


- The mechanisms regulating calcium ion concentration are discussed in detail in Chapter 80.
- The endocrinology of the calcium-regulating hormones is also discussed in Chapter 80.
- These hormones include parathyroid hormone (PTH) and calcitonin.
- Therefore, calcium ion regulation is discussed only briefly in this chapter.
- Extracellular fluid calcium ion concentration is normally maintained within a few percent of its normal value.
- The normal extracellular fluid calcium ion concentration is 2.4 mEq/L.
- When calcium ion concentration falls to low levels (hypocalcemia), excitability of nerve cells increases markedly.
- When calcium ion concentration falls to low levels (hypocalcemia), excitability of muscle cells increases markedly.
- Severe hypocalcemia can cause hypocalcemic tetany.
- Hypocalcemic tetany is characterized by spastic skeletal muscle contractions.
- Hypercalcemia is an increase in calcium concentration.
- Hypercalcemia depresses neuromuscular excitability.
- Hypercalcemia can lead to cardiac arrhythmias.
- About 50% of total plasma calcium exists in the ionized form.
- Ionized calcium is the biologically active form at cell membranes.
- About 40% of plasma calcium is bound to plasma proteins.
- About 10% of plasma calcium is complexed with anions such as phosphate and citrate.
- Changes in plasma hydrogen ion concentration influence calcium binding to plasma proteins.
- During acidosis, less calcium is bound to plasma proteins.
- During alkalosis, more calcium is bound to plasma proteins.
- Patients with alkalosis are more susceptible to hypocalcemic tetany.
Intestinal Calcium Absorption and Secretion Play a Major Role in Calcium Homeostasis
- Calcium intake must be balanced with net calcium loss over the long term.
- Unlike sodium and chloride, much of calcium excretion occurs in the feces.
- The usual dietary calcium intake is about 1000 mg/day.
- About 800 mg/day of calcium is excreted in the feces.
- Under certain conditions, fecal calcium excretion can exceed calcium intake.
- Calcium can also be secreted into the intestinal lumen.
- The gastrointestinal tract plays a major role in calcium homeostasis.
- Regulatory mechanisms controlling intestinal calcium absorption and secretion also play a major role in calcium homeostasis.
Most of the Body’s Calcium Is Stored in Bones and Regulated By Parathyroid Hormone (PTH)
- About 99% of the body’s calcium is stored in bones.
- About 0.1% of body calcium is present in the extracellular fluid.
- About 1.0% of body calcium is present in the intracellular fluid and cell organelles.
- Bone acts as a large reservoir for calcium.
- Bone serves as a source of calcium when extracellular fluid calcium concentration decreases.
- One of the most important regulators of bone calcium uptake and release is PTH.
- When extracellular fluid calcium concentration falls below normal, activity of calcium-sensing receptors (CSRs) on parathyroid gland cells decreases.
- Reduced CSR activity promotes increased PTH secretion.
- PTH acts directly on bones.
- PTH increases bone salt resorption.
- Bone salt resorption releases large amounts of calcium into the extracellular fluid.
- This returns calcium levels toward normal.
- When calcium ion concentration is elevated, CSR activity in parathyroid cells increases.
- Increased CSR activity reduces PTH secretion.
- With reduced PTH secretion, almost no bone resorption occurs.
- Excess calcium is deposited in the bones.
- Daily regulation of calcium ion concentration is mediated largely by the effects of PTH on bone resorption.
- Bones do not have an unlimited supply of calcium.
- Over the long term, calcium intake must be balanced with calcium excretion by the gastrointestinal tract and kidneys.
- PTH is the most important regulator of calcium at both sites.
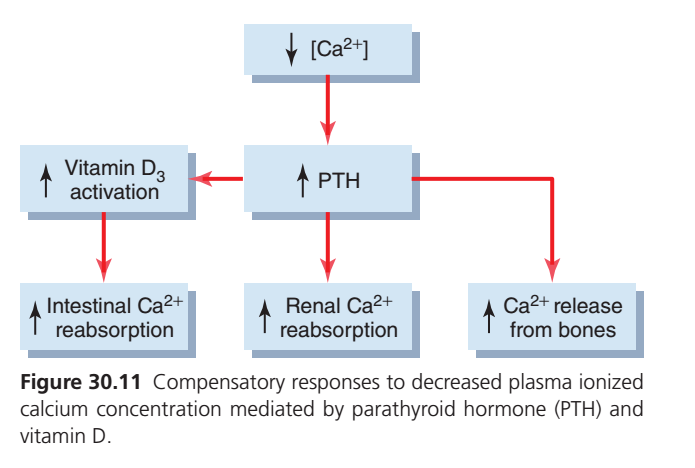
- PTH regulates plasma calcium concentration through three main effects.
- PTH stimulates bone resorption.
- PTH stimulates activation of vitamin D.
- Activated vitamin D increases intestinal calcium absorption.
- PTH increases renal tubular calcium reabsorption.
- Control of gastrointestinal calcium absorption and calcium exchange in bones is discussed in Chapter 80.
- The remainder of this section focuses on mechanisms controlling renal calcium excretion.
KEY CONCEPT
- Extracellular calcium concentration is tightly regulated around 2.4 mEq/L.
- Hypocalcemia increases neuromuscular excitability, while hypercalcemia decreases it.
- About 99% of body calcium is stored in bones.
- PTH is the major regulator of calcium homeostasis.
- PTH increases plasma calcium by:
- Stimulating bone resorption.
- Activating vitamin D to increase intestinal calcium absorption.
- Increasing renal tubular calcium reabsorption.
CONTROL OF CALCIUM EXCRETION BY THE KIDNEYS
- Calcium is filtered and reabsorbed in the kidneys.
- Calcium is not secreted by the kidneys.
- Renal calcium excretion equals filtered calcium minus reabsorbed calcium.
- About 50% of plasma calcium is ionized.
- About 40% of plasma calcium is bound to plasma proteins.
- About 10% of plasma calcium is complexed with anions such as phosphate.
- Only ionized calcium and calcium complexed with anions are filtered by the glomerular capillaries.
- About 60% of plasma calcium is filtered at the glomerulus.
- About 98% to 99% of filtered calcium is reabsorbed by the renal tubules.
- Only about 1% to 2% of filtered calcium is excreted.
- About 60% to 70% of filtered calcium is reabsorbed in the proximal tubule.
- About 20% to 25% of filtered calcium is reabsorbed in the loop of Henle.
- About 5% to 10% of filtered calcium is reabsorbed in the distal and collecting tubules.
- This pattern of calcium reabsorption is similar to that of sodium.
- Calcium excretion is adjusted according to the body’s needs.
- Increased calcium intake causes increased renal calcium excretion.
- Much of the increased calcium intake is eliminated in the feces.
- During calcium depletion, renal calcium excretion decreases.
- Reduced calcium excretion occurs because tubular calcium reabsorption increases.
Proximal Tubular Calcium Reabsorption
- At least 80% to 90% of calcium reabsorption in the proximal tubule occurs through the paracellular pathway.
- Calcium is dissolved in water.
- Calcium moves with the reabsorbed fluid between the cells.
- Only a small amount of proximal tubular calcium reabsorption occurs through the transcellular pathway.
- Calcium diffuses from the tubular lumen into the cell down an electrochemical gradient.
- Calcium concentration is much higher in the tubular lumen than in the epithelial cell cytoplasm.
- The interior of the cell has a negative charge relative to the tubular lumen.
- Calcium leaves the cell across the basolateral membrane.
- Calcium exits through a calcium-ATPase pump.
- Calcium also exits through a sodium-calcium counter-transporter.
Loop of Henle and Distal Tubule Calcium Reabsorption
- In the loop of Henle, calcium reabsorption occurs only in the thick ascending limb.
- Most calcium reabsorption in the thick ascending limb occurs through the paracellular pathway.
- Calcium moves by passive diffusion.
- Passive diffusion occurs because the tubular lumen has a slight positive charge relative to the interstitial fluid.
- Claudins are a family of tight-junction membrane proteins.
- Claudins regulate paracellular permeability of epithelial cells throughout the renal tubule.
- In the thick ascending loop of Henle, claudins play a critical role in paracellular calcium reabsorption.
- Claudins also help reabsorb magnesium.
- Claudins also help reabsorb sodium.
- Claudins are regulated by calcium-sensing receptors (CSRs).
- A small amount of calcium reabsorption in the thick ascending limb occurs through the transcellular pathway.
- This process is stimulated by PTH.
- In the distal tubule, calcium reabsorption occurs almost entirely through the transcellular pathway.
- Calcium reabsorption is coupled to active transport through the cell membrane.
- Calcium diffuses across the luminal membrane through calcium channels.
- Calcium exits across the basolateral membrane through a calcium-ATPase pump.
- Calcium also exits through a sodium-calcium counter-transport mechanism.
- PTH stimulates calcium reabsorption in the distal tubule.
- PTH also stimulates calcium reabsorption in the loops of Henle.
- Vitamin D (calcitriol) stimulates calcium reabsorption in the thick ascending limb of the loop of Henle.
- Vitamin D (calcitriol) stimulates calcium reabsorption in the distal tubule.
- Calcitonin stimulates calcium reabsorption in the thick ascending limb of the loop of Henle.
- Calcitonin stimulates calcium reabsorption in the distal tubule.
- PTH is quantitatively more important than vitamin D and calcitonin in reducing renal calcium excretion.
KEY CONCEPT
- Calcium is filtered and reabsorbed but not secreted by the kidneys.
- About 98% to 99% of filtered calcium is reabsorbed.
- Most proximal tubular calcium reabsorption occurs through the paracellular pathway.
- Calcium reabsorption in the distal tubule occurs mainly through the transcellular pathway.
- PTH is the most important hormone that increases renal calcium reabsorption and decreases calcium excretion.
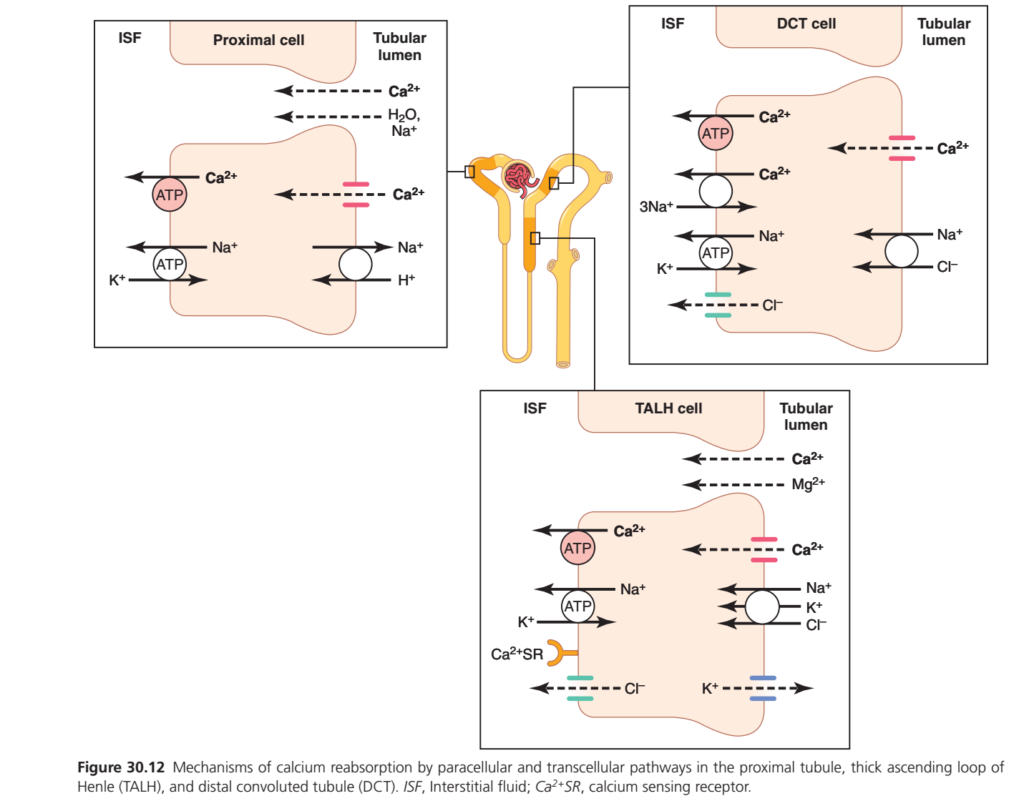
CALCIUM (Ca²⁺) REABSORPTION IN THE NEPHRON (Figure 30.12)
BIG PICTURE
This figure shows where and how calcium is reabsorbed in different parts of the nephron.
Three Major Sites
| Nephron Segment | Main % of Ca²⁺ Reabsorbed | Main Mechanism |
|---|---|---|
| Proximal Tubule (PT) | ~65% | Paracellular (between cells) |
| Thick Ascending Loop of Henle (TALH) | ~25% | Mostly Paracellular |
| Distal Convoluted Tubule (DCT) | ~8% | Transcellular (through cells) |
Easy Memory
65 → 25 → 8 Rule
PT = 65%
TALH = 25%
DCT = 8%
1. PROXIMAL TUBULE (PT)
Main Idea
Most calcium follows sodium and water.
What Happens?
As the proximal tubule reabsorbs:
- Na⁺
- Water
Calcium is dragged along with them.
Route
➡️ Calcium mainly moves between cells
(paracellular pathway)
Not through the cell itself.
Easy Concept
Imagine people leaving a stadium.
Sodium and water leave first
Calcium simply follows the crowd through side gaps.
No special transporter is needed.
What Drives Calcium Reabsorption Here?
Water Reabsorption
⬇️
Calcium becomes concentrated in tubular fluid
⬇️
Calcium moves into blood
and
Sodium Reabsorption
⬇️
Creates favorable forces
⬇️
Calcium follows
Memory Trick
PT = “Calcium follows Na⁺ and Water”
2. THICK ASCENDING LOOP OF HENLE (TALH)
Main Idea
This segment creates a positive lumen charge that pushes calcium into blood.
Important Transporter
NKCC2 Cotransporter
Moves:
- Na⁺
- K⁺
- 2Cl⁻
from lumen into cell.
What Happens Next?
Some K⁺ leaks back into the lumen.
This creates:
Positive Charge in Tubular Lumen
Result
Positive lumen repels positive ions:
- Ca²⁺
- Mg²⁺
and pushes them:
From Tubule → Blood
through spaces between cells.
Easy Concept
Imagine the lumen becoming crowded with positive charges.
The extra positive charge pushes calcium out of the tubule.
Memory Trick
TALH = “Positive lumen pushes Ca²⁺ and Mg²⁺ out”
Role of Calcium-Sensing Receptor (CaSR)
Look at the receptor shown in the TALH cell.
When Blood Calcium Becomes High
CaSR is activated.
Effects
- Decreases NKCC2 activity
- Decreases K⁺ recycling
⬇️
Less positive lumen potential
⬇️
Less Ca²⁺ reabsorption
⬇️
More Ca²⁺ excreted in urine
Easy Memory
High Ca²⁺ → CaSR ON → Less Ca²⁺ Reabsorption
3. DISTAL CONVOLUTED TUBULE (DCT)
Main Idea
This is the major regulatory site for calcium reabsorption.
Unlike PT and TALH:
Calcium moves THROUGH the cell
(transcellular transport)
Step 1: Calcium Enters Cell
From tubular lumen:
Through Calcium Channels
Ca²⁺ enters the DCT cell.
Step 2: Calcium Leaves Cell
On the blood side:
Ca²⁺ ATPase Pump
Pumps calcium into blood.
and
Na⁺–Ca²⁺ Exchanger
Moves:
- Na⁺ into cell
- Ca²⁺ out to blood
Result
Calcium is reabsorbed into circulation.
Easy Concept
Think of DCT as a VIP checkpoint.
Calcium cannot sneak between cells.
It must:
Enter the cell
⬇️
Cross the cell
⬇️
Exit into blood
Why Is DCT So Important?
Because hormones control calcium here.
Parathyroid Hormone (PTH)
Increases:
- Calcium channel activity
- Calcium transport
⬇️
More Ca²⁺ reabsorbed
⬇️
Less Ca²⁺ lost in urine
Memory Trick
DCT = “Hormonal control center for calcium”
COMPARISON OF THE THREE SEGMENTS
| Feature | PT | TALH | DCT |
|---|---|---|---|
| Main Ca²⁺ Reabsorption | Highest | Moderate | Small but regulated |
| Pathway | Between cells | Between cells | Through cells |
| Driven By | Na⁺ & Water | Positive lumen voltage | Ca²⁺ channels & pumps |
| Regulation | Minimal | Moderate | Major |
| Hormone Control | Little | Little | Strong (PTH) |
THE WHOLE STORY IN ONE FLOWCHART
Filtered Ca²⁺
↓
Proximal Tubule
(65% reabsorbed)
Ca²⁺ follows Na⁺ and Water
↓
Thick Ascending Loop
(25% reabsorbed)
Positive lumen pushes Ca²⁺ out
↓
Distal Convoluted Tubule
(8% reabsorbed)
Ca²⁺ enters cell → exits to blood
(PTH regulated)
↓
Very little Ca²⁺ appears in urineHIGH-YIELD EXAM PEARLS
✅ 65% of filtered calcium is reabsorbed in the proximal tubule.
✅ Calcium reabsorption in PT occurs mainly by the paracellular pathway.
✅ 25% is reabsorbed in the thick ascending loop of Henle.
✅ Positive lumen voltage in TALH drives Ca²⁺ and Mg²⁺ reabsorption.
✅ CaSR activation decreases calcium reabsorption in TALH.
✅ Distal convoluted tubule is the major regulatory site for calcium handling.
✅ Calcium reabsorption in DCT occurs by the transcellular pathway.
✅ PTH increases calcium reabsorption in DCT and decreases urinary calcium loss.
KEY CONCEPT
Proximal Tubule = Calcium follows Na⁺ and water.
TALH = Positive lumen pushes Ca²⁺ and Mg²⁺ into blood.
DCT = Hormone-controlled calcium transport through the cell (especially by PTH).
Memory Formula
PT (65%) → TALH (25%) → DCT (8%)
Follow → Push → Pump ✔️
Regulation of Tubular Calcium Reabsorption
- One of the primary regulators of renal tubular calcium reabsorption is PTH.
- Increased PTH levels stimulate calcium reabsorption in the thick ascending loops of Henle.
- Increased PTH levels stimulate calcium reabsorption in the distal tubules.
- Increased calcium reabsorption reduces urinary calcium excretion.
- Reduced PTH levels promote calcium excretion.
- Reduced PTH levels decrease calcium reabsorption in the loops of Henle.
- Reduced PTH levels decrease calcium reabsorption in the distal tubules.
- Increased extracellular fluid calcium ion concentration directly stimulates calcium-sensing receptors (CSRs).
- Activation of CSRs inhibits calcium reabsorption in the thick ascending loops of Henle.
- Reduced calcium concentration decreases CSR activity.
- Reduced CSR activity increases calcium reabsorption in the thick ascending loop of Henle.
- In the proximal tubule, calcium reabsorption usually parallels sodium reabsorption.
- In the proximal tubule, calcium reabsorption usually parallels water reabsorption.
- Proximal tubular calcium reabsorption is independent of PTH.
- Extracellular volume expansion decreases proximal sodium and water reabsorption.
- Increased arterial pressure decreases proximal sodium and water reabsorption.
- Reduced sodium and water reabsorption also reduces calcium reabsorption.
- Reduced calcium reabsorption increases urinary calcium excretion.
- Reduced extracellular volume increases proximal tubular calcium reabsorption.
- Decreased blood pressure increases proximal tubular calcium reabsorption.
- Increased proximal tubular calcium reabsorption decreases calcium excretion.
- Plasma phosphate concentration also influences calcium reabsorption.
- Increased plasma phosphate concentration tends to reduce ionized calcium concentration.
- Reduced ionized calcium concentration stimulates PTH secretion.
- Increased PTH secretion increases calcium reabsorption by the renal tubules.
- Increased calcium reabsorption reduces calcium excretion.
- The opposite effects occur when plasma phosphate concentration decreases.
- Calcium reabsorption is inhibited by metabolic acidosis.
- Calcium reabsorption is stimulated by metabolic alkalosis.
- Acidosis tends to increase calcium excretion.
- Alkalosis tends to reduce calcium excretion.
- Most of the effect of increased hydrogen ion concentration on calcium excretion results from inhibition of active calcium reabsorption in the distal tubule.
- Table 30.2 summarizes the major factors that influence calcium excretion.
KEY CONCEPT
- PTH is a major regulator of renal calcium reabsorption.
- Increased PTH increases calcium reabsorption and decreases calcium excretion.
- Increased extracellular calcium activates CSRs and decreases calcium reabsorption.
- Proximal tubular calcium reabsorption follows sodium and water reabsorption.
- Increased phosphate stimulates PTH and increases calcium reabsorption.
- Acidosis increases calcium excretion, whereas alkalosis decreases calcium excretion.
SUMMARY
Regulation of Renal Calcium Excretion and Extracellular Calcium Ion Concentration
Calcium is an essential mineral that plays a critical role in many physiological functions, including muscle contraction, nerve impulse transmission, blood clotting, and maintenance of normal cardiac rhythm. Because of these important functions, the concentration of calcium ions in the extracellular fluid is maintained within a very narrow range. Even small deviations from the normal calcium level can produce significant clinical consequences. When calcium concentration falls below normal (hypocalcemia), nerve and muscle cells become highly excitable, which may lead to muscle spasms and hypocalcemic tetany. In contrast, when calcium concentration rises above normal (hypercalcemia), neuromuscular activity is depressed and cardiac arrhythmias may occur.
In plasma, calcium exists in three forms. Approximately 50% is present as ionized calcium, which is the biologically active form responsible for physiological effects at cell membranes. About 40% is bound to plasma proteins, while the remaining 10% is complexed with anions such as phosphate and citrate. Changes in blood pH influence the amount of calcium bound to proteins. During acidosis, less calcium binds to proteins, resulting in increased ionized calcium levels. During alkalosis, more calcium binds to proteins, reducing the concentration of ionized calcium and increasing the risk of tetany.
Maintenance of calcium balance depends on the coordinated actions of the intestines, bones, kidneys, and hormones. The gastrointestinal tract plays a major role in calcium homeostasis because calcium intake must be balanced with calcium loss. An average person consumes approximately 1000 mg of calcium daily, and a large portion is excreted in the feces. Calcium absorption from the intestine is strongly influenced by vitamin D and other regulatory mechanisms.
The largest reservoir of calcium in the body is the skeleton. Approximately 99% of total body calcium is stored in bones, while only a very small fraction is found in the extracellular and intracellular fluids. Bones serve as a storage site from which calcium can be released when plasma calcium concentration decreases. The most important hormone regulating this process is parathyroid hormone (PTH). When extracellular calcium concentration falls, calcium-sensing receptors in the parathyroid glands detect the decrease and stimulate the secretion of PTH. This hormone restores plasma calcium levels through three major mechanisms. First, it increases bone resorption, releasing calcium from bone into the bloodstream. Second, it stimulates activation of vitamin D, which enhances intestinal absorption of calcium. Third, it increases calcium reabsorption by the kidneys, thereby reducing urinary calcium loss. When plasma calcium concentration rises, PTH secretion decreases, bone resorption is suppressed, and excess calcium is deposited in bone.
The kidneys play a crucial role in regulating calcium excretion. Calcium is filtered at the glomerulus and reabsorbed by the renal tubules, but it is not secreted. Therefore, renal calcium excretion depends on the difference between the amount filtered and the amount reabsorbed. Since only ionized and complexed calcium can pass through the glomerular membrane, approximately 60% of plasma calcium is filtered. Of this filtered load, about 98–99% is reabsorbed, and only 1–2% is ultimately excreted in the urine.
Calcium reabsorption occurs throughout several segments of the nephron. Approximately 60–70% of filtered calcium is reabsorbed in the proximal tubule. Most of this occurs through the paracellular pathway, where calcium moves passively between tubular cells along with water and sodium. A smaller amount is reabsorbed through the transcellular pathway by diffusion into tubular cells followed by active transport across the basolateral membrane.
A further 20–25% of filtered calcium is reabsorbed in the thick ascending limb of the loop of Henle. In this segment, calcium moves primarily through the paracellular pathway due to the positive electrical charge within the tubular lumen. Specialized proteins known as claudins regulate this movement. A smaller portion is reabsorbed actively through tubular cells, a process that is stimulated by PTH.
The distal tubule and collecting tubule reabsorb approximately 5–10% of filtered calcium. Unlike the proximal tubule, calcium reabsorption in these segments occurs almost entirely through active transcellular transport. Calcium enters the tubular cells through calcium channels and leaves through calcium-ATPase pumps and sodium-calcium exchangers. This portion of calcium reabsorption is highly regulated and responds strongly to hormonal control, particularly by PTH. Vitamin D and calcitonin can also enhance calcium reabsorption, although their effects are less important than those of PTH.
Several factors influence renal calcium reabsorption. The most important is PTH, which increases calcium reabsorption in the thick ascending limb and distal tubule, thereby reducing urinary calcium excretion. Extracellular calcium concentration itself also plays a regulatory role. High calcium levels activate calcium-sensing receptors, which inhibit calcium reabsorption and promote calcium excretion. Conversely, low calcium levels reduce receptor activity and enhance calcium conservation by the kidneys.
Changes in extracellular fluid volume and blood pressure also affect calcium handling. Because calcium reabsorption in the proximal tubule parallels sodium and water reabsorption, expansion of extracellular fluid volume decreases calcium reabsorption and increases urinary calcium loss. In contrast, volume depletion enhances proximal tubular reabsorption of sodium, water, and calcium, reducing calcium excretion. Plasma phosphate concentration is another important regulator. Increased phosphate levels lower ionized calcium concentration, stimulate PTH secretion, and increase renal calcium reabsorption. Decreased phosphate levels produce the opposite effect. Acid-base balance also influences calcium handling. Metabolic acidosis decreases calcium reabsorption, particularly in the distal tubule, resulting in increased urinary calcium excretion. Metabolic alkalosis has the opposite effect and promotes calcium retention.
Examples
Example 1: Vitamin D Deficiency
A patient with vitamin D deficiency absorbs less calcium from the intestine. Plasma calcium concentration falls, stimulating PTH secretion. PTH then increases bone resorption and renal calcium reabsorption to restore calcium levels toward normal.
Example 2: Hypercalcemia Due to Excess Calcium Intake
A person taking excessive calcium supplements develops elevated plasma calcium levels. Increased calcium activates calcium-sensing receptors, suppresses PTH secretion, reduces bone resorption, and increases urinary calcium excretion.
Example 3: Metabolic Acidosis
A patient with diabetic ketoacidosis develops metabolic acidosis. Calcium reabsorption in the distal tubule decreases, causing increased urinary calcium loss and potentially contributing to a negative calcium balance.
KEY CONCEPT
Calcium homeostasis is maintained through the integrated actions of the intestines, bones, kidneys, vitamin D, and parathyroid hormone. The kidneys filter calcium and reabsorb nearly all of it, with only a small fraction being excreted. PTH is the most important regulator of renal calcium handling because it increases calcium reabsorption, stimulates vitamin D activation, and promotes calcium release from bone. Factors such as extracellular calcium concentration, phosphate levels, extracellular fluid volume, blood pressure, and acid-base status also influence renal calcium excretion. Together, these mechanisms ensure that extracellular calcium concentration remains within a narrow range necessary for normal neuromuscular and cardiovascular function.