- Excessive bleeding can occur because of a deficiency of one or more blood-clotting factors.
- Three major bleeding disorders are discussed:
- (1) Bleeding due to vitamin K deficiency
- (2) Hemophilia
- (3) Thrombocytopenia (platelet deficiency)
Key Concept
- Excessive bleeding occurs when important clotting factors or platelets are deficient. The three major causes discussed are vitamin K deficiency, hemophilia, and thrombocytopenia.
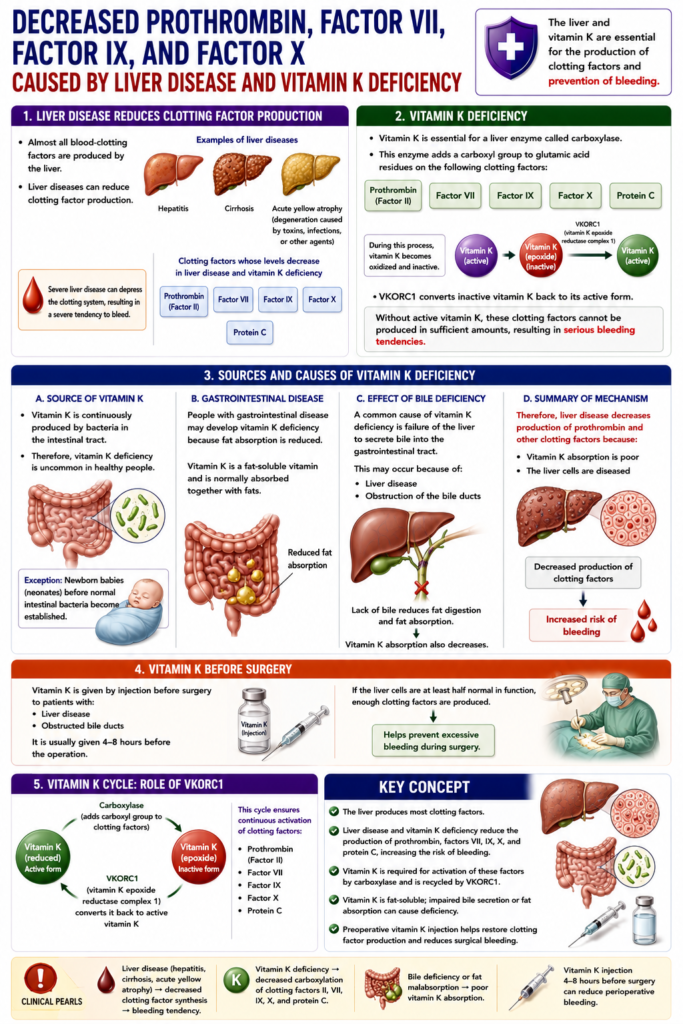
DECREASED PROTHROMBIN, FACTOR VII, FACTOR IX, AND FACTOR X CAUSED BY LIVER DISEASE AND VITAMIN K DEFICIENCY
- Almost all blood-clotting factors are produced by the liver.
- Therefore, liver diseases can reduce clotting factor production.
- Examples of liver diseases include:
- Hepatitis
- Cirrhosis
- Acute yellow atrophy (degeneration of the liver caused by toxins, infections, or other agents)
- Severe liver disease can depress the clotting system.
- As a result, the patient develops a severe tendency to bleed.
Vitamin K Deficiency
- Vitamin K deficiency is another cause of reduced clotting factor production by the liver.
- Vitamin K is essential for a liver enzyme called carboxylase.
- This enzyme adds a carboxyl group to glutamic acid residues on the following clotting factors:
- Prothrombin
- Factor VII
- Factor IX
- Factor X
- Protein C
- During this process, vitamin K becomes oxidized and inactive.
- Vitamin K epoxide reductase complex 1 (VKORC1) converts inactive vitamin K back to its active form.
- Without active vitamin K, these clotting factors cannot be produced in sufficient amounts.
- This results in serious bleeding tendencies.
Source of Vitamin K
- Vitamin K is continuously produced by bacteria in the intestinal tract.
- Therefore, vitamin K deficiency is uncommon in healthy people.
- An exception is newborn babies (neonates) before normal intestinal bacteria become established.
Vitamin K Deficiency in Gastrointestinal Disease
- People with gastrointestinal disease may develop vitamin K deficiency.
- This occurs because fat absorption is reduced.
- Vitamin K is a fat-soluble vitamin.
- It is normally absorbed together with fats.
Effect of Bile Deficiency
- A common cause of vitamin K deficiency is failure of the liver to secrete bile into the gastrointestinal tract.
- This may occur because of:
- Liver disease
- Obstruction of the bile ducts
- Lack of bile reduces fat digestion and fat absorption.
- As a result, vitamin K absorption also decreases.
- Therefore, liver disease decreases production of prothrombin and other clotting factors because:
- Vitamin K absorption is poor
- The liver cells are diseased
Vitamin K Before Surgery
- Vitamin K is given by injection before surgery to patients with:
- Liver disease
- Obstructed bile ducts
- It is usually given 4–8 hours before the operation.
- If the liver cells are at least half normal in function, enough clotting factors are produced.
- This helps prevent excessive bleeding during surgery.
Key Concept
- The liver produces most clotting factors. Liver disease and vitamin K deficiency reduce the production of prothrombin, factors VII, IX, X, and protein C, increasing the risk of bleeding. Vitamin K is required for activation of these factors and is recycled by VKORC1. Because vitamin K is fat-soluble, impaired bile secretion or fat absorption can cause deficiency. Preoperative vitamin K injection helps restore clotting factor production and reduces surgical bleeding.
HEMOPHILIA
- Hemophilia is a bleeding disorder.
- It occurs almost exclusively in men.
- About 85% of cases are caused by deficiency or abnormality of factor VIII.
- This type is called Hemophilia A (classic hemophilia).
- About 1 in every 10,000 men in the United States has classic hemophilia.
- The remaining 15% of cases are Hemophilia B.
- Hemophilia B is caused by deficiency of factor IX.
Inheritance
- Hemophilia A and Hemophilia B are inherited through the female X chromosome.
- They are X-linked recessive disorders.
- Women rarely develop hemophilia because they have two X chromosomes, and one normal gene is usually enough.
- If one X chromosome carries the defective gene, the woman is a carrier.
- A carrier mother has:
- 50% chance of passing hemophilia to each son.
- 50% chance of passing carrier status to each daughter.
Hemophilia in Females
- Most female carriers do not have symptoms because they have one normal allele.
- Some female carriers may have mild bleeding symptoms.
- Mild hemophilia in females can occur because of:
- Loss of part or all of the normal X chromosome (Turner syndrome).
- Inactivation (lyonization) of the normal X chromosome.
- A woman develops full symptomatic Hemophilia A or B only if she inherits:
- One defective X chromosome from her carrier mother, and
- One defective X chromosome from her father with hemophilia.
- Most cases are inherited.
- However, about one-third of patients have no family history.
- These cases are caused by new (novel) genetic mutations.
Severity of Bleeding
- The severity of bleeding depends on the degree of genetic deficiency.
- Bleeding usually occurs after trauma.
- In some patients, even very minor trauma can cause severe and prolonged bleeding.
- For example, bleeding may continue for several days after tooth extraction.
Factor VIII
- Factor VIII has two active components.
- The large component has a molecular weight in the millions.
- The small component has a molecular weight of about 230,000.
- The small component is essential for the intrinsic clotting pathway.
- Deficiency of the small component causes classic Hemophilia A.
von Willebrand Disease
- von Willebrand disease occurs because of loss of the large component of factor VIII.
- It is a different bleeding disorder with different characteristics.
Treatment
- During severe prolonged bleeding, the most effective treatment is:
- Injection of purified factor VIII (for Hemophilia A)
- Injection of purified factor IX (for Hemophilia B)
- Factor VIII and factor IX are also available as recombinant proteins.
- These treatments are:
- Expensive
- Have a short half-life
- Therefore, they are not easily available to many patients, especially in economically disadvantaged countries.
Key Concept
- Hemophilia is an X-linked recessive bleeding disorder. Hemophilia A (85%) results from factor VIII deficiency, while Hemophilia B (15%) results from factor IX deficiency. Bleeding severity depends on the degree of deficiency and usually occurs after trauma. Treatment consists of replacement with factor VIII or factor IX, including recombinant products.

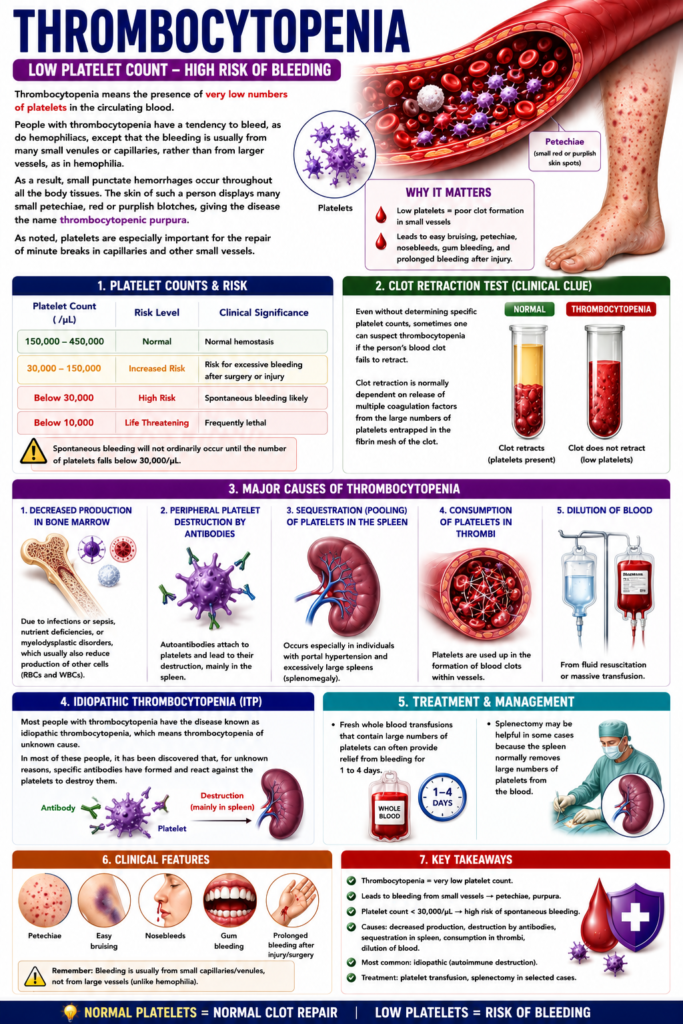
THROMBOCYTOPENIA
- Thrombocytopenia means a very low number of platelets in the circulating blood.
- People with thrombocytopenia have an increased tendency to bleed.
- Unlike hemophilia, the bleeding usually occurs from:
- Small venules
- Capillaries
- Therefore, many small pinpoint hemorrhages develop throughout the body tissues.
- The skin shows many small petechiae.
- Petechiae appear as red or purplish spots (blotches).
- Because of these skin changes, the condition is called thrombocytopenic purpura.
- Platelets are especially important for repairing tiny breaks in capillaries and other small blood vessels.
Platelet Count and Bleeding Risk
- The normal platelet count is 150,000–450,000/μL.
- A platelet count below 30,000/μL increases the risk of excessive bleeding after surgery or injury.
- Spontaneous bleeding usually does not occur until the platelet count falls below 30,000/μL.
- A platelet count of about 10,000/μL is often life-threatening.
Clot Retraction
- Even without measuring the platelet count, thrombocytopenia may be suspected if the blood clot fails to retract.
- Normal clot retraction depends on platelets trapped within the fibrin meshwork.
- These platelets release multiple coagulation factors that help the clot retract.
Major Causes of Thrombocytopenia
- (1) Decreased platelet production in the bone marrow
- Due to:
- Infections or sepsis
- Nutrient deficiencies
- Myelodysplastic disorders
- These conditions usually also reduce red blood cells (RBCs) and white blood cells (WBCs).
- Due to:
- (2) Destruction of platelets by antibodies
- (3) Sequestration (pooling) of platelets in the spleen
- Especially in:
- Portal hypertension
- Splenomegaly (enlarged spleen)
- Especially in:
- (4) Consumption of platelets in thrombi
- (5) Dilution of blood
- Due to:
- Fluid resuscitation
- Massive blood transfusion
- Due to:
Idiopathic Thrombocytopenia
- Most patients have idiopathic thrombocytopenia, meaning the cause is unknown.
- In many of these patients, antibodies are formed against platelets.
- These antibodies destroy the platelets.
Treatment
- Fresh whole blood transfusion containing large numbers of platelets can reduce bleeding for about 1–4 days.
- Splenectomy (removal of the spleen) may help in some patients.
- This is because the spleen normally removes many platelets from the blood.
Key Concept
- Thrombocytopenia is a deficiency of platelets that causes bleeding from small blood vessels, resulting in petechiae and thrombocytopenic purpura. Bleeding risk increases when platelet counts fall below 30,000/μL, and counts around 10,000/μL can be fatal. Major causes include decreased platelet production, immune destruction, splenic sequestration, platelet consumption, and dilution. Treatment includes platelet-containing blood transfusion and, in selected cases, splenectomy.
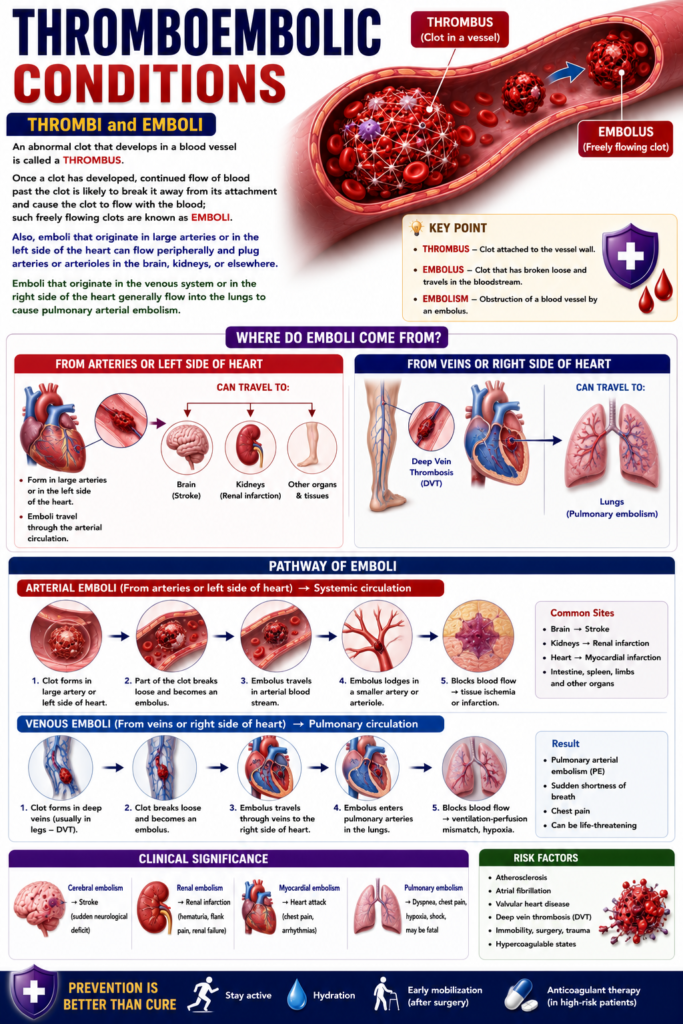
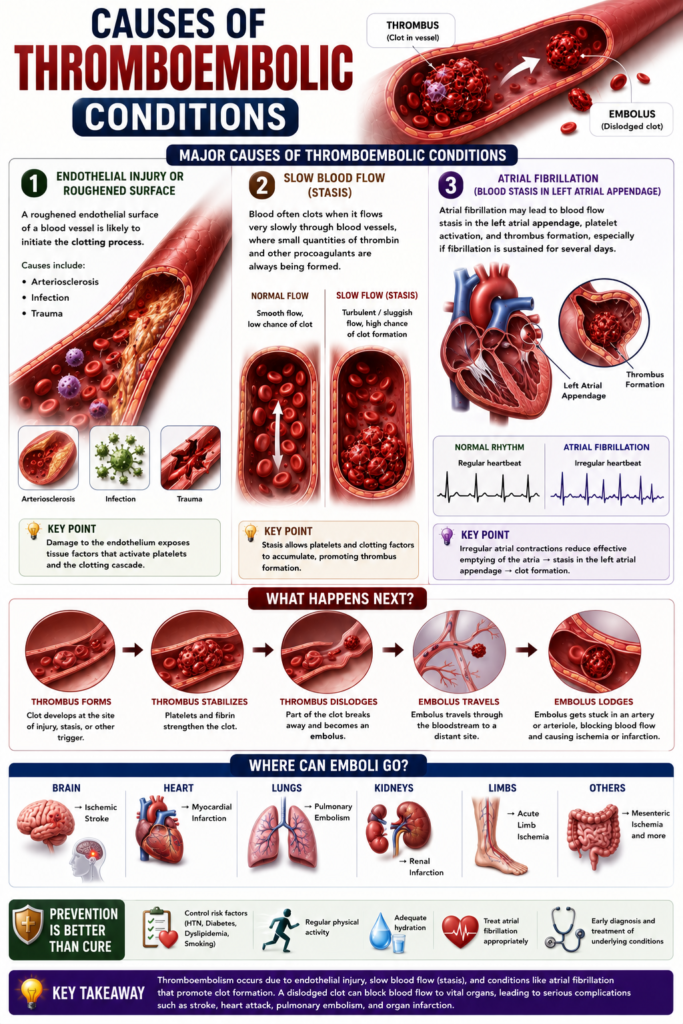
THROMBOEMBOLIC CONDITIONS
Thrombi and Emboli
- An abnormal blood clot formed inside a blood vessel is called a thrombus.
- Once a thrombus forms, the flowing blood may detach it from the vessel wall.
- The detached clot travels with the bloodstream.
- A freely circulating clot is called an embolus (emboli).
- Emboli that originate in large arteries or the left side of the heart can travel through the arterial circulation.
- These emboli may block arteries or arterioles in:
- Brain
- Kidneys
- Other organs
- Emboli that originate in the venous system or the right side of the heart usually travel to the lungs.
- They can cause pulmonary arterial embolism.
Key Concept
- A thrombus is an abnormal clot formed inside a blood vessel. If it detaches, it becomes an embolus. Arterial emboli from the left heart or large arteries can block organs such as the brain and kidneys, whereas venous or right-heart emboli usually travel to the lungs and cause pulmonary arterial embolism.
Causes of Thromboembolic Conditions
- The major causes of thromboembolic conditions include the following:
1. Roughened Endothelial Surface
- A rough or damaged endothelial surface can start the blood-clotting process.
- This may occur because of:
- Arteriosclerosis
- Infection
- Trauma
2. Slow Blood Flow
- Blood is more likely to clot when it flows very slowly through blood vessels.
- This is because small amounts of thrombin and other procoagulants are continuously being formed.
- During slow blood flow, these substances accumulate and promote clot formation.
3. Atrial Fibrillation
- Atrial fibrillation can cause stagnation (stasis) of blood in the left atrial appendage.
- This promotes platelet activation.
- It also promotes thrombus formation.
- The risk is greater when atrial fibrillation continues for several days.
- After the thrombus forms, it may break loose (become dislodged).
- The detached clot can travel as an embolus.
- It may block blood vessels in:
- Peripheral circulation
- Cerebral circulation
- Blockage of cerebral circulation can cause a stroke.
Key Concept
- Thromboembolic conditions commonly result from endothelial injury, slow blood flow, or atrial fibrillation. These factors promote thrombus formation, and if the clot detaches, it becomes an embolus that can obstruct blood vessels, including cerebral arteries, leading to stroke.
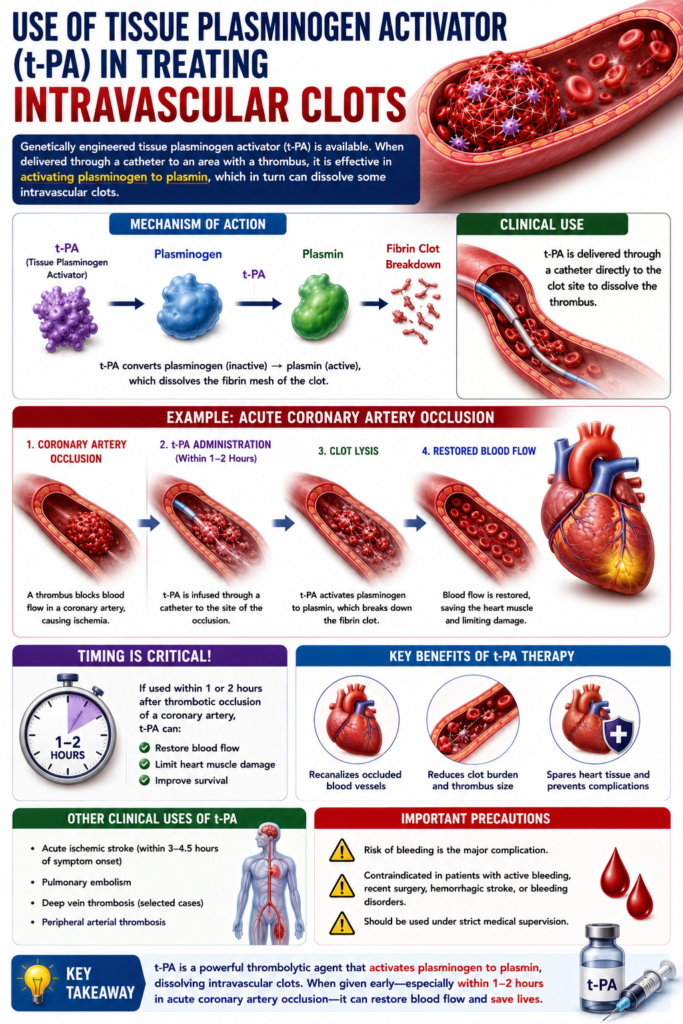
Use of Tissue Plasminogen Activator in Treating Intravascular Clots
- Genetically engineered tissue plasminogen activator (t-PA) is available.
- t-PA can be delivered through a catheter directly to the site of a thrombus.
- t-PA activates plasminogen into plasmin.
- Plasmin dissolves the intravascular blood clot.
- If t-PA is given within 1–2 hours after a thrombotic blockage of a coronary artery, it can often prevent serious damage to the heart.
Key Concept
- Tissue plasminogen activator (t-PA) is a clot-dissolving drug that converts plasminogen into plasmin. When administered early through a catheter to a thrombus, it can dissolve intravascular clots and significantly reduce heart damage after coronary artery occlusion.
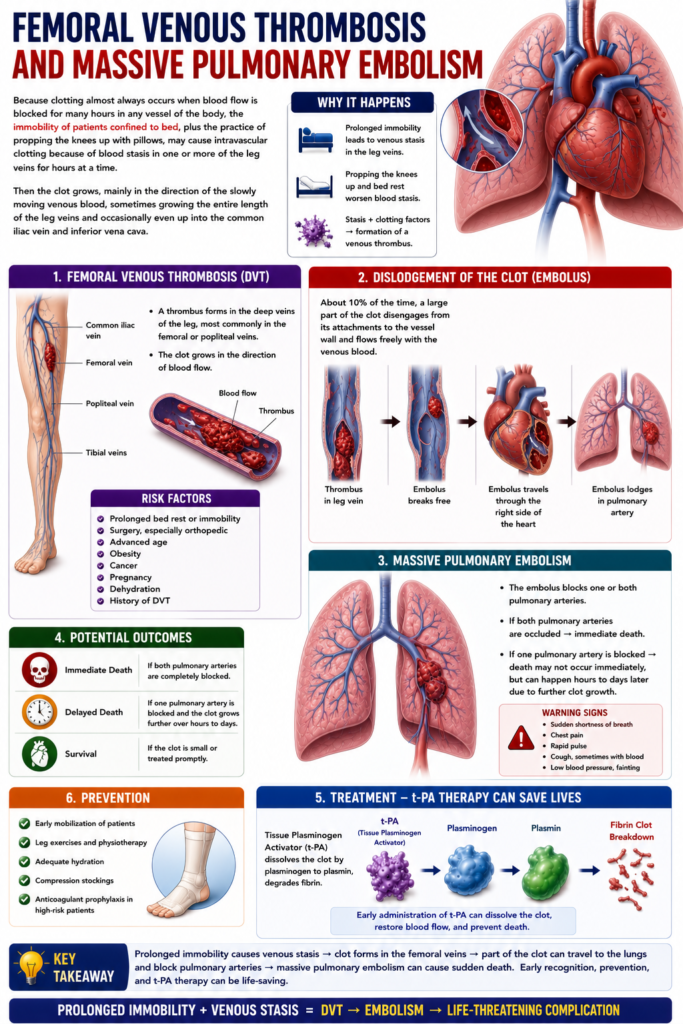
FEMORAL VENOUS THROMBOSIS AND MASSIVE PULMONARY EMBOLISM
- Blood clotting usually occurs when blood flow is blocked for many hours in a blood vessel.
- Patients who remain confined to bed (immobile) are at increased risk of clot formation.
- Keeping the knees propped up with pillows can also slow blood flow in the leg veins.
- Slow blood flow (blood stasis) in the leg veins for many hours can cause intravascular clot formation.
- The clot usually grows in the direction of the slowly flowing venous blood.
- It may extend throughout the leg veins.
- In some cases, it may extend into the common iliac vein and the inferior vena cava.
- About 10% of the time, a large part of the clot breaks away from the vessel wall.
- The detached clot travels through the venous blood.
- It passes through the right side of the heart.
- It then enters the pulmonary arteries.
- This causes massive blockage of the pulmonary arteries, called massive pulmonary embolism.
- If the clot blocks both pulmonary arteries, death occurs immediately.
- If only one pulmonary artery is blocked, the patient may survive initially.
- However, death may occur within a few hours to several days due to continued growth of the clot in the pulmonary vessels.
- Treatment with tissue plasminogen activator (t-PA) can save the patient’s life.
Key Concept
- Prolonged immobility causes blood stasis in the leg veins, leading to femoral venous thrombosis. A detached clot can travel through the right heart to the pulmonary arteries, causing massive pulmonary embolism. Complete blockage of both pulmonary arteries is usually fatal, while early t-PA therapy can be lifesaving.
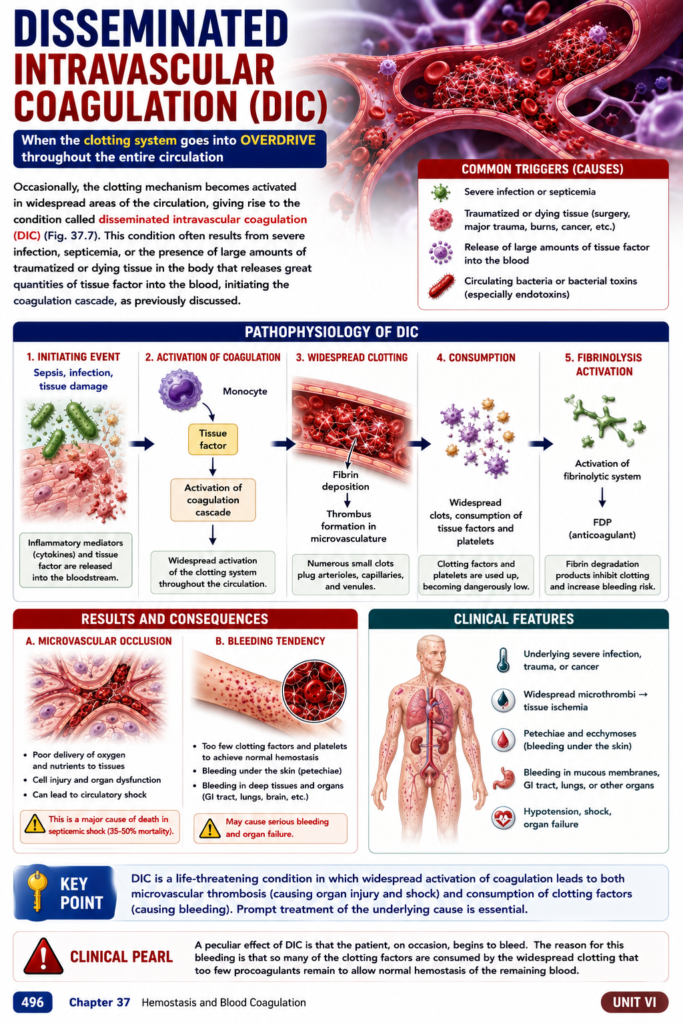
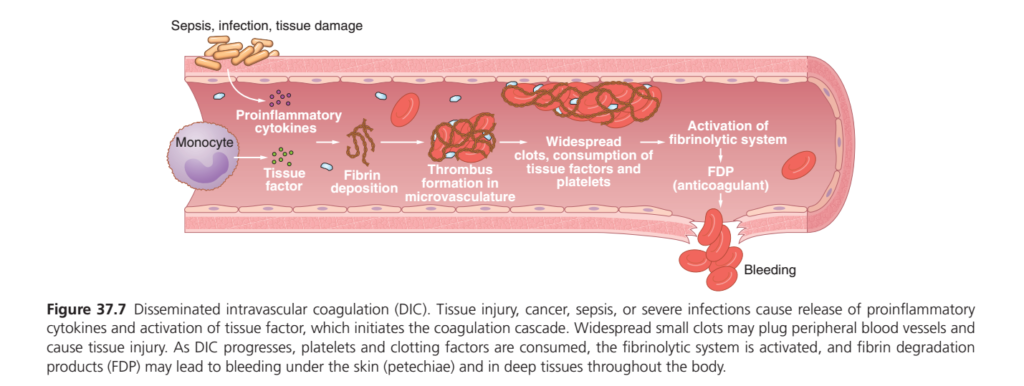
DISSEMINATED INTRAVASCULAR COAGULATION (DIC)
- Disseminated intravascular coagulation (DIC) occurs when the blood-clotting mechanism becomes activated throughout the circulation.
- Figure 37.7 illustrates DIC.
- DIC commonly results from:
- Severe infection
- Septicemia
- Large amounts of injured or dying tissue
- These conditions release large amounts of tissue factor into the blood.
- Tissue factor activates the coagulation cascade.
- As a result, many small blood clots form throughout the circulation.
- These clots are usually small but very numerous.
- They block many small peripheral blood vessels.
- DIC occurs especially in patients with widespread septicemia.
- In septicemia, circulating bacteria or bacterial toxins, especially endotoxins, activate the clotting mechanism.
- Blockage of small peripheral blood vessels reduces the delivery of oxygen and nutrients to tissues.
- This can cause tissue injury.
- It can also lead to circulatory shock.
- Septicemic shock is fatal in about 35%–50% of patients.
Figure 37.7
- Sepsis, severe infection, cancer, or tissue injury causes:
- Release of proinflammatory cytokines
- Activation of tissue factor
- This starts the coagulation cascade.
- Small clots form throughout the microvasculature.
- These clots block peripheral blood vessels.
- As DIC progresses:
- Platelets are consumed
- Clotting factors are consumed
- The fibrinolytic system is activated
- Fibrin degradation products (FDPs) are produced
- FDPs act as anticoagulants.
- This can cause bleeding under the skin (petechiae).
- It can also cause bleeding in deep tissues throughout the body.
Bleeding in DIC
- A patient with DIC may begin to bleed.
- This occurs because large amounts of clotting factors are consumed during widespread clot formation.
- As a result, too few procoagulants remain.
- Therefore, normal hemostasis cannot occur.
Key Concept
- Disseminated intravascular coagulation (DIC) is widespread activation of the coagulation cascade, usually triggered by severe infection, septicemia, or extensive tissue damage. Numerous small clots block the microcirculation, causing tissue injury and shock. As platelets and clotting factors are consumed and fibrinolysis produces anticoagulant FDPs, the patient develops a paradoxical bleeding tendency despite extensive clot formation.
Disseminated Intravascular Coagulation (DIC) – Guyton Figure 37.7
Easiest & Most Conceptual Summary
One-Line Concept
DIC is a dangerous condition in which the body forms thousands of tiny blood clots throughout the bloodstream. This uses up platelets and clotting factors, so eventually the patient starts bleeding everywhere.
Easy Memory:
Too Much Clotting → Clotting Factors Used Up → Severe Bleeding
The Big Story (Easy Understanding)
Normally,
👉 A clot forms only where a blood vessel is injured.
In DIC, the body becomes confused.
Instead of making one clot, it starts making hundreds or thousands of tiny clots everywhere in the blood vessels.
Result
Initially
🩸 Too much clotting
↓
Later
🩸 No clotting factors left
↓
Severe bleeding
This is why DIC is called
“Clotting and bleeding at the same time.”
Step 1: Trigger (What Starts DIC?) 🚨
The figure shows several causes:
- Sepsis (most common cause)
- Severe infection
- Major tissue injury/trauma
- Cancer
These conditions stimulate immune cells (especially monocytes) to release:
- Pro-inflammatory cytokines
- Tissue Factor (Factor III)
Easy Concept
Imagine someone accidentally presses the “Clot Everywhere” button.
Step 2: Tissue Factor Activates the Clotting Cascade ⚡
The released Tissue Factor starts the coagulation cascade.
Instead of clotting at one injured site,
the cascade becomes active throughout the circulation.
Easy Concept
Normally:
One repair crew repairs one hole.
In DIC:
Repair crews start building walls on every road.
Step 3: Fibrin Deposition 🕸️
Thrombin converts fibrinogen into fibrin.
Fibrin starts depositing inside many small blood vessels.
Result
Tiny fibrin strands appear everywhere.
Step 4: Microvascular Thrombi Form 🩸
These fibrin strands trap platelets and blood cells.
Many tiny clots form inside small blood vessels.
These are called:
Microthrombi
Easy Concept
Imagine thousands of tiny traffic jams inside small roads.
Step 5: Blood Supply Becomes Blocked 🚫
These tiny clots block small blood vessels.
Organs receive less oxygen.
Possible organ damage:
❤️ Heart
🧠 Brain
🫁 Lungs
🩺 Kidneys
Liver
Easy Concept
Like blocking water pipes throughout a city.
Step 6: Platelets and Clotting Factors Get Used Up 📉
Making thousands of clots consumes:
- Platelets
- Fibrinogen
- Clotting factors
Eventually,
there are not enough clotting materials left.
This is called:
Consumption Coagulopathy
Easy Concept
Imagine spending all your money on small repairs.
Now you have nothing left for a real emergency.
Step 7: Fibrinolytic System is Activated ✂️
The body now tries to remove the abnormal clots.
It activates:
Fibrinolysis
Plasmin breaks fibrin into:
Fibrin Degradation Products (FDPs)
Step 8: FDPs Prevent Clotting 🚫
FDPs have an anticoagulant effect.
They interfere with normal clot formation.
Now the patient cannot clot properly.
Step 9: Severe Bleeding 🩸
Since
✔ Platelets are exhausted
✔ Clotting factors are depleted
✔ FDPs inhibit clotting
The patient begins bleeding from:
- IV sites
- Nose
- Gums
- Surgical wounds
- Skin (petechiae and purpura)
- Internal organs
Easy Concept
The body first makes too many clots, then cannot make any useful clot.
Complete Flow Chart
Sepsis / Infection / Trauma / Cancer
↓
Monocytes release cytokines
↓
Tissue Factor released
↓
Coagulation cascade activated
↓
Thrombin formation
↓
Fibrin deposition
↓
Microvascular thrombi
↓
Platelets & clotting factors consumed
↓
Consumption coagulopathy
↓
Fibrinolysis activated
↓
FDPs produced
↓
Anticoagulation
↓
Severe bleedingEasy Story (Remember Forever)
Imagine a city.
🚨 1. False emergency alarm → Sepsis or trauma
👷 2. Workers start repairing every road → Clotting everywhere
🚗 3. Roads become blocked → Tiny clots
💰 4. Construction materials run out → Platelets and clotting factors used up
🧹 5. Cleanup teams remove roads → Fibrinolysis
❌ 6. Roads become too weak → Severe bleeding
High-Yield Exam Table
| Step | Event | Result |
|---|---|---|
| 1 | Sepsis/trauma/cancer | Tissue Factor release |
| 2 | Coagulation activated | Thrombin production |
| 3 | Fibrin deposition | Small clots form |
| 4 | Microthrombi | Small vessels blocked |
| 5 | Platelets & clotting factors consumed | Consumption coagulopathy |
| 6 | Fibrinolysis activated | FDPs formed |
| 7 | FDPs inhibit clotting | Bleeding develops |
Why Does DIC Cause Both Clotting and Bleeding?
| Early Stage | Late Stage |
|---|---|
| Excessive clot formation | Excessive bleeding |
| Many fibrin clots | Platelets depleted |
| Microvascular thrombosis | Clotting factors depleted |
| Organ ischemia | FDPs prevent new clot formation |
Easy Memory
Early = Clotting
Late = Bleeding
Clinical Features of DIC
Due to Microthrombi (Clotting)
- Organ ischemia
- Kidney injury
- Respiratory distress
- Stroke-like symptoms
- Shock
Due to Bleeding
- Petechiae (small skin hemorrhages)
- Purpura (larger skin hemorrhages)
- Gum bleeding
- Nosebleeds
- Bleeding from IV or surgical sites
- Internal bleeding
Easy Mnemonic
“DIC = DIE”
- D = Diffuse (widespread) clotting
- I = Ischemia (blocked blood supply)
- E = Excessive bleeding (after clotting factors are consumed)
Quick Exam Pearls
- Most common trigger: Sepsis.
- Tissue Factor (Factor III) initiates widespread coagulation.
- Microvascular thrombi block small vessels and can cause multi-organ damage.
- Consumption coagulopathy occurs because platelets and clotting factors are used up.
- Fibrinolysis produces Fibrin Degradation Products (FDPs), which further impair clotting.
- DIC is often described as “widespread clotting followed by widespread bleeding.”
Final Concept in One Sentence
Disseminated Intravascular Coagulation (DIC) is a life-threatening disorder in which sepsis, severe infection, trauma, or cancer triggers widespread Tissue Factor release and clot formation throughout the circulation, consuming platelets and clotting factors; subsequent fibrinolysis generates FDPs that inhibit clotting, resulting in simultaneous microvascular thrombosis, organ damage, and severe bleeding.