


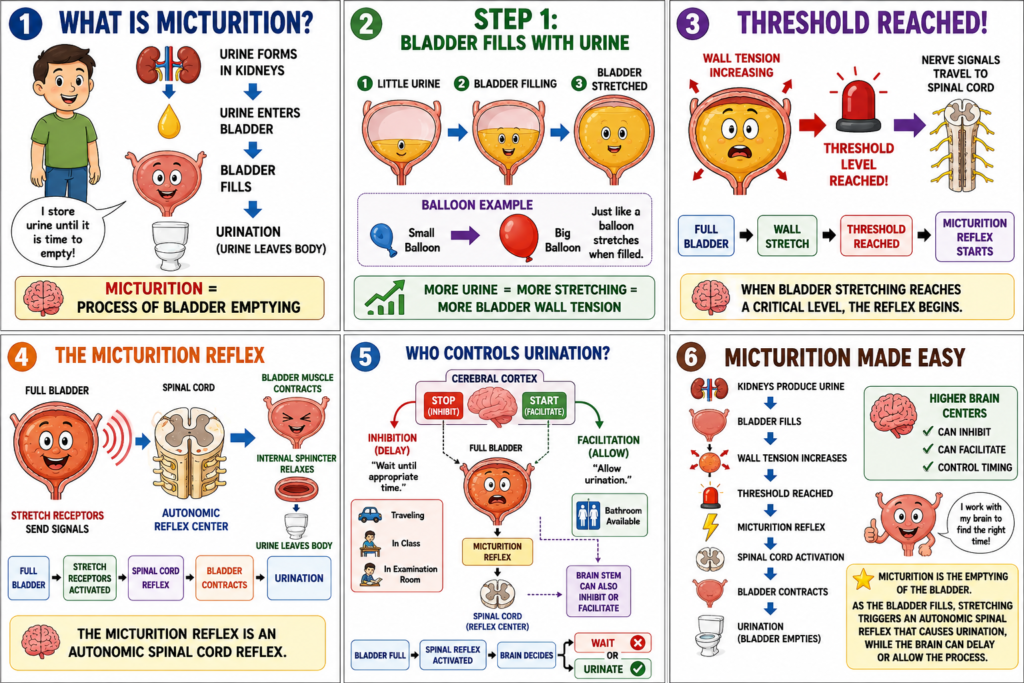
- Micturition is the process by which the urinary bladder empties its urine.
- Micturition occurs when the bladder becomes filled with urine.
- The process of micturition involves two main steps.
- In the first step, the bladder gradually fills with urine.
- As the bladder fills, the tension in the bladder wall progressively increases.
- The tension continues to rise until it reaches a threshold level.
- Reaching this threshold level triggers the second step.
- The second step is a nervous reflex called the micturition reflex.
- The micturition reflex causes the bladder to empty.
- If the bladder does not empty completely, the reflex at least produces a conscious desire to urinate.
- The micturition reflex is an autonomic reflex.
- It is a spinal cord reflex.
- The micturition reflex can be influenced by higher brain centers.
- Centers in the cerebral cortex can inhibit the micturition reflex.
- Centers in the cerebral cortex can also facilitate the micturition reflex.
- Centers in the brain stem can also inhibit or facilitate the micturition reflex.
KEY CONCEPT
Micturition is the process of bladder emptying. As the bladder fills, increasing wall tension triggers the micturition reflex, an autonomic spinal cord reflex that causes urination and can be controlled by higher centers in the brain.
PHYSIOLOGICAL ANATOMY OF THE BLADDER
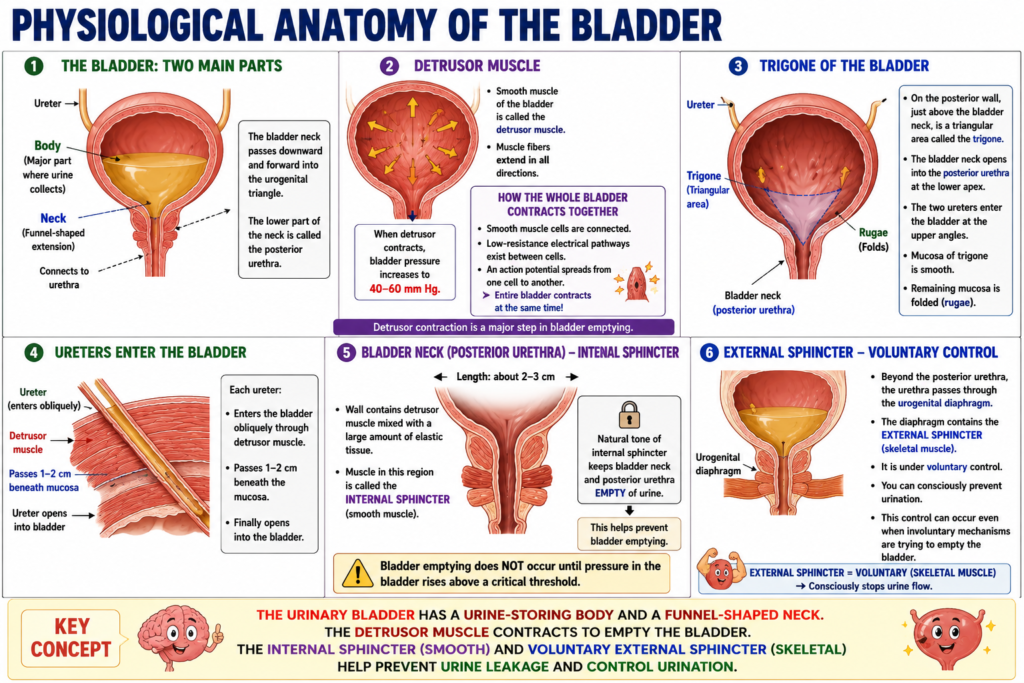
- The urinary bladder is a smooth muscle chamber.
- The bladder has two main parts.
- The first part is the body of the bladder.
- The body is the major part of the bladder where urine collects.
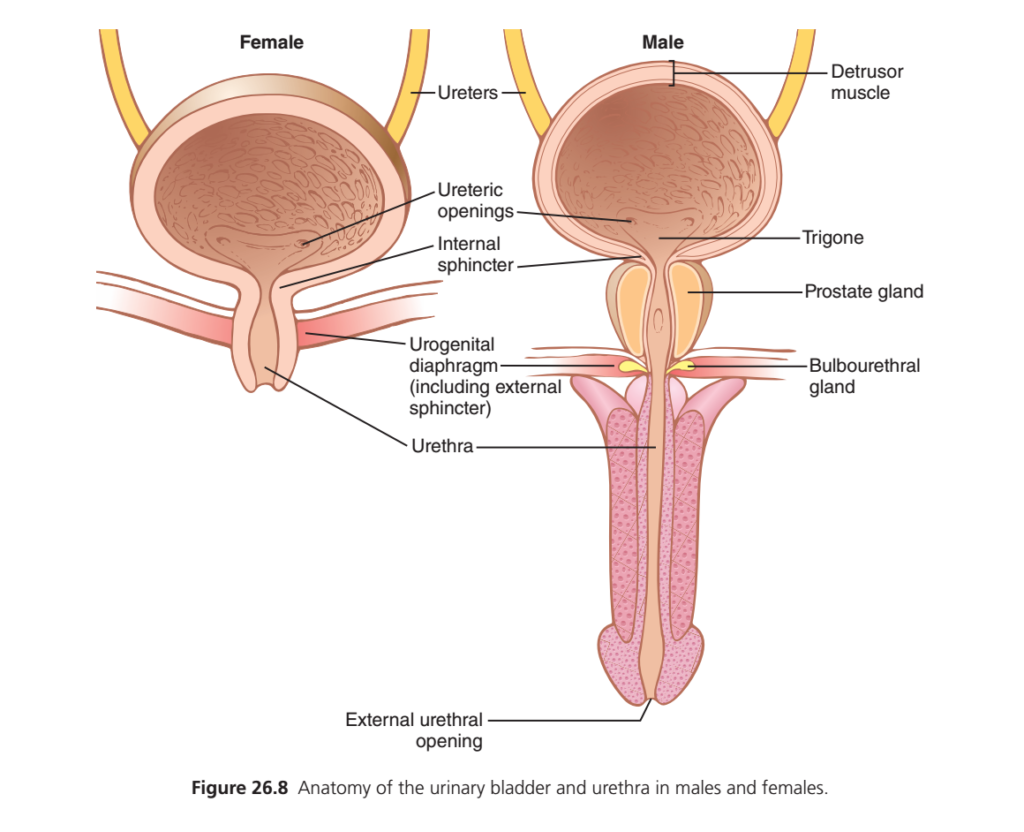
- The second part is the neck of the bladder.
- The bladder neck is a funnel-shaped extension of the bladder body.
- The bladder neck passes downward and forward into the urogenital triangle.
- The bladder neck connects with the urethra.
- The lower part of the bladder neck is also called the posterior urethra.
- The smooth muscle of the bladder is called the detrusor muscle.
- The muscle fibers of the detrusor muscle extend in all directions.
- When the detrusor muscle contracts, bladder pressure can increase to 40–60 mm Hg.
- Contraction of the detrusor muscle is a major step in bladder emptying.
- The smooth muscle cells of the detrusor muscle are connected to one another.
- Low-resistance electrical pathways exist between these muscle cells.
- An action potential can spread from one muscle cell to another.
- This spread of electrical activity causes the entire bladder to contract at the same time.
- On the posterior wall of the bladder, just above the bladder neck, is a small triangular area called the trigone.
- The bladder neck opens into the posterior urethra at the lower apex of the trigone.
- The two ureters enter the bladder at the upper angles of the trigone.
- The mucosa of the trigone is smooth.
- The remaining bladder mucosa is folded.
- These folds are called rugae.
- Each ureter enters the bladder obliquely through the detrusor muscle.
- Each ureter then passes 1–2 centimeters beneath the bladder mucosa.
- The ureter finally opens into the bladder.
- The bladder neck (posterior urethra) is about 2–3 centimeters long.
- Its wall contains detrusor muscle mixed with a large amount of elastic tissue.
- The muscle in this region is called the internal sphincter.
- The natural tone of the internal sphincter keeps the bladder neck and posterior urethra empty of urine.
- This helps prevent bladder emptying.
- Bladder emptying does not occur until pressure in the bladder rises above a critical threshold.
- Beyond the posterior urethra, the urethra passes through the urogenital diaphragm.
- The urogenital diaphragm contains the external sphincter of the bladder.
- The external sphincter is a voluntary skeletal muscle.
- The muscles of the bladder body and bladder neck are smooth muscles.
- The external sphincter is under voluntary control of the nervous system.
- The external sphincter can consciously prevent urination.
- This voluntary control can occur even when involuntary mechanisms are trying to empty the bladder.
KEY CONCEPT
The urinary bladder consists of a urine-storing body and a funnel-shaped neck. The detrusor muscle contracts to empty the bladder, while the internal sphincter and voluntary external sphincter help prevent urine leakage and control urination.
INNERVATION OF THE BLADDER
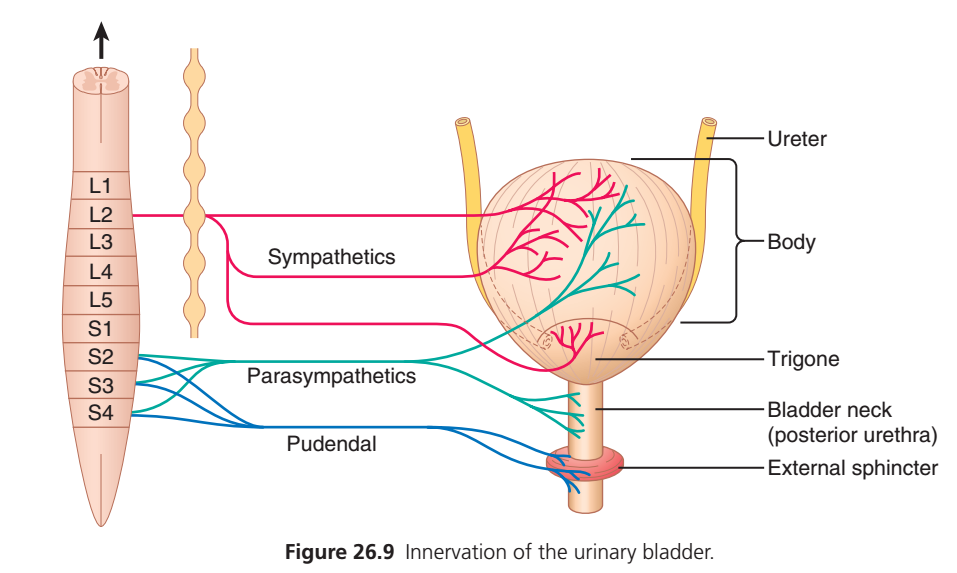
- The main nerve supply of the bladder is through the pelvic nerves.
- The pelvic nerves connect the bladder to the spinal cord through the sacral plexus.
- These nerves mainly connect with spinal cord segments S2 and S3.
- The pelvic nerves contain both sensory and motor nerve fibers.
- The sensory nerve fibers detect stretching of the bladder wall.
- These sensory fibers monitor the degree of bladder filling.
- Stretch signals from the posterior urethra are especially strong.
- These stretch signals are mainly responsible for initiating the reflexes that cause bladder emptying.
- The motor fibers in the pelvic nerves are parasympathetic nerve fibers.
- These parasympathetic fibers end on ganglion cells located in the bladder wall.
- Short postganglionic nerve fibers extend from these ganglion cells.
- These postganglionic fibers innervate the detrusor muscle.
- In addition to the pelvic nerves, other nerves also help control bladder function.
- One important nerve is the pudendal nerve.
- The pudendal nerve carries skeletal motor fibers.
- These fibers supply the external bladder sphincter.
- The fibers of the pudendal nerve are somatic nerve fibers.
- These fibers control the voluntary skeletal muscle of the external sphincter.
- The bladder also receives sympathetic innervation.
- Sympathetic fibers reach the bladder through the hypogastric nerves.
- These nerves connect mainly with the L2 segment of the spinal cord.
- The sympathetic fibers mainly stimulate the blood vessels of the bladder.
- These fibers have little role in bladder contraction.
- Some sensory nerve fibers also travel through the sympathetic nerves.
- These sensory fibers may contribute to the sensation of bladder fullness.
- In some situations, these fibers may also be involved in pain sensation.
KEY CONCEPT
The bladder receives parasympathetic, sympathetic, and somatic nerve supply. Pelvic nerves (S2–S3) detect bladder stretch and stimulate the detrusor muscle, the pudendal nerve controls the voluntary external sphincter, and sympathetic nerves mainly supply bladder blood vessels and contribute to sensations of fullness and pain.
URINE TRANSPORT FROM THE KIDNEYS THROUGH THE URETERS AND INTO THE BLADDER
- Urine leaving the bladder has essentially the same composition as the fluid leaving the collecting ducts.
- No significant changes occur in urine composition as it passes through the renal calyces and ureters to the bladder.
- Urine flowing from the collecting ducts enters the renal calyces.
- The incoming urine stretches the calyces.
- Stretching of the calyces increases their inherent pacemaker activity.
- Increased pacemaker activity initiates peristaltic contractions.
- These peristaltic contractions spread to the renal pelvis.
- The contractions then travel downward along the ureter.
- These contractions propel urine from the renal pelvis toward the bladder.
- In adults, the ureters are normally 25 to 35 centimeters (10–14 inches) long.
- The walls of the ureters contain smooth muscle.
- The ureters receive both sympathetic and parasympathetic nerve supply.
- The ureters also contain an intramural plexus of neurons and nerve fibers.
- This intramural plexus extends throughout the entire length of the ureters.
- Peristaltic contractions of the ureters are enhanced by parasympathetic stimulation.
- Peristaltic contractions are inhibited by sympathetic stimulation.
- The ureters enter the bladder through the detrusor muscle in the trigone region.
- The ureters normally pass obliquely through the bladder wall for several centimeters.
- The normal tone of the detrusor muscle compresses the ureters within the bladder wall.
- This compression helps prevent backflow (reflux) of urine from the bladder into the ureters.
- Reflux is prevented when bladder pressure increases during micturition or bladder compression.
- Each peristaltic wave increases pressure inside the ureter.
- The increased pressure opens the portion of the ureter passing through the bladder wall.
- This opening allows urine to flow into the bladder.
KEY CONCEPT
Urine moves from the kidneys to the bladder by peristaltic contractions of the ureters. The oblique passage of the ureters through the bladder wall and compression by the detrusor muscle prevent backflow of urine, while peristaltic waves allow urine to enter the bladder.
VESICOURETERAL REFLUX
- In some people, the ureter passes through the bladder wall for a shorter distance than normal.
- Because of this shorter course, bladder contraction during micturition may not completely close the ureter.
- As a result, some urine in the bladder flows backward into the ureter.
- This condition is called vesicoureteral reflux.
- Vesicoureteral reflux can cause enlargement of the ureters.
- If the reflux is severe, pressure can increase in the renal calyces.
- Increased pressure can also affect the structures of the renal medulla.
- This increased pressure may damage these kidney structures.
PAIN SENSATION IN THE URETERS AND THE URETERORENAL REFLEX
- The ureters contain a large number of pain nerve fibers.
- When a ureter becomes blocked, intense reflex constriction occurs.
- Ureteral stones are one cause of ureteral blockage.
- This constriction is associated with severe pain.
- Pain impulses travel through nerve pathways.
- These impulses trigger a sympathetic reflex back to the kidney.
- The sympathetic reflex causes constriction of the renal arterioles.
- Constriction of the renal arterioles decreases urine production by the kidney.
- This response is called the ureterorenal reflex.
- The ureterorenal reflex reduces the flow of fluid into the renal pelvis when the ureter is blocked.
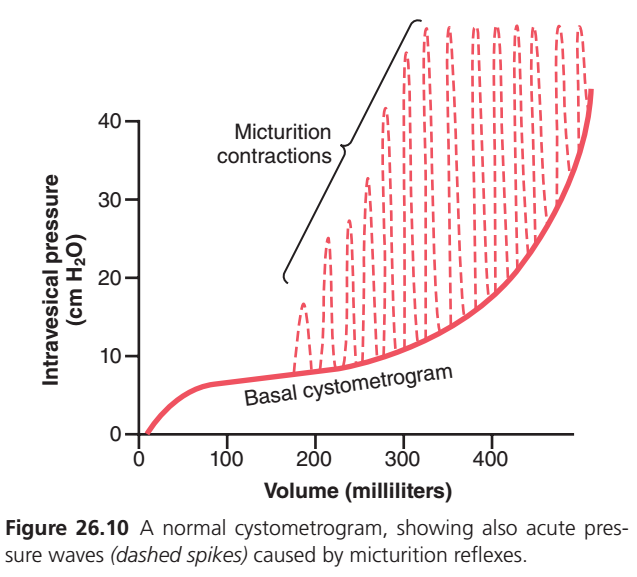
FILLING OF THE BLADDER AND BLADDER WALL TONE — THE CYSTOMETROGRAM
- A cystometrogram records changes in bladder pressure as the bladder fills with urine.
- When the bladder is empty, intravesical pressure is about 0.
- When 30 to 50 mL of urine collects in the bladder, pressure rises to about 5 to 10 cm of water.
- An additional 200 to 300 mL of urine can enter the bladder with only a small further increase in pressure.
- This relatively constant pressure is due to the intrinsic tone of the bladder wall.
- When bladder volume exceeds about 300 to 400 mL, pressure begins to rise rapidly.
- During bladder filling, periodic sudden increases in pressure occur.
- These pressure increases may last from a few seconds to more than one minute.
- The pressure peaks may rise only a few centimeters of water.
- In some cases, the pressure peaks may rise to more than 100 cm of water.
- These periodic pressure peaks are called micturition waves.
- Micturition waves are seen on the cystometrogram.
- Micturition waves are caused by the micturition reflex.
KEY CONCEPT
Vesicoureteral reflux occurs when urine flows backward from the bladder into the ureters because the ureters are not completely compressed during bladder contraction. The ureters are highly sensitive to pain, and blockage can trigger the ureterorenal reflex, which reduces urine formation. As the bladder fills, pressure changes are recorded on a cystometrogram, and periodic micturition waves occur due to the micturition reflex.
Micturition (Urination): Summarized Essay
Micturition is the process by which the urinary bladder empties urine when it becomes sufficiently full. As urine continuously flows from the kidneys through the ureters into the bladder, the bladder gradually fills and stretches. When the stretching reaches a certain threshold, it triggers a nervous mechanism called the micturition reflex, which causes contraction of the bladder and relaxation of the sphincters to allow urination. Although this reflex is primarily a spinal cord reflex, it can be voluntarily controlled or influenced by higher centers in the brain. Thus, a person can delay or facilitate urination when appropriate.
The urinary bladder is a hollow muscular organ composed of two main parts: the body, where urine is stored, and the neck, which connects the bladder to the urethra. The wall of the bladder contains the detrusor muscle, a powerful smooth muscle whose coordinated contraction is responsible for emptying the bladder. Because the muscle fibers are electrically connected, contraction spreads throughout the entire bladder, allowing it to act as a single functional unit during urination.
A specialized triangular region called the trigone lies on the posterior wall of the bladder between the openings of the ureters and the urethra. The bladder neck contains the internal sphincter, a smooth muscle structure that normally remains contracted to prevent urine leakage. Below this is the external sphincter, a voluntary skeletal muscle that allows conscious control over urination.
The bladder receives its main nerve supply through the pelvic nerves, which carry sensory signals from stretch receptors in the bladder wall and parasympathetic motor fibers that stimulate detrusor muscle contraction. The pudendal nerve supplies the external sphincter and enables voluntary control of urination. Sympathetic nerves mainly supply blood vessels and contribute to sensations of bladder fullness and pain.
Urine produced by the kidneys passes through the ureters to the bladder by rhythmic peristaltic contractions. The ureters enter the bladder obliquely through its wall, creating a valve-like mechanism that prevents the backward flow of urine during bladder contraction. If this mechanism is defective, a condition called vesicoureteral reflux may occur, in which urine flows backward into the ureters and kidneys, potentially causing kidney damage.
The bladder can store a large volume of urine with only a slight increase in pressure because of the elasticity and tone of its wall. As filling continues, periodic increases in bladder pressure called micturition waves occur due to activation of the micturition reflex. When bladder volume reaches approximately 300–400 mL, pressure rises rapidly and the urge to urinate becomes strong.
In summary, micturition is a coordinated process involving bladder filling, activation of the micturition reflex, contraction of the detrusor muscle, and relaxation of the urinary sphincters. The nervous system carefully regulates this process, allowing efficient storage and timely elimination of urine while maintaining voluntary control over urination.