Hypertrophy and Vasodilation of Surviving Nephrons
This box has two important words.
Hypertrophy
Hypertrophy means
Increase in size.
The surviving nephrons become larger.
Think of a muscle.
If one arm is injured,
the other arm becomes stronger and bigger because it does more work.
The same happens here.
Remaining nephrons enlarge.
Vasodilation
Vasodilation means
the blood vessels widen.
Why?
Because the surviving nephrons need more blood.
More blood
↓
More filtration
↓
More work can be done.
Think of widening a road.
Small road
↓
Less traffic
Wide road
↓
More traffic
The kidney widens the blood vessels so more blood reaches each surviving nephron.
Why Does This Happen?
The body wants to keep
- GFR normal
- Waste removal normal
- Urine production normal
Even though many nephrons are gone.
Initially,
this compensation is helpful.
Next Arrow
Now look at the arrow going downward.
Fourth Box
↑ Glomerular Pressure and/or ↑ Filtration
Notice there are two upward arrows (↑).
They mean increase.
Both can increase:
- Glomerular pressure
- Filtration (GFR per nephron)
What is Glomerular Pressure?
Normally,
blood enters the glomerulus under a certain pressure.
After nephron loss,
more blood is forced through each surviving glomerulus.
Pressure rises.
Think of a water pipe.
Normal flow
──────►Now half the pipes are blocked.
The same amount of water must pass through fewer pipes.
What happens?
Pressure increases.
Exactly the same thing occurs in the kidneys.
Increased Filtration
Each nephron now filters more plasma than before.
Normally
One nephron filters
100 unitsAfter nephron loss
One nephron filters
150 unitsThis is called
Hyperfiltration
Initially This Is Good
Because total kidney function remains close to normal.
But…
There is a hidden problem.
High Pressure Damages the Glomerulus
Imagine filling a balloon.
Normal pressure
↓
Safe
Very high pressure
↓
Balloon stretches
↓
Eventually tears
Exactly the same happens here.
The glomerular capillaries are exposed to excessive pressure for years.
Eventually they become damaged.
Next Box
Glomerular Sclerosis
This is the dangerous stage.
What is Sclerosis?
Sclerosis means
Hardening
Scarring
Permanent damage
Healthy glomerulus
Soft
Filters bloodDamaged glomerulus
Scarred
Cannot filterOnce sclerosis develops,
that nephron becomes non-functional.
Red Arrow Going Back Up
Notice
The arrow returns to
↓
Nephron number.
Why?
Because
Scarred glomeruli die.
Therefore
More nephrons are lost.
This Is the Vicious Cycle
Now we return to the beginning.
The cycle becomes
Nephron loss
↓
Remaining nephrons work harder
↓
Hypertrophy
↓
Hyperfiltration
↓
High glomerular pressure
↓
Glomerular damage
↓
Glomerular sclerosis
↓
More nephron loss
↓
Remaining nephrons work even harder
↓
Even more damage
↓
More nephron loss
↓
Cycle repeatsThis is why CKD usually gets worse over time if the underlying causes are not controlled.
Extra Pathway on the Right Side
Notice another arrow.
It points toward
↑ Arterial Pressure
The upward arrow means
Blood pressure increases.
Why Does Blood Pressure Rise?
Damaged kidneys
↓
Activate RAAS
↓
Retain sodium
↓
Retain water
↓
Blood volume increases
↓
Blood pressure increases.
High blood pressure now worsens kidney damage.
How Does High Blood Pressure Harm the Kidneys?
High arterial pressure
↓
Higher glomerular pressure
↓
More hyperfiltration
↓
More sclerosis
↓
More nephron loss.
So hypertension both results from kidney disease and accelerates kidney damage.
The Plus (+) Sign
Notice the small plus (+) symbol near the arrow.
This means
Positive feedback.
Positive feedback means
The process makes itself stronger.
Instead of stopping,
it keeps accelerating.
For example:
Lose nephrons
↓
Remaining nephrons overwork
↓
More injury
↓
Lose even more nephrons
↓
Even greater workload
↓
More injuryEach round amplifies the next.
Why Is This Figure Clinically Important?
This figure explains why doctors try to reduce hyperfiltration and glomerular pressure in CKD.
Medications such as ACE inhibitors and ARBs lower pressure inside the glomerulus. Although they may slightly reduce GFR at first, they protect the remaining nephrons over the long term by slowing this vicious cycle.
One-Line Explanation of Every Box
| Box | Meaning |
|---|---|
| Primary kidney disease | The original disease injures the kidneys. |
| ↓ Nephron number | Some nephrons are destroyed and lost. |
| Hypertrophy and vasodilation of surviving nephrons | The remaining nephrons enlarge and receive more blood to compensate. |
| ↑ Glomerular pressure and/or ↑ Filtration | Each surviving nephron filters more blood under higher pressure (hyperfiltration). |
| Glomerular sclerosis | Persistent high pressure scars the glomeruli, making them non-functional. |
| ↑ Arterial pressure | Hypertension develops or worsens, further increasing glomerular pressure and kidney injury. |
| (+) Symbol | Indicates a positive feedback loop in which kidney damage promotes further kidney damage. |
Complete Flow of the Figure
Primary kidney disease
↓
Loss of nephrons
↓
Surviving nephrons enlarge (hypertrophy)
and receive more blood (vasodilation)
↓
Hyperfiltration and increased glomerular pressure
↓
Damage to glomerular capillaries
↓
Glomerular sclerosis (scarring)
↓
More nephron loss
↓
The remaining nephrons must work even harder
↓
The cycle repeats and chronic kidney disease progressesKEY CONCEPT (Exam Point)
- Primary kidney disease destroys functioning nephrons.
- The remaining nephrons compensate by enlarging (hypertrophy) and filtering more blood (hyperfiltration).
- Hyperfiltration increases glomerular pressure, which gradually damages the glomerular capillaries.
- Damaged glomeruli develop glomerular sclerosis (scarring) and stop functioning.
- This causes further nephron loss, forcing the remaining nephrons to work even harder.
- High arterial pressure (hypertension) further increases glomerular pressure and accelerates kidney injury.
- This positive feedback (“vicious cycle”) explains why chronic kidney disease often progresses unless the underlying disease and blood pressure are effectively controlled.
RENAL VASCULAR INJURY AS A CAUSE OF CKD
- Many vascular (blood vessel) lesions can cause renal ischemia.
- Renal ischemia can lead to death of kidney tissue.
- The most common vascular lesions are:
- Atherosclerosis of the large renal arteries, causing progressive sclerotic narrowing (constriction) of the vessels.
- Fibromuscular hyperplasia of one or more large renal arteries, causing occlusion (blockage) of the vessels.
- Nephrosclerosis, caused by sclerotic lesions of the small arteries, arterioles, and glomeruli.
Effects of Large Renal Artery Lesions
- Atherosclerotic or hyperplastic lesions of the large renal arteries often affect one kidney more than the other.
- This causes unilateral (one-sided) reduction in kidney function.
- As discussed in Chapter 19, hypertension often develops when:
- The artery of one kidney is narrowed.
- The artery of the other kidney remains normal.
- This condition is similar to two-kidney Goldblatt hypertension.
Benign Nephrosclerosis
- Benign nephrosclerosis is the most common form of kidney disease.
- It is found in about 70% of postmortem examinations in people who die after 60 years of age.
- This vascular lesion mainly affects:
- Small interlobular arteries
- Afferent arterioles of the kidney
- It is believed to begin with leakage of plasma through the intimal membrane of these blood vessels.
- Plasma leakage causes fibrinoid deposits to develop in the medial layer of the vessels.
- This is followed by progressive thickening of the vessel wall.
- The thickened vessel wall gradually narrows the blood vessel.
- In some cases, the vessel becomes completely occluded (blocked).
Figure 32.2
- Figure 32.2 shows the vicious cycle of primary kidney disease.
- Loss of nephrons increases:
- Glomerular pressure
- Glomerular blood flow (filtration)
- Increased pressure and filtration eventually cause:
- Glomerular injury
- Progressive glomerular sclerosis
- Further nephron loss
- Surviving nephrons undergo:
- Hypertrophy
- Vasodilation
- These changes continue the vicious cycle, eventually leading to End-Stage Renal Disease (ESRD).
Table 32.5 – Most Common Causes of End-Stage Renal Disease (ESRD)
| Cause | Approximate Percentage of Patients with ESRD |
|---|---|
| Diabetes mellitus | 47% |
| Hypertension | 29% |
| Glomerulonephritis | 8% |
| Polycystic kidney disease | 2% |
| Other / Unknown | 14% |
- The percentages are approximate because diabetes mellitus and hypertension often occur together.
Effects of Occlusion of Small Renal Arteries
- The small renal arteries have almost no collateral circulation.
- Therefore, blockage of one or more small arteries destroys a similar number of nephrons.
- The damaged kidney tissue is replaced by small amounts of fibrous tissue.
- When sclerosis occurs in the glomeruli, it is called glomerulosclerosis.
Age-Related Changes
- Nephrosclerosis and glomerulosclerosis develop to some extent in most people after the fourth decade of life.
- There is approximately a 10% decrease in functional nephrons every 10 years after the age of 40 years.
- Figure 32.3 illustrates this age-related nephron loss.
- Loss of glomeruli causes:
- Progressive decrease in renal blood flow
- Progressive decrease in Glomerular Filtration Rate (GFR)
- Even in healthy people without hypertension or diabetes, renal plasma flow and GFR may decrease by 40% to 50% by the age of 80 years.
- Adaptive changes help maintain:
- Relatively normal electrolyte concentrations
- Normal body fluid volume
- These compensatory mechanisms continue until functional nephron number decreases by about 75% or more.
Effect of Hypertension and Diabetes
- Hypertension and diabetes mellitus greatly increase the frequency and severity of:
- Nephrosclerosis
- Glomerulosclerosis
- Benign nephrosclerosis combined with severe hypertension may progress rapidly to malignant nephrosclerosis.
- Malignant nephrosclerosis is characterized by:
- Large amounts of fibrinoid deposits in the arterioles
- Progressive thickening of blood vessel walls
- Severe ischemia of the affected nephrons
KEY CONCEPT
- Renal vascular injury causes renal ischemia, leading to loss of kidney tissue and nephrons.
- The three major vascular causes are atherosclerosis, fibromuscular hyperplasia, and nephrosclerosis.
- Benign nephrosclerosis commonly affects small renal arteries and afferent arterioles.
- Progressive vascular narrowing decreases blood flow and destroys nephrons.
- Glomerulosclerosis refers to sclerosis of the glomeruli.
- Functional nephrons decrease by about 10% every 10 years after age 40.
- By 80 years of age, renal plasma flow and GFR may decrease by 40–50%, even in healthy individuals.
- Hypertension and diabetes mellitus greatly accelerate nephrosclerosis and glomerulosclerosis.
- Severe hypertension can convert benign nephrosclerosis into malignant nephrosclerosis.
- Figure Mentioned: Figure 32.2, Figure 32.3
- Table Mentioned: Table 32.5
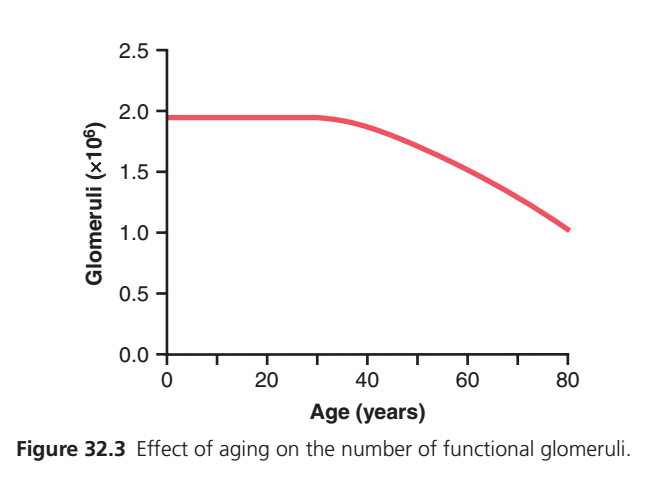
This graph is one of the simplest but most important graphs in renal physiology. It shows how the number of functional glomeruli changes with age.
Main Concept:
As we grow older, the number of working glomeruli gradually decreases. This is a normal part of aging, even in healthy people.
Let’s explain every axis, every line, every point, and every change in the easiest conceptual way.
First, What is a Glomerulus?
A glomerulus is a tiny ball of blood capillaries inside each nephron.
Its main function is to filter blood.
Think of it as a small water filter.
Blood enters
↓
Glomerulus
(Filters blood)
↓
Filtrate is formed
↓
Urine is eventually producedSince each nephron has one glomerulus, the number of glomeruli is almost equal to the number of functioning nephrons.
What Does This Graph Show?
This graph answers one question:
How many functional glomeruli remain as a person gets older?
X-Axis (Horizontal Axis)
Age (Years)
The horizontal axis shows the person’s age.
0 years = Birth
20 years = Young adult
40 years = Middle age
60 years = Older adult
80 years = ElderlyAs you move from left to right, age increases.
Y-Axis (Vertical Axis)
It is labeled:
Glomeruli (×10⁶)
This means the number of functioning glomeruli in both kidneys, expressed in millions.
Examples:
2.0 ×10⁶
=
2,000,000 glomeruli1.5 ×10⁶
=
1,500,000 glomeruli1.0 ×10⁶
=
1,000,000 glomeruliSo the graph measures how many working filters are present.
The Red Line
The red line represents the number of functional glomeruli at different ages.
Let’s follow it from left to right.
Birth to About 30 Years
Notice that the red line is almost perfectly horizontal.
────────────What does a horizontal line mean?
It means no significant change.
The number of functioning glomeruli remains almost constant.
Approximately:
2 million glomeruliDuring this period:
- Kidneys are healthy.
- Nephron loss is minimal.
- Filtration remains efficient.
Why Doesn’t the Number Increase?
Many people think kidneys continue making new nephrons throughout life.
They do not.
Humans are born with a fixed number of nephrons.
After birth:
- New nephrons are not formed.
- The body only uses the nephrons it already has.
So the graph stays flat because there is little loss, not because new glomeruli are being added.
Around 30–40 Years
Notice the red line begins to bend downward.
──────╲This is where normal aging starts to affect the kidneys.
Tiny age-related changes begin, including:
- Loss of some nephrons.
- Mild scarring of some glomeruli.
- Reduced blood flow to the kidneys.
At this stage:
Kidney function is still usually normal because the remaining nephrons compensate.
From 40 to 80 Years
Now the red line slopes downward more noticeably.
╲
╲
╲
╲This means the number of functioning glomeruli gradually decreases with age.
This is not a sudden drop.
It is a slow, continuous decline over many years.
Why Does This Happen?
Several normal aging processes contribute:
1. Glomerular sclerosis
Some glomeruli become scarred.
Scarred glomeruli can no longer filter blood.
↓
They become non-functional.
2. Nephron loss
Since each nephron contains one glomerulus:
Nephron dies
↓
Glomerulus is lost3. Reduced renal blood flow
As people age:
- Renal arteries become stiffer.
- Blood supply decreases.
- Some nephrons receive less oxygen.
Over time, some nephrons stop functioning.
At About 80 Years
According to the graph:
Working glomeruli decrease from about:
2 million
↓
1 millionSo approximately half of the functional glomeruli may be lost by around 80 years of age.
This does not mean every 80-year-old has kidney disease.
It means aging itself normally reduces the number of functioning glomeruli.
Why Don’t Healthy Older Adults Immediately Develop Kidney Failure?
This is a very common question.
The answer is compensation.
The remaining nephrons work harder.
They:
- Become larger (hypertrophy).
- Filter more blood (hyperfiltration).
This compensation helps maintain kidney function despite fewer nephrons.
However, it also means older adults have less kidney reserve.
If another problem develops (such as dehydration, diabetes, severe infection, or certain medications), kidney function can decline more quickly than in younger people.
Relationship to GFR (Glomerular Filtration Rate)
As the number of functioning glomeruli decreases:
Functional glomeruli ↓
↓
Total GFR gradually ↓In healthy aging, the decline in GFR is usually slow and gradual because the remaining nephrons compensate.
Real-Life Analogy
Imagine a factory with 2 million workers.
For the first 30 years:
2 million workers
↓
All are workingAs the factory gets older:
Some workers retire.
2 million
↓
1.8 million
↓
1.6 million
↓
1.4 million
↓
1 millionThe remaining workers take on extra work, so the factory still operates, but it has less reserve capacity.
The kidney behaves in a similar way.
What Does the Shape of the Curve Tell Us?
Flat portion (Birth to ~30 years)
──────────Means:
- Stable number of glomeruli.
- Healthy kidney function.
- Minimal nephron loss.
Downward curve (~30–80 years)
╲
╲
╲Means:
- Progressive loss of functional glomeruli.
- Normal aging process.
- Gradual reduction in nephron number.
Clinical Importance
This graph explains why:
- Kidney function normally declines with age.
- Older adults are more susceptible to acute kidney injury (AKI).
- Drug doses often need adjustment in elderly patients because many medications are eliminated by the kidneys.
- Elderly individuals have less functional renal reserve than younger adults.
One-Line Explanation of Every Part of the Graph
| Graph Part | Meaning |
|---|---|
| X-axis (Age) | Shows increasing age from birth to 80 years. |
| Y-axis (Glomeruli ×10⁶) | Shows the number of functioning glomeruli (in millions). |
| Flat red line (0–30 years) | Functional glomeruli remain almost constant; kidneys are fully developed and nephron loss is minimal. |
| Beginning of downward slope (~30–40 years) | Normal age-related nephron loss starts. |
| Gradual downward slope (40–80 years) | Functional glomeruli progressively decrease due to aging, glomerular sclerosis, and nephron loss. |
| Final point (~80 years) | Approximately half of the original functional glomeruli remain, but the remaining nephrons compensate to maintain kidney function. |
KEY CONCEPT (Exam Point)
- Humans are born with a fixed number of nephrons and glomeruli; new nephrons are not formed after birth.
- The number of functional glomeruli remains nearly constant until about 30 years of age.
- After about 30–40 years, there is a gradual age-related loss of functional glomeruli due to nephron loss, glomerular sclerosis, and reduced renal blood flow.
- By approximately 80 years of age, the number of functioning glomeruli may decrease from about 2 million to around 1 million.
- The remaining nephrons compensate by hypertrophy and hyperfiltration, allowing many healthy older adults to maintain adequate kidney function despite reduced renal reserve.
GLOMERULAR INJURY AS A CAUSE OF CKD—GLOMERULONEPHRITIS
- Chronic glomerulonephritis can be caused by several diseases that produce inflammation and damage of the glomerular capillary loops.
- Unlike acute glomerulonephritis, chronic glomerulonephritis is a slowly progressive disease.
- It often leads to irreversible renal failure.
- Chronic glomerulonephritis may be:
- A primary kidney disease that follows acute glomerulonephritis.
- A disease secondary to a systemic disorder, such as systemic lupus erythematosus (SLE).
- Systemic lupus erythematosus (SLE) is an autoimmune disease.
- In SLE, the immune system attacks the body’s own tissues.
- This causes inflammation and damage to several organs, including the kidneys.
- In most cases, chronic glomerulonephritis begins with accumulation of precipitated antigen-antibody complexes in the glomerular membrane.
- Unlike acute glomerulonephritis, streptococcal infections are responsible for only a small percentage of chronic glomerulonephritis cases.
- Accumulation of antigen-antibody complexes causes:
- Inflammation
- Progressive thickening of the glomerular membranes
- Gradual invasion of the glomeruli by fibrous tissue
- In the later stages of the disease, the glomerular capillary filtration coefficient decreases markedly.
- This occurs because:
- The number of filtering capillaries decreases.
- The glomerular membranes become thickened.
- In the final stage of the disease:
- Many glomeruli are replaced by fibrous tissue.
- These glomeruli can no longer filter fluid.
RENAL INTERSTITIUM INJURY AS A CAUSE OF CKD—INTERSTITIAL NEPHRITIS
- Disease affecting the renal interstitium is called interstitial nephritis.
- It may be:
- Primary
- Secondary
- Interstitial nephritis may result from:
- Vascular damage
- Glomerular damage
- Tubular damage
- These conditions destroy individual nephrons.
- It may also result from primary injury to the renal interstitium caused by:
- Poisons
- Drugs
- Bacterial infections
Pyelonephritis
- Renal interstitial injury caused by bacterial infection is called pyelonephritis.
- Pyelonephritis can be caused by different types of bacteria.
- The most common bacterium is Escherichia coli (E. coli).
- E. coli usually originates from fecal contamination of the urinary tract.
- Bacteria reach the kidneys by:
- The bloodstream
- More commonly, by ascending from the lower urinary tract through the ureters to the kidneys
Conditions That Promote Bladder Infection
- The normal bladder usually flushes bacteria effectively.
- Two conditions interfere with this normal flushing:
- Incomplete emptying of the bladder, leaving residual urine.
- Obstruction of urine outflow.
- When bacteria are not flushed out:
- They multiply in the bladder.
- The bladder becomes inflamed.
- Inflammation of the bladder is called cystitis.
- Cystitis may:
- Remain limited to the bladder.
- Or spread upward to the kidneys.
Vesicoureteral Reflux
- In some people, bacteria reach the renal pelvis because of vesicoureteral reflux.
- Vesicoureteral reflux is a condition in which urine flows backward into one or both ureters during micturition.
- This occurs because the bladder wall fails to close the ureter during micturition.
- As a result:
- Urine moves upward toward the kidney.
- Bacteria are carried with the urine.
- Bacteria reach the renal pelvis and renal medulla.
- This initiates infection and inflammation associated with pyelonephritis.
Effects of Pyelonephritis
- Pyelonephritis begins in the renal medulla.
- Therefore, it initially affects the renal medulla more than the renal cortex.
- One major function of the renal medulla is to provide the countercurrent mechanism for concentrating urine.
- Patients with pyelonephritis often have a markedly reduced ability to concentrate urine.
- Long-standing pyelonephritis allows bacteria to spread throughout the kidney.
- Chronic infection causes progressive damage to:
- Renal medullary interstitium
- Renal tubules
- Glomeruli
- Other kidney structures
- As damage progresses:
- Large amounts of functional kidney tissue are lost.
- Chronic Kidney Disease (CKD) may develop.
Figure 32.3
- Figure 32.3 shows the effect of aging on the number of functional glomeruli.
- The number of functional glomeruli decreases progressively with increasing age.
KEY CONCEPT
- Chronic glomerulonephritis is a slowly progressive inflammatory disease that often causes irreversible renal failure.
- It commonly begins with deposition of antigen-antibody complexes in the glomerular membrane.
- Progressive inflammation causes membrane thickening, fibrosis, and loss of filtration capacity.
- Interstitial nephritis is injury of the renal interstitium caused by vascular, glomerular, tubular disease, or by poisons, drugs, and bacterial infections.
- Pyelonephritis is a bacterial infection of the renal interstitium, most commonly caused by Escherichia coli.
- Cystitis, urinary obstruction, and vesicoureteral reflux increase the risk of pyelonephritis.
- Pyelonephritis first affects the renal medulla, reducing the ability to concentrate urine.
- Long-standing pyelonephritis causes progressive destruction of kidney tissue and can lead to CKD.
- Figure Mentioned: Figure 32.3