Superfast simplified image base self Learning
- Iron is essential for the formation of:
- Hemoglobin
- Myoglobin
- Cytochromes
- Cytochrome oxidase
- Peroxidase
- Catalase
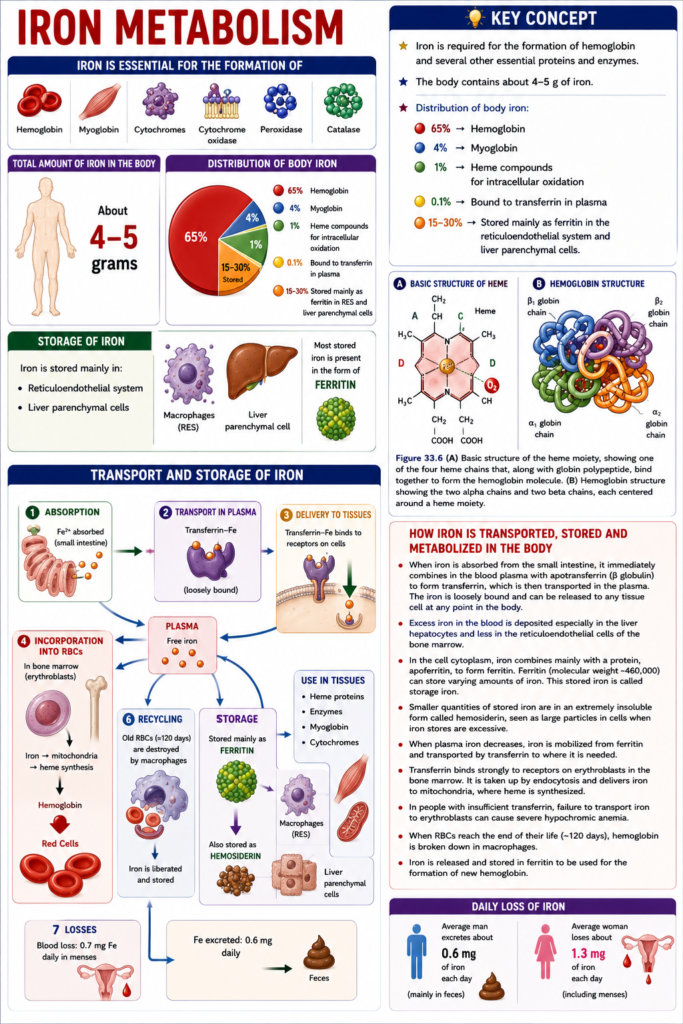
- The total amount of iron in the human body is about 4–5 grams.
- About 65% of the body’s iron is present in the form of hemoglobin.
- About 4% of the body’s iron is present in the form of myoglobin.
- About 1% of the body’s iron is present in the form of various heme compounds that promote intracellular oxidation.
- About 0.1% of the body’s iron is combined with the protein transferrin in the blood plasma.
- About 15–30% of the body’s iron is stored for future use.
- Iron is stored mainly in:
- The reticuloendothelial system
- Liver parenchymal cells
- Most stored iron is present in the form of ferritin.
KEY CONCEPT
- Iron is required for the formation of hemoglobin and several other essential proteins and enzymes.
- The body contains about 4–5 g of iron.
- Distribution of body iron:
- 65% → Hemoglobin
- 4% → Myoglobin
- 1% → Heme compounds for intracellular oxidation
- 0.1% → Bound to transferrin in plasma
- 15–30% → Stored mainly as ferritin in the reticuloendothelial system and liver parenchymal cells.
Transport and Storage of Iron
- Figure 33.7 shows the transport, storage, and metabolism of iron in the body.
- When iron is absorbed from the small intestine, it immediately combines in the blood plasma with a beta globulin called apotransferrin.
- This combination forms transferrin.
- Transferrin transports iron in the plasma.
- Iron is loosely bound to transferrin.
- Because the bond is loose, iron can be released to any tissue cell in the body whenever needed.
- Excess iron in the blood is stored mainly in:
- Liver hepatocytes
- To a lesser extent, the reticuloendothelial cells of the bone marrow
- Inside the cell cytoplasm, iron combines mainly with the protein apoferritin.
- This forms ferritin.
- Apoferritin has a molecular weight of about 460,000.
- Different amounts of iron can combine with apoferritin.
- Therefore, ferritin may contain either a small or a large amount of iron.
- Iron stored as ferritin is called storage iron.
- A smaller amount of storage iron exists as hemosiderin.
- Hemosiderin is an extremely insoluble form of stored iron.
- Hemosiderin is formed especially when the total body iron exceeds the storage capacity of apoferritin.
- Hemosiderin accumulates inside cells as large clusters.
- These large clusters can be seen with a light microscope.
- Ferritin particles are very small and widely dispersed.
- Therefore, ferritin can usually be seen only with an electron microscope.
- When the plasma iron level decreases, iron is easily released from the ferritin storage pool.
- The released iron again binds to transferrin in the plasma.
- Transferrin carries iron to the tissues where it is needed.
- Transferrin has a unique ability to bind strongly to receptors on the cell membranes of erythroblasts in the bone marrow.
- The transferrin–iron complex enters erythroblasts by endocytosis.
- Inside the erythroblasts, transferrin delivers iron directly to the mitochondria.
- Heme is synthesized in the mitochondria.
- If there is not enough transferrin in the blood, iron cannot be transported efficiently to erythroblasts.
- This failure can cause severe hypochromic anemia.
- In hypochromic anemia, RBCs contain much less hemoglobin than normal.
- RBCs normally survive for about 120 days.
- After their lifespan ends, RBCs are destroyed.
- Hemoglobin released from destroyed RBCs is ingested by monocyte-macrophage cells.
- Inside these cells, iron is released from hemoglobin.
- The released iron is stored mainly as ferritin.
- This stored iron is reused for the formation of new hemoglobin.
- Daily Loss of Iron
- An average man loses about 0.6 mg of iron per day.
- Most of this iron is excreted in the feces.
- Additional iron is lost whenever bleeding occurs.
- In women, menstrual blood loss increases the average daily iron loss.
- The average long-term iron loss in women is about 1.3 mg/day.
KEY CONCEPT
- Figure 33.7 illustrates iron transport, storage, and metabolism.
- Iron absorbed from the small intestine binds to apotransferrin to form transferrin.
- Transferrin transports iron throughout the body.
- Excess iron is stored mainly in the liver and bone marrow reticuloendothelial cells.
- Iron combines with apoferritin to form ferritin (storage iron).
- Excess storage iron forms hemosiderin.
- When plasma iron falls, ferritin releases iron, which is transported again by transferrin.
- Transferrin delivers iron to erythroblasts by endocytosis, where heme is synthesized in the mitochondria.
- Lack of transferrin can cause severe hypochromic anemia.
- Iron from old RBCs (lifespan 120 days) is recycled and stored mainly as ferritin.
- Daily iron loss:
- Men: 0.6 mg/day
- Women: 1.3 mg/day (due to menstrual blood loss)
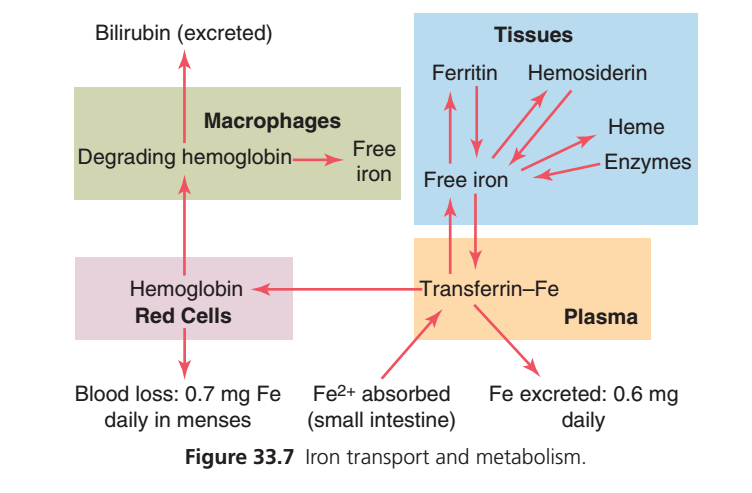
This figure explains Iron Transport, Storage, Recycling, and Metabolism in the human body. It is one of the most important MBBS physiology diagrams because it integrates RBC physiology, iron metabolism, macrophages, liver function, and intestinal absorption.
Instead of memorizing the arrows, understand it as one continuous journey of an iron atom.
BIG PICTURE (One-Minute Concept)
Imagine iron (Fe) is a valuable metal.
The body does not like to waste iron.
Instead, it recycles the same iron again and again.
Think of it like this:
Iron is borrowed to make RBCs → RBCs become old → Iron is recovered → Stored or transported → Used again to make new RBCs.
This recycling continues throughout life.
The Iron Cycle
Food
↓
Small intestine
↓
Transferrin (blood transport)
↓
Bone marrow
↓
Hemoglobin inside RBCs
↓
Old RBC destroyed
↓
Macrophages
↓
Iron recovered
↓
Stored or transported
↓
Bone marrow againThis is exactly what Figure 33.7 shows.
STEP 1: Iron Absorption from the Small Intestine
Look at the bottom center.
Fe²⁺ absorbed (small intestine)
↓
The dietary iron absorbed from the intestine enters the bloodstream.
Important point
Iron is absorbed mainly in the:
- Duodenum
- Upper jejunum
Iron enters blood as ferrous iron (Fe²⁺).
Why Fe²⁺?
Iron exists in two common forms:
- Fe²⁺ (Ferrous)
- Fe³⁺ (Ferric)
The intestine absorbs Fe²⁺ much more efficiently.
STEP 2: Iron Enters Plasma
After absorption,
Iron enters the plasma.
But there is a problem.
Problem
Free iron is dangerous.
It produces harmful free radicals.
Therefore,
The body never allows iron to circulate freely.
STEP 3: Iron Binds to Transferrin
Look at the orange box.
Transferrin–Fe
This means:
Iron combines with Transferrin.
What is Transferrin?
Transferrin is the iron transport protein in plasma.
Think of transferrin as a delivery truck.
It safely carries iron through the blood.
Easy Story
Iron = Passenger
Transferrin = Bus
Blood = Highway
The passenger (iron) cannot travel alone.
It must ride inside the transferrin bus.
STEP 4: Where Does Transferrin Deliver Iron?
The arrows show three major destinations.
Destination 1
Bone Marrow
Transferrin carries iron to the bone marrow.
Why?
Because bone marrow needs iron to produce hemoglobin.
Hemoglobin Formation
Iron
↓
Heme
↓
Hemoglobin
↓
Red Blood Cell
Without iron,
No hemoglobin.
Without hemoglobin,
No RBC.
Without RBC,
No oxygen transport.
Destination 2
Tissues
Some iron leaves transferrin and enters tissues.
Now look inside the blue box.
There are three important fates.
Fate A
Ferritin
Free iron
↓
Ferritin
What is Ferritin?
Ferritin is the main iron storage protein.
Think of ferritin as a bank locker.
When iron is not needed,
It is stored safely inside ferritin.
Clinical Importance
Serum ferritin reflects body iron stores.
Low ferritin
↓
Iron deficiency.
Fate B
Hemosiderin
If iron storage becomes excessive,
Ferritin becomes overloaded.
Extra iron is stored as:
↓
Hemosiderin
Easy Story
Ferritin = Small cupboard
Hemosiderin = Large warehouse
When the cupboard becomes full,
Iron moves into the warehouse.
Clinical Importance
Seen in:
- Repeated blood transfusions
- Hemochromatosis
- Iron overload disorders
Fate C
Heme Enzymes
Some tissue iron is used to make:
- Cytochromes
- Catalase
- Peroxidase
- Other heme-containing enzymes
These enzymes are essential for:
- Cellular respiration
- Detoxification
- Oxidative metabolism
So not all iron goes into hemoglobin.
Some iron helps cells produce energy.
STEP 5: Formation of RBCs
Look at the lower left.
Transferrin
↓
Hemoglobin
↓
Red Blood Cells
Inside developing RBCs,
Iron becomes part of hemoglobin.
Each hemoglobin molecule contains four heme groups, and each heme contains one Fe²⁺ ion that binds oxygen.
STEP 6: RBC Circulate
The RBC carries oxygen throughout the body.
Average life span:
120 days
STEP 7: Old RBCs are Destroyed
After about 120 days,
Old RBCs are removed by:
Macrophages
Especially in:
- Spleen
- Liver
- Bone marrow
Macrophages are the recycling centers of the body.
STEP 8: Hemoglobin is Broken Down
Inside macrophages,
Hemoglobin is degraded.
Look at the green box.
Hemoglobin
↓
Macrophages
↓
Hemoglobin degradation
Now two important products appear.
Product 1
Free Iron
Iron is removed from hemoglobin.
This iron is not wasted.
It immediately re-enters the circulation by binding to transferrin, allowing it to be reused for new hemoglobin synthesis.
This is the body’s iron recycling system.
Product 2
Bilirubin
The heme ring (after iron is removed) is converted into bilirubin.
Bilirubin
↓
Liver
↓
Bile
↓
Intestine
↓
Excreted
So:
Iron is recycled.
The porphyrin ring becomes bilirubin and is eliminated.
STEP 9: Small Daily Iron Loss
Look at the bottom right.
Iron excreted ≈ 0.6 mg/day
Every day,
A small amount of iron is lost through:
- Skin cells
- Sweat
- Intestinal epithelial cells
- Urine (very little)
The body replaces this by absorbing dietary iron.
Menstrual Blood Loss
Look at the lower left.
Women lose about 0.7 mg of additional iron per day on average because of menstruation (this is an average over the menstrual cycle).
Therefore,
Women generally require more dietary iron than men.
Entire Diagram in One Flow
Dietary Iron (Fe²⁺)
│
▼
Small Intestine
│
▼
Plasma
│
▼
Transferrin (Iron Transport Protein)
│
┌──────┼──────────┐
│ │ │
▼ ▼ ▼
Bone Ferritin Heme Enzymes
Marrow Hemosiderin
│
▼
Hemoglobin
│
▼
Red Blood Cells
│
▼
Old RBC (120 days)
│
▼
Macrophages
│
├───────────────┐
▼ ▼
Free Iron Bilirubin
│ │
▼ ▼
Transferrin Excreted in bile
│
▼
Bone Marrow AgainHigh-Yield MBBS Points
| Component | Function | Clinical Importance |
|---|---|---|
| Fe²⁺ | Absorbable form of iron | Absorbed mainly in the duodenum |
| Transferrin | Transports iron in plasma | Increased in iron deficiency |
| Ferritin | Main iron storage protein | Best indicator of body iron stores |
| Hemosiderin | Iron storage during excess | Seen in iron overload |
| Bone marrow | Uses iron to make hemoglobin | Site of erythropoiesis |
| Macrophages | Recycle iron from old RBCs | Prevent iron wastage |
| Bilirubin | Product of heme breakdown | Excreted via bile |
| Menstruation | Additional iron loss | Higher iron requirement in women |
KEY CONCEPT
- Iron is continuously recycled rather than wasted.
- Dietary Fe²⁺ is absorbed in the small intestine and transported in the blood by transferrin.
- Transferrin delivers iron to the bone marrow for hemoglobin synthesis, while excess iron is stored as ferritin or hemosiderin in tissues.
- After approximately 120 days, old RBCs are broken down by macrophages. The iron is recovered, binds transferrin again, and is reused, whereas the heme ring is converted into bilirubin and excreted in bile.
- Only a small amount of iron is lost each day (~0.6 mg in adults, with additional average loss in menstruating women), making efficient iron recycling essential for maintaining normal red blood cell production.
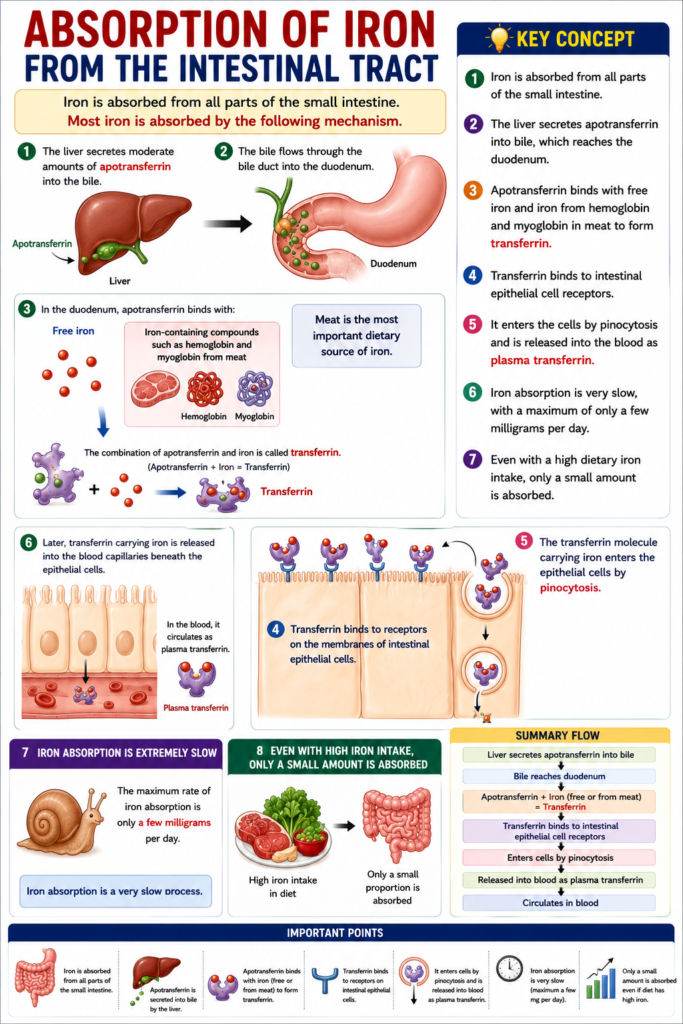
Absorption of Iron From the Intestinal Tract
- Iron is absorbed from all parts of the small intestine.
- Most iron is absorbed by the following mechanism.
- The liver secretes moderate amounts of apotransferrin into the bile.
- The bile flows through the bile duct into the duodenum.
- In the duodenum, apotransferrin binds with:
- Free iron
- Iron-containing compounds such as hemoglobin and myoglobin from meat
- Meat is the most important dietary source of iron.
- The combination of apotransferrin and iron is called transferrin.
- Transferrin binds to receptors on the membranes of intestinal epithelial cells.
- The transferrin molecule carrying iron enters the epithelial cells by pinocytosis.
- Later, transferrin carrying iron is released into the blood capillaries beneath the epithelial cells.
- In the blood, it circulates as plasma transferrin.
- Iron absorption from the intestine is extremely slow.
- The maximum rate of iron absorption is only a few milligrams per day.
- Therefore, even if the diet contains a very large amount of iron, only a small proportion can be absorbed.
KEY CONCEPT
- Iron is absorbed from all parts of the small intestine.
- The liver secretes apotransferrin into bile, which reaches the duodenum.
- Apotransferrin binds with free iron and iron from hemoglobin and myoglobin in meat to form transferrin.
- Transferrin binds to intestinal epithelial cell receptors.
- It enters the cells by pinocytosis and is released into the blood as plasma transferrin.
- Iron absorption is very slow, with a maximum of only a few milligrams per day.
- Even with a high dietary iron intake, only a small amount is absorbed.
Regulation of Total Body Iron By Controlling Absorption Rate
- Total body iron is regulated mainly by controlling the rate of iron absorption from the intestinal tract.
- When the body becomes saturated with iron:
- Almost all apoferritin in the iron storage sites is already filled with iron.
- The rate of additional iron absorption from the intestine decreases markedly.
- When the body’s iron stores become depleted:
- The rate of iron absorption increases.
- Iron absorption can become five or more times greater than normal.
- Thus, the body regulates total iron mainly by changing the intestinal absorption rate.
KEY CONCEPT
- Total body iron is controlled primarily by regulating intestinal iron absorption.
- High iron stores: Apoferritin is saturated → Iron absorption decreases markedly.
- Low iron stores: Iron absorption increases to five or more times the normal rate.
- The main mechanism for maintaining normal body iron is adjusting the rate of iron absorption.
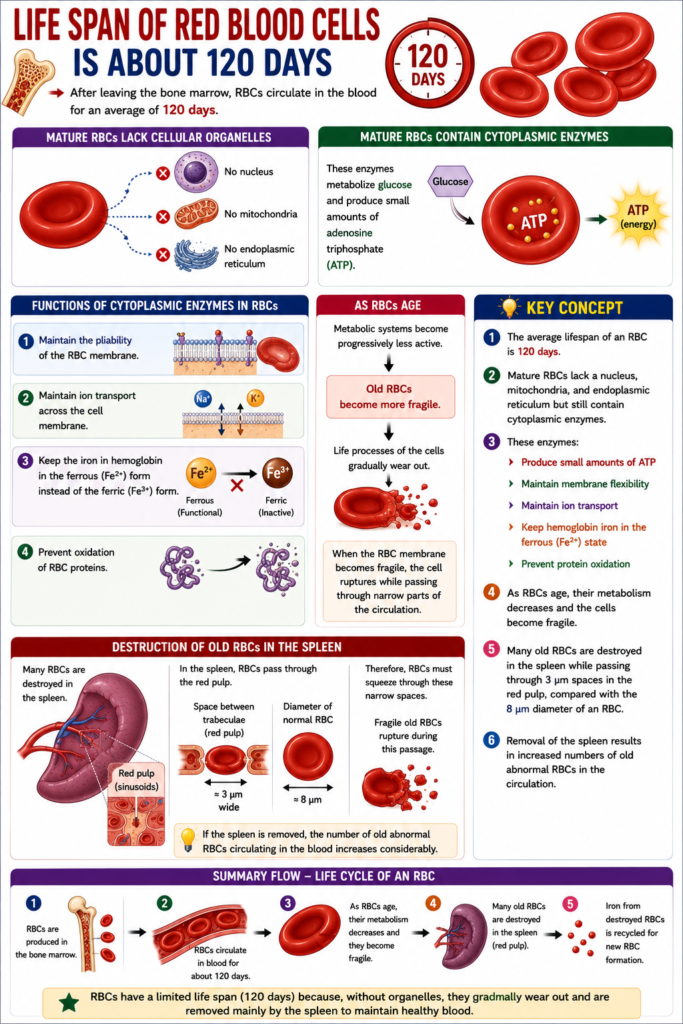
LIFE SPAN OF RED BLOOD CELLS IS ABOUT 120 DAYS
- After leaving the bone marrow, RBCs circulate in the blood for an average of 120 days.
- Mature RBCs do not contain:
- A nucleus
- Mitochondria
- Endoplasmic reticulum
- However, mature RBCs contain cytoplasmic enzymes.
- These enzymes metabolize glucose.
- They also produce small amounts of adenosine triphosphate (ATP).
- The cytoplasmic enzymes perform the following functions:
- Maintain the pliability of the RBC membrane.
- Maintain ion transport across the cell membrane.
- Keep the iron in hemoglobin in the ferrous (Fe²⁺) form instead of the ferric (Fe³⁺) form.
- Prevent oxidation of RBC proteins.
- As RBCs become older, their metabolic systems become progressively less active.
- As a result, old RBCs become more fragile.
- This increased fragility occurs because the life processes of the cells gradually wear out.
- When the RBC membrane becomes fragile, the cell ruptures while passing through narrow parts of the circulation.
- Many RBCs are destroyed in the spleen.
- In the spleen, RBCs pass through the red pulp.
- The spaces between the structural trabeculae of the red pulp are only about 3 micrometers wide.
- The diameter of a normal RBC is about 8 micrometers.
- Therefore, RBCs must squeeze through these narrow spaces.
- Fragile old RBCs rupture during this passage.
- If the spleen is removed, the number of old abnormal RBCs circulating in the blood increases considerably.
KEY CONCEPT
- The average lifespan of an RBC is 120 days.
- Mature RBCs lack a nucleus, mitochondria, and endoplasmic reticulum but still contain cytoplasmic enzymes.
- These enzymes:
- Produce small amounts of ATP
- Maintain membrane flexibility
- Maintain ion transport
- Keep hemoglobin iron in the ferrous (Fe²⁺) state
- Prevent protein oxidation
- As RBCs age, their metabolism decreases and the cells become fragile.
- Many old RBCs are destroyed in the spleen while passing through 3 μm spaces in the red pulp, compared with the 8 μm diameter of an RBC.
- Removal of the spleen results in increased numbers of old abnormal RBCs in the circulation.
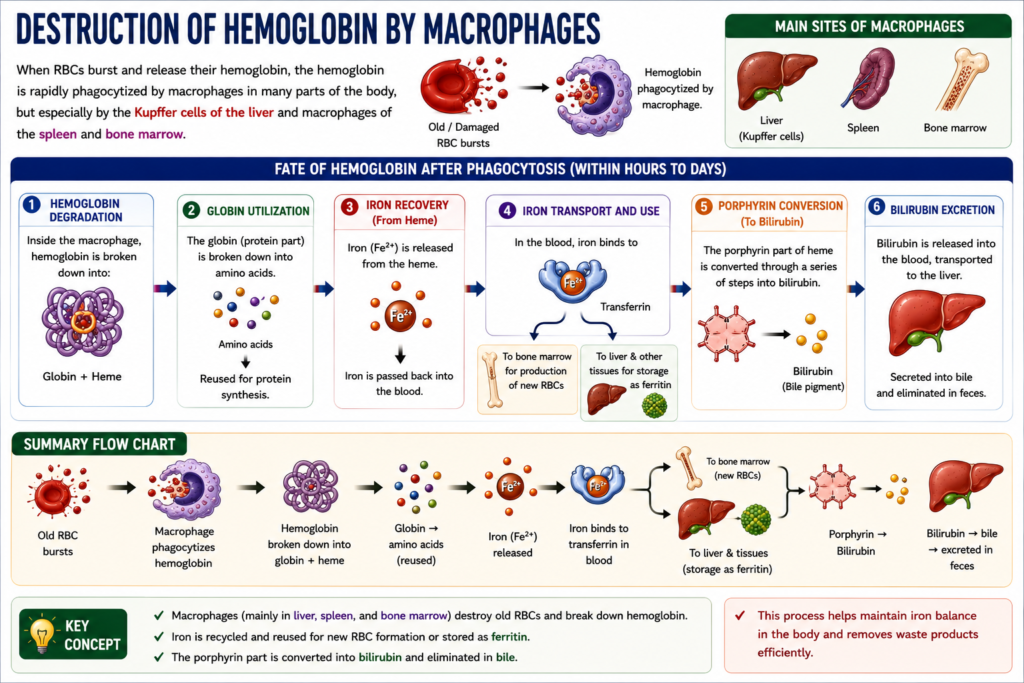
Destruction of Hemoglobin By Macrophages
- When RBCs rupture, they release hemoglobin.
- The released hemoglobin is rapidly phagocytized by macrophages.
- Hemoglobin is mainly phagocytized by:
- Kupffer cells of the liver
- Macrophages of the spleen
- Macrophages of the bone marrow
- During the next few hours to days, macrophages remove iron from the hemoglobin.
- The released iron is returned to the blood.
- In the blood, iron is transported by transferrin.
- Transferrin carries iron to:
- The bone marrow for the production of new RBCs.
- The liver and other tissues for storage as ferritin.
- The porphyrin portion of the hemoglobin molecule is converted by macrophages through a series of stages.
- This conversion forms the bile pigment bilirubin.
- Bilirubin is released into the blood.
- Later, bilirubin is removed from the body by secretion from the liver into the bile.
KEY CONCEPT
- Ruptured RBCs release hemoglobin.
- Hemoglobin is phagocytized mainly by Kupffer cells of the liver and macrophages of the spleen and bone marrow.
- Macrophages separate iron from hemoglobin.
- Iron returns to the blood, binds to transferrin, and is:
- Transported to the bone marrow for new RBC formation.
- Stored in the liver and other tissues as ferritin.
- The porphyrin part of hemoglobin is converted into bilirubin.
- Bilirubin is released into the blood and later excreted by the liver through bile.