


- Extracellular fluid volume is determined mainly by the balance between water and salt intake and output.
- In many cases, salt and fluid intake are determined by personal habits.
- Salt and fluid intake are often not controlled by physiological mechanisms.
- Therefore, regulation of extracellular fluid volume is largely the responsibility of the kidneys.
- The kidneys must adjust salt and water excretion to match intake under steady-state conditions.
- Regulation of extracellular fluid volume mainly depends on controlling the amount of sodium chloride in the extracellular fluid.
- Changes in extracellular fluid sodium chloride content usually cause parallel changes in extracellular fluid volume.
- This occurs when the antidiuretic hormone (ADH)-thirst mechanisms are functioning normally.
- When ADH-thirst mechanisms function normally, changes in extracellular fluid sodium chloride content are accompanied by similar changes in extracellular water.
- This helps maintain relatively constant osmolality.
- This also helps maintain relatively constant sodium concentration.
Sodium Intake and Excretion Are Balanced Under Steady-State Conditions
- Under steady-state conditions, sodium excretion by the kidneys is determined mainly by sodium intake.
- This principle also applies to most electrolytes.
- Over the long term, the kidneys must excrete almost exactly the amount of sodium that is ingested.
- Balance between sodium intake and sodium output is necessary for life.
- Even when kidney function is disturbed, sodium balance is usually restored within a few days.
- This occurs if the kidney disturbance is not too severe.
- When kidney disturbances are mild, sodium balance can be restored mainly through intrarenal adjustments.
- These adjustments may occur with only minimal changes in extracellular fluid volume.
- These adjustments may occur with only minimal systemic changes.
- When kidney disturbances are severe, intrarenal compensatory mechanisms may become exhausted.
- In these situations, systemic adjustments are activated.
- These adjustments may include changes in blood pressure.
- These adjustments may include changes in circulating hormone levels.
- These adjustments may include changes in sympathetic nervous system activity.
- Systemic adjustments may have harmful long-term effects.
- Impaired kidney function may increase blood pressure.
- Increased blood pressure helps maintain normal sodium excretion.
- Over time, high blood pressure may damage blood vessels.
- Over time, high blood pressure may damage the heart.
- Over time, high blood pressure may damage other organs.
- These compensatory responses are necessary.
- Persistent imbalance between fluid and electrolyte intake and excretion would rapidly cause fluid accumulation or fluid loss.
- Persistent imbalance would also cause electrolyte accumulation or electrolyte loss.
- Severe cardiovascular consequences could develop within a few days.
- Systemic adjustments occur in response to abnormal kidney function.
- These adjustments help restore balance between electrolyte intake and excretion.
- These adjustments help restore balance between fluid intake and excretion.
- These adjustments represent a necessary trade-off.
KEY CONCEPT
- Extracellular fluid volume depends mainly on the balance between salt and water intake and output.
- The kidneys adjust sodium and water excretion to match intake.
- Under steady-state conditions, sodium excretion equals sodium intake.
- Mild kidney disturbances are corrected mainly by intrarenal adjustments.
- Severe kidney disturbances require systemic compensations such as changes in blood pressure, hormones, and sympathetic activity.
- These compensations help maintain fluid and electrolyte balance despite potential long-term consequences.
Sodium Excretion Is Controlled By Altering Glomerular Filtration or Tubular Sodium Reabsorption Rates
- Sodium and water excretion are determined by two variables.
- These variables are glomerular filtration rate (GFR) and tubular reabsorption rate.
- Excretion = Glomerular filtration − Tubular reabsorption.
- The average GFR is about 180 L/day.
- Tubular reabsorption averages about 178.5 L/day.
- Urine excretion averages about 1.5 L/day.
- Small changes in GFR can cause large changes in renal excretion.
- Small changes in tubular reabsorption can also cause large changes in renal excretion.
- A 5% increase in GFR increases GFR to about 189 L/day.
- Without tubular compensation, this would increase urine volume by about 9 L/day.
- Such an increase would rapidly cause catastrophic changes in body fluid volume.
- Small changes in tubular reabsorption can also cause major changes in urine volume.
- Small changes in tubular reabsorption can also cause major changes in sodium excretion.
- These effects occur if compensatory changes in GFR do not occur.
- Tubular reabsorption and GFR are usually regulated in parallel.
- This allows renal excretion to match water intake accurately.
- This allows renal excretion to match electrolyte intake accurately.
- Disturbances that alter GFR or tubular reabsorption are buffered by intrarenal mechanisms.
- These mechanisms help minimize changes in urinary excretion.
- Renal vasodilation can greatly increase GFR.
- Renal vasodilation may occur with certain drugs.
- Renal vasodilation may occur during high fever.
- Increased GFR increases sodium chloride delivery to the tubules.
- Increased sodium chloride delivery activates glomerulotubular balance mechanisms.
- These mechanisms increase tubular reabsorption of much of the additional filtered sodium chloride.
- Increased sodium chloride delivery also activates macula densa feedback.
- Increased sodium chloride delivery to the distal tubule causes afferent arteriolar constriction.
- Afferent arteriolar constriction returns GFR toward normal.
- Abnormalities in proximal tubular reabsorption are partially compensated by these intrarenal feedback mechanisms.
- Abnormalities in loop of Henle reabsorption are also partially compensated by these intrarenal feedback mechanisms.
- Glomerulotubular balance and macula densa feedback do not completely restore distal sodium chloride delivery to normal.
- Changes in GFR can still cause significant changes in sodium excretion.
- Changes in GFR can still cause significant changes in water excretion.
- Changes in tubular reabsorption can still cause significant changes in sodium excretion.
- Changes in tubular reabsorption can still cause significant changes in water excretion.
- Additional feedback mechanisms may be activated when these changes occur.
- These mechanisms include changes in blood pressure.
- These mechanisms include changes in hormone levels.
- These feedback mechanisms eventually return sodium excretion to equal sodium intake.
- Sodium and water balance are controlled by multiple interacting mechanisms.
- These mechanisms also help regulate extracellular fluid volume.
- All of these feedback mechanisms control sodium and water excretion by altering GFR or tubular reabsorption.
KEY CONCEPT
- Renal sodium and water excretion depend on GFR and tubular reabsorption.
- Small changes in either process can cause large changes in excretion.
- Intrarenal mechanisms such as glomerulotubular balance and macula densa feedback help minimize these changes.
- Additional systemic mechanisms, including blood pressure and hormonal changes, restore sodium excretion to match sodium intake.
- Regulation of GFR and tubular reabsorption is essential for controlling extracellular fluid volume.
Importance of Pressure Natriuresis and Pressure Diuresis in Maintaining Body Sodium and Fluid Balance
- Pressure natriuresis and pressure diuresis are among the most important mechanisms for maintaining sodium and fluid balance.
- These mechanisms help control blood volume.
- These mechanisms help control extracellular fluid volume.
- Pressure natriuresis refers to the effect of blood pressure on sodium excretion.
- Pressure diuresis refers to the effect of blood pressure on water excretion.
- These mechanisms also play a dominant role in long-term blood pressure regulation.
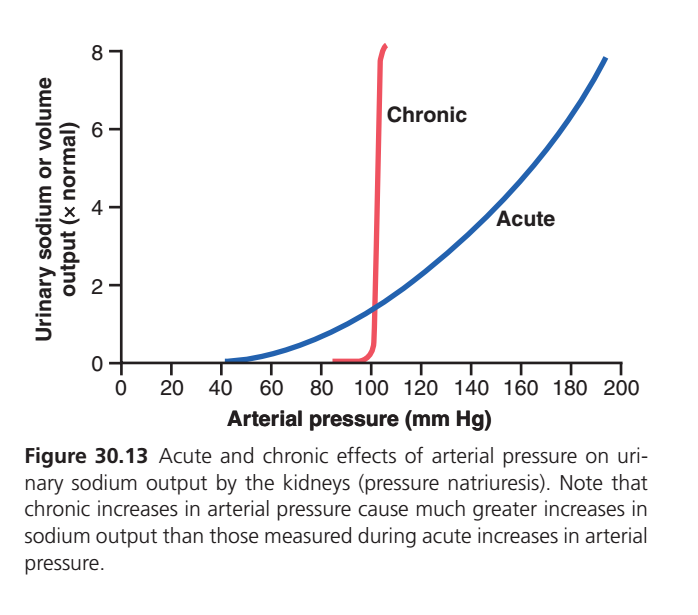
- Acute increases in arterial pressure increase urinary sodium output.
- An acute increase in arterial pressure of 30 to 50 mm Hg causes a 2-fold to 3-fold increase in urinary sodium output.
- Pressure natriuresis occurs independently of changes in sympathetic nervous system activity.
- Pressure natriuresis occurs independently of changes in various hormones.
- Pressure natriuresis can be demonstrated in an isolated kidney.
- An isolated kidney can exhibit pressure natriuresis even when removed from the influence of these factors.
- Chronic increases in blood pressure greatly enhance the effectiveness of pressure natriuresis.
- Increased blood pressure suppresses renin release after a short delay.
- Reduced renin release decreases the formation of angiotensin II (Ang II).
- Reduced renin release also decreases aldosterone formation.
- Decreased levels of Ang II inhibit renal tubular sodium reabsorption.
- Decreased levels of aldosterone inhibit renal tubular sodium reabsorption.
- Reduced sodium reabsorption increases sodium excretion.
- Reduced sodium reabsorption increases water excretion.
- The reduction in Ang II and aldosterone amplifies the direct effects of increased blood pressure.
- Increased blood pressure directly increases sodium excretion.
- Increased blood pressure directly increases water excretion.
KEY CONCEPT
- Pressure natriuresis = increased blood pressure → increased sodium excretion.
- Pressure diuresis = increased blood pressure → increased water excretion.
- Acute increases in blood pressure increase urinary sodium output.
- Chronic increases in blood pressure produce an even greater natriuretic effect.
- Chronic pressure natriuresis is enhanced by decreased renin, Ang II, and aldosterone levels.
- Pressure natriuresis and pressure diuresis are essential for maintaining sodium balance, fluid balance, blood volume, and extracellular fluid volume.
PRESSURE NATRIURESIS CURVE (Figure 30.13)
WHAT IS THIS GRAPH SHOWING?
This graph explains:
When Arterial Blood Pressure Increases
⬇️
Kidneys Excrete More Sodium and Water
⬇️
Blood Volume Falls
⬇️
Blood Pressure Returns Toward Normal
This phenomenon is called:
PRESSURE NATRIURESIS
Pressure = Blood Pressure
Natriuresis = Sodium Excretion in Urine
UNDERSTANDING THE AXES
X-AXIS
Arterial Pressure (mm Hg)
This is blood pressure.
Moving right →
means blood pressure is increasing.
Y-AXIS
Urinary Sodium or Volume Output
(× Normal)
This shows how much sodium and water the kidneys excrete.
Examples
- 1 = Normal output
- 2 = Twice normal output
- 4 = Four times normal output
- 8 = Eight times normal output
THE BLUE CURVE (ACUTE RESPONSE)
What Does “Acute” Mean?
Acute = Minutes to Hours
This is the immediate response of kidneys when blood pressure suddenly rises.
Follow the Blue Line
At 50 mmHg
Urinary sodium output is almost zero.
Kidneys conserve sodium and water.
At 100 mmHg
Output is about normal.
This is approximately the normal operating point.
At 150 mmHg
Output becomes about 4 times normal.
Kidneys start removing large amounts of sodium and water.
At 200 mmHg
Output becomes about 8 times normal.
Massive sodium and water loss occurs.
Why Does the Blue Line Rise?
Higher blood pressure:
⬇️
More renal perfusion pressure
⬇️
Less tubular reabsorption
⬇️
More sodium remains in tubules
⬇️
More sodium lost in urine
Easy Memory
“High Pressure Pushes Salt Out”
THE RED CURVE (CHRONIC RESPONSE)
What Does “Chronic” Mean?
Chronic = Days to Weeks
This represents what happens when blood pressure stays elevated for a long time.
Follow the Red Line
Look carefully.
The red line is almost vertical.
This is the most important message of the graph.
Around 95–100 mmHg
Output is very low.
Only a tiny increase in sodium excretion occurs.
Around 100–105 mmHg
A very small increase in pressure causes:
- Huge sodium loss
- Huge water loss
Output rapidly jumps from almost zero to 8 times normal.
Why Is the Red Line So Steep?
Because over days and weeks:
Additional mechanisms become activated.
Examples:
↓ Renin
⬇️
↓ Angiotensin II
⬇️
↓ Aldosterone
⬇️
Less Sodium Reabsorption
⬇️
More Sodium Excretion
These hormonal changes greatly amplify pressure natriuresis.
KEY DIFFERENCE BETWEEN THE TWO LINES
Blue Line (Acute)
Only direct kidney effects are working.
Response is gradual.
Red Line (Chronic)
Direct kidney effects +
Hormonal adaptations
Response becomes extremely powerful.
SIMPLE STORY
Imagine blood pressure rises from:
100 → 110 mmHg
Acute (Blue Line)
Kidneys remove a little extra sodium.
Small effect.Chronic (Red Line)
After several days:
- Renin falls
- Angiotensin II falls
- Aldosterone falls
Kidneys now remove enormous amounts of sodium.
Very powerful effect.
WHY IS THIS IMPORTANT?
This graph explains:
Long-Term Blood Pressure Control
The kidneys are the body’s most powerful long-term regulator of blood pressure.
If blood pressure rises:
⬇️
Kidneys excrete more sodium and water
⬇️
Blood volume decreases
⬇️
Cardiac output decreases
⬇️
Blood pressure falls
ONE-LINE SUMMARY OF EACH CURVE
Blue Curve (Acute)
Higher BP → Gradual increase in sodium and water excretion.
Red Curve (Chronic)
A tiny rise in BP → Massive increase in sodium and water excretion.
HIGH-YIELD EXAM PEARL
Which curve is steeper?
✅ Chronic Pressure Natriuresis Curve
Why?
Because hormonal adaptations (↓ Renin, ↓ Angiotensin II, ↓ Aldosterone) greatly enhance sodium excretion.
KEY CONCEPT
✅ The graph demonstrates pressure natriuresis.
✅ Increased arterial pressure causes increased sodium and water excretion by the kidneys.
✅ The blue curve shows the immediate (acute) response occurring within hours.
✅ The red curve shows the long-term (chronic) response occurring over days to weeks.
✅ Chronic pressure natriuresis is much more powerful than acute pressure natriuresis.
✅ A small chronic increase in blood pressure causes a very large increase in sodium and water excretion.
✅ This mechanism is the most important long-term regulator of arterial blood pressure.
Memory Formula
↑ BP → ↑ Na⁺ Excretion → ↓ Blood Volume → ↓ BP ✔️
Pressure Natriuresis and Diuresis: Key Components of a Renal–Body Fluid Feedback for Regulating Body Fluid Volumes and Arterial Pressure
- The effect of increased blood pressure on urine output is part of a powerful feedback system.
- This feedback system helps maintain balance between fluid intake and fluid output.
- This mechanism is the same mechanism involved in arterial pressure control.
- Extracellular fluid volume is controlled by this feedback mechanism.
- Blood volume is controlled by this feedback mechanism.
- Cardiac output is controlled by this feedback mechanism.
- Arterial pressure is controlled by this feedback mechanism.
- Urine output is controlled by this feedback mechanism.
- During changes in sodium and fluid intake, this feedback mechanism helps maintain fluid balance.
- This feedback mechanism minimizes changes in blood volume.
- This feedback mechanism minimizes changes in extracellular fluid volume.
- This feedback mechanism minimizes changes in arterial pressure.
Sequence of Events During Increased Fluid Intake
- An increase in fluid intake above urine output causes temporary fluid accumulation in the body.
- This assumes that sodium accompanies the fluid intake.
- As long as fluid intake exceeds urine output, fluid accumulates in the blood and interstitial spaces.
- Fluid accumulation increases blood volume.
- Fluid accumulation increases extracellular fluid volume.
- Increased blood volume raises mean circulatory filling pressure.
- Increased mean circulatory filling pressure increases the pressure gradient for venous return.
- Increased pressure gradient for venous return increases cardiac output.
- Increased cardiac output raises arterial pressure.
- Nervous reflexes and hormonal changes buffer the rise in arterial pressure.
- Increased arterial pressure increases urine output through pressure diuresis.
- The normal pressure natriuresis relationship is very steep.
- Only a slight increase in blood pressure is needed to increase urinary excretion severalfold.
- Increased fluid excretion balances the increased fluid intake.
- Further fluid accumulation is prevented.
- The renal-body fluid feedback mechanism prevents continuous accumulation of salt and water during increased intake.
- Large changes in salt and water intake can be accommodated with minimal changes in blood volume.
- Large changes in salt and water intake can be accommodated with minimal changes in extracellular fluid volume.
- Large changes in salt and water intake can be accommodated with minimal changes in cardiac output.
- Large changes in salt and water intake can be accommodated with minimal changes in arterial pressure.
- This occurs when the kidneys and regulatory mechanisms function effectively.
Sequence of Events During Decreased Fluid Intake
- The opposite sequence occurs when fluid intake falls below normal.
- Reduced fluid intake tends to decrease blood volume.
- Reduced fluid intake tends to decrease extracellular fluid volume.
- Reduced fluid intake tends to decrease arterial pressure.
- Even a small decrease in blood pressure causes a large decrease in urine output.
- Reduced urine output helps maintain fluid balance.
- Fluid balance is maintained with only minimal changes in blood pressure.
- Fluid balance is maintained with only minimal changes in blood volume.
- Fluid balance is maintained with only minimal changes in extracellular fluid volume.
- Changes in blood volume are usually very small despite large variations in daily water and electrolyte intake.
- Significant blood volume reduction occurs only when intake becomes too low to replace unavoidable fluid losses.
- Nervous and hormonal systems can increase sodium excretion to match increased sodium intake.
- Intrarenal mechanisms also contribute to this process.
- In many people, sodium excretion can increase without measurable increases in cardiac output.
- In many people, sodium excretion can increase without measurable increases in arterial pressure.
- Some individuals are more salt-sensitive.
- People with impaired kidney function are often more salt-sensitive.
- These individuals may develop significant increases in arterial pressure with moderate increases in sodium intake.
- Blood pressure responses to salt intake vary among individuals.
- Factors affecting this response include age.
- Factors affecting this response include the number of functional nephrons.
- Factors affecting this response include mechanisms that regulate renal sodium excretion.
- Prolonged high sodium intake over many years may cause high blood pressure.
- This can occur even in people who are not initially salt-sensitive.
- Gradual kidney injury contributes to this effect.
- When blood pressure increases, pressure natriuresis helps maintain balance between sodium intake and sodium excretion.
KEY CONCEPT
- Pressure natriuresis and pressure diuresis form a powerful renal-body fluid feedback system.
- Increased fluid intake → ↑ blood volume → ↑ venous return → ↑ cardiac output → ↑ arterial pressure → ↑ urine output.
- Increased urine output prevents excessive fluid accumulation.
- Decreased fluid intake → ↓ arterial pressure → ↓ urine output, helping conserve fluid.
- This feedback system keeps blood volume, extracellular fluid volume, and arterial pressure relatively stable.
- Pressure natriuresis is essential for matching sodium excretion to sodium intake, especially during long-term changes in salt intake.
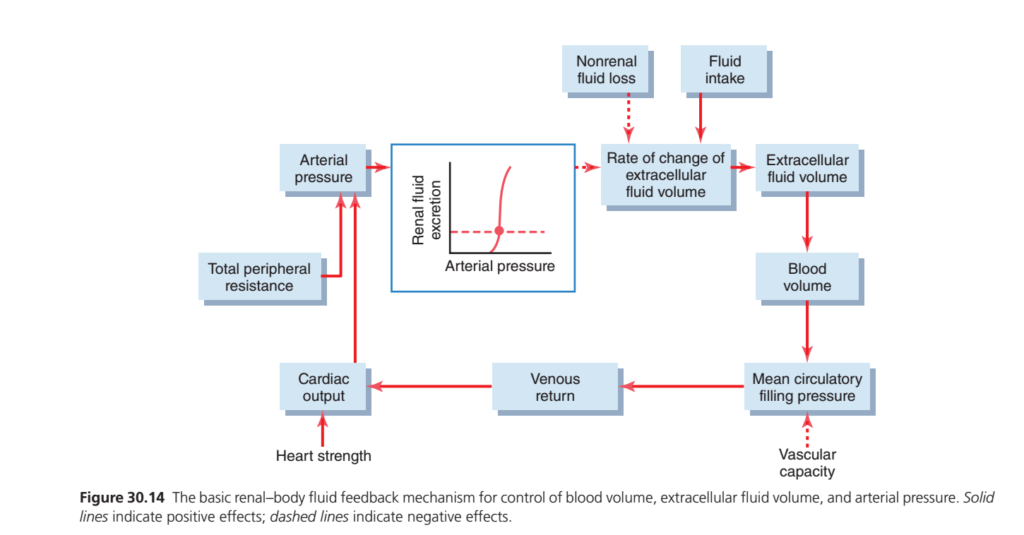
RENAL–BODY FLUID FEEDBACK MECHANISM FOR BLOOD PRESSURE CONTROL, THIS FIGURE 30.14 EXPLAINS
The kidneys act as the body’s long-term blood pressure regulator. When arterial blood pressure increases, the kidneys excrete more sodium and water (pressure natriuresis and diuresis). This decreases extracellular fluid volume and blood volume.
A lower blood volume reduces mean circulatory filling pressure, which decreases venous return to the heart. As venous return falls, cardiac output decreases, causing arterial blood pressure to fall back toward normal.
Conversely, when blood pressure falls, the kidneys retain more sodium and water. This increases extracellular fluid volume, blood volume, venous return, and cardiac output, helping restore blood pressure.
Thus, the kidney continuously balances fluid intake and fluid loss to maintain normal blood volume, extracellular fluid volume, cardiac output, and arterial pressure.
KEY CONCEPT
↑ Blood Pressure → ↑ Renal Excretion of Salt & Water → ↓ Blood Volume → ↓ Venous Return → ↓ Cardiac Output → ↓ Blood Pressure
↓ Blood Pressure → ↓ Renal Excretion of Salt & Water → ↑ Blood Volume → ↑ Venous Return → ↑ Cardiac Output → ↑ Blood Pressure
👉 The kidneys are the most important organs for long-term control of arterial blood pressure.
EFFECTIVENESS OF BLOOD VOLUME AND EXTRACELLULAR FLUID VOLUME REGULATION
- Figure 30.14 shows the basic feedback mechanisms that keep blood volume relatively constant despite large changes in daily fluid intake.
- A slight change in blood volume causes a change in cardiac output.
- A slight change in cardiac output causes a change in blood pressure.
- A slight change in blood pressure causes a large change in urine output.
- These factors work together to provide effective feedback control of blood volume.
- The same control mechanisms also operate during blood loss caused by hemorrhage.
- A fall in blood pressure causes the kidneys to retain fluid.
- Nervous factors also help cause fluid retention by the kidneys.
- Hormonal factors also help cause fluid retention by the kidneys.
- Other parallel processes help restore red blood cells and plasma proteins in the blood.
- If abnormalities in red blood cell volume remain, blood volume can still be maintained.
- This can occur when there is a deficiency of erythropoietin.
- This can also occur when other factors needed for red blood cell production are deficient.
- In these situations, plasma volume usually increases to make up the difference.
- As a result, the overall blood volume returns essentially to normal.
- This occurs even when red blood cell mass remains low.
KEY CONCEPT
- Figure 30.14: Small changes in blood volume → cardiac output → blood pressure → large changes in urine output.
- The kidneys provide powerful feedback control of blood volume.
- During hemorrhage, the kidneys retain fluid to help restore blood volume.
- Plasma volume can compensate for low red blood cell mass and help maintain normal overall blood volume.
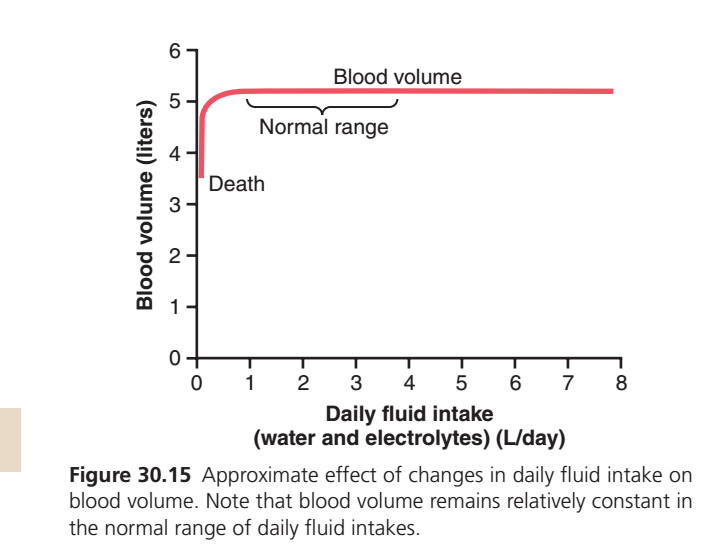
FIGURE 30.15: EFFECT OF DAILY FLUID INTAKE ON BLOOD VOLUME
WHAT IS THIS GRAPH SHOWING?
This graph shows:
How daily fluid intake affects blood volume.
The main message is:
👉 Even large changes in fluid intake cause only very small changes in blood volume because the kidneys adjust fluid excretion.
UNDERSTANDING THE AXES
X-AXIS
Daily Fluid Intake (Water and Electrolytes) (L/day)
This represents how much fluid a person drinks or consumes each day.
Moving to the right means:
➡️ More fluid intake
Examples:
- 1 L/day = Low intake
- 4 L/day = Moderate intake
- 8 L/day = Very high intake
Y-AXIS
Blood Volume (Liters)
This represents the total volume of blood in the body.
Normal blood volume is about:
➡️ 5 liters
THE RED CURVE (BLOOD VOLUME CURVE)
This entire red line represents:
Blood Volume at Different Fluid Intakes
PART 1: LEFT SIDE OF THE CURVE
Very Low Fluid Intake
At the far left:
- Fluid intake is extremely low.
- Blood volume is reduced.
The graph shows blood volume around:
3.5–4 liters
This region is labeled:
DEATH
Why?
If fluid intake becomes extremely low:
⬇️
Severe dehydration develops
⬇️
Blood volume falls dangerously
⬇️
Blood pressure falls
⬇️
Tissues do not receive enough blood
⬇️
Death may occur
PART 2: STEEP RISE OF THE CURVE
Notice the curve rises sharply at the beginning.
What Does This Mean?
A small increase in fluid intake from extremely low levels causes:
A large increase in blood volume
because the body is correcting dehydration.Easy Concept
Imagine a dried sponge.
Adding a little water causes a big change.
Similarly:
A severely dehydrated body quickly restores blood volume when fluid becomes available.
PART 3: THE FLAT PORTION OF THE CURVE
After blood volume reaches about:
5 liters
the curve becomes almost completely flat.
This is the most important part of the graph.What Does a Flat Line Mean?
It means:
Fluid intake changes a lot
BUT
Blood volume changes very little
Example
Fluid intake increases from:
1 L/day → 8 L/day
Yet blood volume remains close to:
5 liters
WHY DOES BLOOD VOLUME STAY CONSTANT?
Because the kidneys automatically adjust urine output.
When Fluid Intake Increases
More fluid enters the body
⬇️
Kidneys produce more urine
⬇️
Extra fluid is removed
⬇️
Blood volume stays normal
When Fluid Intake Decreases
Less fluid enters the body
⬇️
Kidneys conserve water
⬇️
Less urine is produced
⬇️
Blood volume stays near normal
NORMAL RANGE
The bracket labeled:
NORMAL RANGE
shows the usual blood volume range.
Within this range:
- Blood volume remains very stable.
- The kidneys match fluid output to fluid intake.
MOST IMPORTANT MESSAGE OF THE GRAPH
Fluid Intake Can Change Greatly
⬇️
Blood Volume Changes Very Little
because
⬇️
Kidneys Continuously Adjust Water and Salt Excretion
ONE-LINE INTERPRETATION OF THE RED CURVE
Extremely Low Fluid Intake
→ Blood volume falls dangerously.
Normal to High Fluid Intake
→ Blood volume remains almost constant at about 5 liters.
HIGH-YIELD EXAM POINT
Why is the curve almost flat over most of its length?
✅ Because the kidneys provide powerful regulation of blood volume by matching fluid excretion to fluid intake.
KEY CONCEPT
✅ Figure 30.15 shows the relationship between daily fluid intake and blood volume.
✅ At extremely low fluid intake, blood volume falls sharply and may reach life-threatening levels.
✅ Once normal hydration is achieved, blood volume remains close to 5 liters.
✅ Large increases in fluid intake cause little change in blood volume.
✅ The kidneys maintain this stability by increasing or decreasing urine output.
✅ Normal fluid intake → Nearly constant blood volume despite wide variations in water consumption.