

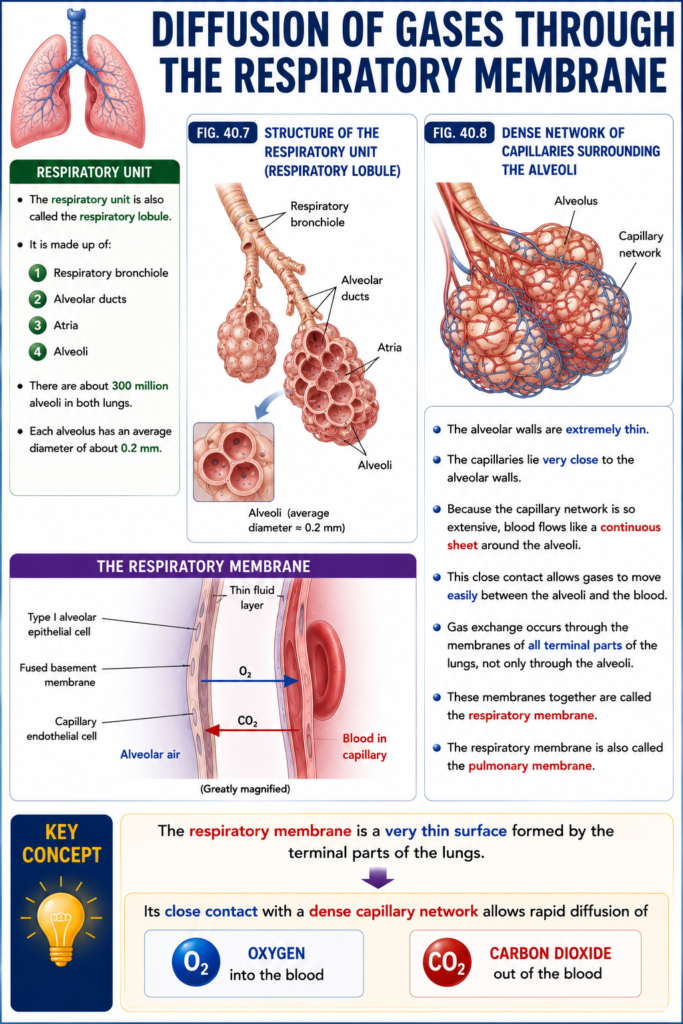
Respiratory Unit
- The respiratory unit is also called the respiratory lobule.
- It is made up of:
- Respiratory bronchiole
- Alveolar ducts
- Atria
- Alveoli
- There are about 300 million alveoli in both lungs.
- Each alveolus has an average diameter of about 0.2 mm.
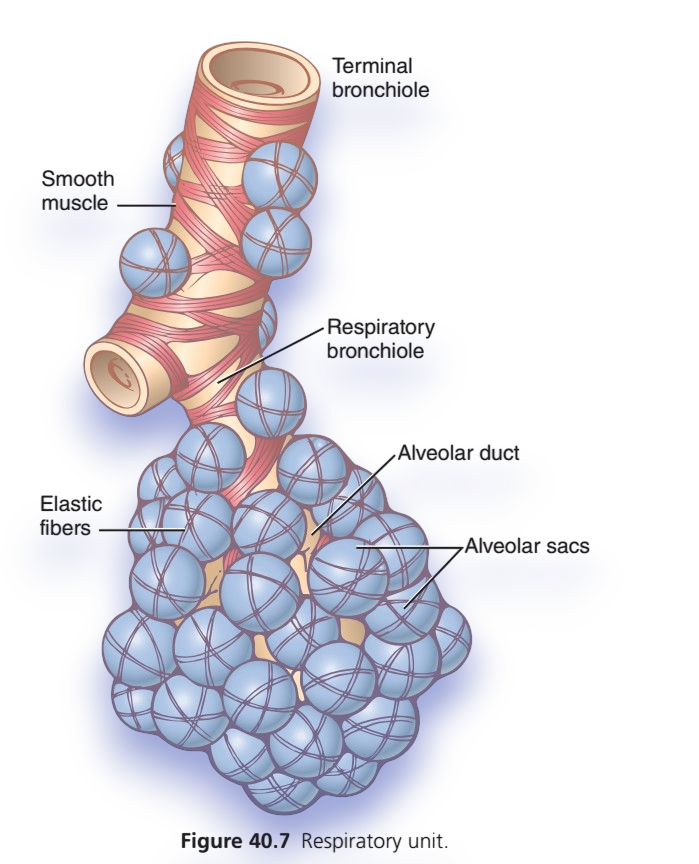
Fig. 40.7
- Fig. 40.7 shows the structure of the respiratory unit (respiratory lobule).
Fig. 40.8
- Fig. 40.8 shows the dense network of interconnected capillaries surrounding the alveoli.
- The alveolar walls are extremely thin.
- The capillaries lie very close to the alveolar walls.
- Because the capillary network is so extensive, blood flows like a continuous sheet around the alveoli.
- This close contact allows gases to move easily between the alveoli and the blood.
- Gas exchange occurs through the membranes of all terminal parts of the lungs, not only through the alveoli.
- These membranes together are called the respiratory membrane.
- The respiratory membrane is also called the pulmonary membrane.
KEY CONCEPT
- The respiratory membrane is a very thin surface formed by the terminal parts of the lungs. Its close contact with a dense capillary network allows rapid diffusion of O₂ into the blood and CO₂ out of the blood.
Figure 40.7 – Respiratory Unit (Respiratory Lobule)
Super Easy & Conceptual Explanation for MBBS Students
This figure shows the smallest functional part of the lung where gas exchange occurs.
👉 Think of it as a tree with a bunch of grapes:
- 🌳 Branches = Bronchioles
- 🍇 Grapes = Alveoli (air sacs)
The oxygen you breathe in finally reaches these tiny grape-like sacs.
Follow the Air Step by Step
Terminal Bronchiole
↓
Respiratory Bronchiole
↓
Alveolar Duct
↓
Alveolar Sacs
↓
AlveoliThis is the exact pathway air follows before oxygen enters the blood.
1. Terminal Bronchiole
📍 Last conducting airway
- It is the last part that only conducts air.
- No gas exchange occurs here.
Easy Memory
🚗 It is like the last road before reaching a parking area.
Function:
- Carries air toward the respiratory zone.
2. Smooth Muscle
📍 Muscle around bronchioles
The pink spiral bands represent smooth muscle.
Function
- Controls the diameter of bronchioles.
- Can become narrow or wide.
Clinical Correlation
- Contraction → Bronchoconstriction (Asthma)
- Relaxation → Bronchodilation
Easy Memory
🚪 Like a door that can open wider or become narrow.
3. Respiratory Bronchiole
📍 Beginning of the respiratory zone
This is where gas exchange starts.
Unlike the terminal bronchiole:
- Small alveoli begin appearing on its walls.
- Oxygen and carbon dioxide can now diffuse.
Easy Memory
🚪 This is the entrance to the gas exchange area.
4. Alveolar Duct
📍 Passage surrounded by alveoli
This tube is almost completely lined by alveoli.
Air passes through it before entering the alveolar sacs.
Function
- Conducts air deeper.
- Participates in gas exchange.
Easy Memory
🏠 Think of it as the main hallway leading to many rooms.
5. Alveolar Sacs
📍 Cluster of alveoli
Several alveoli join together to form one alveolar sac.
Easy Memory
🍇 Like a bunch of grapes attached together.
6. Alveoli (Blue Sacs)
📍 Site of gas exchange
These tiny air sacs are the most important part of the respiratory system.
Here:
- Oxygen enters pulmonary capillaries.
- Carbon dioxide leaves the blood.
Facts
- About 300 million alveoli in both lungs.
- Diameter ≈ 0.2 mm
- Very thin wall (one cell thick).
Easy Memory
🫧 Tiny balloons where oxygen enters blood and carbon dioxide leaves blood.
7. Elastic Fibers
📍 Elastic support around alveoli
The thin fibers surrounding alveoli are elastic fibers.
Function
During inspiration:
- Stretch
During expiration:
- Recoil
- Push air out
Easy Memory
🧵 Like a rubber band around each balloon.
Stretch → Inhale
Snap back → Exhale
Whole Figure in One Story
Imagine entering a grape garden.
🚶 You walk through:
Road
➡️ Terminal bronchiole
↓
Small pathway
➡️ Respiratory bronchiole
↓
Main corridor
➡️ Alveolar duct
↓
Bunches of grapes
➡️ Alveolar sacs
↓
Each grape
➡️ Alveolus
Inside every grape:
🩸 Blood arrives with CO₂
🌬️ Oxygen enters blood
CO₂ leaves blood
Blood becomes oxygen-rich and returns to the heart.
Concept Flow Chart
r
↓
Terminal Bronchiole
(No gas exchange)
↓
Respiratory Bronchiole
(Gas exchange begins)
↓
Alveolar Duct
(More gas exchange)
↓
Alveolar Sac
(Collection of alveoli)
↓
Alveoli
(Main gas exchange site)
↓
Pulmonary Capillaries
O₂ → Blood
CO₂ → AlveolusExam Pearls ⭐
✅ Terminal bronchiole
- Last conducting airway
- No gas exchange
✅ Respiratory bronchiole
- First respiratory airway
- Gas exchange begins
✅ Alveolar duct
- Air passage lined by alveoli
- Gas exchange continues
✅ Alveolar sac
- Cluster of alveoli
✅ Alveolus
- Functional unit of gas exchange
- Thin wall for rapid diffusion
✅ Smooth muscle
- Regulates airway diameter
- Bronchoconstriction in asthma
✅ Elastic fibers
Ultra-Short Revision
🫁 Respiratory Unit = The gas-exchange factory of the lung
Terminal Bronchiole
↓
Respiratory Bronchiole
↓
Alveolar Duct
↓
Alveolar Sac
↓
Alveoli
↓
O₂ enters blood
CO₂ leaves bloodOne-Line Concept
The respiratory unit is the smallest functional part of the lung, consisting of the respiratory bronchiole, alveolar duct, alveolar sacs, and alveoli, where oxygen diffuses into the blood and carbon dioxide diffuses out of the blood.
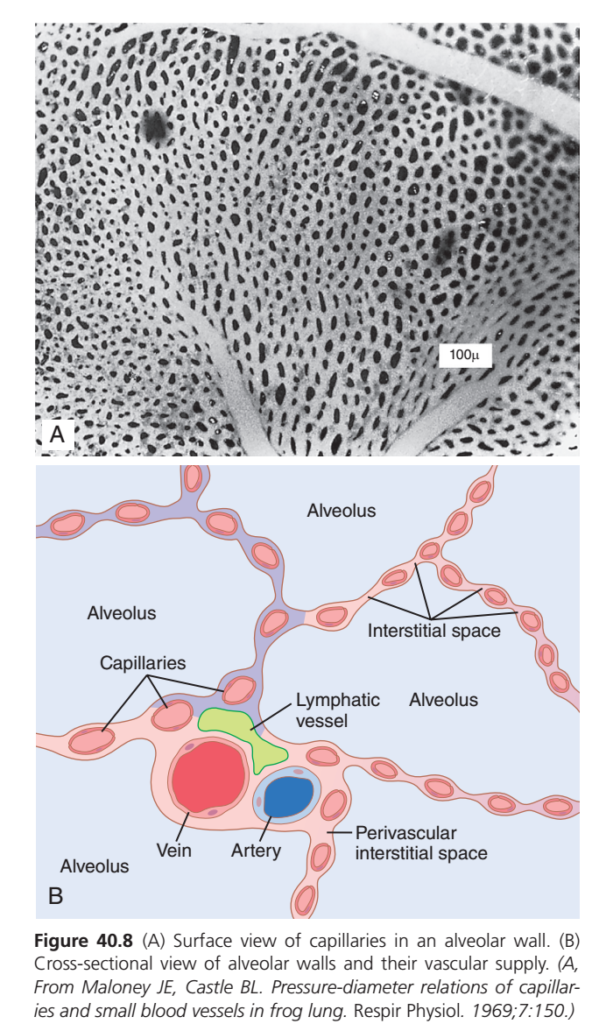
Figure 40.8 – Blood Capillaries in the Alveolar Wall
Super Easy & Conceptual Explanation for MBBS Students
This figure explains how the alveoli receive blood and where oxygen and carbon dioxide are exchanged.
It has two parts:
- A = Real microscopic view
- B = Simplified diagram (easy to understand)
Part A – Microscopic View of the Alveolar Wall
What are the black oval structures?
The numerous black oval structures are red blood cells (RBCs) flowing inside pulmonary capillaries.
What does this tell us?
The alveolar wall is covered by a dense network of capillaries.
👉 This means almost every part of an alveolus is touching blood.
Why is this important?
The greater the contact between air and blood, the faster oxygen and carbon dioxide can diffuse.
Easy Memory
Imagine wrapping a balloon with a very fine fishing net.
- 🎈 Balloon = Alveolus
- 🕸️ Net = Capillary network
Almost the entire balloon is covered, so gas exchange can occur everywhere.
Part B – Cross-Section of the Alveolar Wall
This diagram cuts through the alveolus to show what lies inside its wall.
Let’s identify each structure.
1. Alveolus
🩵 The large empty blue spaces are alveoli.
Function
They contain the inhaled air.
Here:
- Oxygen waits to enter the blood.
- Carbon dioxide arrives from the blood to be exhaled.
Easy Memory
🫧 Think of an alveolus as a tiny air balloon.
2. Capillaries
The tiny blood vessels running within the alveolar wall are pulmonary capillaries.
Function
They bring blood close to the air.
Inside these capillaries:
- Blood arriving has low O₂ and high CO₂.
- Blood leaving has high O₂ and low CO₂.
Easy Memory
🚚 Capillaries are delivery trucks carrying blood to the alveoli.
3. Interstitial Space
This is the very thin tissue layer between:
- The alveolar wall
- The capillary wall
Function
It contains:
- Small amount of connective tissue
- Elastic fibers
- Fluid
Why is it important?
Oxygen must pass through this thin space to reach the blood.
The thinner it is, the faster diffusion occurs.
Easy Memory
🚪 It is the tiny hallway between the air and the blood.
4. Artery (Pulmonary Arteriole)
The blue vessel labeled artery carries blood toward the alveoli.
Blood inside
- Low oxygen
- High carbon dioxide
Although it is called an artery, it carries deoxygenated blood because it is part of the pulmonary circulation.
Easy Memory
➡️ Artery = Brings blood to the gas exchange site.
5. Vein (Pulmonary Venule)
The red vessel labeled vein carries blood away from the alveoli.
Blood inside
- High oxygen
- Low carbon dioxide
Easy Memory
⬅️ Vein = Takes freshly oxygenated blood back to the heart.
6. Lymphatic Vessel
The green structure is a lymphatic vessel.
Function
It removes:
- Extra tissue fluid
- Proteins
- Waste
This prevents fluid from collecting around the alveoli.
Clinical Importance
If lymph drainage fails:
➡️ Fluid accumulates.
➡️ Diffusion becomes difficult.
➡️ Pulmonary edema develops.
Easy Memory
🚰 The lymphatic vessel is the lung’s drainage pipe.
7. Perivascular Interstitial Space
This is the tissue space surrounding the larger blood vessels.
Function
It acts as a passage for:
- Tissue fluid
- Lymph
It also helps prevent excessive fluid buildup around vessels.
How Does Gas Exchange Occur?
Step 1
You inhale.
The alveolus fills with oxygen-rich air.
⬇️
Step 2
Blood arriving in the capillary contains:
- Low oxygen
- High carbon dioxide
⬇️
Step 3
Because oxygen concentration is higher inside the alveolus:
O₂ diffuses from alveolus → capillary blood.
⬇️
Step 4
Because carbon dioxide concentration is higher in blood:
CO₂ diffuses from blood → alveolus.
⬇️
Step 5
Blood leaves oxygenated.
Carbon dioxide is exhaled.
Concept Flow
Inhaled Air
↓
Alveolus
↓
O₂ diffuses
↓
Interstitial Space
↓
Capillary Wall
↓
Red Blood Cell
↓
Pulmonary Vein
↓
Left Side of Heart
------------------------
Blood brings CO₂
↓
Capillary
↓
Interstitial Space
↓
Alveolus
↓
Exhaled AirWhy Are There So Many Capillaries?
Because the lungs need an enormous surface area for rapid gas exchange.
More capillaries mean:
- ✅ More blood reaches the alveoli.
- ✅ Larger contact area.
- ✅ Faster oxygen uptake.
- ✅ Faster carbon dioxide removal.
Clinical Correlation
Pulmonary Edema
When fluid accumulates in the interstitial space or inside the alveoli:
- The diffusion distance increases.
- Oxygen cannot reach the blood efficiently.
- The patient develops hypoxemia and shortness of breath.
Key Concept: The thinner the alveolar wall, the faster the diffusion. Thickening (e.g., edema or fibrosis) slows gas exchange.
Exam Pearls ⭐
- ✅ Alveoli are surrounded by a dense capillary network.
- ✅ Oxygen diffuses from alveoli to capillaries.
- ✅ Carbon dioxide diffuses from capillaries to alveoli.
- ✅ The interstitial space is normally very thin, allowing rapid diffusion.
- ✅ Lymphatic vessels remove excess fluid and help keep the lungs dry.
- ✅ Pulmonary arteries carry deoxygenated blood to the lungs.
- ✅ Pulmonary veins carry oxygenated blood back to the heart.
Ultra-Short Revision
🫧 Alveolus = Air-filled sac
🩸 Capillary = Brings blood for gas exchange
🚪 Interstitial space = Very thin diffusion pathway
💙 Pulmonary artery = Low O₂, high CO₂ blood arrives
❤️ Pulmonary vein = High O₂, low CO₂ blood leaves
🚰 Lymphatic vessel = Removes excess fluid
One-Line Concept:
Each alveolus is wrapped by an extensive capillary network separated by an extremely thin interstitial space, allowing rapid diffusion of oxygen into the blood and carbon dioxide out of the blood while lymphatic vessels prevent fluid accumulation that would impair gas exchange.
Respiratory Membrane
Fig. 40.9
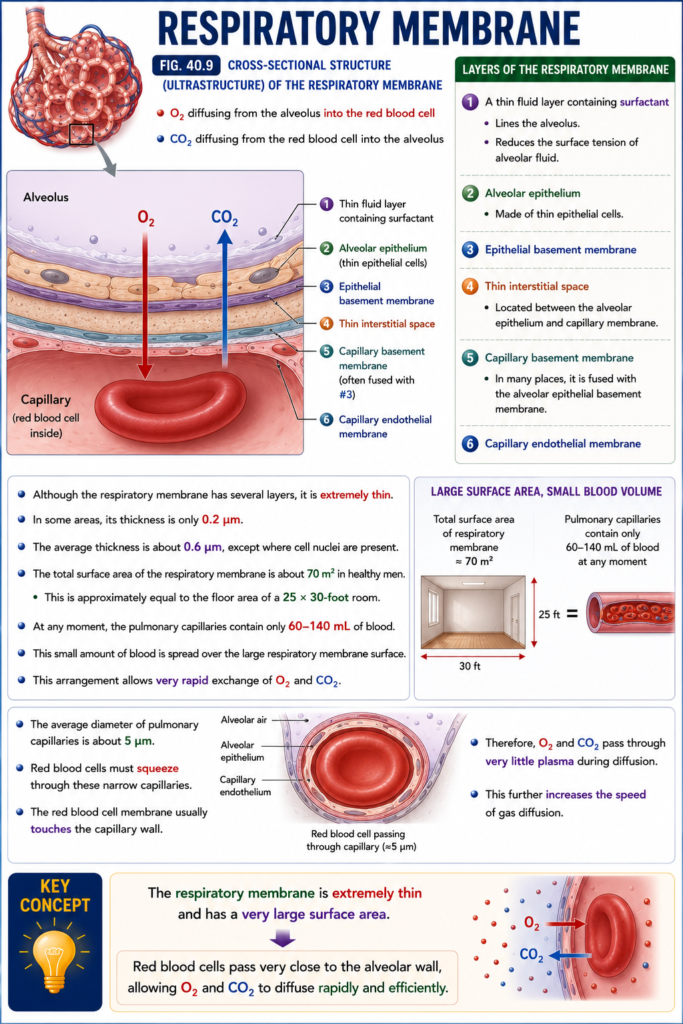
- Fig. 40.9 shows the cross-sectional structure (ultrastructure) of the respiratory membrane.
- It also shows:
- O₂ diffusing from the alveolus into the red blood cell
- CO₂ diffusing from the red blood cell into the alveolus
- The respiratory membrane consists of the following layers:
- A thin fluid layer containing surfactant
- Lines the alveolus.
- Reduces the surface tension of alveolar fluid.
- Alveolar epithelium
- Made of thin epithelial cells.
- Epithelial basement membrane
- Thin interstitial space
- Located between the alveolar epithelium and capillary membrane.
- Capillary basement membrane
- In many places, it is fused with the alveolar epithelial basement membrane.
- Capillary endothelial membrane
- A thin fluid layer containing surfactant
- Although the respiratory membrane has several layers, it is extremely thin.
- In some areas, its thickness is only 0.2 μm.
- The average thickness is about 0.6 μm, except where cell nuclei are present.
- The total surface area of the respiratory membrane is about 70 m² in healthy men.
- This is approximately equal to the floor area of a 25 × 30-foot room.
- At any moment, the pulmonary capillaries contain only 60–140 mL of blood.
- This small amount of blood is spread over the large respiratory membrane surface.
- This arrangement allows very rapid exchange of O₂ and CO₂.
- The average diameter of pulmonary capillaries is about 5 μm.
- Red blood cells must squeeze through these narrow capillaries.
- The red blood cell membrane usually touches the capillary wall.
- Therefore, O₂ and CO₂ pass through very little plasma during diffusion.
- This further increases the speed of gas diffusion.
KEY CONCEPT
- The respiratory membrane is extremely thin and has a very large surface area. Red blood cells pass very close to the alveolar wall, allowing O₂ and CO₂ to diffuse rapidly and efficiently.
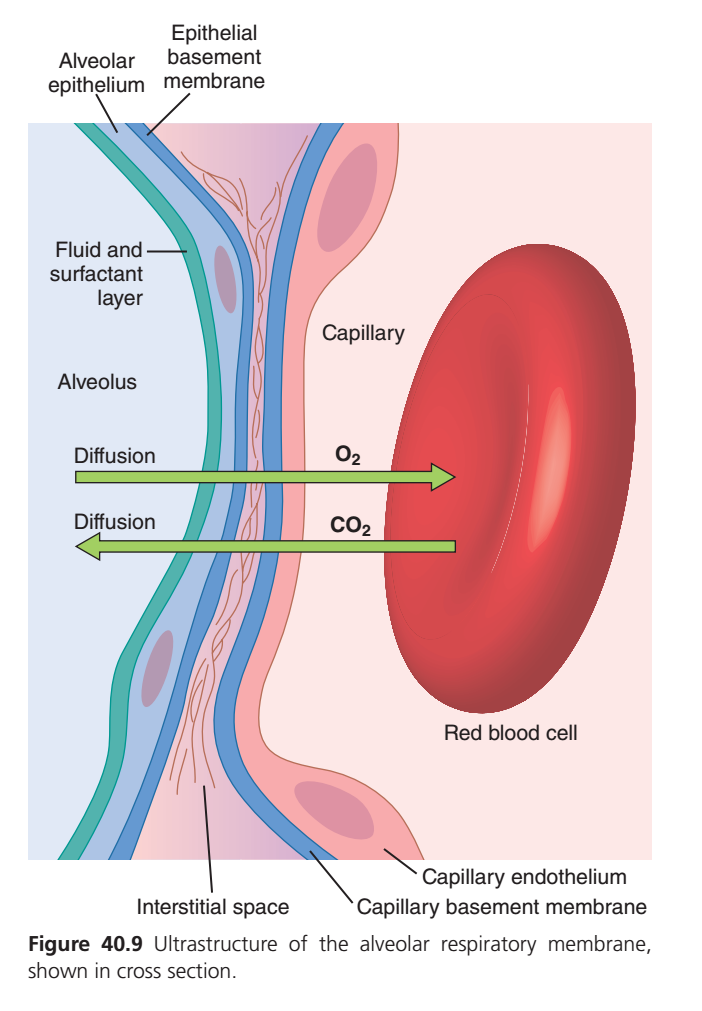
Figure 40.9 – Ultrastructure of the Respiratory (Alveolar-Capillary) Membrane
Super Easy & Conceptual Explanation for MBBS Students
This figure shows the respiratory membrane, which is the very thin barrier between the air inside the alveolus and the blood inside the pulmonary capillary.
👉 This is the exact place where gas exchange occurs.
Golden Rule
Oxygen (O₂) moves from the alveolus → blood, while carbon dioxide (CO₂) moves from the blood → alveolus.
Imagine This Figure as Crossing a Thin Wall
Think of the alveolus as one room and the red blood cell (RBC) as another room.
Between them is a very thin wall.
- 🚶 Oxygen crosses this wall to enter the blood.
- 🚶 Carbon dioxide crosses the same wall in the opposite direction.
The thinner the wall, the faster the gases cross.
Layers of the Respiratory Membrane (From Air to Blood)
To understand diffusion, follow the oxygen molecule from the alveolus to the RBC.
1. Fluid and Surfactant Layer
(Innermost layer facing the air)
This thin film covers the inside of every alveolus.
Functions
- Keeps the alveolus moist.
- Surfactant reduces surface tension, preventing alveolar collapse during expiration.
- Oxygen first dissolves in this thin fluid before diffusing further.
Easy Memory
🧴 Like a thin soap film coating the inside of a balloon.
2. Alveolar Epithelium
(Type I alveolar cells)
This is the thin wall of the alveolus.
Function
- Allows oxygen and carbon dioxide to diffuse rapidly.
Easy Memory
🫧 It is the wall of the tiny air balloon.
3. Epithelial Basement Membrane
A very thin supporting layer beneath the alveolar epithelium.
Function
- Provides structural support.
- Helps maintain the integrity of the alveolar wall.
Easy Memory
🏗️ Like the foundation under a building wall.
4. Interstitial Space
The narrow space between the alveolar wall and the capillary wall.
Normally it contains:
- A tiny amount of tissue fluid
- Connective tissue
- Elastic fibers
Function
- Acts as the pathway through which gases pass.
Clinical Importance
If this space becomes thick because of pulmonary edema or pulmonary fibrosis, oxygen diffusion slows.
Easy Memory
🚪 A tiny hallway connecting the alveolus to the capillary.
5. Capillary Basement Membrane
A thin supporting layer beneath the capillary endothelium.
Function
- Supports the capillary wall.
- Often fuses with the epithelial basement membrane, making the diffusion barrier extremely thin.
Easy Memory
🏗️ Foundation of the blood vessel wall.
6. Capillary Endothelium
This is the inner lining of the pulmonary capillary.
Function
- The last barrier before oxygen enters the blood.
Easy Memory
🩸 The wall of the blood vessel.
7. Red Blood Cell (RBC)
Once oxygen crosses all the membrane layers, it enters the RBC.
Inside the RBC:
- Oxygen binds to hemoglobin (Hb).
- Hemoglobin transports oxygen throughout the body.
At the same time:
- Carbon dioxide leaves the RBC.
- It diffuses back into the alveolus to be exhaled.
Easy Memory
🚚 The RBC is the oxygen delivery truck.
How Oxygen Travels
Inspired Air
↓
Fluid + Surfactant Layer
↓
Alveolar Epithelium
↓
Epithelial Basement Membrane
↓
Interstitial Space
↓
Capillary Basement Membrane
↓
Capillary Endothelium
↓
Red Blood Cell
↓
HemoglobinHow Carbon Dioxide Travels
Red Blood Cell
↓
Capillary Endothelium
↓
Capillary Basement Membrane
↓
Interstitial Space
↓
Epithelial Basement Membrane
↓
Alveolar Epithelium
↓
Fluid + Surfactant Layer
↓
Alveolus
↓
Expired AirWhy Does Oxygen Move Into the Blood?
Because:
- Alveolus has a high oxygen concentration (high PO₂).
- Blood arriving at the lungs has a low oxygen concentration (low PO₂).
➡️ Oxygen naturally diffuses from high concentration to low concentration.
Why Does Carbon Dioxide Move Into the Alveolus?
Because:
- Blood has a high carbon dioxide concentration (high PCO₂).
- Alveolus has a low carbon dioxide concentration (low PCO₂).
➡️ Carbon dioxide diffuses from blood to alveolus.
Why Is the Respiratory Membrane So Thin?
The respiratory membrane is extremely thin (about 0.2–0.6 µm).
Advantages
- ⚡ Very rapid oxygen diffusion.
- ⚡ Very rapid carbon dioxide diffusion.
- ⚡ Efficient gas exchange during every heartbeat and breath.
Key Concept: Diffusion speed is inversely proportional to membrane thickness. A thinner membrane allows gases to diffuse more quickly.
Clinical Correlation
Pulmonary Edema
Fluid accumulates in the interstitial space or alveoli.
➡️ Diffusion distance increases.
➡️ Oxygen reaches the blood more slowly.
➡️ Patient develops hypoxemia and shortness of breath.
Pulmonary Fibrosis
Scar tissue thickens the respiratory membrane.
➡️ Oxygen diffusion becomes difficult.
➡️ Patients often experience exertional breathlessness because oxygen cannot cross the thickened membrane efficiently.
Exam Pearls ⭐
- ✅ The respiratory membrane is the site of gas exchange.
- ✅ O₂ diffuses from alveolus → blood.
- ✅ CO₂ diffuses from blood → alveolus.
- ✅ The membrane consists of:
- Fluid + surfactant layer
- Alveolar epithelium
- Epithelial basement membrane
- Interstitial space
- Capillary basement membrane
- Capillary endothelium
- ✅ A thin respiratory membrane allows rapid diffusion.
- ✅ Edema or fibrosis increases membrane thickness and impairs oxygen diffusion.
Ultra-Short Revision
Respiratory Membrane Layers
Alveolus
│
Fluid + Surfactant
│
Alveolar Epithelium
│
Epithelial Basement Membrane
│
Interstitial Space
│
Capillary Basement Membrane
│
Capillary Endothelium
│
Red Blood CellGas Movement
🟢 O₂: Alveolus ➜ Blood ➜ Hemoglobin
🔴 CO₂: Blood ➜ Alveolus ➜ Exhaled Air
One-Line Concept
The respiratory (alveolar-capillary) membrane is an extremely thin barrier separating alveolar air from pulmonary capillary blood, allowing rapid diffusion of oxygen into the blood and carbon dioxide out of the blood to maintain efficient gas exchange.
Factors Affecting Rate of Gas Diffusion Through the Respiratory Membrane
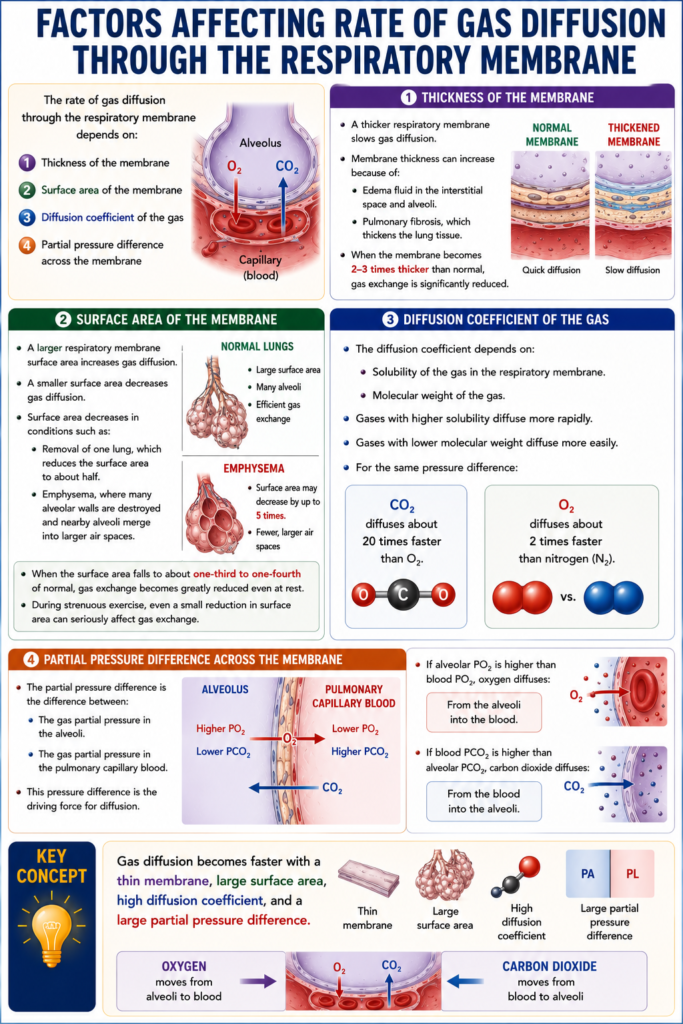
- The rate of gas diffusion through the respiratory membrane depends on:
- Thickness of the membrane
- Surface area of the membrane
- Diffusion coefficient of the gas
- Partial pressure difference across the membrane
- A thicker respiratory membrane slows gas diffusion.
- Membrane thickness can increase because of:
- Edema fluid in the interstitial space and alveoli.
- Pulmonary fibrosis, which thickens the lung tissue.
- When the membrane becomes 2–3 times thicker than normal, gas exchange is significantly reduced.
- A larger respiratory membrane surface area increases gas diffusion.
- A smaller surface area decreases gas diffusion.
- Surface area decreases in conditions such as:
- Removal of one lung, which reduces the surface area to about half.
- Emphysema, where many alveolar walls are destroyed and nearby alveoli merge into larger air spaces.
- In emphysema, the total respiratory membrane surface area may decrease by up to 5 times.
- When the surface area falls to about one-third to one-fourth of normal, gas exchange becomes greatly reduced even at rest.
- During strenuous exercise, even a small reduction in surface area can seriously affect gas exchange.
- The diffusion coefficient depends on:
- Solubility of the gas in the respiratory membrane.
- Molecular weight of the gas.
- Gases with higher solubility diffuse more rapidly.
- Gases with lower molecular weight diffuse more easily.
- For the same pressure difference:
- CO₂ diffuses about 20 times faster than O₂.
- O₂ diffuses about 2 times faster than nitrogen (N₂).
- The partial pressure difference is the difference between:
- The gas partial pressure in the alveoli.
- The gas partial pressure in the pulmonary capillary blood.
- This pressure difference is the driving force for diffusion.
- If alveolar PO₂ is higher than blood PO₂, oxygen diffuses:
- From the alveoli into the blood.
- If blood PCO₂ is higher than alveolar PCO₂, carbon dioxide diffuses:
- From the blood into the alveoli.
KEY CONCEPT
- Gas diffusion becomes faster with a thin membrane, large surface area, high diffusion coefficient, and a large partial pressure difference. Oxygen moves from alveoli to blood, while carbon dioxide moves from blood to alveoli.
Diffusing Capacity of the Respiratory Membrane
- Diffusing capacity measures how well the respiratory membrane exchanges a gas between the alveoli and the pulmonary blood.
- It is defined as:
- The volume of a gas that diffuses through the respiratory membrane in one minute for a partial pressure difference of 1 mm Hg.
- Diffusing capacity depends on all the factors that affect gas diffusion through the respiratory membrane.
KEY CONCEPT
- Diffusing capacity is a measure of how efficiently the respiratory membrane transfers gases. It is the amount of gas that diffuses per minute for each 1 mm Hg pressure difference.
Lung Diffusing Capacity for Oxygen
- In an average healthy young man, the lung diffusing capacity for oxygen (O₂) at rest is about 21 mL/min/mm Hg.
- This means that 21 mL of O₂ diffuses through the respiratory membrane each minute for every 1 mm Hg pressure difference.
- During normal quiet breathing, the average O₂ partial pressure difference across the respiratory membrane is about 11 mm Hg.
- Total oxygen diffusion is calculated as: 11 mm Hg × 21 mL/min/mm Hg = 231 mL/min (≈230 mL/min)
- Therefore, about 230 mL of O₂ diffuses through the respiratory membrane each minute.
- This amount is approximately equal to the oxygen used by the body at rest.
KEY CONCEPT
- At rest, the lungs transfer about 230 mL of O₂ per minute, which matches the body’s normal oxygen requirement.
Increased Lung Diffusing Capacity for Oxygen During Exercise
- During strenuous exercise, pulmonary blood flow and alveolar ventilation increase greatly.
- As a result, the lung diffusing capacity for O₂ increases to about 3 times the resting value.
- This increase occurs because:
- Previously inactive pulmonary capillaries open, and already open capillaries dilate.
- This increases the surface area available for oxygen diffusion.
- Ventilation and blood flow become better matched.
- This is called the ventilation-perfusion (V/Q) ratio.
- Previously inactive pulmonary capillaries open, and already open capillaries dilate.
- During exercise, blood receives more oxygen because:
- Alveolar ventilation increases.
- The respiratory membrane diffuses oxygen more efficiently.
KEY CONCEPT
- During exercise, the lung diffusing capacity for O₂ increases about threefold due to increased capillary surface area and better ventilation-perfusion matching, allowing more oxygen to enter the blood.
Lung Diffusing Capacity for Carbon Dioxide
- The total lung diffusing capacity for CO₂ has not been measured directly.
- This is because CO₂ diffuses through the respiratory membrane very rapidly.
- The average PCO₂ difference between the pulmonary blood and alveoli is less than 1 mm Hg.
- This pressure difference is too small to measure accurately with current techniques.
- Studies of other gases show that diffusing capacity is directly related to the diffusion coefficient of the gas.
- Since CO₂ has a diffusion coefficient more than 20 times greater than O₂, its diffusing capacity is much higher.
- Estimated lung diffusing capacity for CO₂:
- At rest: about 400–450 mL/min/mm Hg
- During exercise: about 1200–1300 mL/min/mm Hg
Fig. 40.10
- Fig. 40.10 compares the lung diffusing capacities of:
- Carbon monoxide (CO)
- Oxygen (O₂)
- Carbon dioxide (CO₂)
- It shows that:
- CO₂ has the highest diffusing capacity.
- Exercise increases the diffusing capacity of all three gases.
KEY CONCEPT
- CO₂ diffuses much faster than O₂, giving it a much higher diffusing capacity. During exercise, the diffusing capacity of CO₂ increases further because gas exchange becomes more efficient.
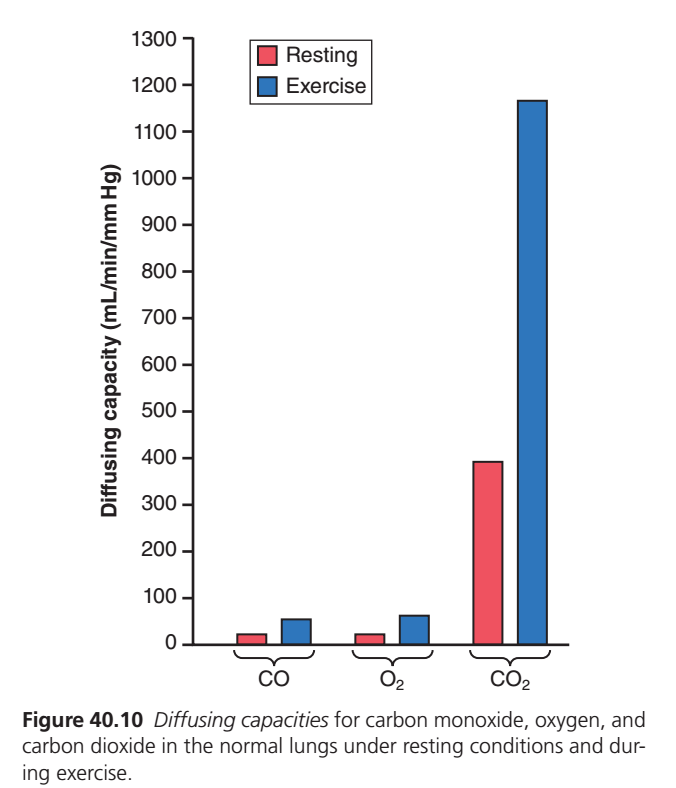
Figure 40.10 – Diffusing Capacity of CO, O₂, and CO₂
Superfast self learning concept
This graph compares how easily different gases diffuse across the respiratory (alveolar-capillary) membrane.
It also compares diffusion:
- ❤️ At Rest (Red bars)
- 🏃 During Exercise (Blue bars)
First Understand the Y-Axis
Diffusing Capacity (mL/min/mmHg)
This means:
How many milliliters of a gas can cross the respiratory membrane in one minute for every 1 mmHg pressure difference.
Simple Meaning
Higher bar = Gas diffuses more easily and more rapidly.
Lower bar = Gas diffuses more slowly.
The Three Gases on the X-Axis
- CO = Carbon Monoxide
- O₂ = Oxygen
- CO₂ = Carbon Dioxide
1. Carbon Monoxide (CO)
At Rest
📊 About 21 mL/min/mmHg
During Exercise
📊 About 50–65 mL/min/mmHg
Why is CO measured?
CO binds very strongly to hemoglobin.
As soon as CO enters the blood:
➡️ Hemoglobin immediately binds it.
Therefore,
Blood CO pressure remains almost zero.
This makes CO useful for measuring the diffusing capacity of the lungs (DLCO).
Easy Memory
CO behaves like a passenger who immediately jumps into a taxi (hemoglobin).
So it never builds up in the blood.
2. Oxygen (O₂)
At Rest
📊 About 21 mL/min/mmHg
During Exercise
📊 About 65 mL/min/mmHg
Why does oxygen diffuse faster during exercise?
During exercise:
- More pulmonary capillaries open (capillary recruitment).
- Existing capillaries widen (capillary distension).
- More blood comes into contact with alveoli.
- Surface area for diffusion increases.
Therefore,
✅ Oxygen diffusing capacity approximately triples.
Easy Memory
🏃 During exercise, the lungs open more exchange counters, allowing oxygen to enter the blood much faster.
3. Carbon Dioxide (CO₂)
At Rest
📊 About 400 mL/min/mmHg
During Exercise
📊 About 1200 mL/min/mmHg
Notice something amazing!
CO₂ has the tallest bars.
This means:
👉 Carbon dioxide diffuses much more easily than oxygen.
Why Does CO₂ Diffuse Much Faster?
Even though CO₂ is heavier than oxygen, it is far more soluble in the respiratory membrane and body fluids.
Because diffusion depends greatly on solubility, CO₂ crosses the membrane about 20 times more readily than oxygen.
Easy Memory
Think of two people trying to pass through a crowd:
- 🚶 Oxygen moves normally.
- 🏃 Carbon dioxide is like someone who can slip through every gap effortlessly because it dissolves so well.
Why Do All Bars Become Taller During Exercise?
During exercise:
❤️ Cardiac output increases.
🫁 Pulmonary blood flow increases.
🩸 More capillaries become perfused.
🫧 Surface area for gas exchange increases.
The respiratory membrane becomes more effective.
Therefore,
Diffusing capacity increases for every gas.
Comparison Table
| Gas | Rest | Exercise | Main Reason |
|---|---|---|---|
| CO | Low (~21) | Moderate (~50–65) | Used to measure lung diffusing capacity because it binds avidly to hemoglobin. |
| O₂ | Low (~21) | Higher (~65) | More capillaries are recruited and surface area increases during exercise. |
| CO₂ | Very High (~400) | Extremely High (~1200) | Very high solubility allows rapid diffusion. |
Why Is CO₂ Diffusing Capacity So High?
Remember:
Diffusion depends on:
- Membrane thickness
- Surface area
- Pressure difference
- Diffusion coefficient
The diffusion coefficient depends mainly on:
- Solubility
- Molecular weight
Although CO₂ has a larger molecular weight than O₂, its much greater solubility dominates, making its diffusion coefficient—and therefore its diffusing capacity—much higher.
Easy Story
Imagine three students crossing a doorway.
👦 CO
Walks normally but immediately disappears into a room (binds to Hb).
👦 O₂
Walks at a normal speed.
👦 CO₂
Slides through the doorway very easily because the floor is slippery (high solubility).
When the doorway becomes wider during exercise:
🚪 Everyone crosses faster.
Exam Pearls ⭐
✅ Diffusing capacity = Amount of gas diffusing per minute per 1 mmHg pressure difference.
✅ CO is used to measure lung diffusing capacity (DLCO) because it binds strongly to hemoglobin, keeping capillary CO partial pressure nearly zero.
✅ Oxygen diffusing capacity increases about threefold during exercise due to capillary recruitment and increased surface area.
✅ Carbon dioxide diffuses about 20 times more readily than oxygen because of its much greater solubility.
✅ Exercise increases the diffusing capacity of all gases by improving pulmonary perfusion and available surface area.
Ultra-Short Revision
📊 Graph Message
Rest → Lower diffusion
Exercise → Higher diffusionDiffusion Ability
🥇 CO₂ → Highest
🥈 O₂ → Moderate
🥉 CO → Similar measured diffusing capacity to O₂, but mainly used as a test gas
During Exercise
⬆️ More pulmonary capillaries open
⬆️ Surface area increases
⬆️ Diffusing capacity increases
One-Line Concept
The lungs diffuse gases more efficiently during exercise because pulmonary capillary recruitment and distension increase the surface area for gas exchange. Among the gases shown, carbon dioxide has the highest diffusing capacity because of its very high solubility, while carbon monoxide is used clinically to measure lung diffusing capacity (DLCO) due to its strong binding to hemoglobin.
Carbon Monoxide Method for Measuring Lung Diffusing Capacity
- The O₂ diffusing capacity can be calculated by measuring:
- Alveolar PO₂
- PO₂ in the pulmonary capillary blood
- Rate of O₂ uptake by the blood
- However, measuring PO₂ in the pulmonary capillary blood is very difficult and not practical in routine use.
- Therefore, physiologists usually measure carbon monoxide (CO) diffusing capacity instead.
- The O₂ diffusing capacity is then calculated from the CO diffusing capacity.
- The CO method works as follows:
- A small amount of CO is inhaled into the alveoli.
- The partial pressure of CO in the alveoli is measured from alveolar air samples.
- The CO partial pressure in the blood is almost zero.
- This is because hemoglobin binds CO very rapidly.
- Therefore, the pressure difference across the respiratory membrane is equal to the alveolar CO partial pressure.
- The amount of CO absorbed in a short time is measured.
- The CO diffusing capacity is calculated by dividing:
- Volume of CO absorbed
- Alveolar CO partial pressure
- To calculate the O₂ diffusing capacity:
- Multiply the CO diffusing capacity by 1.23.
- This is because O₂ has a diffusion coefficient 1.23 times greater than CO.
- In healthy young men at rest:
- CO diffusing capacity = 17 mL/min/mm Hg
- O₂ diffusing capacity = 17 × 1.23 = 21 mL/min/mm Hg
KEY CONCEPT
- Because CO binds rapidly to hemoglobin, its blood partial pressure remains almost zero, making it easy to measure lung diffusing capacity. The O₂ diffusing capacity is obtained by multiplying the CO diffusing capacity by 1.23.
Effect of Ventilation-Perfusion Ratio on Alveolar Gas Concentration
- The PO₂ and PCO₂ in the alveoli depend on:
- Rate of alveolar ventilation
- Rate of O₂ and CO₂ transfer through the respiratory membrane
- In normal lungs:
- All alveoli receive similar ventilation.
- All alveoli receive similar blood flow.
- In many lung diseases:
- Some alveoli are well ventilated but receive little or no blood flow.
- Other alveoli receive good blood flow but little or no ventilation.
- In these conditions:
- Gas exchange becomes seriously impaired.
- Severe respiratory distress can occur.
- This can happen even when:
- Total ventilation is normal.
- Total pulmonary blood flow is normal.
- The problem is that ventilation and blood flow are not matched in the same lung areas.
- To understand this imbalance, the ventilation-perfusion (V̇A/Q̇) ratio is used.
- Normal V̇A/Q̇ ratio:
- Alveolar ventilation (V̇A) is normal.
- Blood flow (Q̇) is normal.
- Therefore, the V̇A/Q̇ ratio is normal.
- When V̇A = 0 and Q̇ is present:
- Ventilation is absent.
- Blood flow is present.
- V̇A/Q̇ = 0
- When V̇A is present and Q̇ = 0:
- Ventilation is present.
- Blood flow is absent.
- V̇A/Q̇ = ∞ (infinity)
- At both extremes (V̇A/Q̇ = 0 or V̇A/Q̇ = ∞):
- Gas exchange does not occur in the affected alveoli.
KEY CONCEPT
- Efficient gas exchange requires both ventilation and blood flow. If either ventilation or perfusion is absent, the V̇A/Q̇ ratio becomes abnormal and gas exchange stops in those alveoli.
Ventilation-Perfusion (V/Q) Ratio – The Easiest Concept
Step 1: What is Ventilation (V)?
Ventilation = Air reaching the alveoli
Think of ventilation as oxygen delivery.
➡️ Air enters the alveolus.
➡️ Oxygen enters.
➡️ Carbon dioxide leaves.
Easy memory
V = Ventilation = Wind (Air)
Step 2: What is Perfusion (Q)?
Perfusion = Blood reaching the alveoli
Think of perfusion as blood delivery.
➡️ Blood comes to pick up oxygen.
➡️ Blood unloads CO₂.
Easy memory
Q = Blood Flow
Imagine an Alveolus as a Bus Stop
AIR (Ventilation)
↓
___________
| |
| Alveolus |
|___________|
↑
Blood (Perfusion)For gas exchange,
✅ Air must come.
AND
✅ Blood must come.
Both are required.
Example 1 — Normal Lung
Air arrives ✔
Blood arrives ✔
O2 → Blood
CO2 → AlveolusEverything works perfectly.
Normal V/Q.
Example 2 — Air Comes but Blood Doesn’t
Imagine
A bus stop is ready.
Passengers (oxygen) are waiting.
But…
No bus arrives.
Passengers 😐😐😐
No Bus ❌In lungs
Air ✔
Blood ❌Oxygen has nobody to enter.
CO₂ cannot arrive.
Gas exchange = Almost zero.
This is called
High V/Q
or
Dead Space
Examples
- Pulmonary embolism
- Blocked pulmonary artery
Remember
Air is present.
Blood is absent.
No exchange.
Example 3 — Blood Comes but Air Doesn’t
Now imagine
A bus arrives full of people.
But…
The station is closed.
Bus ✔
Passengers waiting
Station Closed ❌In lungs
Blood ✔
Air ❌Blood wants oxygen.
There is no oxygen.
Blood cannot unload CO₂.
Gas exchange = Almost zero.
This is called
Low V/Q
or
Shunt
Examples
- Airway obstruction
- Pneumonia
- Atelectasis
Remember
Blood is present.
Air is absent.
No exchange.
Why is it Called a Ratio?
The ratio compares
Ventilation
------------
Perfusionor
V
---
QIt simply asks:
“Is the amount of air matching the amount of blood?”
Three Situations
| Ventilation | Blood Flow | V/Q | Result |
|---|---|---|---|
| ✔ | ✔ | Normal | Excellent gas exchange |
| ✔ | ❌ | Very High (∞) | Dead space |
| ❌ | ✔ | Zero | Shunt |
Visual Memory Trick
Normal
Air ↓
[Alveolus]
Blood →O₂ enters blood.
CO₂ leaves blood.
Perfect exchange.
Dead Space (Pulmonary Embolism)
Air ↓
[Alveolus]
No Blood ❌Oxygen waits.
Nobody picks it up.
Shunt (Airway Block)
No Air ❌
[Alveolus]
Blood →Blood passes by.
No oxygen available.
Easy Real-Life Analogy
Imagine a restaurant.
- Food = Oxygen (Ventilation)
- Customers = Blood (Perfusion)
Normal Restaurant
Food ✔
Customers ✔
Everyone eats.
Too Much Food, No Customers
Food ✔✔✔
Customers ❌
Food is wasted.
➡️ High V/Q (Dead Space)
Customers, No Food
Customers ✔✔✔
Food ❌
Customers leave hungry.
➡️ Low V/Q (Shunt)Clinical Examples
Normal Lung
Pulmonary Embolism
A blood clot blocks the pulmonary artery.
Air ✔
Blood ❌➡️ High V/Q
➡️ Dead space
Pneumonia
Alveoli are filled with pus/fluid.
Blood ✔
Air ❌➡️ Low V/Q
➡️ ShuntAtelectasis
Collapsed alveoli.
Blood ✔
Air ❌➡️ Low V/Q
➡️ Shunt
One-Line Exam Trick
- Ventilation without perfusion = Dead Space (High V/Q or ∞)
- Perfusion without ventilation = Shunt (Low V/Q or 0)
SUPER MBBS MEMORY FORMULA
AIR + BLOOD = LIFEAIR only
↓
Dead Space
(V/Q = ∞)BLOOD only
↓
Shunt
(V/Q = 0)AIR + BLOOD
↓
Normal Gas ExchangeKEY CONCEPT
The V/Q ratio tells us whether air and blood are reaching the same alveolus at the same time. Gas exchange occurs only when both ventilation (air) and perfusion (blood) are present together. Too much air without blood causes dead space, while too much blood without air causes a shunt.
Alveolar Oxygen and Carbon Dioxide Partial Pressures When V̇A/Q̇ Equals Zero
- V̇A/Q̇ = 0 means:
- No alveolar ventilation (no air enters the alveolus).
- Blood flow is still present.
- Since no fresh air enters the alveolus:
- Oxygen (O₂) continues to move from the alveolus into the blood.
- Carbon dioxide (CO₂) continues to move from the blood into the alveolus.
- After some time:
- The gases in the alveolus become equal (equilibrate) with the gases in the blood flowing through the pulmonary capillaries.
- The blood reaching these capillaries is venous blood returning from the body’s tissues.
- Normal venous blood has:
- PO₂ = 40 mm Hg
- PCO₂ = 45 mm Hg
- Therefore, an alveolus with blood flow but no ventilation (V̇A/Q̇ = 0) will also have:
- Alveolar PO₂ = 40 mm Hg
- Alveolar PCO₂ = 45 mm Hg
Easy Concept
Imagine an alveolus as a closed classroom.
- Students (blood) keep entering and leaving.
- No fresh teacher (fresh air) comes into the classroom.
As time passes:
- The oxygen inside the classroom is used up.
- Carbon dioxide keeps building up.
- Eventually, the air inside the classroom becomes exactly like the air carried by the incoming venous blood.
Clinical Example
Airway Blockage (Mucus Plug)
Air ❌
[ Alveolus ]
Blood ✔- Fresh oxygen cannot enter.
- Blood continues flowing.
- Oxygen falls to 40 mm Hg.
- Carbon dioxide rises to 45 mm Hg.
- This alveolus cannot oxygenate the blood.
Examples:
- Atelectasis
- Pneumonia
- Complete airway obstruction
KEY CONCEPT
- When V̇A/Q̇ = 0, there is blood flow but no ventilation. The alveolar gases become the same as venous blood: PO₂ falls to 40 mm Hg and PCO₂ rises to 45 mm Hg because no fresh air enters the alveolus.
Gas Exchange and Alveolar Partial Pressures When V̇A/Q̇ Is Normal
- Normal V̇A/Q̇ means:
- Normal alveolar ventilation (air reaches the alveolus).
- Normal alveolar perfusion (blood reaches the alveolus).
- When both air and blood are present:
- Gas exchange through the respiratory membrane is almost optimal.
- Oxygen (O₂):
- Inspired air has a PO₂ of 149 mm Hg.
- Venous blood has a PO₂ of 40 mm Hg.
- After gas exchange, the alveolar PO₂ becomes 104 mm Hg.
- This value lies between inspired air and venous blood.
- Carbon dioxide (CO₂):
- Inspired air has a PCO₂ of 0 mm Hg.
- Venous blood has a PCO₂ of 45 mm Hg.
- After gas exchange, the alveolar PCO₂ becomes 40 mm Hg.
- This value lies between inspired air and venous blood.
- Therefore, under normal conditions:
- Alveolar PO₂ = 104 mm Hg
- Alveolar PCO₂ = 40 mm Hg
Easy Concept
Imagine an alveolus as a busy railway station.
- 🚆 Fresh air brings oxygen (O₂) into the station.
- 🚍 Blood arrives carrying carbon dioxide (CO₂).
At the station:
- Oxygen leaves the air and enters the blood.
- Carbon dioxide leaves the blood and enters the air.
Because both air and blood arrive in the correct amounts, gas exchange is highly efficient.
Easy Memory Comparison
| Source | PO₂ (mm Hg) | PCO₂ (mm Hg) |
|---|---|---|
| Inspired air | 149 | 0 |
| Normal alveolus | 104 | 40 |
| Venous blood | 40 | 45 |
Why is alveolar PO₂ not 149 mm Hg?
- Oxygen is continuously leaving the alveolus to enter the blood.
- Therefore, alveolar PO₂ falls from 149 → 104 mm Hg.
Why is alveolar PCO₂ not 0 mm Hg?
- Carbon dioxide is continuously entering the alveolus from the blood.
- Therefore, alveolar PCO₂ rises from 0 → 40 mm Hg.
Clinical Example
Healthy Person at Rest
Fresh Air ✔
↓
[ Alveolus ]
↑
Blood ✔- O₂ moves into the blood.
- CO₂ moves into the alveolus.
- Efficient gas exchange occurs.
Final alveolar values:
- PO₂ = 104 mm Hg
- PCO₂ = 40 mm Hg
KEY CONCEPT
- When the V̇A/Q̇ ratio is normal, ventilation and blood flow are well matched. This allows efficient gas exchange, producing a normal alveolar PO₂ of 104 mm Hg and a normal alveolar PCO₂ of 40 mm Hg.
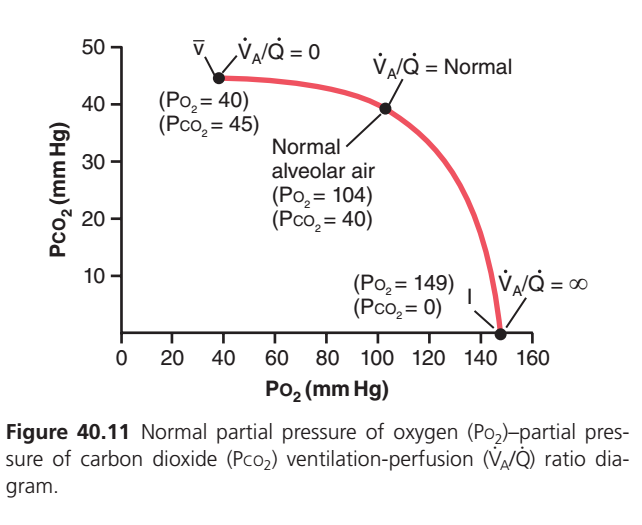
PO₂–PCO₂, V̇A/Q̇ Diagram
Fig. 40.11
- Fig. 40.11 is called the PO₂–PCO₂, V̇A/Q̇ diagram.
- It shows all possible combinations of PO₂ and PCO₂ at different V̇A/Q̇ ratios.
- The curve extends from:
- V̇A/Q̇ = 0
- To V̇A/Q̇ = ∞ (infinity)
- The diagram assumes:
- Normal venous blood gas values
- Breathing normal air at sea level
Point V (V̇A/Q̇ = 0)
- No ventilation
- Blood flow is present
- Alveolar gases become equal to venous blood.
- Values at Point V:
- PO₂ = 40 mm Hg
- PCO₂ = 45 mm Hg
Point I (V̇A/Q̇ = ∞)
- Ventilation is present
- No blood flow
- Alveolar air becomes the same as inspired air.
- Values at Point I:
- PO₂ = 149 mm Hg
- PCO₂ = 0 mm Hg
Normal Point (Normal V̇A/Q̇)
- Ventilation is normal
- Perfusion is normal
- Gas exchange is efficient.
- Normal alveolar values:
- PO₂ = 104 mm Hg
- PCO₂ = 40 mm Hg
Easy Concept
Think of the graph as a journey from no air to no blood.
Point V → No Air (V̇A/Q̇ = 0)
Air ❌
Blood ✔
PO₂ = 40
PCO₂ = 45The alveolus behaves like venous blood.
⬇️
Normal Point
Air ✔
Blood ✔
PO₂ = 104
PCO₂ = 40The alveolus has the best gas exchange.
⬇️
Point I → No Blood (V̇A/Q̇ = ∞)
Air ✔
Blood ❌
PO₂ = 149
PCO₂ = 0The alveolus behaves like inspired air.
Easy Memory Trick
| V̇A/Q̇ Ratio | Air | Blood | PO₂ (mm Hg) | PCO₂ (mm Hg) | Alveolus Resembles |
|---|---|---|---|---|---|
| 0 | ❌ | ✔ | 40 | 45 | Venous blood |
| Normal | ✔ | ✔ | 104 | 40 | Normal alveolar air |
| ∞ | ✔ | ❌ | 149 | 0 | Inspired air |
KEY CONCEPT
- The PO₂–PCO₂, V̇A/Q̇ diagram shows how alveolar gas composition changes as the ventilation-perfusion ratio changes. At V̇A/Q̇ = 0, alveolar air becomes like venous blood. At normal V̇A/Q̇, gas exchange is optimal. At V̇A/Q̇ = ∞, alveolar air becomes like inspired air.
This is Figure 40.11 from Guyton Physiology, one of the most important MBBS graphs because it combines oxygen (PO₂), carbon dioxide (PCO₂), alveolar ventilation (V̇A), and pulmonary blood flow/perfusion (Q̇) in a single diagram.
Many students memorize it, but once you understand the concept, the entire graph becomes very logical.
Figure 40.11: PO₂–PCO₂ Ventilation–Perfusion (V̇A/Q̇) Diagram
⭐ One-Line Concept
This graph shows how the oxygen (PO₂) and carbon dioxide (PCO₂) inside the alveoli change when the ventilation-perfusion ratio (V̇A/Q̇) changes.
- Low V̇A/Q̇ → Low PO₂, High PCO₂
- Normal V̇A/Q̇ → Normal PO₂ and PCO₂
- High V̇A/Q̇ → High PO₂, Low PCO₂
Step 1: Understand the Axes
X-Axis (Horizontal)
PO₂ (mmHg)
This represents alveolar oxygen partial pressure.
Moving to the right means:
➡️ More oxygen in the alveoli
Values:
- Left = Low oxygen
- Right = High oxygen
Y-Axis (Vertical)
PCO₂ (mmHg)
This represents alveolar carbon dioxide partial pressure.
Moving upward means:
⬆️ More CO₂
Moving downward means:
⬇️ Less CO₂
What Does the Red Curve Represent?
The red curve shows all possible combinations of alveolar PO₂ and PCO₂ for different V̇A/Q̇ ratios.
Every point on the curve corresponds to a different balance between:
- Ventilation (fresh air entering)
- Perfusion (blood flowing through pulmonary capillaries)
First Learn What V̇A/Q̇ Means
VA/Q=Pulmonary Blood FlowAlveolar Ventilation
Where:
- V̇A = Air reaching alveoli
- Q̇ = Blood reaching alveoli
Think of an alveolus:
Fresh Air (V̇A)
↓
[ Alveolus ]
↑↓ Gas exchange
Blood Flow (Q̇)Gas exchange depends on both air and blood.
Three Important Points on the Curve
The graph has three key points.
① Left Point → V̇A/Q̇ = 0
What Does It Mean?
Ventilation = 0
Blood flow = Normal
So:
Air = ❌ No
Blood = ✅ YesThis means:
Blood keeps arriving,
but
No fresh oxygen enters.
Examples
- Airway obstruction
- Mucus plug
- Severe asthma
- Atelectasis
What Happens?
Blood keeps taking oxygen.
Blood keeps delivering CO₂.
But there is no fresh air.
Eventually,
Alveolar gas becomes identical to mixed venous blood.
PO₂
Look at the graph.
PO₂
≈40 mmHg
Why?
Because mixed venous blood entering pulmonary capillaries has
PO₂
≈40 mmHg.
Without ventilation,
Alveolar oxygen falls to the same value.
PCO₂
≈45 mmHg
Why?
Mixed venous blood contains
PCO₂
≈45 mmHg.
Without ventilation,
CO₂ accumulates until alveolar PCO₂ also becomes
45 mmHg.Easy Memory
No ventilation
↓
Alveolus behaves like venous blood.
Therefore,
PO₂ = 40
PCO₂ = 45
Think of an Empty Classroom
Imagine a classroom with students (blood) entering continuously but no fresh air coming through the windows.
- Oxygen is used up.
- CO₂ accumulates.
Eventually, the room has low O₂ and high CO₂, just like mixed venous blood.
② Middle Point → Normal V̇A/Q̇
This is the normal operating point.
Here,
Ventilation and perfusion are perfectly matched.
Normal values:
| Variable | Value |
|---|---|
| PO₂ | ≈104 mmHg |
| PCO₂ | ≈40 mmHg |
This is normal alveolar air.
Why PO₂ Is Not 149 mmHg?
Fresh inspired air has a PO₂ of about 149 mmHg (after humidification).
However:
- Blood continuously removes oxygen.
- Therefore, alveolar PO₂ falls to about 104 mmHg.
Why PCO₂ Is 40 mmHg?
Blood continuously delivers CO₂.
Ventilation continuously removes it.
At equilibrium,
Alveolar PCO₂ stays around 40 mmHg.
Easy Memory
Normal breathing
Normal blood flow
=
PO₂ 104
PCO₂ 40③ Right Point → V̇A/Q̇ = ∞ (Infinity)
This is the most confusing point.
Let’s make it simple.
What Does Infinity Mean?
Ventilation = Present
Blood flow = 0
So:
Air = ✅ Yes
Blood = ❌ NoNo blood reaches the alveolus.
Examples:
- Pulmonary embolism
- Blocked pulmonary artery
What Happens?
Fresh air keeps entering.
But no blood removes oxygen.
Therefore,
PO₂ rises to the inspired air value.
PO₂
≈149 mmHg
Highest possible value.
PCO₂
≈0 mmHg
Why?
No blood arrives.
No CO₂ is delivered.
Fresh air washes away any residual CO₂.
Easy Memory
No blood
↓
No oxygen removal
↓
High PO₂
↓
No CO₂ delivery
↓
PCO₂ becomes almost zero.
Think of an Empty House
Imagine an empty house.
- Windows are open (ventilation).
- No people inside (no blood).
Since nobody is breathing:
- Oxygen stays high.
- CO₂ stays almost zero.
Exactly like V̇A/Q̇ = ∞.
Why Is the Curve Curved?
Notice:
The graph is not a straight line.
Why?
Because oxygen and carbon dioxide do not change at the same rate.
Initially,
A small reduction in ventilation causes a large fall in PO₂.
Later,
Changes become slower.
Similarly,
PCO₂ rises rapidly initially and then levels off.
This creates a smooth physiological curve.
Compare the Three Important Points
| V̇A/Q̇ Ratio | Ventilation | Perfusion | PO₂ | PCO₂ | Example |
|---|---|---|---|---|---|
| 0 | ❌ None | ✅ Normal | 40 mmHg | 45 mmHg | Airway obstruction, atelectasis |
| Normal (~0.8) | ✅ Normal | ✅ Normal | 104 mmHg | 40 mmHg | Healthy lung |
| ∞ | ✅ Normal | ❌ None | 149 mmHg | 0 mmHg | Pulmonary embolism |
Clinical Correlation
1. Airway Obstruction (Low V̇A/Q̇)
Examples:
- Asthma
- COPD
- Mucus plug
Air cannot reach alveoli.
Blood still flows.
Result:
- ↓ PO₂
- ↑ PCO₂
2. Pulmonary Embolism (High V̇A/Q̇)
Blood flow stops.
Air still reaches alveoli.
Result:
- ↑ PO₂
- ↓ PCO₂
This alveolus behaves like physiological dead space because it is ventilated but not perfused.
3. Normal Lung
Ventilation matches perfusion.
Efficient gas exchange occurs.
- PO₂ ≈104 mmHg
- PCO₂ ≈40 mmHg
The Big Concept to Remember
Think of the alveolus as a gas-exchange room:
- Ventilation (V̇A) = A fan bringing in fresh oxygen and removing CO₂.
- Perfusion (Q̇) = Workers (blood) entering the room, taking oxygen, and bringing CO₂.
Case 1: No fan, workers present (V̇A/Q̇ = 0)
- Workers use up oxygen.
- Workers release CO₂.
- Low PO₂ (40), high PCO₂ (45).
Case 2: Fan and workers balanced (Normal V̇A/Q̇)
- Oxygen supply matches demand.
- CO₂ removal matches production.
- PO₂ ≈104, PCO₂ ≈40.
Case 3: Fan running, no workers (V̇A/Q̇ = ∞)
- Oxygen is not consumed.
- CO₂ is not produced.
- PO₂ rises to inspired air (~149), PCO₂ falls to ~0.
Super Easy Memory Trick
Imagine an alveolus as a petrol station:
- 🚚 Trucks = Blood (Q̇) bring CO₂ and carry away O₂.
- 🌬️ Fresh air = Ventilation (V̇A) brings O₂ and removes CO₂.
- No fresh air (V̇A/Q̇ = 0): Trucks keep arriving, so oxygen runs out and CO₂ builds up → PO₂ 40, PCO₂ 45.
- Balanced air and trucks (Normal V̇A/Q̇): Efficient exchange → PO₂ 104, PCO₂ 40.
- Fresh air but no trucks (V̇A/Q̇ = ∞): Oxygen remains high because nobody takes it away, and CO₂ remains almost zero because nobody brings it → PO₂ 149, PCO₂ 0.
Final MBBS Golden Rule
| V̇A/Q̇ Ratio | PO₂ | PCO₂ | Key Idea |
|---|---|---|---|
| 0 | ↓ 40 mmHg | ↑ 45 mmHg | Perfusion without ventilation (Shunt-like state) |
| Normal (~0.8) | 104 mmHg | 40 mmHg | Efficient gas exchange |
| ∞ | ↑ 149 mmHg | ↓ 0 mmHg | Ventilation without perfusion (Dead space-like state) |
This single graph summarizes how ventilation-perfusion matching determines alveolar oxygen and carbon dioxide levels, making it one of the highest-yield concepts in respiratory physiology.
Concept of Physiological Shunt (When V̇A/Q̇ Is Below Normal)
- When V̇A/Q̇ is below normal, ventilation is not enough to supply the oxygen needed by the blood flowing through the alveolar capillaries.
- As a result, some venous blood passes through the lungs without becoming fully oxygenated.
- This blood is called shunted blood.
- In addition, about 2% of the cardiac output normally flows through the bronchial vessels instead of the alveolar capillaries.
- This blood also does not become oxygenated and is part of the shunted blood.
- The total amount of shunted blood per minute is called the physiological shunt.
- In pulmonary function laboratories, the physiological shunt is measured by:
- Measuring the oxygen concentration in mixed venous blood.
- Measuring the oxygen concentration in arterial blood.
- Measuring the cardiac output at the same time.
- The physiological shunt is calculated by:
Q˙TQ˙PS=CiO2−CvO2CiO2−CaO2
Easy Concept of the Equation
- Q̇PS = Physiological shunt blood flow
- Q̇T = Total cardiac output
- CiO₂ = Ideal oxygen concentration in arterial blood (with perfect V̇A/Q̇)
- CaO₂ = Measured oxygen concentration in arterial blood
- CvO₂ = Measured oxygen concentration in mixed venous blood
- If arterial oxygen (CaO₂) becomes much lower than the ideal oxygen level (CiO₂), the physiological shunt becomes larger.
- The greater the physiological shunt, the more blood passes through the lungs without being oxygenated.
KEY CONCEPT
- A physiological shunt occurs when ventilation is lower than perfusion (low V̇A/Q̇). As a result, some blood leaves the lungs without receiving enough oxygen. A larger physiological shunt means poorer oxygenation of the blood.
This equation is much easier if you understand what each oxygen concentration is measuring rather than trying to memorize the formula.
The physiological shunt equation is:Q˙TQ˙PS=CiO2−CvO2CiO2−CaO2
Step 1: What is the equation asking?
It is asking:
“What fraction of the total blood passed through the lungs without getting enough oxygen?”
So,
- Top (Q̇PS) = Shunted blood
- Bottom (Q̇T) = Total blood pumped by the heart
Therefore,Total BloodShunted Blood
= Percentage of blood that escaped oxygenation.
Step 2: Understand each oxygen concentration
Imagine 100 students take an oxygen exam.
CiO₂ = Ideal Score
Everyone studies perfectly.
Everyone gets
100/100This is the maximum oxygen content blood could have if every alveolus worked perfectly.
CaO₂ = Actual Score
Some alveoli are diseased.
Some blood is not oxygenated.
Actual score becomes
90/100This is the oxygen actually measured in arterial blood.CvO₂ = Starting Score
Before entering the lungs,
blood has already delivered oxygen to the tissues.
So it returns with less oxygen.
Example
60/100This is mixed venous blood.
Step 3: Now understand the numerator
CiO2−CaO2
This means
Ideal oxygen − Actual oxygen
Example
Ideal =100
Actual =90
Difference =10This 10 represents the oxygen lost because of shunting.
Think of it as
“How much oxygen did the lungs fail to add?”
Step 4: Understand the denominator
CiO2−CvO2
This means
Ideal oxygen − Venous oxygen
Example
Ideal =100
Venous =60
Difference =40This 40 is the maximum oxygen that could possibly be added by perfectly functioning lungs.
Think of it as
“What was the total oxygen-adding capacity?”
Step 5: Put them together
Example
| Oxygen Content | Value |
|---|---|
| CiO₂ | 100 |
| CaO₂ | 90 |
| CvO₂ | 60 |
Numerator
100 − 90 = 10Denominator
100 − 60 = 40ThereforeQTQPS=4010=0.25
Meaning
25%Twenty-five percent of the blood passed through the lungs without being properly oxygenated.
Step 6: Why does the equation work?
Imagine a factory.
Workers enter the factory to receive oxygen.
Perfect factory
100 workers enter
100 workers receive oxygenNo shunt.
Diseased factory
100 workers enter
Only 75 receive oxygen
25 leave without oxygenThose 25 workers represent the physiological shunt.
The equation simply calculates
How many workers (blood cells) left without receiving oxygen?
Super Easy Memory Trick
Think of the equation as:
Missing Oxygen
--------------------------
Maximum Oxygen Possibleor
Oxygen Lost
------------------
Oxygen That Could Be AddedOne-Line Interpretation
| If CaO₂ is… | Meaning |
|---|---|
| Close to CiO₂ | Very little shunt (normal lungs) |
| Much lower than CiO₂ | Large physiological shunt |
| Equal to CiO₂ | No shunt |
MBBS Exam Memory Formula
CiO₂
│
│ ← Ideal oxygen (Perfect lungs)
│
├───────────────
│ ↓
│ CaO₂
│ (Actual oxygen)
│
├───────────────
│ ↓
│ CvO₂
│ (Venous oxygen)- CiO₂ − CaO₂ = Oxygen missing because of shunting.
- CiO₂ − CvO₂ = Maximum oxygen the lungs could have added.
- Their ratio = Fraction of blood that was shunted.
FINAL KEY CONCEPT
- The numerator (CiO₂ − CaO₂) measures the oxygen the lungs failed to add.
- The denominator (CiO₂ − CvO₂) measures the maximum oxygen the lungs could have added.
- Their ratio gives the physiological shunt—the fraction of blood that passed through the lungs without being properly oxygenated.
Concept of Physiological Dead Space When V̇A/Q̇ Is Greater Than Normal
- When V̇A/Q̇ is greater than normal, ventilation is high but blood flow to some alveoli is low.
- These alveoli contain more oxygen than the blood can carry away.
- Therefore, part of the ventilation is wasted because little or no blood is available for gas exchange.
- Ventilation of the anatomical dead space (conducting airways) is also wasted.
- The total wasted ventilation is called the physiological dead space.
- In pulmonary function laboratories, physiological dead space is measured using the Bohr equation.
Bohr Equation
V˙TV˙Dphys=PaCO2PaCO2−PeCO2
Easy Concept of the Equation
- V̇Dphys = Physiological dead space
- V̇T = Tidal volume
- PaCO₂ = CO₂ partial pressure in arterial blood
- PeCO₂ = Average CO₂ partial pressure in expired air
Step-by-Step Understanding
- PaCO₂ represents the CO₂ level in blood that reaches ventilated alveoli.
- PeCO₂ represents the average CO₂ level in all expired air.
- If a large amount of expired air comes from dead space, it contains little or no CO₂.
- This lowers PeCO₂.
- Therefore:
- A bigger difference (PaCO₂ − PeCO₂) means more wasted ventilation (larger dead space).
- A smaller difference means less wasted ventilation (smaller dead space).
Simple Numerical Example
Suppose:
- PaCO₂ = 40 mm Hg
- PeCO₂ = 30 mm Hg
Then:V˙TV˙Dphys=4040−30=4010=0.25
Interpretation:
- 0.25 = 25%
- Twenty-five percent of the tidal volume is physiological dead space.
- Only 75% of the inspired air takes part in gas exchange.
- When physiological dead space becomes large:
- A large portion of ventilation is wasted.
- Much of the inspired air never reaches blood for gas exchange.
KEY CONCEPT
- Physiological dead space occurs when ventilation is greater than perfusion (high V̇A/Q̇). Air reaches the alveoli, but little blood is available, so ventilation is wasted. The Bohr equation calculates what fraction of the tidal volume is wasted as dead space.
Abnormalities of Ventilation-Perfusion Ratio
Abnormal V̇A/Q̇ in Upper and Lower Normal Lung
- In a healthy person standing upright:
- Pulmonary blood flow is lower in the upper lung than in the lower lung.
- Alveolar ventilation is also lower in the upper lung than in the lower lung.
- However, blood flow decreases more than ventilation in the upper lung.
- Therefore, in the upper part of the lung:
- V̇A/Q̇ is about 2.5 times higher than the ideal value.
- Ventilation is greater than perfusion.
- This produces a moderate physiological dead space.
- In the lower part of the lung:
- Blood flow is relatively greater than ventilation.
- V̇A/Q̇ is about 0.6 times the ideal value.
- Ventilation is slightly less than perfusion.
- A small amount of blood is not fully oxygenated.
- This produces a physiological shunt.
- Both the upper and lower lung have unequal ventilation and perfusion.
- This slightly reduces the lung’s efficiency in exchanging:
- O₂
- CO₂
- During exercise:
- Blood flow to the upper lung increases markedly.
- Physiological dead space decreases.
- Gas exchange becomes closer to optimal.
KEY CONCEPT
- In the upright lung, the upper lung has a high V̇A/Q̇ ratio (more ventilation than blood flow → physiological dead space), while the lower lung has a low V̇A/Q̇ ratio (more blood flow than ventilation → physiological shunt). During exercise, increased blood flow to the upper lung improves V̇A/Q̇ matching and gas exchange.
Abnormal V̇A/Q̇ in Chronic Obstructive Lung Disease
- People who smoke for many years often develop bronchial obstruction.
- In many people, the obstruction becomes severe enough to cause alveolar air trapping.
- Air trapping can lead to emphysema.
- In emphysema, many alveolar walls are destroyed.
- These changes produce two types of V̇A/Q̇ abnormalities:
- Obstructed bronchioles
- Air cannot reach the alveoli beyond the obstruction.
- These alveoli receive blood flow but little or no ventilation.
- V̇A/Q̇ approaches 0.
- This produces a physiological shunt.
- Destroyed alveolar walls (emphysema)
- Air still reaches these alveoli.
- However, destruction of the alveolar walls reduces the surrounding capillary blood flow.
- Ventilation is present, but blood flow is inadequate.
- Much of the ventilation is wasted.
- This produces a physiological dead space.
- Therefore, in chronic obstructive lung disease (COPD):
- Some lung areas develop physiological shunt.
- Other lung areas develop physiological dead space.
- Both abnormalities greatly reduce the lungs’ ability to exchange:
- O₂
- CO₂
- In severe cases, lung gas exchange may decrease to about one-tenth of normal.
- This condition is one of the most common causes of pulmonary disability.
Fig. 40.11
- Fig. 40.11 illustrates:
- V̇A/Q̇ = 0 → Physiological shunt (ventilation absent, blood flow present).
- Normal V̇A/Q̇ → Efficient gas exchange.
- V̇A/Q̇ = ∞ → Physiological dead space (ventilation present, blood flow absent).
KEY CONCEPT
- COPD causes both extremes of V̇A/Q̇ mismatch. Bronchial obstruction creates low V̇A/Q̇ (physiological shunt), while emphysema creates high V̇A/Q̇ (physiological dead space). Together, these severely impair gas exchange.