


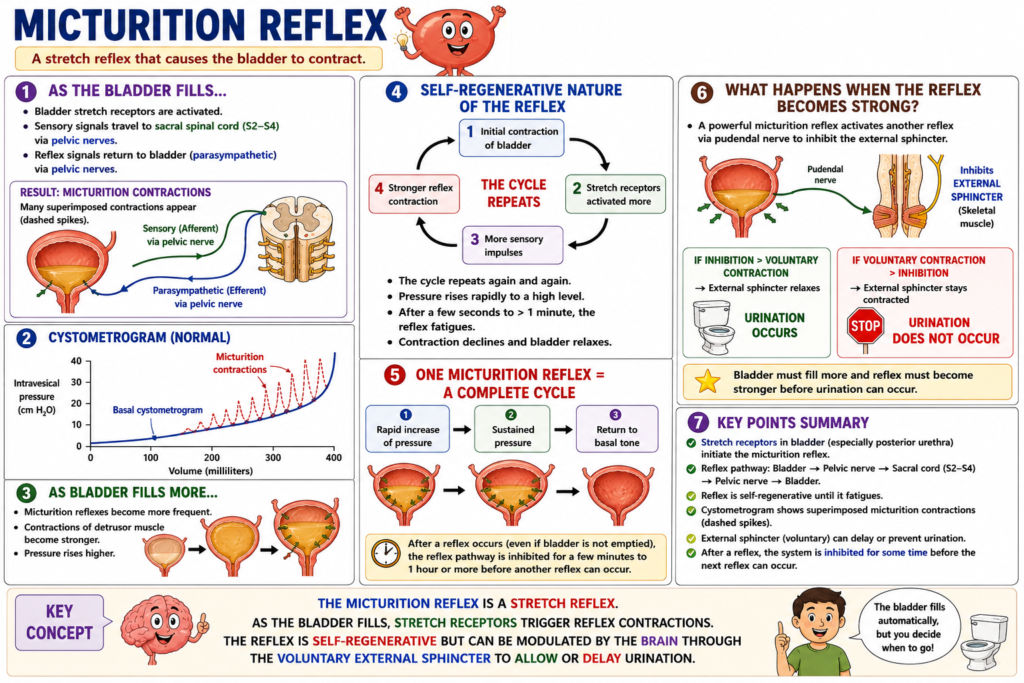
- As the bladder fills with urine, micturition contractions begin to appear.
- These contractions are produced by a stretch reflex.
- The stretch reflex is initiated by stretch receptors in the bladder wall.
- Stretch receptors in the posterior urethra are especially important.
- These receptors are strongly stimulated when the posterior urethra begins to fill with urine at higher bladder pressures.
- Sensory signals from the stretch receptors travel to the sacral segments of the spinal cord.
- These signals pass through the pelvic nerves.
- Reflex signals then return from the spinal cord to the bladder through parasympathetic fibers in the pelvic nerves.
- When the bladder is only partially filled, micturition contractions usually stop spontaneously after a short time.
- The detrusor muscle relaxes.
- Bladder pressure returns to its baseline level.
- As the bladder continues to fill, micturition reflexes occur more frequently.
- These reflexes also produce stronger contractions of the detrusor muscle.
- Once a micturition reflex begins, it becomes self-regenerative.
- Initial contraction of the bladder further stimulates the stretch receptors.
- Increased stretch receptor activity produces more sensory impulses.
- More sensory impulses cause stronger reflex contraction of the bladder.
- This cycle repeats again and again.
- The repeated cycle continues until the bladder reaches a strong contraction.
- After a few seconds to more than one minute, the self-regenerative reflex begins to fatigue.
- The micturition reflex then stops.
- The bladder relaxes.
- A complete micturition reflex consists of three phases.
- The first phase is a progressive and rapid increase in bladder pressure.
- The second phase is a period of sustained pressure.
- The third phase is a return of pressure to the basal tone of the bladder.
- If a micturition reflex occurs but does not empty the bladder, the reflex pathway becomes temporarily inhibited.
- This inhibition may last for a few minutes to more than one hour.
- After this period, another micturition reflex can occur.
- As the bladder fills further, micturition reflexes become more frequent.
- They also become more powerful.
- When the micturition reflex becomes strong enough, it triggers another reflex.
- This reflex travels through the pudendal nerves to the external sphincter.
- The reflex inhibits the external sphincter.
- If this inhibition is stronger than the voluntary constrictor signals to the external sphincter, urination occurs.
- If voluntary constrictor signals remain stronger, urination does not occur.
- The bladder then continues to fill.
- As filling continues, the micturition reflex becomes even stronger.
KEY CONCEPT
The micturition reflex is a self-regenerating spinal reflex triggered by bladder stretch receptors. As the bladder fills, stretch signals activate the detrusor muscle, causing progressively stronger contractions. Urination occurs when the micturition reflex becomes strong enough to inhibit the external sphincter and overcome voluntary control.
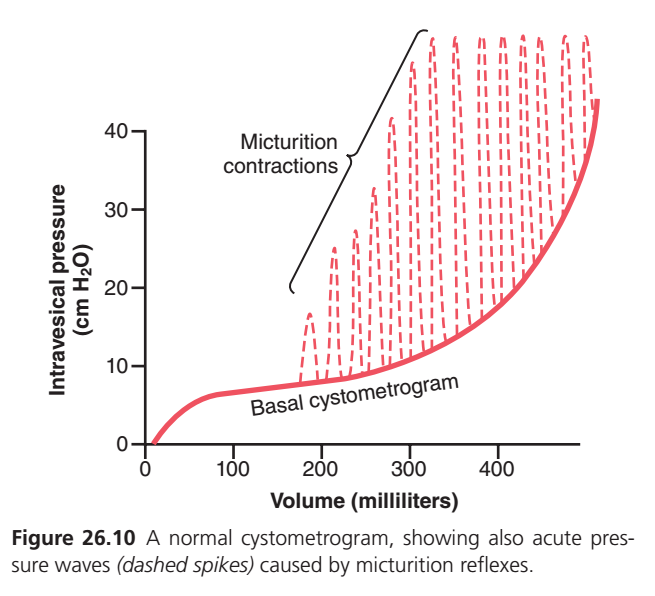
FIGURE 26.10 IN ONE MINUTE
Solid Red Line = Normal Bladder Pressure
- Urine enters the bladder.
- Bladder pressure rises slightly at first.
- Then the bladder stretches easily, so pressure stays almost constant.
- After about 300–400 mL, the bladder becomes full and pressure rises rapidly.
Dashed Red Spikes = Micturition Reflexes
- Each spike = one temporary bladder contraction.
- Caused by stretch receptors in the bladder wall.
- The bladder is trying to empty itself.
As Bladder Volume Increases
Small amount of urine
→ Small contractions
More urine
→ Bigger contractions
Very full bladder
→ Very strong contractions
Why Do Spikes Rise and Fall?
- Bladder stretches
- Reflex starts
- Detrusor contracts
- Pressure rises
- Reflex fatigues
- Bladder relaxes
- Pressure falls
One rise-and-fall = one micturition reflex.
SUPER EASY MEMORY TRICK
Red Solid Line
= How full the bladder is
Red Dotted Spikes
= How badly the bladder wants to empty
Small bladder → Small spikes 😌
Full bladder → Big spikes 😣
Very full bladder → Huge spikes 🚽
KEY CONCEPT
As the bladder fills, the background pressure increases slowly (solid line), while micturition reflex contractions become larger and more frequent (dotted spikes), creating a stronger urge to urinate.
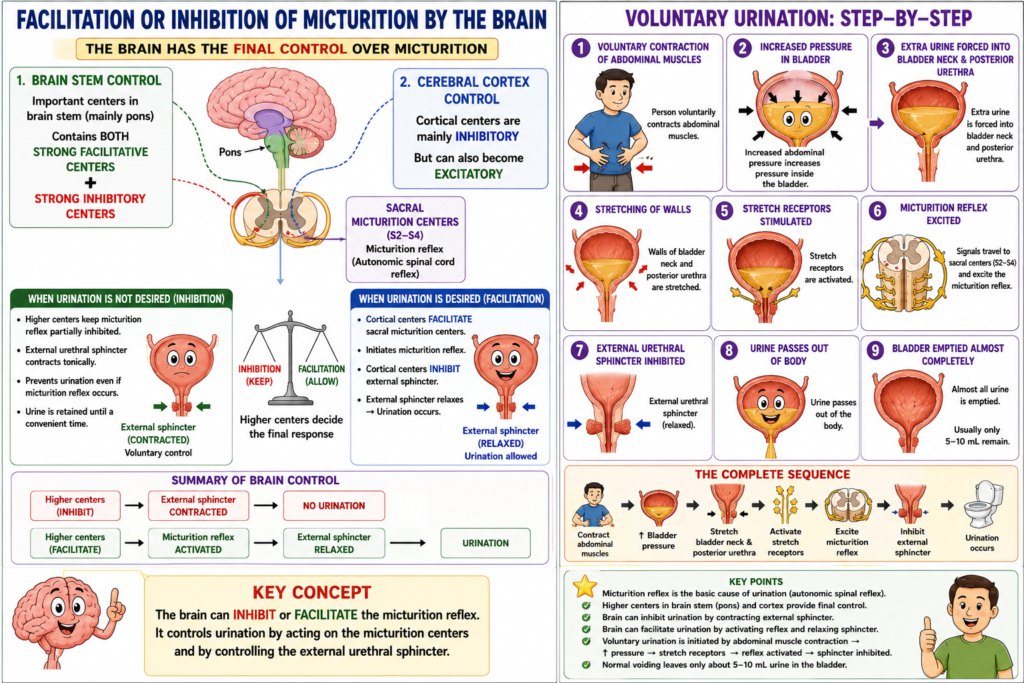
FACILITATION OR INHIBITION OF MICTURITION BY THE BRAIN
- The micturition reflex is an autonomic spinal cord reflex.
- The brain can inhibit or facilitate the micturition reflex.
- Important control centers are located in the brain stem.
- These centers are mainly located in the pons.
- The brain stem contains both strong facilitative and inhibitory centers.
- Additional control centers are present in the cerebral cortex.
- The cortical centers are mainly inhibitory.
- However, the cortical centers can also become excitatory.
- The micturition reflex is the basic cause of urination.
- However, higher brain centers provide the final control over micturition.
- The higher centers normally keep the micturition reflex partially inhibited.
- This inhibition remains in effect until urination is desired.
- The higher centers can prevent urination even when the micturition reflex occurs.
- This is achieved by tonic contraction of the external bladder sphincter.
- The external sphincter remains contracted until a convenient time for urination.
- When it is time to urinate, the cortical centers facilitate the sacral micturition centers.
- This helps initiate the micturition reflex.
- At the same time, the cortical centers inhibit the external urinary sphincter.
- This allows urination to occur.
VOLUNTARY URINATION
- Voluntary urination is usually initiated consciously.
- First, a person voluntarily contracts the abdominal muscles.
- Contraction of the abdominal muscles increases pressure inside the bladder.
- The increased pressure forces extra urine into the bladder neck and posterior urethra.
- This causes stretching of the walls of the bladder neck and posterior urethra.
- The stretch stimulates stretch receptors.
- Activation of these receptors excites the micturition reflex.
- At the same time, the external urethral sphincter is inhibited.
- This allows urine to pass out of the body.
- Normally, almost all urine is emptied from the bladder.
- Usually, only about 5 to 10 milliliters of urine remain in the bladder after urination.
KEY CONCEPT
The brain has the final control over micturition. Higher centers can inhibit urination by keeping the external sphincter contracted or facilitate urination by activating the micturition reflex and relaxing the external sphincter. Voluntary urination occurs when abdominal muscle contraction increases bladder pressure, stimulates stretch receptors, activates the micturition reflex, and inhibits the external sphincter.
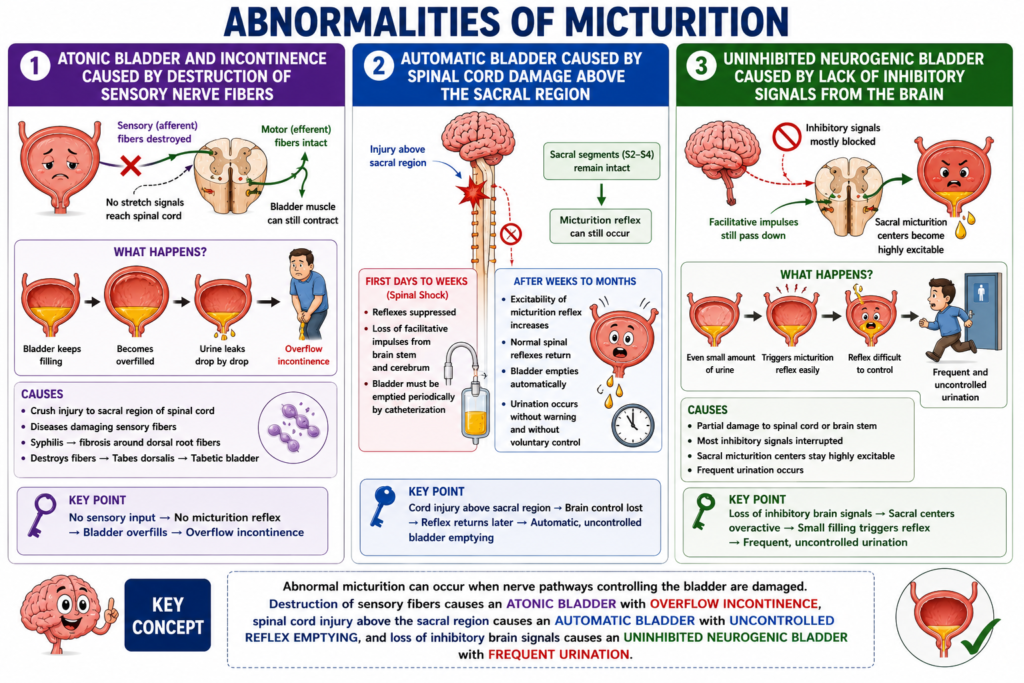
ABNORMALITIES OF MICTURITION
ATONIC BLADDER AND INCONTINENCE CAUSED BY DESTRUCTION OF SENSORY NERVE FIBERS
- The micturition reflex cannot occur if the sensory nerve fibers from the bladder to the spinal cord are destroyed.
- Destruction of these fibers prevents stretch signals from reaching the spinal cord.
- As a result, bladder filling cannot properly activate the micturition reflex.
- The person loses normal bladder control.
- This occurs even when the motor nerve fibers to the bladder remain intact.
- It also occurs even when the neural connections within the brain remain intact.
- Instead of emptying periodically, the bladder continues to fill.
- The bladder eventually reaches its maximum capacity.
- After becoming overfilled, urine leaks out through the urethra a few drops at a time.
- This condition is called overflow incontinence.
- A common cause of atonic bladder is a crush injury to the sacral region of the spinal cord.
- Some diseases can also damage the sensory nerve fibers entering the spinal cord.
- Syphilis can cause fibrosis around the dorsal root nerve fibers.
- This fibrosis can destroy the dorsal root nerve fibers.
- This condition is called tabes dorsalis.
- The resulting bladder disorder is called tabetic bladder.
AUTOMATIC BLADDER CAUSED BY SPINAL CORD DAMAGE ABOVE THE SACRAL REGION
- Automatic bladder occurs when the spinal cord is damaged above the sacral region.
- In this condition, the sacral spinal cord segments remain intact.
- The micturition reflex can still occur.
- However, the reflex is no longer controlled by the brain.
- During the first few days to several weeks after injury, micturition reflexes are usually suppressed.
- This suppression occurs because of spinal shock.
- Spinal shock results from the sudden loss of facilitative impulses from the brain stem and cerebrum.
- During this period, the bladder must be emptied periodically by catheterization.
- Catheterization prevents bladder injury caused by overstretching.
- Over time, the excitability of the micturition reflex gradually increases.
- Eventually, normal spinal micturition reflexes return.
- After the reflex returns, periodic bladder emptying occurs automatically.
- These episodes of urination occur without warning and without voluntary control.
UNINHIBITED NEUROGENIC BLADDER CAUSED BY LACK OF INHIBITORY SIGNALS FROM THE BRAIN
- Uninhibited neurogenic bladder is another abnormality of micturition.
- This condition causes frequent and relatively uncontrolled urination.
- It results from partial damage to the spinal cord or brain stem.
- The damage interrupts most of the inhibitory signals from the brain.
- Facilitative impulses continue to travel down the spinal cord.
- These impulses keep the sacral micturition centers highly excitable.
- Because of this increased excitability, even a small amount of urine can trigger the micturition reflex.
- The resulting reflex is difficult to control.
- Frequent urination occurs as a result.
KEY CONCEPT
Abnormal micturition can occur when nerve pathways controlling the bladder are damaged. Destruction of sensory fibers causes an atonic bladder with overflow incontinence, spinal cord injury above the sacral region causes an automatic bladder with uncontrolled reflex emptying, and loss of inhibitory brain signals causes an uninhibited neurogenic bladder with frequent urination.
Micturition Reflex, SUMMARY
The micturition reflex is the nervous reflex responsible for emptying the urinary bladder when it becomes sufficiently filled with urine. As the bladder fills, stretch receptors located in the bladder wall, particularly in the posterior urethra, are stimulated. These receptors send sensory signals through the pelvic nerves to the sacral segments of the spinal cord. In response, parasympathetic nerve fibers carry motor signals back to the bladder, causing contraction of the detrusor muscle and initiating urination.
When the bladder contains only a small amount of urine, these reflex contractions are usually weak and disappear after a short time. However, as the bladder continues to fill, the stretch receptors are stimulated more strongly, causing the micturition reflex to become increasingly frequent and powerful. The reflex is self-regenerative, meaning that an initial bladder contraction further stimulates stretch receptors, which in turn produce stronger contractions. This positive feedback cycle continues until a strong bladder contraction develops. After a short period, the reflex fatigues, the bladder relaxes, and pressure returns to normal if urination has not occurred.
A complete micturition reflex consists of three phases: a rapid rise in bladder pressure due to detrusor contraction, a period of sustained contraction, and finally a return to the resting pressure level. If the bladder is not emptied, the reflex remains temporarily inhibited and reappears later with greater strength as bladder filling continues.
When the reflex becomes sufficiently strong, it also inhibits the external urethral sphincter through pathways involving the pudendal nerve. If voluntary control does not oppose this inhibition, urination occurs. If voluntary contraction of the external sphincter is maintained, urination is delayed until the bladder fills further and the reflex becomes stronger.
Although the micturition reflex is fundamentally a spinal cord reflex, it is strongly influenced by higher centers in the brain. Centers in the pons and cerebral cortex can either facilitate or inhibit the reflex. Under normal conditions, these higher centers keep the reflex partially suppressed until an appropriate time for urination. They can voluntarily maintain contraction of the external sphincter to prevent urination or facilitate the reflex and relax the sphincter when urination is desired.
Voluntary urination is usually initiated by contracting the abdominal muscles, which increases bladder pressure and forces urine into the bladder neck and posterior urethra. Stretching of these regions activates stretch receptors, strengthens the micturition reflex, and promotes relaxation of the external sphincter. As a result, the bladder empties almost completely, usually leaving only a few milliliters of urine behind.
Several abnormalities can affect the micturition reflex. One disorder is atonic bladder, which occurs when sensory nerve fibers carrying stretch signals from the bladder to the spinal cord are damaged. Because the reflex cannot be initiated, the bladder becomes excessively filled and eventually overflows, causing continuous dribbling of urine. This condition is known as overflow incontinence. Causes include sacral spinal cord injuries and diseases such as tabes dorsalis.
Another disorder is the automatic bladder, which develops when the spinal cord is damaged above the sacral region while the sacral reflex pathways remain intact. Initially, spinal shock suppresses bladder reflexes, causing urinary retention. Over time, however, the micturition reflex recovers independently of brain control, resulting in periodic automatic bladder emptying without conscious awareness.
A third condition is the uninhibited neurogenic bladder, which occurs when inhibitory signals from the brain are partially lost due to damage in the spinal cord or brain stem. Without adequate inhibition, the sacral micturition centers become excessively excitable. Even a small amount of urine in the bladder can trigger a strong micturition reflex, leading to frequent and often uncontrollable urination.
In summary, the micturition reflex is a complex but highly coordinated spinal reflex that controls bladder emptying. Stretch receptors, spinal cord pathways, parasympathetic nerves, and higher brain centers work together to regulate urination. Damage to any part of this control system can result in disorders such as atonic bladder, automatic bladder, or uninhibited neurogenic bladder, each affecting normal urinary control in different ways.