Inflammation
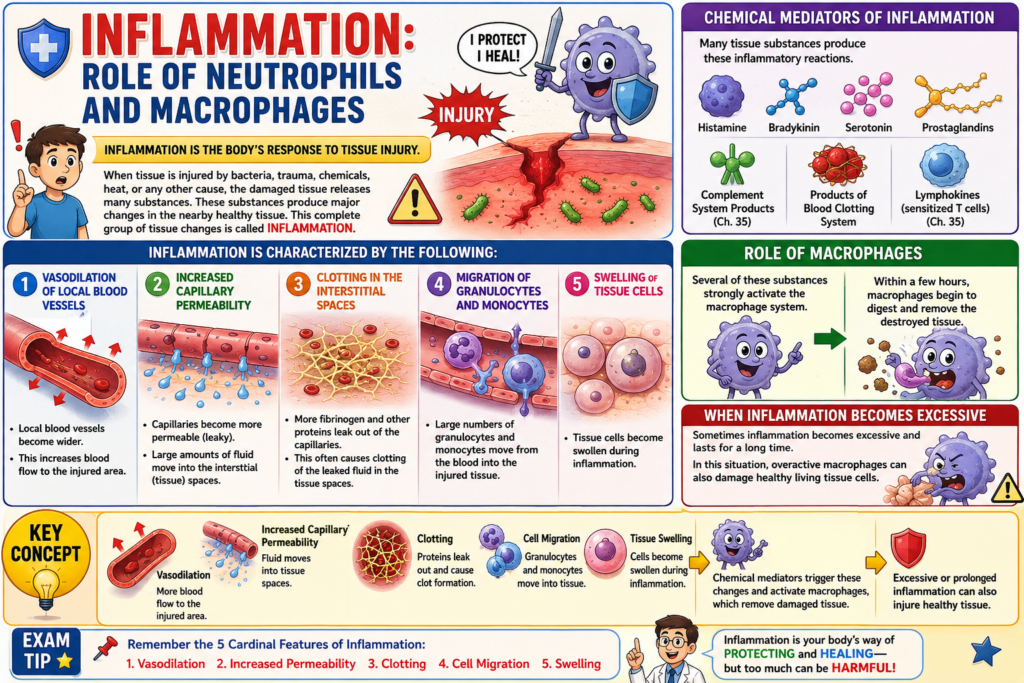
- When tissue is injured by bacteria, trauma, chemicals, heat, or any other cause, the damaged tissue releases many substances.
- These substances produce major changes in the nearby healthy tissue.
- This complete group of tissue changes is called inflammation.
- Inflammation is characterized by the following:
- (1) Vasodilation of local blood vessels
- Local blood vessels become wider.
- This increases blood flow to the injured area.
- (2) Increased capillary permeability
- Capillaries become more permeable (leaky).
- Large amounts of fluid move into the interstitial (tissue) spaces.
- (3) Clotting in the interstitial spaces
- More fibrinogen and other proteins leak out of the capillaries.
- This often causes clotting of the leaked fluid in the tissue spaces.
- (4) Migration of granulocytes and monocytes
- Large numbers of granulocytes and monocytes move from the blood into the injured tissue.
- (5) Swelling of tissue cells
- Tissue cells become swollen during inflammation.
- (1) Vasodilation of local blood vessels
- Many tissue substances produce these inflammatory reactions.
- These substances include:
- Histamine
- Bradykinin
- Serotonin
- Prostaglandins
- Different products of the complement system (Chapter 35)
- Products of the blood clotting system
- Lymphokines released by sensitized T cells (Chapter 35)
- Several of these substances strongly activate the macrophage system.
- Within a few hours, macrophages begin to digest and remove the destroyed tissue.
- Sometimes inflammation becomes excessive and lasts for a long time.
- In this situation, overactive macrophages can also damage healthy living tissue cells.
Key Concept
- Inflammation is the body’s response to tissue injury.
- It causes vasodilation, increased capillary permeability, clot formation, movement of granulocytes and monocytes, and tissue swelling.
- Chemical mediators trigger these changes and activate macrophages, which remove damaged tissue.
- Excessive or prolonged inflammation can also injure healthy tissue.
INFLAMMATION: ROLE OF NEUTROPHILS AND MACROPHAGES
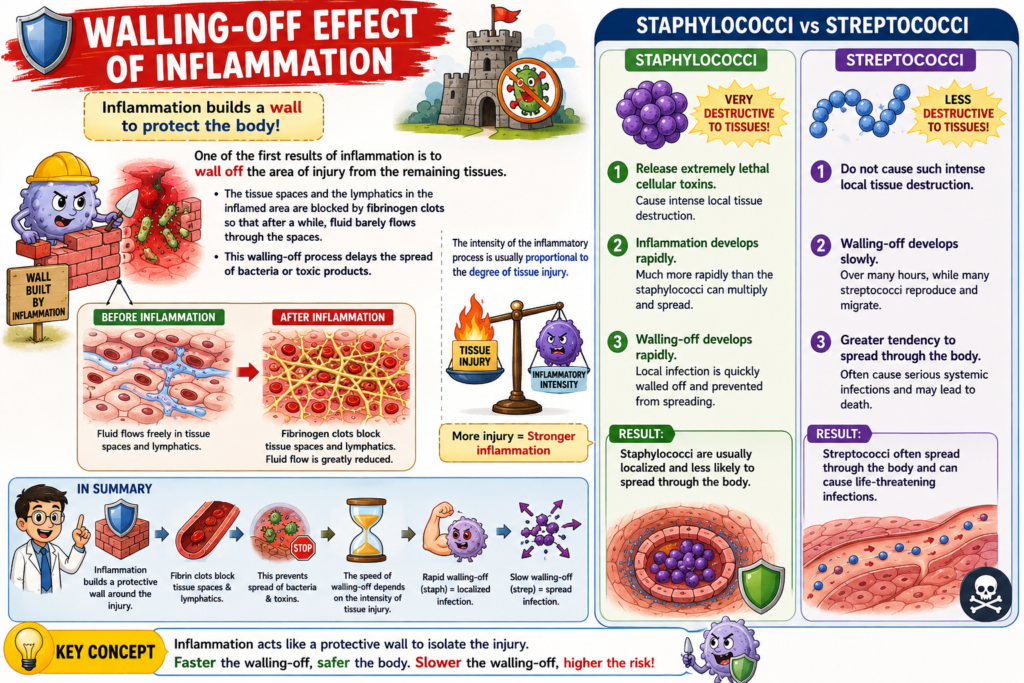
- One of the earliest effects of inflammation is to isolate (wall off) the injured area from the surrounding healthy tissues.
- The tissue spaces and lymphatic vessels in the inflamed area become blocked by fibrinogen clots.
- After some time, only a very small amount of fluid can pass through these blocked tissue spaces.
- This walling-off process slows the spread of bacteria and toxic substances to other parts of the body.
- The severity of inflammation usually depends on the severity of tissue injury.
- Staphylococci enter the tissues.
- They release very strong toxins that destroy tissue cells.
- As a result, inflammation develops very quickly.
- Inflammation develops faster than the staphylococci can multiply and spread.
- Therefore, the local staphylococcal infection is rapidly walled off.
- This rapid walling-off prevents the infection from spreading throughout the body.
- Streptococci do not cause severe local tissue destruction.
- Therefore, the walling-off process develops slowly over many hours.
- During this time, many streptococci multiply and spread into nearby tissues.
- As a result, streptococci have a much greater tendency to spread throughout the body.
- They can cause death more easily than staphylococci.
- This happens even though staphylococci cause much greater tissue destruction.
Key Concept
- Inflammation quickly isolates the injured area by forming fibrinogen clots.
- Walling-off reduces the spread of bacteria and toxins.
- More severe tissue injury produces a stronger and faster inflammatory response.
- Staphylococci are rapidly contained because they cause intense inflammation, while streptococci spread more easily because the walling-off process develops slowly.
INFLAMMATION: ROLE OF NEUTROPHILS AND MACROPHAGES
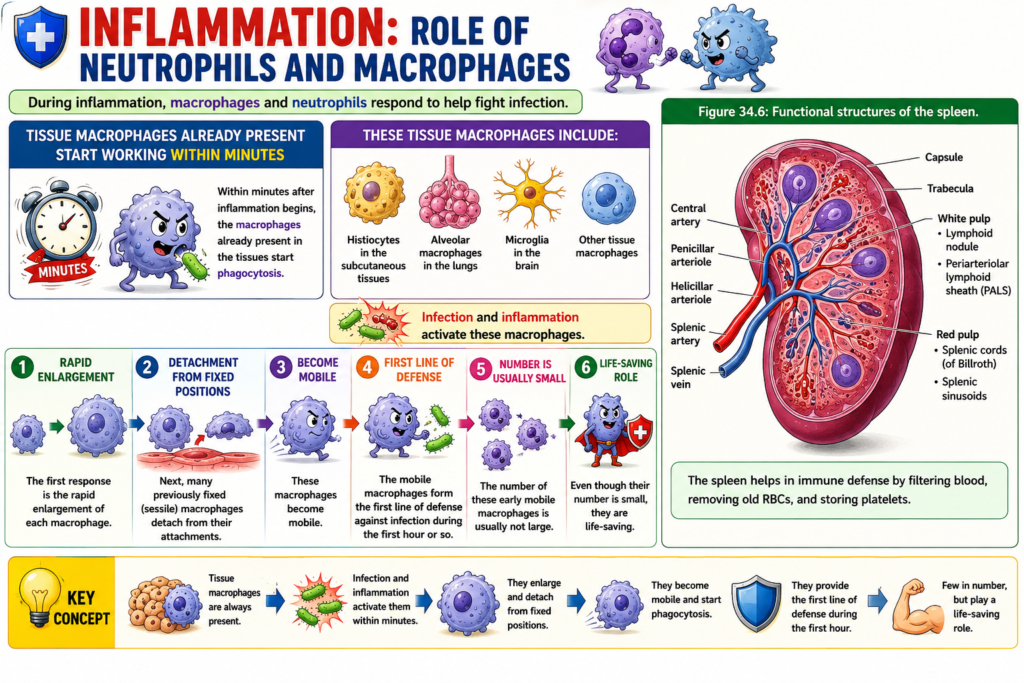
- During inflammation, macrophages and neutrophils respond to help fight infection.
- Within minutes after inflammation begins, the macrophages already present in the tissues start phagocytosis.
- These tissue macrophages include:
- Histiocytes in the subcutaneous tissues.
- Alveolar macrophages in the lungs.
- Microglia in the brain.
- Other tissue macrophages.
- Infection and inflammation activate these macrophages.
- The first response is the rapid enlargement of each macrophage.
- Next, many previously fixed (sessile) macrophages detach from their attachments.
- These macrophages become mobile.
- The mobile macrophages form the first line of defense against infection during the first hour or so.
- The number of these early mobile macrophages is usually not large.
- Even though their number is small, they are life-saving.
Figure Number
- Figure 34.6: Functional structures of the spleen.
Key Concept
- Tissue macrophages provide the first line of defense during inflammation.
- They become activated within minutes, enlarge, become mobile, and start phagocytosis.
- Although few in number, these early macrophages play a life-saving role during the first hour of infection.
INFLAMMATION: ROLE OF NEUTROPHILS AND MACROPHAGES
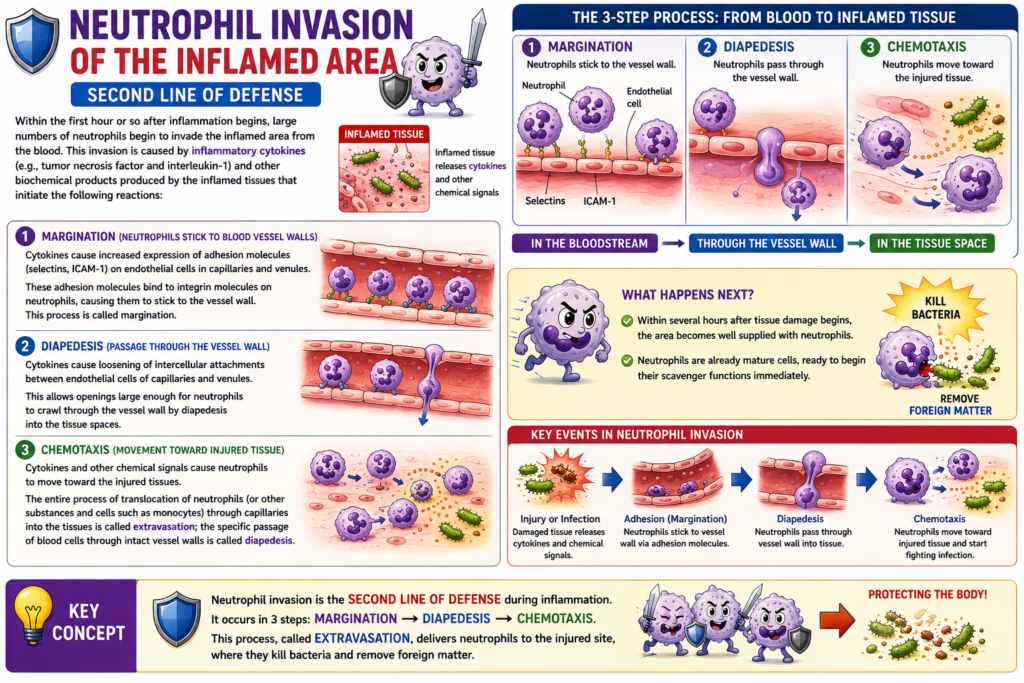
- Neutrophil invasion of the inflamed area is the second line of defense.
- Within the first hour after inflammation begins, large numbers of neutrophils move from the blood into the inflamed area.
- This neutrophil invasion is caused by inflammatory cytokines, such as tumor necrosis factor (TNF) and interleukin-1 (IL-1).
- Other biochemical substances released by the inflamed tissues also help start this process.
- These substances increase the expression of adhesion molecules, such as selectins and intercellular adhesion molecule-1 (ICAM-1), on the surface of endothelial cells in capillaries and venules.
- These adhesion molecules bind with complementary integrin molecules on neutrophils.
- This binding causes neutrophils to stick to the walls of capillaries and venules in the inflamed area.
- This process is called margination.
- These substances also loosen the attachments between endothelial cells of capillaries and small venules.
- This creates openings large enough for neutrophils to pass through the vessel wall.
- Neutrophils move through the capillary wall into the tissue spaces by diapedesis.
- These substances also cause chemotaxis, which attracts neutrophils toward the injured tissues.
- The movement of neutrophils and other cells, such as monocytes, from blood vessels into the surrounding tissues is called extravasation.
- The specific movement of blood cells through the intact capillary wall is called diapedesis.
- The term diapedesis is often used interchangeably with extravasation when describing blood cell movement into tissues.
- Within several hours after tissue injury begins, the damaged area becomes filled with neutrophils.
- Blood neutrophils are already mature cells.
- They immediately begin killing bacteria and removing foreign material.
Figure Number
- Figure 34.2: Margination.
- Figure 34.7: Margination in greater detail.
Key Concept
- Neutrophils provide the second line of defense during inflammation.
- Inflammatory cytokines cause margination, diapedesis, chemotaxis, and extravasation.
- Within a few hours, mature neutrophils enter the injured tissue and immediately destroy bacteria and remove foreign material.
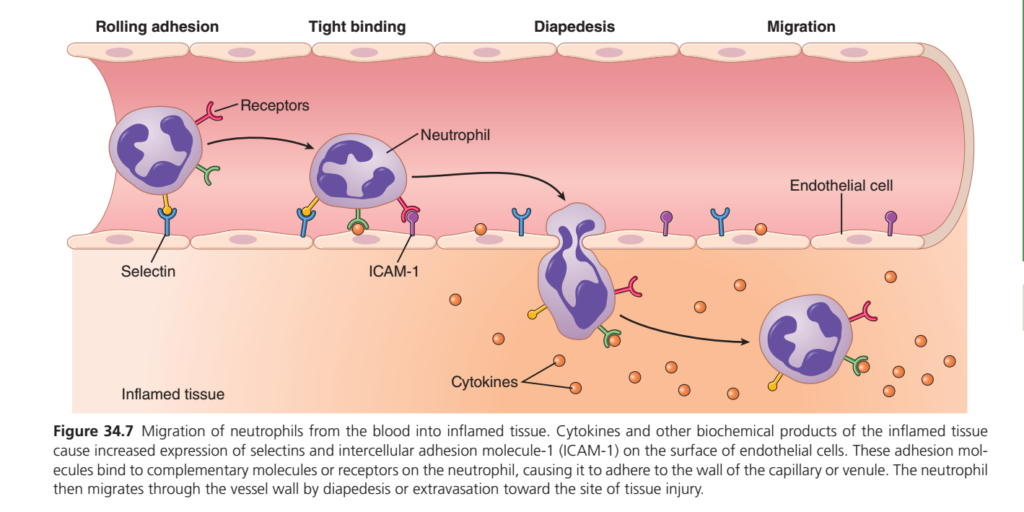
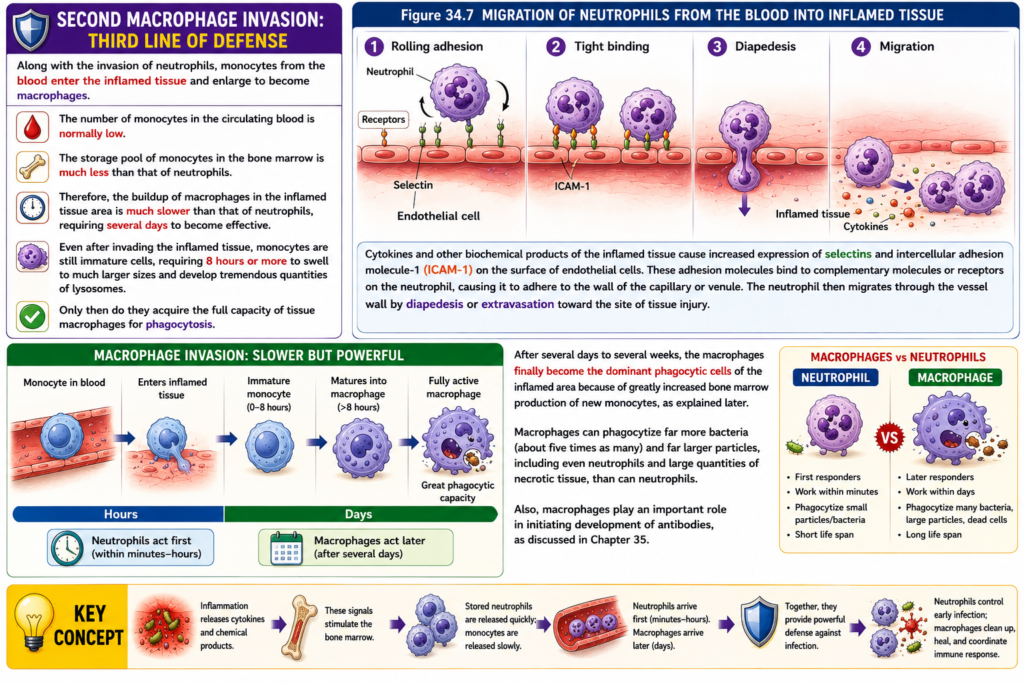
(Guyton Physiology): Migration of Neutrophils from Blood to Inflamed Tissue (Figure 34.7)
This figure explains how neutrophils (the first responder white blood cells) leave the bloodstream and reach the site of infection or tissue injury. This entire process is called leukocyte extravasation or neutrophil recruitment.
The figure shows four major sequential steps:
- Rolling adhesion
- Tight binding (Firm adhesion)
- Diapedesis (Transmigration)
- Migration (Chemotaxis)
The process occurs mainly in post-capillary venules, where blood flow is slow enough for neutrophils to interact with endothelial cells.
Overall Concept
Imagine there is a house on fire.
- Blood vessel = Road
- Neutrophil = Firefighter
- Endothelial cells = Roadside fence
- Cytokines = Emergency phone calls
- Selectins = Speed breakers
- ICAM-1 = Strong gate handles
- Diapedesis = Firefighter squeezing through the fence
- Chemotaxis = Following smoke toward the fire
Without these steps, neutrophils would simply continue flowing in the blood and never reach the infected tissue.
First Look at the Image
The figure has two main regions.
Upper Pink Area
This represents the blood vessel (capillary/venule).
Inside this area:
- flowing blood
- neutrophils
- endothelial cells
Lower Orange Area
This represents the
Inflamed tissue
This is where
- bacteria
- dead cells
- inflammatory mediators
- cytokines
are present.
This is the destination of neutrophils.
Endothelial Cells
The thin flat cells lining the blood vessel are called
Endothelial cells
Normally they form a smooth wall.
During inflammation they become activated.
Activated endothelial cells produce:
- Selectins
- ICAM-1
- VCAM-1
- Chemokines
Their job is to stop neutrophils from simply flowing away.
Cytokines (Orange Dots)
The orange dots represent
Cytokines
Examples
- TNF-α
- IL-1
- IL-8
- Chemokines
These cytokines are released by
- macrophages
- mast cells
- damaged tissue
- endothelial cells
Their function is to tell blood vessels
“There is infection here. Bring neutrophils immediately.”
Step 1 — Rolling Adhesion
The first heading in the figure is
Rolling Adhesion
Notice the neutrophil touching the endothelial wall but not sticking tightly.
Instead it keeps moving slowly.
Why?
Because the bonds are weak.
Which Molecule is Responsible?
The figure labels
Selectin
Selectins are weak adhesion molecules.
Types include
- P-selectin
- E-selectin
Neutrophils have complementary ligands.
What Happens?
Normally blood moves rapidly.
Neutrophils also move rapidly.
When inflammation occurs,
cytokines stimulate endothelial cells to express selectins.
Now neutrophils start making repeated weak attachments.
Attach…
Release…
Attach…
Release…
This produces
Rolling
instead of free-flowing movement.
Real-Life Example
Imagine driving on a highway.
Normally your car travels at 100 km/hour.
Now many speed breakers appear.
You slow down.
You are still moving,
but much more slowly.
Selectins are those speed breakers.
Why Rolling Is Important
If neutrophils kept flowing rapidly,
they would never detect infection.
Rolling gives them time to inspect the vessel wall.
Neutrophil Receptors
The figure labels
Receptors
These are proteins present on the neutrophil surface.
Examples
- L-selectin
- Integrins
- Ligands for selectins
These receptors recognize endothelial adhesion molecules.
Think of them as
“Hands of the neutrophil.”
Step 2 — Tight Binding (Firm Adhesion)
The second stage is
Tight Binding
Now the neutrophil suddenly stops moving.
Why?
Because weak selectin interactions change into
strong integrin-mediated attachment.
ICAM-1
The figure labels
ICAM-1
Full name
Intercellular Adhesion Molecule-1
ICAM-1 expression increases because of
- TNF
- IL-1
Integrins
Neutrophils contain
Integrins
Examples
- LFA-1
- Mac-1
These integrins bind strongly with ICAM-1.
What Happens?
Weak bond
↓
Strong bond
↓
Neutrophil completely stops.
This is called
Firm adhesion
Analogy
Suppose someone is climbing a mountain.
First,
they lightly touch a rock.
Later,
they hold it firmly with both hands.
Firm adhesion is that strong grip.
Why Firm Adhesion Is Necessary
The blood is still flowing.
Without firm adhesion,
blood pressure would wash the neutrophil away.
ICAM-1 prevents this.
Step 3 — Diapedesis
The next heading is
Diapedesis
Also called
- Extravasation
- Transmigration
This is the most dramatic step.
Look at the figure carefully.
The neutrophil changes its shape.
It becomes elongated.
It squeezes between endothelial cells.
It is literally leaving the bloodstream.
Why Does It Change Shape?
Neutrophils are highly flexible.
Their cytoskeleton rearranges.
They become soft and elongated.
This allows them to pass through spaces much smaller than their diameter.
Through What Does It Pass?
Not through the endothelial cell itself.
Instead,
between adjacent endothelial cells.
This process involves molecules like
- PECAM-1 (CD31)
- JAMs
- CD99
Analogy
Imagine
a large person squeezing through a narrow gate.
The body changes shape temporarily.
Neutrophils do the same.
Why Is It Called Extravasation?
Extra = outside
Vascular = blood vessel
Therefore
Leaving the blood vessel
↓
Extravasation
Step 4 — Migration
After leaving the vessel,
the neutrophil is still not at the infection.
Now it must travel through tissue.
This is shown in the last part of the figure.
Chemotaxis
Migration occurs because of
Chemotaxis
Meaning
Movement toward chemicals.
Which Chemicals Guide Neutrophils?
Examples
- IL-8
- C5a
- Leukotriene B4
- Bacterial peptides (fMLP)
These chemicals form a concentration gradient.
Higher concentration
↓
Closer to infection
Analogy
Imagine smelling fresh food.
The smell becomes stronger as you approach the kitchen.
You naturally walk toward the stronger smell.
Neutrophils behave similarly by moving toward increasing concentrations of chemotactic substances.
What Happens After Reaching the Infection?
Once neutrophils arrive,
they
- recognize bacteria
- engulf microbes (phagocytosis)
- release lysosomal enzymes
- produce reactive oxygen species
- kill microorganisms
- eventually die
Their accumulation contributes to the formation of pus, which consists mainly of dead neutrophils, bacteria, and tissue debris.
Why Cytokines Are Shown Everywhere
Notice the orange cytokine dots are mainly in inflamed tissue.
This shows they are released from injured tissue and diffuse outward.
They perform two important jobs:
- Activate endothelial cells to express adhesion molecules.
- Create a chemical gradient that guides neutrophils to the exact site of injury.
Complete Sequence (Flow Chart)
Tissue injury or bacterial infection
↓
Macrophages and damaged cells release cytokines
(TNF, IL-1, IL-8)
↓
Endothelial cells express Selectins
↓
Neutrophils slow down (Rolling adhesion)
↓
Integrins on neutrophils become activated
↓
Strong binding to ICAM-1 (Firm adhesion)
↓
Neutrophils squeeze between endothelial cells
(Diapedesis/Extravasation)
↓
Neutrophils follow chemotactic signals
(Migration/Chemotaxis)
↓
Arrival at infection
↓
Phagocytosis and killing of microorganismsClinical Correlation
Case 1: Bacterial Pneumonia
Bacteria infect the lungs. Alveolar macrophages release TNF-α, IL-1, and IL-8. Pulmonary endothelial cells express selectins and ICAM-1, neutrophils roll, adhere, undergo diapedesis, migrate into the alveoli, and phagocytose bacteria. The large number of dead neutrophils contributes to the purulent sputum seen in pneumonia.
Case 2: Acute Appendicitis
Inflammation of the appendix triggers cytokine release. Neutrophils leave nearby venules by the sequence shown in the figure. Histologically, dense neutrophilic infiltration is a hallmark of acute appendicitis.
Case 3: Leukocyte Adhesion Deficiency (LAD)
Patients with defects in β2 integrins cannot achieve firm adhesion to ICAM-1. Neutrophils fail to leave the bloodstream, leading to recurrent bacterial infections, delayed wound healing, and little or no pus formation despite severe infections.
High-Yield MBBS Points
- Rolling adhesion: mediated primarily by selectins (weak, reversible interactions).
- Firm adhesion: mediated by integrins on neutrophils binding ICAM-1 on endothelial cells.
- Diapedesis (extravasation): neutrophils pass between endothelial cells, especially in post-capillary venules.
- Migration: directed by chemotaxis toward increasing concentrations of inflammatory mediators.
- Major cytokines activating endothelium: TNF-α and IL-1.
- Major chemotactic factors: IL-8, C5a, leukotriene B4, and bacterial peptides (fMLP).
- Primary function of neutrophils after migration: rapid phagocytosis and destruction of invading microorganisms.
INFLAMMATION: ROLE OF NEUTROPHILS AND MACROPHAGES
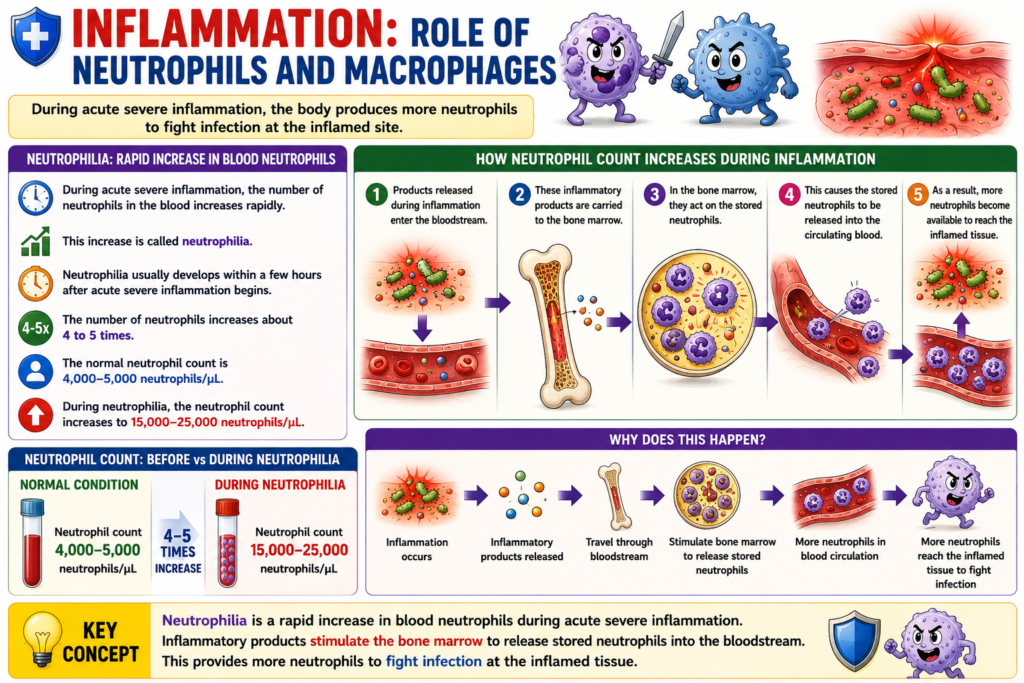
- During acute severe inflammation, the number of neutrophils in the blood increases rapidly.
- This increase is called neutrophilia.
- Neutrophilia usually develops within a few hours after acute severe inflammation begins.
- The number of neutrophils increases about 4 to 5 times.
- The normal neutrophil count is 4,000–5,000 neutrophils/μL.
- During neutrophilia, the neutrophil count increases to 15,000–25,000 neutrophils/μL.
- Products released during inflammation enter the bloodstream.
- These inflammatory products are carried to the bone marrow.
- In the bone marrow, they act on the stored neutrophils.
- This causes the stored neutrophils to be released into the circulating blood.
- As a result, more neutrophils become available to reach the inflamed tissue.
Key Concept
- Neutrophilia is a rapid increase in blood neutrophils during acute severe inflammation.
- Inflammatory products stimulate the bone marrow to release stored neutrophils into the bloodstream.
- This provides more neutrophils to fight infection at the inflamed tissue.
INFLAMMATION: ROLE OF NEUTROPHILS AND MACROPHAGES
- The second invasion of macrophages into the inflamed tissue is the third line of defense.
- Along with neutrophils, monocytes move from the blood into the inflamed tissue.
- After entering the tissue, monocytes enlarge and become macrophages.
- The number of monocytes in the circulating blood is normally low.
- The storage pool of monocytes in the bone marrow is much smaller than that of neutrophils.
- Therefore, macrophages accumulate in the inflamed tissue much more slowly than neutrophils.
- It takes several days for macrophages to become effective.
- Even after entering the inflamed tissue, monocytes are still immature cells.
- They require 8 hours or more to enlarge and develop large numbers of lysosomes.
- After this maturation, they gain the full phagocytic ability of tissue macrophages.
- After several days to several weeks, macrophages become the main phagocytic cells in the inflamed area.
- This happens because the bone marrow greatly increases the production of new monocytes.
- Macrophages can phagocytose about five times more bacteria than neutrophils.
- Macrophages can also engulf much larger particles.
- They can phagocytose neutrophils and large amounts of necrotic tissue.
- Macrophages also help start the development of antibodies.
Figure Number
- Figure 34.7: Migration of neutrophils from the blood into inflamed tissue.
- Cytokines increase the expression of selectins and ICAM-1 on endothelial cells.
- These adhesion molecules bind to receptors on neutrophils.
- Neutrophils attach to the vessel wall.
- Neutrophils then pass through the vessel wall by diapedesis (extravasation).
- They migrate toward the site of tissue injury.
Key Concept
- The third line of defense is the invasion of monocytes that mature into macrophages.
- Macrophages develop more slowly than neutrophils but become the dominant phagocytic cells after several days.
- They destroy more bacteria, remove large particles and dead tissue, and help initiate antibody formation.
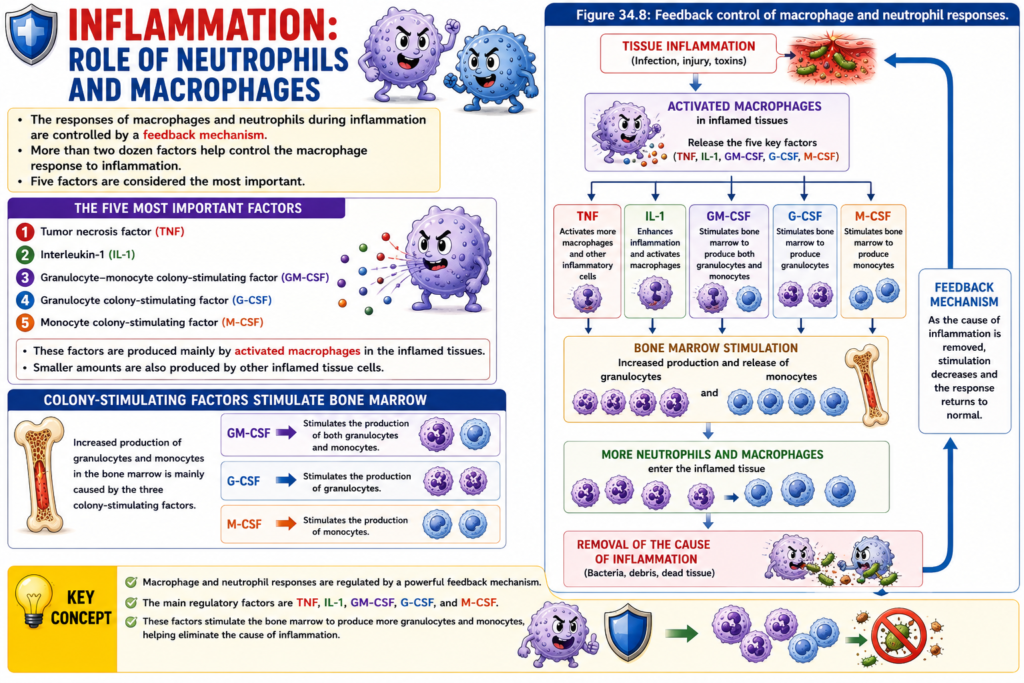
INFLAMMATION: ROLE OF NEUTROPHILS AND MACROPHAGES
- The responses of macrophages and neutrophils during inflammation are controlled by a feedback mechanism.
- More than two dozen factors help control the macrophage response to inflammation.
- Five factors are considered the most important.
- These five factors are:
- Tumor necrosis factor (TNF)
- Interleukin-1 (IL-1)
- Granulocyte-monocyte colony-stimulating factor (GM-CSF)
- Granulocyte colony-stimulating factor (G-CSF)
- Monocyte colony-stimulating factor (M-CSF)
- These factors are produced mainly by activated macrophages in the inflamed tissues.
- Smaller amounts are also produced by other inflamed tissue cells.
- Increased production of granulocytes and monocytes in the bone marrow is mainly caused by the three colony-stimulating factors.
- GM-CSF stimulates the production of both granulocytes and monocytes.
- G-CSF stimulates the production of granulocytes.
- M-CSF stimulates the production of monocytes.
- TNF, IL-1, and the colony-stimulating factors work together to produce a powerful feedback mechanism.
- This feedback mechanism starts with tissue inflammation.
- It increases the production of large numbers of defensive white blood cells.
- These white blood cells help remove the cause of inflammation.
Figure Number
- Figure 34.8: Feedback control of macrophage and neutrophil responses.
Key Concept
- Macrophage and neutrophil responses are regulated by a powerful feedback mechanism.
- The main regulatory factors are TNF, IL-1, GM-CSF, G-CSF, and M-CSF.
- These factors stimulate the bone marrow to produce more granulocytes and monocytes, helping eliminate the cause of inflammation.
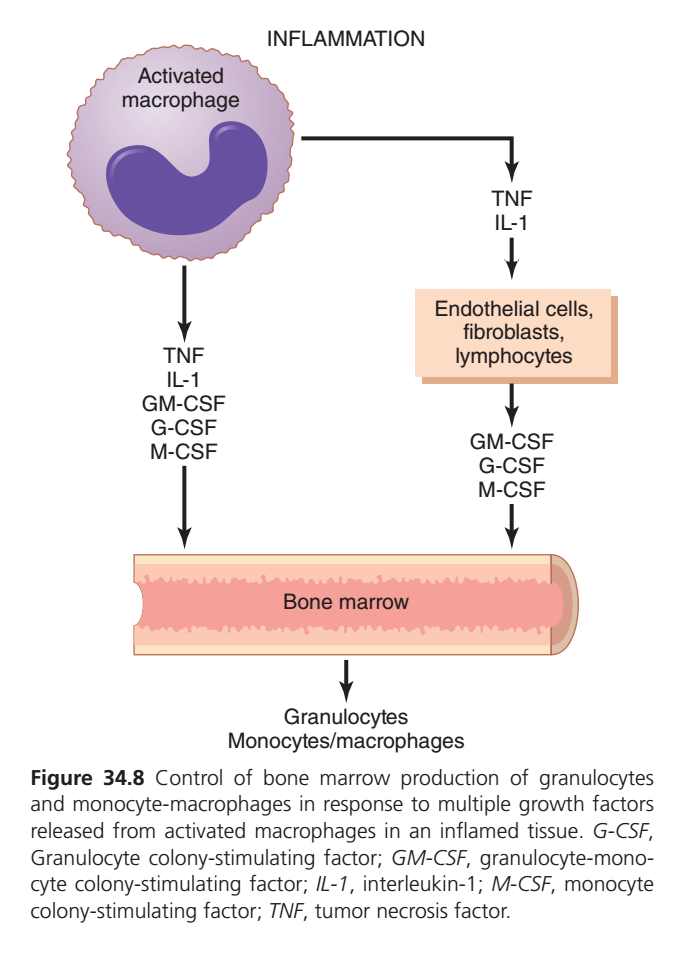
Guyton Physiology Figure 34.8 Explained in Detail
Control of Bone Marrow Production of Neutrophils and Monocytes During Inflammation
This figure explains how the body increases the production of white blood cells (especially neutrophils and monocytes) during inflammation.
Think of this figure as the “Emergency Reinforcement System” of the immune system.
In Figure 34.7, you learned how neutrophils leave the blood vessel and reach the infected tissue.
This figure (34.8) explains a different but equally important question:
“Where do all those extra neutrophils come from?”
The answer is:
Bone marrow produces them after receiving emergency signals from the inflamed tissue.
Overall Concept
Imagine a country is attacked.
Initially,
local police control the situation.
But if the attack becomes severe,
the police chief immediately contacts military headquarters asking for more soldiers.
Military headquarters quickly trains and sends thousands of new soldiers.
Exactly the same thing happens during inflammation.
Here,
| Real Life | Human Body |
|---|---|
| Police Chief | Activated macrophage |
| Emergency phone call | Cytokines |
| Military Headquarters | Bone marrow |
| Newly trained soldiers | Neutrophils and Monocytes |
First Look at the Figure
The figure has five important parts
- Activated macrophage
- Cytokines released by macrophage
- Endothelial cells, fibroblasts and lymphocytes
- Bone marrow
- Newly produced granulocytes and monocytes
Everything begins from the activated macrophage.
PART 1
Activated Macrophage
Look at the large cell on the upper left.
It represents an
Activated macrophage
What is a macrophage?
A macrophage is a large immune cell that
- eats bacteria
- removes dead tissue
- destroys viruses
- cleans injured tissue
- controls inflammation
Think of macrophages as
The Commander of the Immune System
Why is it called Activated?
Normally macrophages remain quiet.
When they detect
- bacteria
- viruses
- fungi
- damaged tissue
they become activated.
Activation means
“They wake up and begin sending emergency messages.”
Clinical Example
Suppose a nail enters your foot.
Immediately,
macrophages around the wound detect bacteria.
Within minutes,
they become activated.
Now they start producing many inflammatory chemicals.
PART 2
Cytokines Released by Activated Macrophage
Below the macrophage the figure lists five important molecules.
- TNF
- IL-1
- GM-CSF
- G-CSF
- M-CSF
These are communication molecules.
Think of them as
Emergency WhatsApp Messages
They tell the rest of the body
“We need more white blood cells immediately.”
TNF (Tumor Necrosis Factor)
Usually produced first.
Main functions
✔ Causes fever
✔ Activates endothelial cells
✔ Increases vascular permeability
✔ Stimulates bone marrow
✔ Increases inflammation
Clinical Example
In severe bacterial infection (sepsis),
very large amounts of TNF are released.
Excess TNF may produce
- hypotension
- septic shock
- multiple organ failure
So TNF is useful in controlled amounts but harmful in excess.
IL-1 (Interleukin-1)
IL-1 works together with TNF.
Functions
- fever
- activates endothelial cells
- stimulates liver
- stimulates bone marrow
- increases inflammatory response
Easy Analogy
TNF and IL-1 are like
Two emergency officers making hundreds of phone calls asking for help.
GM-CSF
(Granulocyte-Monocyte Colony Stimulating Factor)
This growth factor stimulates bone marrow to produce
Both
- granulocytes
- monocytes
Remember
GM = Granulocyte + Monocyte
Very easy to remember.
G-CSF
Granulocyte Colony Stimulating Factor
This specifically increases production of
Granulocytes
Especially
Neutrophils
Clinical Importance
Doctors give
Filgrastim (G-CSF)
to cancer patients after chemotherapy.
Why?
Because chemotherapy destroys bone marrow.
G-CSF tells bone marrow
“Start making neutrophils quickly.”
M-CSF
Monocyte Colony Stimulating Factor
Stimulates production of
Monocytes
Later these monocytes enter tissues and become
Macrophages
Easy Trick
M-CSF
↓
Monocytes
↓
Macrophages
Why Are These Called Colony Stimulating Factors?
Inside bone marrow,
one stem cell divides repeatedly.
One stem cell forms a colony of similar cells.
These growth factors stimulate that colony.
Hence
Colony Stimulating Factors.
PART 3
Endothelial Cells, Fibroblasts and Lymphocytes
Look at the right side of the figure.
It shows
- Endothelial cells
- Fibroblasts
- Lymphocytes
Why Are They Included?
Macrophages are not working alone.
TNF and IL-1 stimulate these neighboring cells.
After stimulation,
they also begin producing
- GM-CSF
- G-CSF
- M-CSF
Now even more growth factors reach bone marrow.
Analogy
Imagine one person shouting
“Fire!”
Soon
everyone in the neighborhood also starts shouting.
The message becomes much stronger.
Similarly,
many cells amplify the inflammatory signal.Endothelial Cells
These line blood vessels.
During inflammation they
- express adhesion molecules
- release cytokines
- help recruit neutrophils
- produce growth factors
Fibroblasts
Normally fibroblasts repair damaged tissue.
During inflammation they also
produce growth factors.
Lymphocytes
These are adaptive immune cells.
They also contribute cytokines that help regulate inflammation and stimulate immune cell production.
PART 4
Bone Marrow
Look at the large structure at the bottom.
This represents
Bone marrow
Bone marrow is the
Factory of Blood Cells.
It producesuring Normal Conditions
Only the required number of neutrophils are produced each day.
During Infection
The bone marrow receives
- TNF
- IL-1
- GM-CSF
- G-CSF
- M-CSF
Now it dramatically increases production.
Clinical Example
Suppose someone develops pneumonia.
Bone marrow may produce millions of extra neutrophils within a short time.
Blood tests show
High WBC count
called
Leukocytosis.
PART 5
Granulocytes and Monocytes
At the bottom,
the figure shows
Granulocytes
and
Monocytes/Macrophages.
These are the final products released from bone marrow.
Granulocytes
Granulocytes include
- Neutrophils
- Eosinophils
- Basophils
During bacterial infection,
mainly
Neutrophils increase.
Why Are They Called Granulocytes?
Because their cytoplasm contains many granules filled with enzymes used to kill microorganisms.
Monocytes
Monocytes circulate in blood.
After entering tissues,
they become
Macrophages.
Notice something interesting.
The figure starts with
Macrophage
↓
and ends with
Macrophages.
This forms a
Positive Feedback Loop.
Positive Feedback Loop
Step 1
One macrophage detects bacteria.
↓
Step 2
Releases cytokines.
↓
Step 3
Bone marrow produces many monocytes.
↓
Step 4
Monocytes become macrophages.
↓
Step 5
More macrophages release more cytokines.
↓
Immune response becomes stronger until the infection is controlled.
Connecting Figure 34.8 with Figure 34.7
These two figures describe different stages of the same inflammatory response.
| Figure 34.8 | Figure 34.7 |
|---|---|
| Produces new neutrophils and monocytes in bone marrow | Shows how neutrophils leave the bloodstream |
| Focuses on cytokine signaling | Focuses on leukocyte recruitment |
| Begins with activated macrophages | Begins with circulating neutrophils |
| Ends with increased leukocyte production | Ends with neutrophils reaching infected tissue |
Together, they explain how the body first creates more immune cells and then delivers them efficiently to the site of infection.
Clinical Correlations
1. Bacterial Infection
A patient with bacterial pneumonia activates macrophages in the lungs. TNF, IL-1, and colony-stimulating factors stimulate the bone marrow, increasing neutrophil production. This results in neutrophilic leukocytosis, a common laboratory finding.
2. Chemotherapy-Induced Neutropenia
Chemotherapy suppresses bone marrow, reducing neutrophil production and increasing infection risk. Administration of G-CSF (e.g., filgrastim) accelerates neutrophil recovery and lowers the risk of severe infections.
3. Chronic Inflammation
In chronic inflammatory diseases such as rheumatoid arthritis, persistent cytokine production continuously stimulates the bone marrow, contributing to sustained immune cell production and ongoing inflammation.
High-Yield MBBS Points
- Activated macrophages are the primary initiators of this response.
- TNF and IL-1 activate endothelial cells, induce fever, and stimulate the production of colony-stimulating factors.
- GM-CSF promotes the production of both granulocytes and monocytes.
- G-CSF specifically increases granulocyte (especially neutrophil) production.
- M-CSF specifically increases monocyte production.
- Endothelial cells, fibroblasts, and lymphocytes amplify the response by producing additional colony-stimulating factors.
- Bone marrow responds by increasing the release of neutrophils and monocytes into the bloodstream.
- Monocytes migrate into tissues and differentiate into macrophages, reinforcing the immune response.
Complete Flow Chart
Bacterial infection or tissue injury
↓
Macrophages become activated
↓
Release TNF and IL-1
↓
Direct stimulation of bone marrow
↓
Activation of endothelial cells, fibroblasts, and lymphocytes
↓
Production of GM-CSF, G-CSF, and M-CSF
↓
Bone marrow increases hematopoiesis
↓
More granulocytes (especially neutrophils)
and monocytes are released
↓
Monocytes enter tissues and become macrophages
↓
Enhanced elimination of pathogens and tissue repairKey Concept
Figure 34.8 demonstrates the systemic regulation of inflammation. Activated macrophages do not merely destroy pathogens; they orchestrate the entire immune response by releasing TNF, IL-1, and colony-stimulating factors. These mediators stimulate the bone marrow to produce additional neutrophils and monocytes, ensuring a continuous supply of immune cells. This bone marrow response, combined with the leukocyte recruitment process shown in Figure 34.7, enables the body to mount a rapid and effective defense against infection while supporting tissue repair.
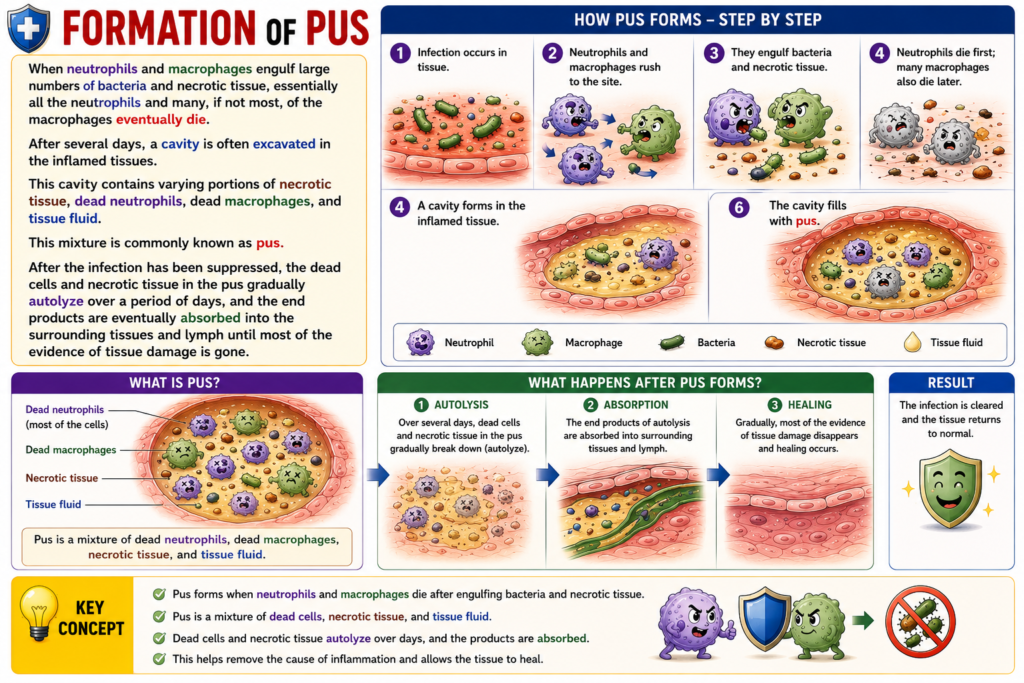
FOMATION OF PUS
- When neutrophils and macrophages engulf large numbers of bacteria and necrotic tissue, almost all neutrophils and many, or most, macrophages eventually die.
- After several days, a cavity often forms in the inflamed tissue.
- This cavity contains:
- Necrotic tissue.
- Dead neutrophils.
- Dead macrophages.
- Tissue fluid.
- This mixture is called pus.
- After the infection has been suppressed, the dead cells and necrotic tissue in the pus gradually undergo autolysis over several days.
- The end products are eventually absorbed into the surrounding tissues and lymph.
- Finally, most of the evidence of tissue damage disappears.
Key Concept
- Pus forms after neutrophils and macrophages die while engulfing bacteria and necrotic tissue.
- Pus contains necrotic tissue, dead neutrophils, dead macrophages, and tissue fluid.
- After the infection is controlled, pus undergoes autolysis, and its breakdown products are absorbed until most tissue damage disappears.