


- Phosphate excretion by the kidneys is controlled mainly by an overflow mechanism.
- The renal tubules have a normal transport maximum for phosphate reabsorption of about 0.1 mmol/min.
- When less than 0.1 mmol/min of phosphate is present in the glomerular filtrate, almost all filtered phosphate is reabsorbed.
- When more than 0.1 mmol/min of phosphate is present in the filtrate, the excess phosphate is excreted.
- Phosphate begins to appear in the urine when extracellular fluid phosphate concentration rises above about 0.8 mM/L.
- At this concentration, the tubular phosphate load is about 0.1 mmol/min.
- This assumes a GFR of 125 mL/min.
- Most people consume large amounts of phosphate in milk products and meat.
- Therefore, plasma phosphate concentration is usually maintained above 1 mM/L.
- At this level, phosphate is continuously excreted in the urine.
- The proximal tubule normally reabsorbs 75% to 80% of the filtered phosphate.
- The distal tubule reabsorbs about 10% of the filtered phosphate.
- Only small amounts of phosphate are reabsorbed in the loop of Henle.
- Only small amounts of phosphate are reabsorbed in the collecting tubules.
- Only small amounts of phosphate are reabsorbed in the collecting ducts.
- Approximately 10% of the filtered phosphate is excreted in the urine.
- In the proximal tubule, phosphate reabsorption occurs mainly through the transcellular pathway.
- Phosphate enters the cell from the tubular lumen through at least three sodium-phosphate co-transporters.
- This transport is driven by the inward sodium gradient.
- The sodium gradient is generated by the basolateral Na⁺-K⁺ ATPase pump.
- Phosphate exits the cell across the basolateral membrane.
- The mechanism of phosphate exit is not completely understood.
- It may involve a counter-transport mechanism.
- In this mechanism, phosphate is exchanged for an anion.
- Changes in phosphate reabsorptive capacity can influence phosphate excretion.
- A low-phosphate diet can increase the transport maximum for phosphate reabsorption over time.
- Increased transport maximum reduces the tendency of phosphate to spill into the urine.
- PTH plays an important role in regulating phosphate concentration.
- PTH promotes bone resorption.
- Bone resorption releases large amounts of phosphate into the extracellular fluid.
- PTH decreases the abundance of sodium-phosphate co-transporters in the apical membrane.
- Reduced sodium-phosphate co-transporter abundance decreases phosphate reabsorption by the renal tubules.
- Increased PTH decreases tubular phosphate reabsorption.
- Increased PTH causes more phosphate to be excreted in the urine.
KEY CONCEPT
- Renal phosphate excretion is controlled mainly by an overflow mechanism.
- Phosphate is excreted when the filtered load exceeds the tubular transport maximum.
- The proximal tubule reabsorbs most filtered phosphate.
- Phosphate reabsorption occurs mainly through sodium-phosphate co-transporters.
- PTH decreases phosphate reabsorption and increases phosphate excretion.
REGULATION OF RENAL MAGNESIUM EXCRETION AND EXTRACELLULAR MAGNESIUM ION CONCENTRATION
- More than half of the body’s magnesium is stored in the bones.
- Most of the remaining magnesium is located inside cells.
- Less than 1% of the body’s magnesium is located in the extracellular fluid.
- The total plasma magnesium concentration is about 1.8 mEq/L.
- More than half of the plasma magnesium is bound to plasma proteins.
- The free ionized magnesium concentration is about 0.8 mEq/L.
- The normal daily intake of magnesium is about 250 to 300 mg/day.
- Only about half of the ingested magnesium is absorbed by the gastrointestinal tract.
- To maintain magnesium balance, the kidneys must excrete the absorbed magnesium.
- The kidneys must excrete about 125 to 150 mg/day of magnesium.
- The kidneys normally excrete about 10% to 15% of the magnesium in the glomerular filtrate.
- Renal magnesium excretion can increase markedly during magnesium excess.
- Renal magnesium excretion can decrease to almost zero during magnesium depletion.
- Magnesium participates in many biochemical processes in the body.
- Magnesium is involved in the activation of many enzymes.
- Therefore, magnesium concentration must be closely regulated.
- Regulation of magnesium excretion occurs mainly by changing tubular reabsorption.
- The proximal tubule normally reabsorbs about 25% of the filtered magnesium.
- The thick ascending loop of Henle is the primary site of magnesium reabsorption.
- About 65% of the filtered magnesium load is reabsorbed in the thick ascending loop of Henle.
- Most magnesium reabsorption in the thick ascending loop of Henle occurs through the paracellular pathway.
- The driving force for paracellular magnesium reabsorption is the lumen-positive voltage in the thick ascending loop of Henle.
- Claudins play a critical role in paracellular magnesium reabsorption in the thick ascending loop of Henle.
- Only a small amount of filtered magnesium is reabsorbed in the distal and collecting tubules.
- Usually less than 5% of filtered magnesium is reabsorbed in these segments.
- Magnesium reabsorption in these segments occurs mainly through the transcellular pathway.
- Magnesium reabsorption in these segments occurs by active transport.
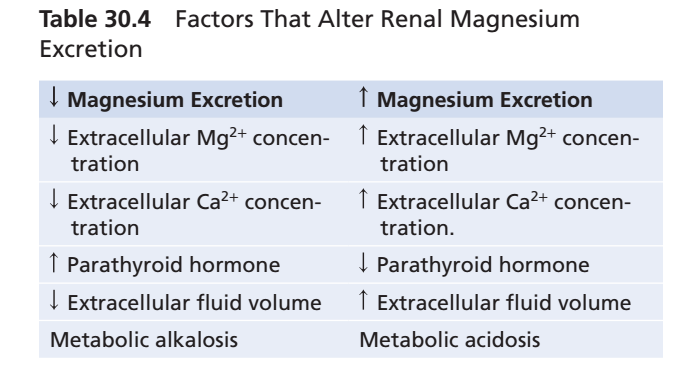
- Table 30.4 summarizes the major factors that influence renal magnesium excretion.
- Several factors that affect renal calcium excretion have similar effects on magnesium excretion.
KEY CONCEPT
- More than half of body magnesium is stored in bone.
- Only a small amount of magnesium is present in the extracellular fluid.
- Magnesium balance is maintained mainly by renal regulation of tubular reabsorption.
- The thick ascending loop of Henle is the major site of magnesium reabsorption.
- Most magnesium reabsorption occurs through the paracellular pathway.
- Many factors that regulate calcium excretion also regulate magnesium excretion.
SUMMARY
Regulation of Renal Phosphate Excretion
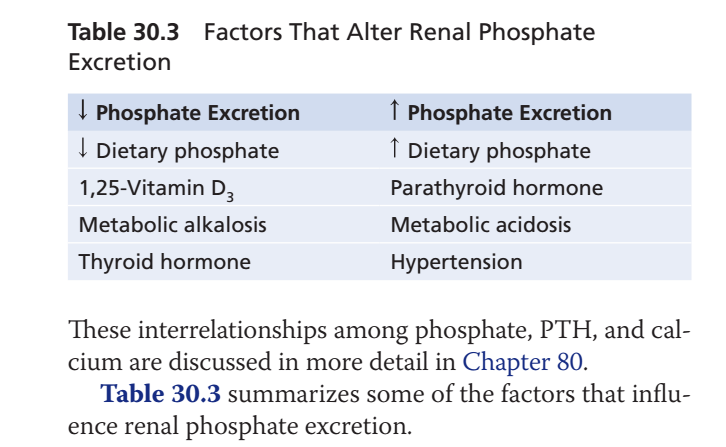
Phosphate is an essential component of bones, teeth, nucleic acids, ATP, and many intracellular metabolic reactions. Because phosphate plays important roles in energy metabolism and cellular function, its concentration in the extracellular fluid must be carefully regulated. The kidneys are the primary organs responsible for controlling phosphate balance, and renal phosphate excretion occurs mainly through an overflow mechanism.
The renal tubules have a limited capacity to reabsorb phosphate, known as the transport maximum (Tm), which is approximately 0.1 mmol/min. When the filtered phosphate load is less than this value, nearly all filtered phosphate is reabsorbed by the renal tubules, and very little appears in the urine. However, when the filtered phosphate load exceeds the transport maximum, the excess phosphate cannot be reabsorbed and is therefore excreted in the urine.
Phosphate begins to appear in the urine when the extracellular fluid phosphate concentration rises above approximately 0.8 mmol/L. At this concentration, assuming a normal glomerular filtration rate (GFR) of 125 mL/min, the filtered phosphate load reaches the tubular transport maximum. Since most individuals consume diets rich in phosphate-containing foods such as milk products and meat, plasma phosphate concentration is usually maintained above 1 mmol/L, resulting in continuous urinary phosphate excretion.
Most phosphate reabsorption occurs in the proximal tubule, where approximately 75% to 80% of the filtered phosphate load is reabsorbed. The distal tubule reabsorbs about 10%, while only small amounts are reabsorbed in the loop of Henle, collecting tubules, and collecting ducts. As a result, approximately 10% of the filtered phosphate load is normally excreted in the urine.
In the proximal tubule, phosphate reabsorption occurs primarily through the transcellular pathway. Phosphate enters the tubular epithelial cells through specialized sodium-phosphate co-transporters located on the luminal membrane. This process is driven by the inward sodium gradient established by the Na⁺-K⁺ ATPase pump on the basolateral membrane. After entering the cell, phosphate exits across the basolateral membrane and enters the interstitial fluid. Although the exact mechanism of phosphate exit is not fully understood, it may involve exchange with another anion through a counter-transport system.
The kidneys can adapt their phosphate reabsorptive capacity according to the body’s needs. For example, a low-phosphate diet increases the transport maximum for phosphate reabsorption, allowing the kidneys to conserve phosphate and reducing its urinary loss. This adaptation helps maintain phosphate balance during periods of dietary deficiency.
An important hormonal regulator of phosphate balance is parathyroid hormone (PTH). PTH promotes bone resorption, releasing both calcium and phosphate into the extracellular fluid. At the same time, PTH decreases the number of sodium-phosphate co-transporters in the apical membrane of proximal tubular cells. As a result, phosphate reabsorption decreases and urinary phosphate excretion increases. Thus, although PTH releases phosphate from bone, it simultaneously prevents excessive phosphate accumulation in the extracellular fluid by increasing renal phosphate loss.
Examples
Example 1: High-Phosphate Diet
A person consumes a diet rich in dairy products and meat. Plasma phosphate concentration rises, increasing the filtered phosphate load above the transport maximum. The excess phosphate cannot be reabsorbed and is excreted in the urine.
Example 2: Low-Phosphate Diet
A patient with poor dietary phosphate intake develops phosphate deficiency. Over time, the kidneys increase the transport maximum for phosphate reabsorption, reducing urinary phosphate loss and conserving phosphate.
Example 3: Hyperparathyroidism
Increased PTH secretion reduces the number of sodium-phosphate co-transporters in the proximal tubule. Consequently, phosphate reabsorption decreases and large amounts of phosphate are excreted in the urine.
Regulation of Renal Magnesium Excretion
Magnesium is the second most abundant intracellular cation and is essential for numerous biochemical reactions in the body. It participates in enzyme activation, ATP-dependent processes, protein synthesis, neuromuscular function, and cellular metabolism. Because magnesium is involved in so many physiological functions, its concentration must be closely regulated.
More than half of the body’s magnesium is stored in bones, while most of the remaining magnesium is located inside cells. Less than 1% of total body magnesium is found in the extracellular fluid. The total plasma magnesium concentration is approximately 1.8 mEq/L, and more than half of this magnesium is bound to plasma proteins. The free ionized magnesium concentration is about 0.8 mEq/L, which represents the physiologically active form.
The normal dietary intake of magnesium is approximately 250–300 mg/day. However, only about half of the ingested magnesium is absorbed by the gastrointestinal tract. Therefore, to maintain magnesium balance, the kidneys must excrete approximately 125–150 mg/day of magnesium. Under normal conditions, the kidneys excrete about 10–15% of the filtered magnesium load. During magnesium excess, urinary magnesium excretion can increase substantially, whereas during magnesium deficiency, renal magnesium excretion can decrease to almost zero.
Regulation of magnesium balance occurs primarily through changes in tubular reabsorption rather than filtration. The proximal tubule reabsorbs approximately 25% of the filtered magnesium load. However, the major site of magnesium reabsorption is the thick ascending limb of the loop of Henle, where approximately 65% of filtered magnesium is reabsorbed.
Most magnesium reabsorption in the thick ascending limb occurs through the paracellular pathway. Magnesium moves between tubular cells rather than through them. The driving force for this movement is the lumen-positive electrical potential present in the thick ascending limb. Specialized tight-junction proteins known as claudins play a critical role in regulating this paracellular transport.
Only small amounts of magnesium are reabsorbed in the distal tubules and collecting tubules. Typically, less than 5% of the filtered magnesium load is reabsorbed in these segments. Unlike the thick ascending limb, magnesium reabsorption here occurs mainly through the transcellular pathway and requires active transport mechanisms.
Many of the factors that influence calcium excretion also affect magnesium excretion. Therefore, changes in extracellular fluid volume, hormonal regulation, and tubular transport processes often alter both calcium and magnesium handling by the kidneys.
Examples
Example 1: Magnesium Deficiency
A patient with chronic gastrointestinal losses develops magnesium depletion. The kidneys respond by increasing magnesium reabsorption and reducing urinary magnesium excretion to nearly zero.
Example 2: Magnesium Excess
A patient receives excessive magnesium-containing antacids. Plasma magnesium concentration rises, causing the kidneys to increase urinary magnesium excretion and restore normal magnesium levels.
Example 3: Loop Diuretic Therapy
A patient taking a loop diuretic experiences reduced magnesium reabsorption in the thick ascending limb. As a result, urinary magnesium loss increases and hypomagnesemia may develop.
KEY CONCEPT
Renal phosphate excretion is regulated mainly by an overflow mechanism in which phosphate is excreted whenever the filtered load exceeds the tubular transport maximum. Most phosphate reabsorption occurs in the proximal tubule through sodium-phosphate co-transporters. Parathyroid hormone decreases phosphate reabsorption and increases urinary phosphate excretion.
Magnesium is an essential intracellular ion, with most body magnesium stored in bone and cells. The kidneys maintain magnesium balance primarily by adjusting tubular reabsorption. The thick ascending loop of Henle is the major site of magnesium reabsorption, where magnesium is reabsorbed mainly through the paracellular pathway driven by a lumen-positive voltage. Many of the same factors that regulate calcium excretion also influence magnesium excretion, allowing the kidneys to maintain normal magnesium homeostasis despite wide variations in intake.