

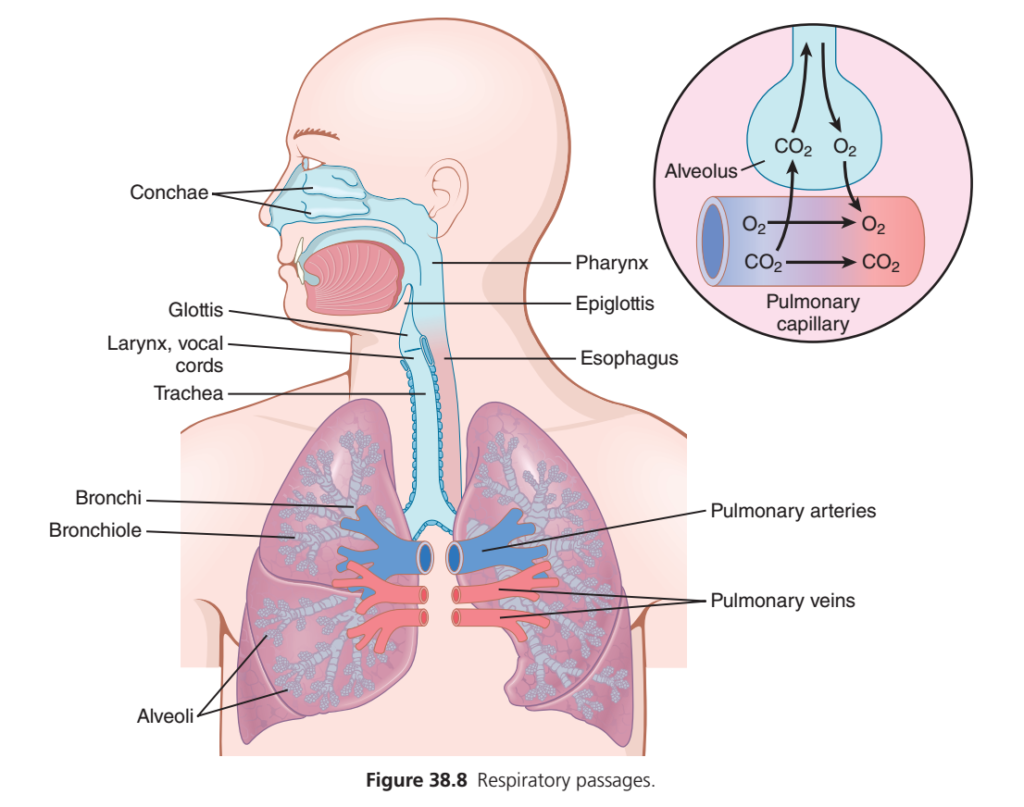
Figure: Fig. 38.8
- Fig. 38.8 shows the respiratory passageways.
- Air travels to the lungs through:
- Trachea
- Bronchi
- Bronchioles
Main Function of the Respiratory Passageways
- One of the most important functions of the respiratory passageways is to keep the airways open.
- Open airways allow easy movement of air to and from the alveoli.
Trachea
- The trachea is kept open by multiple cartilage rings.
- These cartilage rings extend around about five-sixths of the trachea.
- The cartilage prevents the trachea from collapsing.
Bronchi
- The walls of the bronchi contain curved cartilage plates.
- These cartilage plates:
- Keep the bronchi reasonably rigid.
- Still allow movement when the lungs expand and contract.
- As the bronchi divide into smaller branches:
- The cartilage plates become progressively smaller and less extensive.
Bronchioles
- Bronchioles do not contain cartilage plates.
- Their diameter is usually less than 1.5 mm.
- Since they have no cartilage, they are not kept open by rigid walls.
How Bronchioles Stay Open
- Bronchioles remain open mainly because of transpulmonary pressure.
- This is the same pressure that keeps the alveoli expanded.
- When the alveoli enlarge, the bronchioles also enlarge.
- However, the bronchioles expand less than the alveoli.
Easy Concept
Think of the respiratory passageways as a tree:
Trachea
│
▼
Bronchi
│
▼
Bronchioles
│
▼
Alveoli- Trachea → Strong support (many cartilage rings)
- Bronchi → Moderate support (cartilage plates)
- Bronchioles → No cartilage; kept open by transpulmonary pressure
Key Concept
- Fig. 38.8 shows the trachea, bronchi, and bronchioles.
- Their main function is to keep the airways open for easy airflow to and from the alveoli.
- Trachea is supported by cartilage rings.
- Bronchi are supported by curved cartilage plates, which become smaller in successive branches.
- Bronchioles have no cartilage and are usually less than 1.5 mm in diameter.
- Bronchioles remain open because of transpulmonary pressure, the same pressure that expands the alveoli.
- As the alveoli expand, the bronchioles also expand, but to a lesser extent.
Muscular Wall of the Bronchi and Bronchioles
Figure: Fig. 38.8
- In the trachea and bronchi, the areas not covered by cartilage plates are mainly made of smooth muscle.
Smooth Muscle in the Bronchioles
- The walls of the bronchioles are made almost entirely of smooth muscle.
- The terminal bronchiole, called the respiratory bronchiole, is an exception.
- The respiratory bronchiole is mainly made of:
- Pulmonary epithelium
- Underlying fibrous tissue
- A few smooth muscle fibers
Narrowing of the Airways
- Many obstructive lung diseases occur because the smaller bronchi and larger bronchioles become narrow.
- This narrowing is often caused by excessive contraction of the smooth muscle.
Key Concept
- Fig. 38.8 shows the respiratory passageways.
- In the trachea and bronchi, areas without cartilage plates are mainly composed of smooth muscle.
- Bronchioles are made almost entirely of smooth muscle.
- The respiratory bronchiole is mainly composed of pulmonary epithelium, fibrous tissue, and a few smooth muscle fibers.
- Many obstructive lung diseases result from narrowing of the smaller bronchi and larger bronchioles due to excessive smooth muscle contraction.
Resistance to Airflow in the Bronchial Tree
- Under normal breathing conditions, air moves through the respiratory passageways very easily.
- A pressure difference of less than 1 cm H₂O between the alveoli and the atmosphere is enough for quiet breathing.
- The greatest resistance to airflow does not occur in the terminal bronchioles.
- Instead, it occurs in the larger bronchioles and bronchi near the trachea.
- This is because there are only a few larger bronchi, while there are about 65,000 terminal bronchioles.
- Therefore, each terminal bronchiole carries only a very small amount of air.
Airflow Resistance in Disease
- In some lung diseases, smaller bronchioles become the main site of airflow resistance.
- This happens because they are small in size and are easily blocked.
- The smaller bronchioles may become blocked due to:
- Contraction of smooth muscle in their walls
- Edema (swelling) of the walls
- Mucus collecting inside the bronchioles
Nervous and Local Control of the Bronchiolar Musculature—Sympathetic Dilation of the Bronchioles
- Direct sympathetic nerve control of the bronchioles is relatively weak.
- This is because only a few sympathetic nerve fibers reach the central parts of the lungs.
- However, the bronchial tree is strongly influenced by norepinephrine and epinephrine released into the blood from the adrenal gland medullae during sympathetic stimulation.
- Both hormones dilate the bronchial tree.
- Epinephrine produces greater bronchodilation because it stimulates beta-adrenergic receptors more strongly.
Parasympathetic Constriction of the Bronchioles
- A few parasympathetic nerve fibers from the vagus nerves enter the lung tissue.
- These nerves release acetylcholine.
- When activated, acetylcholine causes mild to moderate constriction of the bronchioles.
- In diseases such as asthma, where bronchioles are already narrowed, parasympathetic stimulation can make the narrowing worse.
- In this situation, drugs that block acetylcholine, such as atropine, may relax the respiratory passageways and reduce the obstruction.
Parasympathetic Reflexes
- Parasympathetic nerves can also be activated by reflexes that begin in the lungs.
- Most of these reflexes start when the epithelial lining of the respiratory passageways is irritated.
- Irritation may be caused by:
- Noxious gases
- Dust
- Cigarette smoke
- Bronchial infection
- A bronchiolar constrictor reflex may also occur when microemboli block small pulmonary arteries.
Local Secretory Factors May Cause Bronchiolar Constriction
- Several substances produced in the lungs can cause bronchiolar constriction.
- Two of the most important substances are:
- Histamine
- Slow reactive substance of anaphylaxis
- These substances are released from mast cells during allergic reactions.
- Allergic reactions are especially caused by pollen in the air.
- These substances play an important role in airway obstruction in allergic asthma.
- The slow reactive substance of anaphylaxis is especially important in allergic asthma.
Direct Local Effects of Irritants
- The same irritants that trigger parasympathetic constrictor reflexes can also directly affect the lung tissues.
- These irritants include:
- Smoke
- Dust
- Sulfur dioxide
- Acidic substances in smog
- These irritants can produce local, non-nervous reactions.
- These reactions cause obstructive constriction of the airways.
Key Concept
- Less than 1 cm H₂O pressure difference is enough for normal quiet breathing.
- The greatest normal airflow resistance occurs in the larger bronchi and bronchioles near the trachea, not in the terminal bronchioles.
- In disease, small bronchioles become the main site of airflow resistance because of:
- Smooth muscle contraction
- Edema
- Mucus accumulation
- Sympathetic stimulation causes bronchodilation mainly through epinephrine acting on beta-adrenergic receptors.
- Parasympathetic stimulation releases acetylcholine, causing bronchoconstriction.
- Atropine can reduce bronchoconstriction by blocking the action of acetylcholine.
- Histamine and the slow reactive substance of anaphylaxis cause bronchiolar constriction during allergic reactions.
- Smoke, dust, sulfur dioxide, acidic smog, bronchial infection, noxious gases, and microemboli can all contribute to bronchiolar constriction.
Mucus Lining the Respiratory Passageways and Cilia Action to Clear the Passageways
- All the respiratory passageways, from the nose to the terminal bronchioles, are covered by a layer of mucus.
- This mucus keeps the entire surface moist.
Mucus Secretion
- The mucus is secreted partly by mucous goblet cells present in the epithelial lining of the respiratory passageways.
- It is also secreted partly by small submucosal glands.
Functions of Mucus
- Mucus keeps the respiratory surfaces moist.
- Mucus traps small particles present in the inspired air.
- This prevents most particles from reaching the alveoli.
- The mucus and trapped particles are removed from the respiratory passageways.
Cilia Action to Clear the Passageways
- The entire respiratory passageway, from the nose to the terminal bronchioles, is lined with ciliated epithelium.
- Each epithelial cell has about 200 cilia.
- These cilia beat continuously.
- The cilia beat at a rate of 10–20 times per second.
- The power stroke of the cilia is always directed toward the pharynx.
- In the lungs, the cilia beat upward.
- In the nose, the cilia beat downward.
- The continuous beating of the cilia moves the mucus slowly toward the pharynx.
- The mucus moves at a speed of a few millimeters per minute.
- After reaching the pharynx, the mucus and trapped particles are:
- Swallowed, or
- Coughed out and expelled from the body.
Key Concept
- Mucus covers the respiratory passageways from the nose to the terminal bronchioles.
- It is secreted by goblet cells and submucosal glands.
- Mucus keeps the airways moist and traps inhaled particles.
- The respiratory epithelium contains about 200 cilia per epithelial cell.
- Cilia beat 10–20 times per second.
- The cilia always move mucus toward the pharynx.
- In the lungs, cilia beat upward; in the nose, they beat downward.
- The mucus carrying trapped particles is swallowed or coughed out, helping to keep the respiratory passageways clean.
Cough Reflex
- The bronchi and trachea are very sensitive to light touch.
- Even a small amount of foreign material or irritation can trigger the cough reflex.
- The larynx and the carina (where the trachea divides into the bronchi) are especially sensitive.
- The terminal bronchioles and even the alveoli are sensitive to corrosive chemical irritants, such as:
- Sulfur dioxide gas
- Chlorine gas
Nerve Pathway of the Cough Reflex
- Sensory (afferent) nerve impulses travel mainly through the vagus nerves.
- These impulses reach the medulla of the brain.
- The neuronal circuits in the medulla automatically trigger the cough reflex.
Sequence of Events During the Cough Reflex
Step 1: Deep Inspiration
- About 2.5 liters of air are rapidly inhaled.
Step 2: Air Is Trapped
- The epiglottis closes.
- The vocal cords close tightly.
- This traps the air inside the lungs.
Step 3: Pressure Builds Up
- The abdominal muscles contract forcefully.
- They push against the diaphragm.
- Other expiratory muscles, such as the internal intercostal muscles, also contract forcefully.
- As a result, lung pressure rises rapidly.
- Lung pressure may increase to 100 mm Hg or more.
Step 4: Forceful Expulsion of Air
- The vocal cords and epiglottis suddenly open widely.
- The high-pressure air explodes out of the lungs.
- The expelled air may reach a speed of 75–100 miles/hour.
Removal of Foreign Matter
- The strong compression of the lungs collapses the bronchi and trachea.
- The non-cartilaginous parts of the bronchi and trachea move inward.
- This forms narrow slits in the airways.
- The rapidly moving air passes through these slits.
- The forceful airflow carries foreign material out of the bronchi and trachea.
Key Concept
- The cough reflex protects the respiratory tract by removing foreign material and irritants.
- It is triggered by irritation of the bronchi, trachea, larynx, carina, terminal bronchioles, or alveoli.
- Afferent impulses travel through the vagus nerves to the medulla, where the reflex is initiated.
- The sequence of the cough reflex is:
- Rapid inspiration (about 2.5 L)
- Closure of the epiglottis and vocal cords
- Forceful contraction of expiratory muscles, raising lung pressure to about 100 mm Hg or more
- Sudden opening of the vocal cords and epiglottis, producing a high-speed burst of air (75–100 miles/hour)
- The high-speed airflow removes foreign particles from the bronchi and trachea.
Sneeze Reflex
- The sneeze reflex is very similar to the cough reflex.
- The difference is that the sneeze reflex protects the nasal passageways, while the cough reflex protects the lower respiratory passages.
- The sneeze reflex begins when there is irritation in the nasal passageways.
- Sensory (afferent) nerve impulses travel through the fifth cranial nerve to the medulla.
- The medulla triggers the sneeze reflex.
- A sequence of reactions similar to the cough reflex occurs.
- During the sneeze reflex, the uvula is depressed.
- This allows large amounts of air to pass rapidly through the nose.
- The forceful airflow helps remove foreign matter from the nasal passageways.
Normal Respiratory Functions of the Nose
Figure: Fig. 38.8
- As air passes through the nose, the nasal cavities perform three normal respiratory functions.
Warming the Air
- The inspired air is warmed by the large surface area of the conchae and nasal septum.
- These structures have a total surface area of about 160 cm².
Humidifying the Air
- The inspired air becomes almost completely humidified.
- This occurs before the air passes beyond the nose.
Filtering the Air
- The inspired air is partially filtered.
Air-Conditioning Function
- These three functions together are called the air-conditioning function of the upper respiratory passageways.
- Normally, before reaching the trachea:
- The inspired air is warmed to within 1°F of body temperature.
- The inspired air reaches within 2%–3% of full water vapor saturation.
- When a person breathes directly into the trachea through a tracheostomy, the lower lungs do not receive properly warmed and humidified air.
- This may cause:
- Drying of the lower lungs
- Lung crusting
- Infection
Filtration Function of the Nose
- The hairs at the entrance of the nostrils filter out large particles.
- A more important filtering mechanism is turbulent precipitation.
- As air passes through the nasal cavity, it strikes:
- Conchae (turbinates)
- Nasal septum
- Pharyngeal wall
- Each obstacle changes the direction of airflow.
- Air changes direction quickly.
- Suspended particles have greater mass and momentum than air.
- Therefore, the particles cannot change direction as quickly as the air.
- The particles strike the nasal surfaces.
- They become trapped in the mucus.
- The cilia move the trapped particles toward the pharynx, where they are swallowed.
Size of Particles Entrapped in the Respiratory Passages
- The nasal turbulence mechanism is very effective.
- Almost no particles larger than 6 micrometers enter the lungs through the nose.
- This size is smaller than a red blood cell.
Particles Between 1 and 5 Micrometers
- Many particles measuring 1–5 micrometers settle in the smaller bronchioles.
- This occurs because of gravitational precipitation.
- Coal miners commonly develop terminal bronchiolar disease due to deposited dust particles.
Particles Smaller Than 1 Micrometer
- Some particles smaller than 1 micrometer diffuse to the alveolar walls.
- These particles stick to the alveolar fluid.
Particles Smaller Than 0.5 Micrometer
- Many particles smaller than 0.5 micrometer remain suspended in the alveolar air.
- These particles are removed during expiration.
- Cigarette smoke particles are about 0.3 micrometer in diameter.
- Almost none of these particles are trapped before reaching the alveoli.
- About one-third of these particles deposit in the alveoli by diffusion.
- The remaining particles stay suspended and are exhaled.
Removal of Particles From the Alveoli
- Many particles trapped in the alveoli are removed by alveolar macrophages.
- Other particles are removed through the lung lymphatics.
- If too many particles accumulate, fibrous tissue grows in the alveolar septa.
- This may lead to permanent debility.
Key Concept
- The sneeze reflex protects the nasal passageways.
- It is triggered by nasal irritation, and afferent impulses travel through the fifth cranial nerve to the medulla.
- During a sneeze, the uvula is depressed, allowing rapid airflow through the nose to remove foreign material.
- The nose performs three main respiratory functions:
- Warms inspired air
- Humidifies inspired air
- Filters inspired air
- These functions are called the air-conditioning function of the upper respiratory passageways.
- The conchae, septum, and pharyngeal wall create turbulent airflow, which helps trap particles in mucus.
- Large particles (>6 µm) are filtered in the nose.
- Particles 1–5 µm settle in the bronchioles.
- Particles <1 µm may reach the alveoli.
- Cigarette smoke particles (~0.3 µm) often reach the alveoli, where about one-third deposit by diffusion.
- Alveolar macrophages and lung lymphatics remove deposited particles, but excessive accumulation may cause fibrous tissue formation and permanent debility.
Vocalization
- Speech involves the respiratory system.
- Speech also involves:
- Specific speech nervous control centers in the cerebral cortex
- Respiratory control centers of the brain
- The articulation and resonance structures of the mouth and nasal cavities
- Speech is produced by two mechanical functions:
- Phonation
- Articulation
Phonation
Figure: Fig. 38.9A and Fig. 38.9B
- Phonation is produced by the larynx.
- The larynx is specially adapted to act as a vibrator.
- The vibrating structures are the vocal folds (vocal cords).
- The vocal cords project from the lateral walls of the larynx toward the center of the glottis.
- Several laryngeal muscles stretch and position the vocal cords.
Vocal Cords During Breathing and Speech
- Fig. 38.9B shows the vocal cords viewed through a laryngoscope.
- During normal breathing, the vocal cords remain widely open.
- This allows easy passage of air.
- During phonation, the vocal cords move close together.
- Air passing between them causes the vocal cords to vibrate.
Pitch of the Voice
- The pitch of the voice depends mainly on:
- The degree of stretching of the vocal cords
- Pitch also depends on:
- How closely the vocal cords are brought together
- The mass of the edges of the vocal cords
Vocal Ligament
- Fig. 38.9A shows the vocal folds after the mucous epithelial lining has been removed.
- Inside each vocal cord is a strong elastic vocal ligament.
- The vocal ligament is attached:
- Anteriorly to the thyroid cartilage
- Posteriorly to the vocal processes of the arytenoid cartilages
- The thyroid cartilage forms the Adam’s apple on the front of the neck.
- The thyroid cartilage and arytenoid cartilages articulate with the cricoid cartilage.
Stretching and Loosening the Vocal Cords
- The vocal cords are stretched by:
- Forward rotation of the thyroid cartilage
- Posterior rotation of the arytenoid cartilages
- These movements are produced by muscles connecting the thyroid and arytenoid cartilages to the cricoid cartilage.
- The thyroarytenoid muscles, located beside the vocal ligaments:
- Pull the arytenoid cartilages toward the thyroid cartilage
- Loosen the vocal cords
- Small slips of the thyroarytenoid muscles can change:
- The shape of the vocal cord edges
- The mass of the vocal cord edges
- Sharp vocal cord edges produce high-pitched sounds.
- Blunt vocal cord edges produce low-pitched (bass) sounds.
Other Laryngeal Muscles
- Several small laryngeal muscles lie between the arytenoid cartilages and the cricoid cartilage.
- These muscles can:
- Rotate the arytenoid cartilages inward or outward
- Pull their bases together or apart
- These movements produce different positions of the vocal cords, as shown in Fig. 38.9B.
Articulation and Resonance
- The three major organs of articulation are:
- Lips
- Tongue
- Soft palate
Resonators
- The structures that act as resonators include:
- Mouth
- Nose
- Nasal sinuses
- Pharynx
- Chest cavity
- These structures modify the quality of the voice.
- The role of the nasal resonators is demonstrated during a severe cold, when blockage of the nasal passages changes the quality of the voice.
Key Concept
- Speech requires the respiratory system, cerebral cortex, respiratory control centers, and the articulation and resonance structures.
- Speech consists of two mechanical functions:
- Phonation (produced by the larynx)
- Articulation (produced by the mouth)
- Fig. 38.9A and Fig. 38.9B show the larynx and vocal cords.
- During breathing, the vocal cords remain open.
- During phonation, the vocal cords move together and vibrate as air passes between them.
- Voice pitch depends mainly on the stretch of the vocal cords, and also on their closeness and edge mass.
- The vocal ligament extends from the thyroid cartilage (Adam’s apple) to the arytenoid cartilages.
- Thyroarytenoid muscles loosen the vocal cords and modify their shape for high-pitched and low-pitched sounds.
- Articulation is performed by the lips, tongue, and soft palate.
- Resonance is produced by the mouth, nose, nasal sinuses, pharynx, and chest cavity.
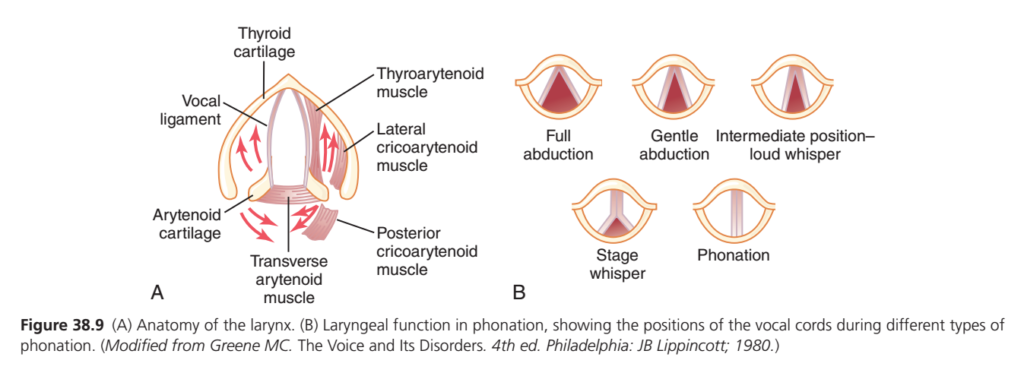
Figure 38.9 — Larynx (Voice Box) & Vocal Cord Positions (Guyton Physiology)
Easiest MBBS Conceptual Summary
This figure answers two simple questions:
- Which muscles move the vocal cords? (Part A)
- How do different vocal cord positions produce breathing, whispering, and speaking? (Part B)
PART A — Anatomy of the Larynx (Voice Box)
Think of the larynx like a door.
- Thyroid cartilage = Door frame
- Vocal ligaments = Two doors (vocal cords)
- Arytenoid cartilages = Door hinges
- Laryngeal muscles = People opening and closing the doors
The muscles pull the arytenoid cartilages, which move the vocal cords.
1. Vocal Ligaments (Vocal Cords)
- White bands in the middle
- Produce sound when air passes through them
👉 No vibration = No voice
👉 Vibration = Voice
2. Arytenoid Cartilages
Located at the back of the larynx.
Function:
They rotate and slide to
- Open vocal cords
- Close vocal cords
- Tighten vocal cords
Remember:
Arytenoids are the “controllers” of vocal cord movement.
3. Thyroarytenoid Muscle
Runs beside each vocal cord.
Function
- Relaxes the vocal cords
- Makes them shorter and thicker
Result
- Lower pitch
- Deeper voice
Easy Memory
Thyroarytenoid = Thick vocal cords = Low pitch
4. Posterior Cricoarytenoid Muscle
This is the only muscle that opens the vocal cords.
Function
Pulls arytenoids apart.
Result:
➡ Vocal cords move apart.
This is called
Abduction
Why?
During breathing, lots of air must enter the lungs.
So the airway must become wide.Easy Memory
Posterior = Pulls Open
Only abductor of the vocal cords.
This is a very common MBBS viva question.
5. Lateral Cricoarytenoid Muscle
Opposite action.
Function
Pulls vocal cords together.
This is called
Adduction
Result
Airway becomes narrow.
Necessary for
- Speaking
- Singing
- Loud sounds
Easy Memory
Lateral = Locks cords together
6. Transverse Arytenoid Muscle
Joins the two arytenoid cartilages.
Function
Brings both arytenoids together.
This completely closes the posterior part of the vocal cords.
Useful during
- Speech
- Swallowing
- Protecting airway
PART B — Vocal Cord Positions
The picture on the right shows how wide the vocal cords are opened.
1. Full Abduction
Vocal cords are opened as wide as possible.
Occurs during
Deep inspiration
Exercise
Heavy breathing
Airflow
⭐⭐⭐⭐⭐ Maximum
Voice
None
Think
Big opening = Easy breathing
2. Gentle Abduction
Vocal cords are slightly open.
Occurs during
Normal quiet breathing
Airflow
⭐⭐⭐⭐
Think
Normal breathing needs only a moderate opening.
3. Intermediate Position (Loud Whisper)
Opening is narrow.
Air still passes.
No vibration occurs.
Result
Loud whisper.
Think
Small gap
↓
Air escapes
↓
No vibration
↓
Whisper4. Stage Whisper
Posterior part remains open.
Front part nearly closed.
Air passes through the back.
Again,
No vibration.
Used for
- Dramatic whisper
- Loud whisper on stage
5. Phonation (Speaking)
Both vocal cords come together almost completely.
Only a tiny slit remains.
Air from lungs forces its way through.
The cords vibrate rapidly.
This vibration produces sound.
Concept
Lungs
↓
Air moves upward
↓
Closed vocal cords vibrate
↓
Voice is produced
Simple Flow of Voice Production
Brain
↓
Laryngeal muscles contract
↓
Vocal cords move together
↓
Air comes from lungs
↓
Air vibrates vocal cords
↓
Sound is produced
↓
Tongue + Lips + Mouth shape the sound
↓
SpeechMuscle Actions at a Glance
| Muscle | Main Action | Easy Memory |
|---|---|---|
| Posterior cricoarytenoid | Opens vocal cords (Abduction) | Only opener |
| Lateral cricoarytenoid | Closes vocal cords (Adduction) | Closer |
| Transverse arytenoid | Brings arytenoids together, closes posterior gap | Completes closure |
| Thyroarytenoid | Relaxes/shortens vocal cords | Low pitch |
Vocal Cord Positions at a Glance
| Position | Vocal Cord Position | Function |
|---|---|---|
| Full abduction | Fully open | Deep breathing |
| Gentle abduction | Slightly open | Quiet breathing |
| Intermediate | Narrow gap | Loud whisper |
| Stage whisper | Posterior gap only | Whisper without vibration |
| Phonation | Nearly closed | Speaking (vibration occurs) |
High-Yield MBBS Viva Points
- ✅ Posterior cricoarytenoid is the only abductor (opener) of the vocal cords.
- ✅ Lateral cricoarytenoid adducts (closes) the vocal cords.
- ✅ Transverse arytenoid closes the posterior part of the glottis.
- ✅ Thyroarytenoid relaxes and shortens the vocal cords, producing a lower-pitched voice.
- ✅ Voice is produced only when the vocal cords vibrate.
- ✅ During quiet breathing, the vocal cords are gently abducted.
- ✅ During deep inspiration, they are fully abducted.
- ✅ During phonation (speaking), the vocal cords are almost completely closed so exhaled air can make them vibrate.
One-Line Concept to Remember
The laryngeal muscles act like door operators: they open the vocal cords for breathing, partially open them for whispering, and bring them together so exhaled air can vibrate them to produce speech.