


- Diuretics increase the amount of urine produced by the kidneys.
- Most diuretics also increase the excretion of solutes, especially sodium (Na⁺) and chloride (Cl⁻).
- Most clinically used diuretics work by decreasing sodium reabsorption in the renal tubules.
- Decreased sodium reabsorption causes natriuresis (increased sodium excretion).
- Decreased sodium reabsorption also causes diuresis (increased water excretion).
- Water excretion increases because sodium remaining inside the renal tubules holds water by osmotic effect, reducing water reabsorption.
- Sodium reabsorption also affects the reabsorption of other solutes.
- Therefore, many diuretics increase the urinary excretion of:
- Potassium (K⁺)
- Chloride (Cl⁻)
- Magnesium (Mg²⁺)
- Calcium (Ca²⁺)
Clinical Use of Diuretics
- The most common use of diuretics is to reduce extracellular fluid (ECF) volume.
- Diuretics are mainly used in diseases associated with:
- Edema
- Hypertension
- Loss of sodium from the body mainly decreases extracellular fluid volume.
- Therefore, diuretics are commonly given in conditions where extracellular fluid volume is increased.
Effect of Diuretics on Urine Output
- Some diuretics can increase urine output by more than 20 times within a few minutes after administration.
- In most cases, the increased excretion of salt and water lasts only a few days.
- The effect decreases because the body activates compensatory mechanisms after extracellular fluid volume falls.
- Figure 32.1 shows these compensatory mechanisms.
Compensatory Mechanisms
- A decrease in extracellular fluid volume may:
- Reduce arterial pressure.
- Reduce glomerular filtration rate (GFR).
- Increase renin secretion.
- Increase angiotensin II (Ang II) formation.
- Together, these responses gradually oppose the long-term effect of diuretics on urine output.
Steady-State Response
- Eventually, urine output again becomes equal to fluid intake.
- This steady state occurs after arterial pressure and extracellular fluid volume have decreased.
- These reductions help relieve:
- Hypertension
- Edema
- These are the conditions for which diuretics are originally prescribed.
Different Classes of Diuretics
- Different diuretics have different mechanisms of action.
- They inhibit tubular reabsorption at different parts of the nephron.
- Table 32.1 shows:
- The general classes of diuretics.
- Their mechanisms of action.
- Their sites of action in the renal tubules.
KEY CONCEPT
- Diuretics increase urine production mainly by reducing sodium reabsorption.
- Reduced sodium reabsorption causes natriuresis and diuresis.
- They also increase the excretion of potassium, chloride, magnesium, and calcium.
- Their major clinical use is to treat edema and hypertension by reducing extracellular fluid volume.
- Their long-term effect decreases because compensatory mechanisms restore urine output to match fluid intake.
- Figure 32.1 illustrates the compensatory mechanisms.
- Table 32.1 summarizes the classes of diuretics, their mechanisms, and their nephron sites of action.
This figure explains what happens after a person starts taking a diuretic (“water pill”). It shows two important changes over time:
- Top Graph: What happens to sodium (Na⁺) excretion
- Bottom Graph: What happens to extracellular fluid (ECF) volume
The easiest way to understand this figure is to remember just one principle:
Diuretics make the kidneys lose more sodium. Water follows sodium. Therefore, the body loses extracellular fluid.
Now let’s explain every line, every label, every shaded area, and every change step by step.
Step 1: The X-axis (Horizontal Axis)
Time (days)
- Shows what happens over several days.
- Before Day 0 = No diuretic
- Day 0 = Diuretic therapy starts
- After Day 0 = Body begins adapting to the diuretic.
Think of it like this:
Before Day 0
Normal life
↓
Day 0
Start taking a diuretic
↓
Next several days
Body adjusts itselfStep 2: The Blue Shaded Area
At the top you see a blue shaded rectangle labeled
Diuretic therapy
This means
During this whole shaded period, the patient is taking the diuretic medicine continuously.
The medicine is ON throughout this shaded area.
Step 3: The Two Vertical Dashed Lines
There are two dashed vertical lines.
First dashed line (Day 0)
This is the most important line.
It means
The patient starts taking the diuretic here.
Everything before this line
= No medicine.
Everything after this line
= Medicine is working.
Second dashed line (End of graph)
This simply marks the end of the observation period.
Nothing special happens here.
It only shows the graph stops.
TOP GRAPH
What is the Y-axis?
It says
Sodium excretion or sodium intake (mEq/day)
This means
How much sodium
- enters the body (food)
- leaves the body (urine)
each day.
The Blue Dashed Horizontal Line
This line represents
Sodium Intake
The person eats
about
100 mEq sodium/dayevery day.
Notice something very important.
The blue dashed line is perfectly flat.
Why?
Because
The person is eating the same amount of salt every day.
Nothing changes.
Monday
100
Tuesday
100
Wednesday
100
Thursday
100
Every day
100So the intake line never moves.
The Red Line Before Day 0
Before taking the medicine
The red line is exactly on top of the blue line.
Why?
Because
Normal kidneys maintain sodium balance.
If you eat
100 mEq sodiumthe kidneys excrete
100 mEq sodiumTherefore
Intake = ExcretionNo sodium is stored.
No sodium is lost.
The body is perfectly balanced.
This is called
Sodium balance
Eat 100
↓
Lose 100
↓
BalanceDay 0 (Medicine Starts)
Suddenly
The red line shoots upward.
Why?
Because the diuretic blocks sodium reabsorption.
Instead of keeping sodium,
the kidneys now throw much more sodium into the urine.
Imagine
Normally
Eat 100
↓
Urine 100After diuretic
Eat 100
↓
Urine 210Now
Excretion > IntakeThe body is losing sodium.
This is called
Negative sodium balance
Why Does the Red Line Rise So High?
Because
Diuretics suddenly increase sodium excretion.
The kidneys cannot reabsorb sodium normally.
So
lots of sodium leaves.
Water follows sodium.
Therefore
lots of water also leaves.
Why Doesn’t the Red Line Stay High Forever?
This is the key concept.
The body does not like losing sodium continuously.
So it activates many compensatory mechanisms.
Examples include
- RAAS activation
- Increased aldosterone
- Increased sympathetic activity
- Reduced GFR
- Increased tubular sodium reabsorption
These mechanisms try to save sodium.
Therefore
every day
less sodium is lost than the previous day.
That is why the red curve slowly falls.
Think of it like this
Day 1
Excrete 210Day 2
170Day 3
150Day 4
120Day 5
105Eventually
100Again.
Why Does It Return to 100?
Because the body reaches a new steady state.
The kidneys adjust until
Sodium intake
=
Sodium excretionagain.
Notice
The diuretic is still being taken.
But
the body has adapted.
This is called
New sodium balance
Bottom Graph
Now look at the second graph.
Its Y-axis says
Extracellular Fluid Volume (Liters)
This means
How much fluid exists outside the body’s cells.
Normal value here is about
14 LBefore Day 0
The red line is flat.
The ECF volume stays constant.
Because
No sodium is being lost.
Water is not leaving.
Everything is balanced.
After Day 0
As soon as sodium leaves,
water follows sodium.
Remember the golden rule:
Where sodium goes, water goes.
So
The kidneys lose
Sodium
↓
Water
↓
ECF volume decreasesThat is why the red line starts falling.
Why Does It Fall Slowly?
Fluid is not lost all at once.
Each day
a little sodium is lost
↓
water follows
↓
ECF gradually decreases.Imagine
Day 0
14 LDay 1
13.8Day 2
13.5Day 3
13.3Day 4
13.1Day 5
13.0Why Does the Line Become Flat Again?
Because
Eventually
the kidneys stop losing extra sodium.
Now
Intake = Excretionagain.
Since sodium balance has returned,
water balance also returns.
Therefore
The ECF volume stops falling.
It becomes stable.
Notice
It stabilizes at
13 Linstead of
14 LSo
The body has a new normal volume, but it is 1 liter lower than before.Very Important Concept
Many students ask
“If sodium excretion returns to normal, why doesn’t ECF return to 14 L?”
Answer:
Because the body has already lost sodium and water.
The new, lower ECF volume activates compensatory mechanisms (such as RAAS and sympathetic nervous system), allowing the kidneys to match sodium excretion to intake at this lower volume. Thus, sodium balance is restored, but around a reduced ECF volume.
Relationship Between Both Graphs
The two graphs are directly connected.
Diuretic starts
↓
Kidneys lose sodium
↓
Water follows sodium
↓
Urine increases
↓
ECF volume falls
↓
Body activates compensatory mechanisms
↓
Kidneys conserve sodium
↓
Sodium excretion gradually returns to intake
↓
ECF volume becomes stable at a lower levelOne-Line Explanation of Every Line
| Graph Part | Meaning |
|---|---|
| Blue shaded area | Period during which the patient is taking the diuretic continuously. |
| First vertical dashed line | Diuretic therapy begins (Day 0). |
| Second vertical dashed line | End of the observation period. |
| Blue dashed horizontal line | Sodium intake remains constant at about 100 mEq/day. |
| Red line before Day 0 | Sodium excretion equals sodium intake (normal sodium balance). |
| Sharp rise in red line | Diuretic causes a sudden increase in sodium excretion (natriuresis). |
| Gradual fall of red line | The body activates compensatory mechanisms that reduce sodium loss over several days. |
| Flat red line at the end | Sodium excretion again equals sodium intake, establishing a new steady-state sodium balance. |
| Bottom red line before Day 0 | Normal extracellular fluid (ECF) volume of about 14 L. |
| Falling bottom red line | Sodium and water loss decrease ECF volume progressively. |
| Final flat bottom line | ECF volume stabilizes at a lower level (about 13 L) because sodium balance has been restored at this reduced volume. |
KEY CONCEPT (Exam Point)
- Before diuretics: Sodium intake = sodium excretion → ECF volume remains constant.
- Immediately after starting a diuretic: Sodium excretion rises sharply above intake → negative sodium balance → water follows sodium → ECF volume decreases.
- After several days: Compensatory mechanisms (RAAS, sympathetic nervous system, etc.) reduce sodium loss until sodium excretion again equals sodium intake.
- Final result: Sodium balance is restored, but at a lower extracellular fluid volume. This reduced ECF volume is the therapeutic effect of diuretics in conditions such as edema and hypertension.
Osmotic Diuretics Decrease Water Reabsorption By Increasing Osmotic Pressure of Tubular Fluid
- Substances such as urea, mannitol, and sucrose are filtered by the glomerular capillaries.
- These substances are not easily reabsorbed by the renal tubules.
- Their presence greatly increases the concentration of osmotically active molecules in the tubular fluid.
- The increased osmotic pressure of the tubular fluid reduces water reabsorption.
- As a result, large amounts of tubular fluid are flushed into the urine.
- Large urine volumes also occur in diseases where excess solutes remain in the tubular fluid.
- One example is diabetes mellitus.
- In diabetes mellitus, blood glucose concentration becomes very high.
- The increased filtered load of glucose exceeds the tubules’ ability to reabsorb glucose.
- This means the filtered glucose exceeds the transport maximum (Tm) for glucose.
- When plasma glucose concentration rises above about 250 mg/dL, very little of the extra glucose is reabsorbed.
- The excess glucose remains in the renal tubules.
- This glucose acts as an osmotic diuretic.
- As a result, urine flow rate increases.
- One of the hallmarks of uncontrolled diabetes mellitus is polyuria (frequent urination).
- Polyuria is balanced by increased fluid intake (polydipsia).
- Increased thirst occurs because of:
- Dehydration.
- Increased extracellular fluid osmolarity.
- Activation of the thirst mechanism.
Loop Diuretics Decrease Sodium-Chloride-Potassium Reabsorption in the Thick Ascending Loop of Henle
- Furosemide, ethacrynic acid, and bumetanide are powerful loop diuretics.
- They act mainly on the thick ascending limb of the loop of Henle.
- They block the 1-sodium, 2-chloride, 1-potassium (Na⁺-K⁺-2Cl⁻) co-transporter in the luminal membrane of epithelial cells.
- Figure 28.9 shows this transporter.
- Loop diuretics are among the most powerful clinically used diuretics.
- Blocking the Na⁺-K⁺-2Cl⁻ co-transporter increases urinary excretion of:
- Sodium.
- Chloride.
- Potassium.
- Other electrolytes.
- Water.
- This occurs for two reasons:
- (1) More solutes reach the distal nephron, where they act as osmotic agents and reduce water reabsorption.
- (2) The countercurrent multiplier system is disrupted because fewer ions are absorbed into the medullary interstitium.
- This lowers the osmolarity of the renal medullary interstitial fluid.
- Therefore, loop diuretics reduce the kidneys’ ability to:
- Concentrate urine.
- Dilute urine.
Effect on Urine Dilution
- Urinary dilution is impaired because sodium and chloride reabsorption in the loop of Henle is inhibited.
- More sodium and chloride are excreted.
- Water excretion also increases.
Effect on Urine Concentration
- Urine concentrating ability is impaired because the concentration of sodium and chloride in the renal medulla decreases.
- Renal medullary osmolarity also decreases.
- As a result, water reabsorption from the collecting ducts decreases.
- Therefore, the kidneys’ maximum concentrating ability is greatly reduced.
- Reduced medullary osmolarity also decreases water reabsorption from the descending loop of Henle.
- Because of these combined effects:
- 20% to 25% of the glomerular filtrate may be excreted in the urine.
- Under acute conditions, urine output may become about 25 times normal for a few minutes.
Effect on Calcium
- Loop diuretics also increase renal calcium excretion.
- Calcium reabsorption in the thick ascending limb mainly occurs by the passive paracellular pathway.
- This process depends on the electrochemical gradient produced by active sodium chloride transport.
- Therefore, inhibition of sodium chloride reabsorption also reduces calcium reabsorption.
- As a result, calcium excretion increases.
Effect on Potassium
- Loop diuretics inhibit the Na⁺-K⁺-2Cl⁻ co-transporter.
- They also increase fluid delivery to the distal nephron and collecting tubules.
- Therefore, potassium excretion increases.
- Significant hypokalemia may occur.
Thiazide Diuretics Inhibit Sodium-Chloride Reabsorption in the Distal Convoluted Tubule
- Chlorothiazide is an example of a thiazide diuretic.
- Thiazide diuretics act mainly on the distal convoluted tubule.
- They block the Na⁺-Cl⁻ co-transporter in the luminal membrane of tubular cells.
- Figure 28.10 shows this transporter.
- Under favorable conditions, thiazide diuretics allow a maximum of 5% of the glomerular filtrate to be excreted in the urine.
- High doses of thiazide diuretics may increase potassium excretion.
- They may cause hypokalemia.
- This occurs partly because more sodium chloride reaches the collecting tubules.
- Thiazide diuretics also activate the renin-angiotensin-aldosterone system (RAAS).
- RAAS activation occurs because sodium and fluid are lost from the body.
- Increased sodium delivery to the collecting tubules stimulates potassium secretion.
- Increased aldosterone also stimulates potassium secretion.
- Therefore, both mechanisms increase potassium excretion.
- Thiazide diuretics are among the most widely used drugs for:
- Hypertension.
- Heart failure.
- Other cardiovascular disorders.
- Multiple randomized controlled trials have shown that low-dose thiazide diuretics:
- Lower blood pressure in patients with primary hypertension.
- Reduce mortality.
- Reduce adverse cardiovascular events.
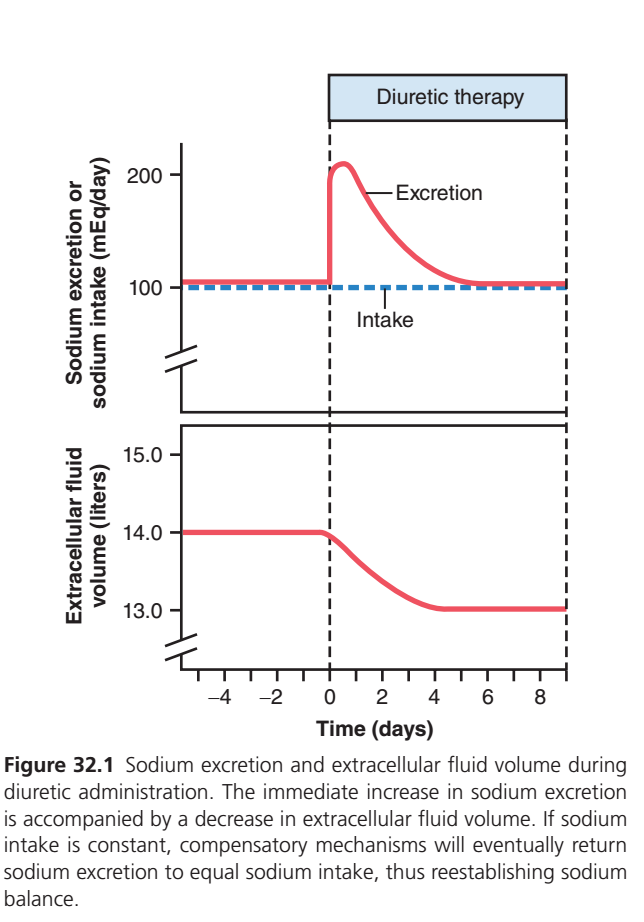
Figure 32.1
- Figure 32.1 shows the changes in sodium excretion and extracellular fluid volume during diuretic therapy.
- Diuretic administration causes an immediate increase in sodium excretion.
- Increased sodium excretion is accompanied by a decrease in extracellular fluid volume.
- If sodium intake remains constant, compensatory mechanisms gradually reduce sodium excretion.
- Eventually, sodium excretion again becomes equal to sodium intake.
- Sodium balance is therefore re-established.
Table 32.1 – Classes of Diuretics
| Class | Mechanism of Action | Site of Action |
|---|---|---|
| Osmotic diuretics (mannitol) | Increase tubular fluid osmolarity and inhibit water and solute reabsorption | Mainly proximal tubules |
| Loop diuretics (furosemide, bumetanide) | Inhibit Na⁺-K⁺-2Cl⁻ co-transporter | Thick ascending loop of Henle |
| Thiazide diuretics (hydrochlorothiazide, chlorthalidone) | Inhibit Na⁺-Cl⁻ co-transporter | Early distal tubules |
| Carbonic anhydrase inhibitors (acetazolamide) | Inhibit H⁺ secretion and HCO₃⁻ reabsorption, reducing Na⁺ reabsorption | Mainly proximal tubules |
| Mineralocorticoid receptor antagonists (spironolactone, eplerenone, finerenone) | Block aldosterone action, decrease Na⁺ reabsorption, decrease K⁺ secretion | Collecting tubules |
| Epithelial sodium channel blockers (triamterene, amiloride) | Block Na⁺ entry through epithelial sodium channels, decrease Na⁺ reabsorption, decrease K⁺ secretion | Collecting tubules |
KEY CONCEPT
- Osmotic diuretics increase urine output by raising tubular fluid osmolarity, which reduces water reabsorption.
- In diabetes mellitus, plasma glucose above about 250 mg/dL acts as an osmotic diuretic, causing polyuria and polydipsia.
- Loop diuretics block the Na⁺-K⁺-2Cl⁻ co-transporter in the thick ascending loop of Henle (Figure 28.9).
- Loop diuretics decrease both the urine-concentrating and urine-diluting abilities of the kidneys.
- Loop diuretics increase excretion of sodium, chloride, potassium, calcium, electrolytes, and water, and may cause hypokalemia.
- Thiazide diuretics block the Na⁺-Cl⁻ co-transporter in the distal convoluted tubule (Figure 28.10).
- Thiazide diuretics can cause hypokalemia by increasing sodium delivery to the collecting tubules and activating RAAS.
- Figure 32.1 demonstrates that compensatory mechanisms eventually return sodium excretion to equal sodium intake.
- Table 32.1 summarizes the classes of diuretics, their mechanisms of action, and their nephron sites of action.
Carbonic Anhydrase Inhibitors Block Sodium Bicarbonate Reabsorption
- Acetazolamide inhibits the enzyme carbonic anhydrase.
- Carbonic anhydrase is essential for the reabsorption of bicarbonate (HCO₃⁻) in the renal tubules.
- Details of this mechanism are discussed in Chapter 31.
- Carbonic anhydrase is especially abundant in the proximal tubule.
- Therefore, the proximal tubule is the primary site of action of carbonic anhydrase inhibitors.
- Some carbonic anhydrase is also present in other tubular cells.
- It is present in the intercalated cells of the collecting tubule.
- In the proximal tubule, H⁺ secretion and HCO₃⁻ reabsorption are coupled with sodium (Na⁺) reabsorption.
- This coupling occurs through the Na⁺-H⁺ counter-transporter in the luminal membrane.
- Therefore, decreasing HCO₃⁻ reabsorption also decreases Na⁺ reabsorption.
- Blocking sodium and bicarbonate reabsorption causes these ions to remain in the tubular fluid.
- Sodium and bicarbonate then act as osmotic diuretics.
- As a result, water excretion increases.
- A disadvantage of carbonic anhydrase inhibitors is that they cause acidosis.
- Acidosis occurs because excessive HCO₃⁻ is lost in the urine.
Mineralocorticoid Receptor Antagonists Decrease Sodium Reabsorption and Potassium Secretion in the Collecting Tubules
- Spironolactone, eplerenone, and finerenone are mineralocorticoid receptor antagonists.
- They compete with aldosterone for receptor-binding sites.
- These receptors are located in the epithelial cells of the collecting tubule and collecting duct.
- Figure 28.12 shows this site of action.
- Blocking aldosterone receptors decreases sodium reabsorption.
- It also decreases potassium secretion in these tubular segments.
- As a result, sodium remains in the tubular fluid.
- Sodium acts as an osmotic diuretic.
- This increases the excretion of:
- Water.
- Sodium.
- These drugs also block the action of aldosterone that normally promotes potassium secretion.
- Therefore, potassium excretion decreases.
Effect on Potassium
- Mineralocorticoid receptor antagonists also move potassium from the cells into the extracellular fluid.
- In some patients, this causes excessive increases in extracellular fluid potassium concentration.
- This condition is called hyperkalemia.
- Because these drugs reduce potassium loss, they are called potassium-sparing diuretics.
- Most other diuretics increase potassium loss in the urine.
- Mineralocorticoid receptor antagonists help preserve body potassium.
Clinical Uses
- Mineralocorticoid receptor antagonists are especially useful in:
- Primary aldosteronism (excess aldosterone secretion).
- Hypertension.
- Heart failure.
- These drugs may cause hyperkalemia, especially in patients with chronic kidney disease (CKD) who have impaired potassium excretion.
- The risk of hyperkalemia is dose-dependent.
- Hyperkalemia appears to be less severe with nonsteroidal mineralocorticoid receptor antagonists such as finerenone.
- It is more common with steroidal antagonists such as spironolactone.
Epithelial Sodium Channel Blockers Decrease Sodium Reabsorption in the Collecting Tubules
- Amiloride and triamterene are epithelial sodium channel blockers.
- They inhibit sodium reabsorption and potassium secretion in the collecting tubules.
- Their effects are similar to those of spironolactone.
- However, these drugs work by a different cellular mechanism.
- They directly block the entry of sodium through the epithelial sodium channels in the luminal membrane of collecting tubule epithelial cells.
- Figure 28.12 shows this mechanism.
- Reduced sodium entry into epithelial cells decreases sodium transport across the basolateral membrane.
- This decreases the activity of the Na⁺-K⁺ ATPase pump.
- Reduced Na⁺-K⁺ ATPase activity decreases potassium transport into the epithelial cells.
- As a result, potassium secretion into the tubular fluid decreases.
- Therefore, epithelial sodium channel blockers are also potassium-sparing diuretics.
- They decrease the urinary excretion of potassium.
Clinical Uses
- Epithelial sodium channel blockers are used as potassium-sparing diuretics.
- They are used in the treatment of:
- Edema.
- Hypertension.
- These drugs are often combined with other antihypertensive medications.
- They are especially useful in patients with treatment-resistant hypertension.
- Treatment-resistant hypertension requires three or more drugs to control blood pressure.
KEY CONCEPT
- Acetazolamide inhibits carbonic anhydrase, reducing HCO₃⁻ and Na⁺ reabsorption, causing osmotic diuresis.
- Carbonic anhydrase inhibitors mainly act in the proximal tubule and may cause metabolic acidosis because of excessive bicarbonate loss.
- Spironolactone, eplerenone, and finerenone block aldosterone receptors in the collecting tubules and collecting ducts (Figure 28.12).
- Mineralocorticoid receptor antagonists decrease Na⁺ reabsorption, decrease K⁺ secretion, and are potassium-sparing diuretics.
- These drugs are useful for primary aldosteronism, hypertension, and heart failure, but may cause hyperkalemia, especially in CKD.
- Amiloride and triamterene directly block epithelial sodium channels in the collecting tubules (Figure 28.12).
- Epithelial sodium channel blockers decrease Na⁺ reabsorption, reduce Na⁺-K⁺ ATPase activity, decrease K⁺ secretion, and are also potassium-sparing diuretics.
- They are commonly used for edema, hypertension, and treatment-resistant hypertension.