


- Redistribution of potassium helps buffer changes in extracellular fluid potassium concentration.
- Potassium homeostasis requires a balance between potassium intake and potassium excretion.
- Renal potassium excretion depends on three processes:
- Rate of potassium filtration.
- Rate of potassium reabsorption by the tubules.
- Rate of potassium secretion by the tubules.
- Potassium filtration rate = GFR × plasma potassium concentration.
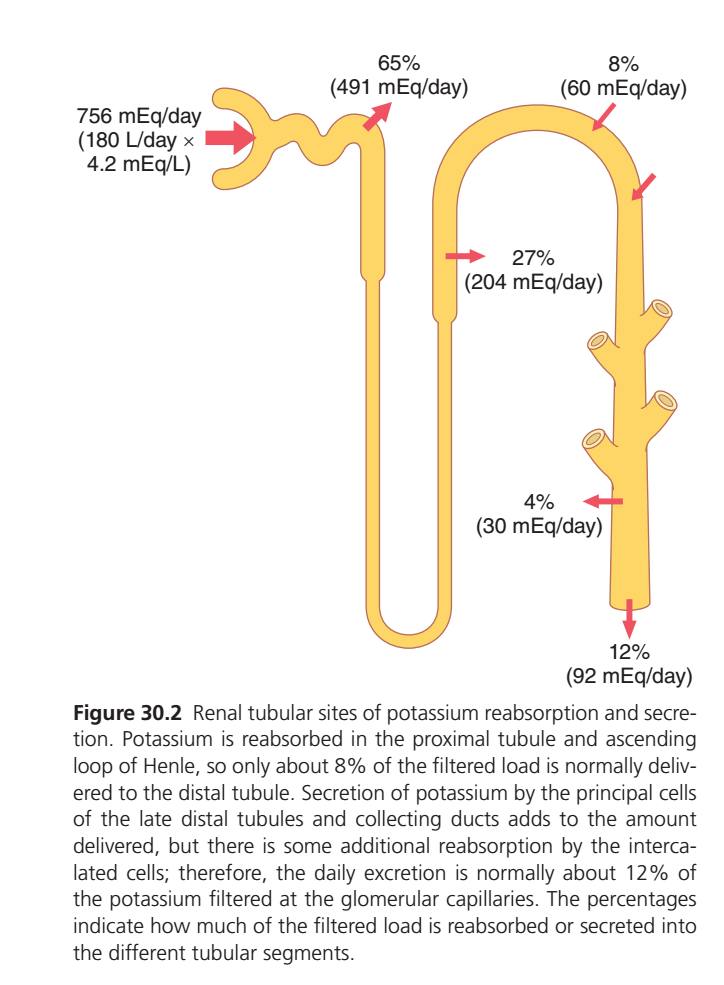
- The normal average potassium filtration rate is about 756 mEq/day.
- This filtration rate is based on a GFR of 180 L/day and a plasma potassium concentration of 4.2 mEq/L.
- Potassium filtration remains relatively constant in healthy people.
- GFR autoregulatory mechanisms help maintain a stable filtration rate.
- Precise regulation of plasma potassium concentration also helps maintain a stable filtration rate.
- Severe decreases in GFR can cause potassium accumulation.
- Potassium accumulation can lead to hyperkalemia.
- About 65% of filtered potassium is reabsorbed in the proximal tubule.
- Another 25% to 30% of filtered potassium is reabsorbed in the thick ascending loop of Henle.
- In the thick ascending loop of Henle, potassium is actively co-transported with sodium and chloride.
- In the proximal tubule and loop of Henle, a relatively constant fraction of filtered potassium is reabsorbed.
- Changes in potassium reabsorption in these segments can influence potassium excretion.
- Most daily variations in potassium excretion are not due to changes in proximal tubule reabsorption.
- Most daily variations in potassium excretion are not due to changes in loop of Henle reabsorption.
- The distal tubules, collecting tubules, and collecting ducts can either reabsorb or secrete potassium.
- Potassium reabsorption and secretion in these segments occur at variable rates.
- These rates depend on potassium intake.
KEY CONCEPT
- Renal potassium excretion depends on filtration, reabsorption, and secretion.
- Most filtered potassium is reabsorbed in the proximal tubule and loop of Henle.
- Daily regulation of potassium excretion mainly occurs in the distal and collecting tubules and collecting ducts.
REGULATION OF RENAL POTASSIUM EXCRETION (Figure 30.2) – Simplest Concept
BIG PICTURE
The kidneys filter a huge amount of potassium (K⁺) every day, but most of it is reabsorbed back into the blood. Only a small amount is finally excreted in urine.
Step 1: Potassium Filtered at the Glomerulus
- GFR = 180 L/day
- Plasma K⁺ = 4.2 mEq/L
- Filtered K⁺ = 756 mEq/day
➡️ This is the total potassium entering the nephron each day.
Step 2: Proximal Tubule Reabsorbs Most Potassium
Proximal Tubule
- Reabsorbs 65%
- Amount reabsorbed = 491 mEq/day
Easy Memory
“Proximal tubule is the biggest potassium saver.”
Step 3: Loop of Henle Reabsorbs More Potassium
Thick Ascending Loop of Henle
- Reabsorbs 27%
- Amount reabsorbed = 204 mEq/day
Total Reabsorbed So Far
- 65% + 27% = 92%
Only 8% remains in the tubular fluid.
Amount Reaching Distal Tubule
- 60 mEq/day (8%)
Easy Memory
“By the time filtrate reaches the distal nephron, 92% of potassium has already been saved.”
Step 4: Distal Tubule & Collecting Duct Can ADD Potassium
Principal Cells
- Secrete potassium into urine
- Add about 30 mEq/day (4%)
This increases tubular potassium.
Easy Memory
“Principal cells throw potassium out.”
Step 5: Intercalated Cells Can SAVE Some Potassium
Intercalated Cells
- Reabsorb potassium when needed
- Prevent excessive potassium loss
Easy Memory
“Intercalated cells rescue potassium.”
Final Potassium Excretion
Urine Output
- About 92 mEq/day
- Equals 12% of filtered load
Therefore
- Filtered = 756 mEq/day
- Reabsorbed = Most of it
- Excreted = Only 12%
NEPHRON STORY IN ONE LINE
Filter → Save → Save More → Secrete Some → Rescue Some → Excrete
756 mEq/day filtered
⬇️
65% reabsorbed in Proximal Tubule
⬇️
27% reabsorbed in Loop of Henle
⬇️
Only 8% reaches Distal Tubule
⬇️
Principal Cells secrete K⁺
⬇️
Intercalated Cells reabsorb some K⁺
⬇️
12% finally excreted in urineKEY CONCEPT
✅ Kidneys filter 756 mEq/day of potassium.
✅ 65% is reabsorbed in the Proximal Tubule.
✅ 27% is reabsorbed in the Thick Ascending Loop of Henle.
✅ Only 8% reaches the distal nephron.
✅ Principal cells secrete K⁺ into the tubule.
✅ Intercalated cells reabsorb K⁺ when needed.
✅ Final urinary excretion is about 12% of filtered potassium (92 mEq/day).
✅ The distal tubule and collecting ducts are the main regulators of potassium excretion.
Variable Potassium Secretion in Distal and Collecting Tubules Mediates Most Daily Changes in Potassium Excretion
- The late distal tubules and cortical collecting tubules are the most important sites for regulating potassium excretion.
- In these tubular segments, potassium can be reabsorbed or secreted.
- Potassium handling depends on the needs of the body.
- With a normal potassium intake of 100 mEq/day, the kidneys must excrete about 92 mEq/day.
- The remaining 8 mEq/day of potassium is lost in the feces.
- About 60 mEq/day of potassium is secreted into the distal and collecting tubules.
- This secretion accounts for most of the excreted potassium.
- With a high potassium intake, additional potassium excretion occurs mainly by increasing potassium secretion into the late distal and collecting tubules.
- In people consuming extremely high-potassium diets, potassium excretion can exceed the amount of potassium filtered by the glomeruli.
- This indicates a powerful mechanism for potassium secretion.
- When potassium intake decreases, potassium secretion in the distal and collecting tubules also decreases.
- Reduced secretion causes a decrease in urinary potassium excretion.
- Potassium reabsorption by intercalated cells in the distal nephron increases.
- Potassium excretion can fall to less than 1% of the potassium in the glomerular filtrate.
- Potassium excretion can decrease to less than 10 mEq/day.
- Potassium intake below this level can lead to severe hypokalemia.
- Most daily regulation of potassium excretion occurs in the late distal tubules, cortical collecting tubules, and collecting ducts.
- In these segments, potassium can be reabsorbed or secreted.
- Potassium handling changes according to the body’s needs.
- The basic mechanisms of potassium secretion and its regulation are discussed in the next section.
KEY CONCEPT
- The late distal tubules and cortical collecting tubules are the main sites for daily potassium regulation.
- High potassium intake increases potassium secretion.
- Low potassium intake decreases secretion and increases reabsorption.
- Potassium excretion is adjusted according to the body’s potassium needs.
Principal Cells of Late Distal and Cortical Collecting Tubules Secrete Potassium
- The cells that secrete potassium in the late distal and cortical collecting tubules are called principal cells.
- Principal cells make up most of the epithelial cells in these regions.
- Potassium secretion from the interstitial fluid into the tubular lumen occurs in two steps.
- The first step is uptake of potassium from the interstitium into the cell.
- This uptake occurs through the Na⁺-K⁺ ATPase pump in the basolateral membrane.
- The pump moves sodium out of the cell into the interstitium.
- At the same time, the pump moves potassium into the cell.
- The second step is passive diffusion of potassium from the cell into the tubular fluid.
- The Na⁺-K⁺ ATPase pump creates a high intracellular potassium concentration.
- This high intracellular potassium concentration provides the driving force for potassium diffusion into the tubular lumen.
- The luminal membrane of principal cells is highly permeable to potassium.
- Special potassium channels allow rapid diffusion of potassium across the luminal membrane.
- Two important potassium channels are present in the luminal membrane:
- Renal Outer Medullary Potassium (ROMK) channels.
- High-conductance “Big” Potassium (BK) channels.
- Both ROMK and BK channels are required for efficient renal potassium excretion.
- The number of these channels increases during high potassium intake.
- Potassium is reabsorbed in the proximal tubule and ascending loop of Henle.
- Only about 8% of the filtered potassium load normally reaches the distal tubule.
- Potassium secretion by principal cells increases the amount of potassium in the tubular fluid.
- Some potassium is reabsorbed again by intercalated cells.
- Daily potassium excretion is normally about 12% of the potassium filtered at the glomerulus.
- Potassium secretion by principal cells is controlled by three main factors:
- Activity of the Na⁺-K⁺ ATPase pump.
- Electrochemical gradient for potassium secretion from blood to tubular lumen.
- Permeability of the luminal membrane to potassium.
- These determinants are regulated by several factors.
KEY CONCEPT
- Principal cells are the main potassium-secreting cells in the late distal and cortical collecting tubules.
- Potassium secretion occurs through uptake by the Na⁺-K⁺ ATPase pump followed by diffusion through ROMK and BK channels.
- Potassium secretion depends on pump activity, the electrochemical gradient, and membrane permeability to potassium.
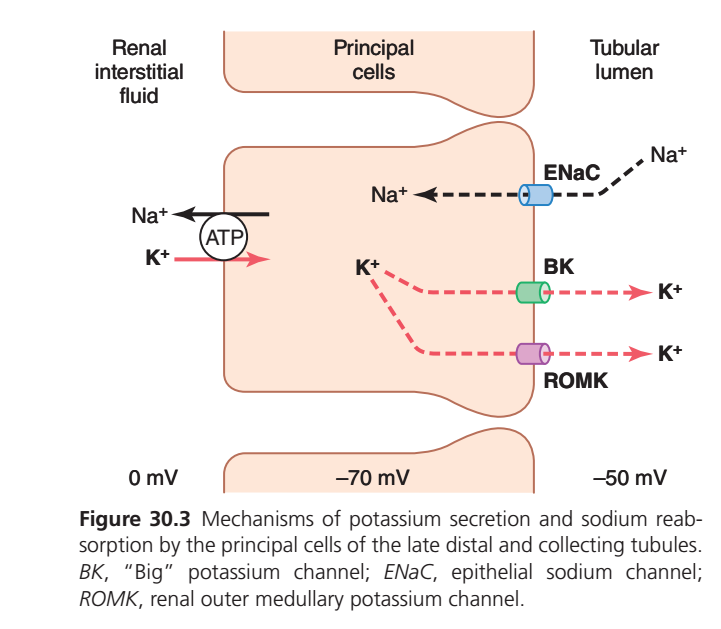
PRINCIPAL CELLS: POTASSIUM SECRETION (GUYTON FIGURE 30.3) — EASY CONCEPT
ONE-LINE SUMMARY
Principal cells reabsorb Na⁺ and secrete K⁺.
The more sodium that enters the cell, the more potassium is pushed into the urine.
STEP 1: Na⁺/K⁺ Pump Loads the Cell with Potassium
On the blood side (renal interstitial fluid side):
- Na⁺/K⁺-ATPase pump uses ATP.
- Pumps 3 Na⁺ out of the cell.
- Pumps 2 K⁺ into the cell.
Result:
✅ Intracellular K⁺ becomes high.
✅ Cell becomes negatively charged (~ -70 mV).
Think: The pump “fills” the cell with potassium.
STEP 2: Sodium Enters from Tubular Fluid
On the urine side (luminal side):
- Sodium enters the principal cell through ENaC channels.
Result:
✅ Na⁺ moves from urine → cell.
✅ Lumen loses positive charge.
✅ Tubular lumen becomes more negative (~ -50 mV).
Think: Sodium is being reabsorbed back into the body.
STEP 3: Potassium Leaves the Cell
Because:
- Cell contains lots of K⁺ (from Na⁺/K⁺ pump)
- Tubular lumen is relatively negative
Potassium moves out of the cell into the urine through:
Potassium Channels
- ROMK channel (major pathway)
- BK channel (activated especially when tubular flow is high)
Result:
✅ K⁺ secretion into urine
WHY DOES POTASSIUM MOVE INTO URINE?
Force 1: High Intracellular K⁺
Na⁺/K⁺ pump continuously loads K⁺ into the cell.
Force 2: Negative Tubular Lumen
Na⁺ reabsorption through ENaC makes the lumen electrically negative.
Combined Effect
Both forces push K⁺:
Cell → Tubular Lumen → Urine
SIMPLE FLOW CHART
Na+/K+ Pump
↓
K+ accumulates inside cell
↓
Na+ enters via ENaC
↓
Lumen becomes negative
↓
K+ exits through ROMK & BK
↓
K+ secreted into urineEXAM PEARL
Increased ENaC Activity
→ More Na⁺ reabsorption
→ Lumen becomes more negative
→ More K⁺ secretion
Increased Aldosterone
→ ↑ Na⁺/K⁺ pump activity
→ ↑ ENaC channels
→ ↑ ROMK channels
→ Marked increase in K⁺ secretion
KEY CONCEPT
Principal cells of the late distal tubule and cortical collecting duct regulate potassium excretion. Na⁺ reabsorption through ENaC creates a negative lumen, while the Na⁺/K⁺ pump loads the cell with K⁺. These two forces drive K⁺ secretion through ROMK and BK channels into the urine.
Intercalated Cells Can Reabsorb or Secrete Potassium
- During severe potassium depletion, potassium secretion stops.
- During severe potassium depletion, there is net potassium reabsorption in the late distal and collecting tubules.
- This potassium reabsorption occurs through type A intercalated cells.
- One mechanism for potassium reabsorption is the hydrogen-potassium ATPase transporter in the luminal membrane.
- This transporter reabsorbs potassium from the tubular lumen.
- At the same time, it secretes hydrogen ions into the tubular lumen.
- The reabsorbed potassium then diffuses through potassium channels in the basolateral membrane.
- Potassium moves from the cell into the interstitial fluid.
- The number of hydrogen-potassium ATPase transporters increases during potassium depletion.
- The number of these transporters also increases during hypokalemia.
- This causes increased hydrogen ion secretion.
- Increased hydrogen ion secretion can lead to alkalosis.
- Under normal conditions, potassium reabsorption by intercalated cells plays only a small role in controlling potassium excretion.
- When excess potassium is present in the body fluids, type B intercalated cells actively secrete potassium into the tubular lumen.
- Type B intercalated cells have functions opposite to those of type A intercalated cells.
- Potassium is pumped into the type B intercalated cell by a hydrogen-potassium ATPase transporter in the basolateral membrane.
- Potassium then diffuses into the tubular lumen through potassium channels.
KEY CONCEPT
- Type A intercalated cells reabsorb potassium during potassium depletion and hypokalemia.
- Potassium reabsorption occurs through the hydrogen-potassium ATPase transporter.
- Increased activity of this transporter increases hydrogen ion secretion and may cause alkalosis.
- Type B intercalated cells secrete potassium when body potassium levels are high.
- Type A and Type B intercalated cells have opposite effects on potassium handling.
Summary of Major Factors That Regulate Potassium Secretion
- Normal regulation of potassium excretion occurs mainly through changes in potassium secretion by principal cells.
- These principal cells are located in the late distal and collecting tubules.
- The most important factors that increase potassium secretion are:
- Increased extracellular fluid potassium concentration.
- Increased aldosterone.
- Increased tubular flow rate.
- One factor that decreases potassium secretion is increased hydrogen ion concentration (acidosis).
Increased Extracellular Fluid Potassium Concentration Stimulates Potassium Secretion
- Increased extracellular fluid potassium concentration directly stimulates potassium secretion in the late distal and cortical collecting tubules.
- Increased potassium secretion leads to increased potassium excretion.
- This effect becomes especially strong when extracellular fluid potassium concentration rises above about 4.1 mEq/L.
- Increased plasma potassium concentration is one of the most important mechanisms for regulating extracellular fluid potassium concentration.
- Increased dietary potassium intake also stimulates potassium secretion.
Mechanism 1: Stimulation of Na⁺-K⁺ ATPase Pump
- Increased extracellular fluid potassium concentration stimulates the Na⁺-K⁺ ATPase pump.
- This increases potassium uptake into the cell across the basolateral membrane.
- Increased potassium uptake raises intracellular potassium concentration.
- Increased intracellular potassium promotes diffusion of potassium into the tubular lumen.
Mechanism 2: Reduction of Potassium Backleak
- Increased extracellular potassium concentration increases the potassium gradient from the renal interstitial fluid to the epithelial cell.
- This reduces backleak of potassium from the cell through the basolateral membrane.
- More potassium remains inside the cell for secretion into the tubular lumen.
Mechanism 3: Increase in Potassium Channels
- Increased potassium intake stimulates synthesis of potassium channels.
- It also promotes movement of potassium channels from the cytosol to the luminal membrane.
- The number of potassium channels in the luminal membrane increases.
- Potassium diffuses more easily through the membrane.
Mechanism 4: Stimulation of Aldosterone Secretion
- Increased potassium concentration stimulates aldosterone secretion from the adrenal cortex.
- Increased aldosterone further stimulates potassium secretion.
KEY CONCEPT
- Potassium secretion is mainly regulated by principal cells of the late distal and collecting tubules.
- Increased extracellular potassium concentration is a major stimulus for potassium secretion.
- Increased potassium secretion occurs through:
- Increased Na⁺-K⁺ ATPase activity.
- Reduced potassium backleak.
- Increased potassium channels.
- Increased aldosterone secretion.
- Acidosis decreases potassium secretion.
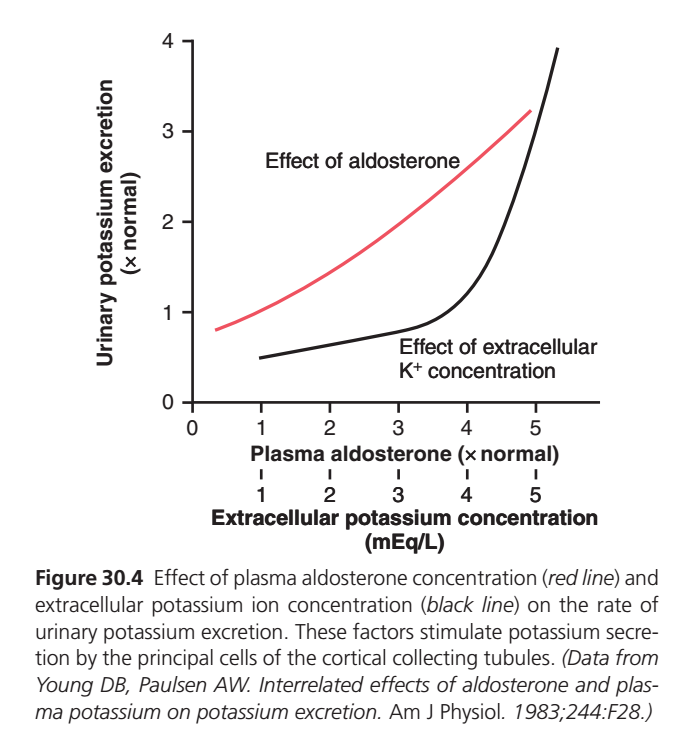
EFFECT OF ALDOSTERONE & EXTRACELLULAR K⁺ ON POTASSIUM EXCRETION (GUYTON FIGURE 30.4)
ONE-LINE SUMMARY
Both aldosterone and increased extracellular K⁺ increase urinary potassium excretion, but high extracellular K⁺ is the most powerful stimulus.
WHAT IS THIS GRAPH SHOWING?
The graph compares two major regulators of potassium secretion by principal cells:
🔴 Red Line = Effect of Aldosterone
⚫ Black Line = Effect of Extracellular K⁺ Concentration
Y-axis:
- Urinary potassium excretion
X-axis:
- Aldosterone level (red line)
- Extracellular K⁺ concentration (black line)
1. EFFECT OF ALDOSTERONE (RED LINE)
As aldosterone increases:
- Na⁺/K⁺ pump activity increases
- More K⁺ enters principal cells
- ENaC channels increase
- ROMK channels increase
- More K⁺ is secreted into urine
Result
↑ Aldosterone
→ ↑ K⁺ secretion
→ ↑ Urinary K⁺ excretion
The increase is steady and progressive.
2. EFFECT OF EXTRACELLULAR K⁺ (BLACK LINE)
When plasma K⁺ rises:
- More K⁺ enters principal cells
- Intracellular K⁺ increases
- Strong driving force develops for K⁺ secretion
At normal K⁺ levels (≈3–4 mEq/L)
- Small increase in K⁺ excretion
At higher K⁺ levels (>4–5 mEq/L)
- Potassium excretion rises very rapidly
Result
↑ Plasma K⁺
→ Massive stimulation of K⁺ secretion
→ Large increase in urinary K⁺ excretion
WHY IS THE BLACK CURVE SO STEEP?
The kidneys strongly protect against hyperkalemia.
When plasma K⁺ starts rising:
- Principal cells secrete much more K⁺
- Aldosterone release is stimulated
- Excess K⁺ is rapidly removed in urine
Purpose
Prevent dangerous increases in plasma potassium.
IMPORTANT RELATIONSHIP
Increased Plasma K⁺ Directly Stimulates
- Principal cells
- Aldosterone secretion from adrenal cortex
Therefore:
↑ Plasma K+
↓
↑ Aldosterone
↓
↑ K+ Secretion
↓
↑ Urinary K+ ExcretionSo potassium has:
✅ Direct effect on kidney
AND
✅ Indirect effect through aldosterone
WHICH FACTOR IS MORE IMPORTANT?
Acute Regulation
⭐ Extracellular K⁺ concentration
The black curve becomes much steeper, showing that even small increases in plasma K⁺ can produce large increases in K⁺ excretion.
Supportive Hormone
⭐ Aldosterone
Aldosterone enhances the response but is not usually as powerful as a rise in plasma K⁺ itself.
EASY MEMORY TRICK
“K⁺ Controls K⁺”
When plasma potassium rises:
- Kidney senses it
- Aldosterone rises
- Potassium secretion increases
- Excess potassium is excreted
KEY CONCEPT
The two most important stimulators of potassium secretion by principal cells are aldosterone and extracellular potassium concentration. Aldosterone causes a gradual increase in urinary potassium excretion, whereas increased extracellular K⁺ causes a much stronger and more rapid increase, making plasma K⁺ concentration the primary regulator of potassium excretion.
Aldosterone Stimulates Potassium Secretion
- Aldosterone strongly stimulates sodium reabsorption and potassium secretion by principal cells.
- These principal cells are located in the late distal tubules and collecting ducts.
- Aldosterone acts through the Na⁺-K⁺ ATPase pump.
- The Na⁺-K⁺ ATPase pump transports sodium out of the cell through the basolateral membrane.
- Sodium moves into the renal interstitial fluid.
- At the same time, the pump transports potassium into the cell.
Effect of Aldosterone on Potassium Channels
- Aldosterone increases the number of potassium channels in the luminal membrane.
- This increases the permeability of the luminal membrane to potassium.
- Potassium can diffuse more easily into the tubular lumen.
- This further enhances potassium secretion.
Effect on Potassium Excretion
- Aldosterone has a powerful effect on increasing potassium secretion.
- Increased potassium secretion leads to increased potassium excretion.
KEY CONCEPT
- Aldosterone is a major stimulator of potassium secretion.
- It increases Na⁺-K⁺ ATPase pump activity.
- It increases the number of luminal potassium channels.
- These actions increase potassium secretion and potassium excretion.
Increased Extracellular Potassium Ion Concentration Stimulates Aldosterone Secretion
- In negative feedback control systems, the controlled factor usually has a feedback effect on the controller.
- In the aldosterone-potassium control system, aldosterone secretion is strongly controlled by extracellular fluid potassium concentration.
- An increase in plasma potassium concentration of about 3 mEq/L can increase plasma aldosterone concentration from nearly 0 to as high as 60 ng/100 mL.
- This aldosterone concentration is almost 10 times the normal level.
- Stimulation of aldosterone secretion by potassium is part of a powerful feedback system that regulates potassium excretion.
- An increase in plasma potassium concentration stimulates aldosterone secretion.
- Increased aldosterone secretion raises plasma aldosterone concentration.
- Increased plasma aldosterone causes a marked increase in potassium secretion by the kidneys.
- Increased plasma aldosterone also causes a marked increase in potassium excretion by the kidneys.
- Increased potassium excretion reduces extracellular fluid potassium concentration toward normal.
- This feedback mechanism works together with the direct effect of increased extracellular potassium concentration.
- Both mechanisms increase potassium excretion when potassium intake is increased.
KEY CONCEPT
- Increased extracellular potassium stimulates aldosterone secretion.
- Increased aldosterone increases renal potassium secretion and excretion.
- Increased potassium excretion lowers extracellular potassium concentration toward normal.
- This is a powerful negative feedback system for potassium regulation.
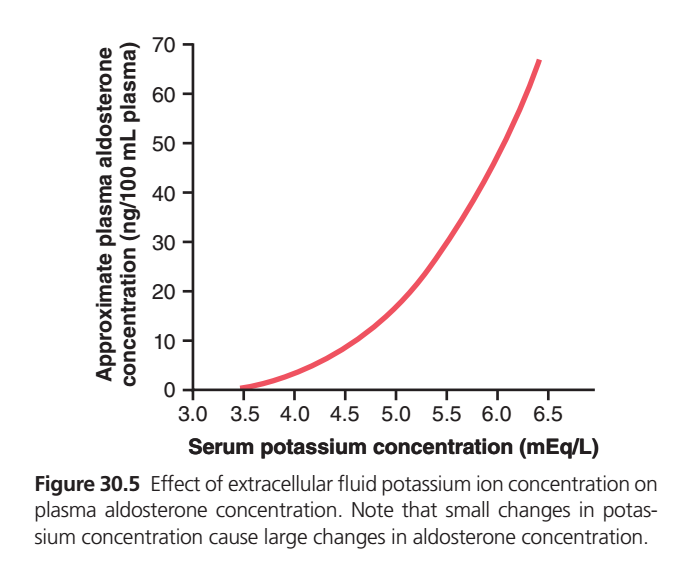
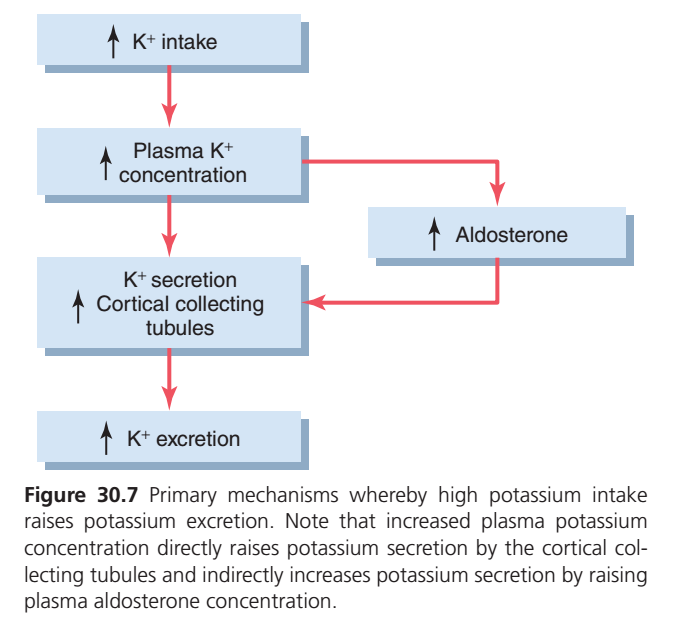
INCREASED EXTRACELLULAR POTASSIUM STIMULATES ALDOSTERONE SECRETION (Figure 30.5)
BIG PICTURE
This graph shows a very important relationship:
↑ Potassium in Blood (K⁺)
⬇️
↑ Aldosterone Secretion
⬇️
↑ Potassium Excretion by Kidneys
⬇️
Blood Potassium Returns to Normal
This is a classic negative feedback system.
What Does the Graph Show?
X-Axis
Serum Potassium Concentration (mEq/L)
Normal range:
- Around 3.5–5.0 mEq/L
Y-Axis
Plasma Aldosterone Concentration
Represents how much aldosterone is being secreted by the adrenal cortex.
Key Observation
The curve rises very steeply.
This means:
✅ Small increase in blood potassium
➡️ Causes a large increase in aldosterone secretion
Example
Potassium = 3.5 mEq/L
- Aldosterone secretion is very low.
Potassium = 5.0 mEq/L
- Aldosterone rises significantly.
Potassium = 6.5 mEq/L
- Aldosterone becomes extremely high.
WHY DOES THIS HAPPEN?
The body wants to prevent dangerous hyperkalemia.
When Blood Potassium Rises
High K⁺ directly stimulates the:
Adrenal Cortex (Zona Glomerulosa)
which releases:
Aldosterone
Effects of Aldosterone
Aldosterone acts mainly on:
- Late distal tubule
- Cortical collecting duct
- Principal cells
Aldosterone Causes
- ↑ Na⁺ reabsorption
- ↑ K⁺ secretion
- ↑ K⁺ excretion in urine
Easy Flow Diagram
High Potassium Intake
⬇️
↑ Plasma K⁺
⬇️
Stimulates Adrenal Cortex
⬇️
↑ Aldosterone
⬇️
Principal Cells Secrete More K⁺
⬇️
↑ Urinary K⁺ Loss
⬇️
Plasma K⁺ Returns to Normal
NEGATIVE FEEDBACK LOOP
Step 1
Blood potassium rises.
Step 2
Aldosterone secretion increases.
Step 3
Kidneys excrete more potassium.
Step 4
Blood potassium falls back toward normal.
Step 5
Aldosterone secretion decreases again.
HIGH-YIELD EXAM POINT
Which electrolyte directly stimulates aldosterone secretion?
✅ Potassium (K⁺)
Potassium is one of the strongest direct stimulators of aldosterone release.
CLINICAL IMPORTANCE
Hyperkalemia (High K⁺)
Causes:
- Increased aldosterone secretion
- Increased renal potassium excretion
Hypokalemia (Low K⁺)
Causes:
- Decreased aldosterone secretion
- Reduced potassium excretion
- Conservation of body potassium
EASY MEMORY TRICK
“K⁺ Controls Aldosterone”
↑ K⁺ → ↑ Aldosterone → ↑ K⁺ Excretion
↓ K⁺ → ↓ Aldosterone → ↓ K⁺ Excretion
KEY CONCEPT
✅ Small increases in extracellular potassium cause large increases in aldosterone secretion.
✅ Potassium directly stimulates the zona glomerulosa of the adrenal cortex.
✅ Aldosterone acts on principal cells in the distal nephron.
✅ Aldosterone increases potassium secretion and urinary potassium excretion.
✅ This forms a negative feedback system that keeps plasma potassium concentration within a narrow normal range.
✅ ↑ K⁺ → ↑ Aldosterone → ↑ K⁺ Excretion → Normalization of plasma K⁺
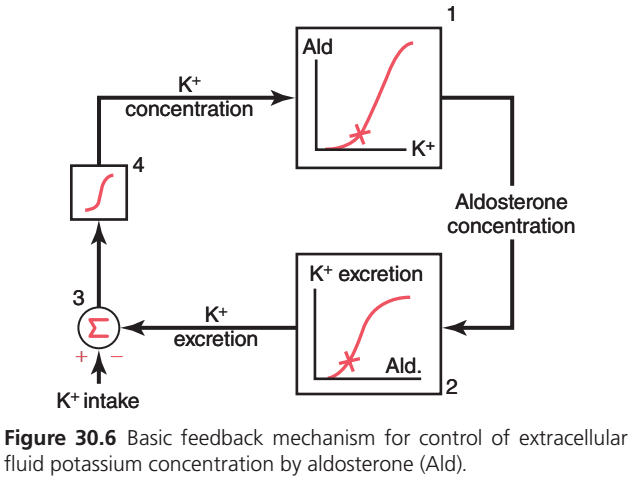
ALDOSTERONE–POTASSIUM FEEDBACK SYSTEM (Figure 30.6)
BIG PICTURE
This figure shows how the body automatically keeps blood potassium (K⁺) normal using aldosterone.
Think of it as a thermostat for potassium.
Simple Rule
↑ Blood K⁺ → ↑ Aldosterone → ↑ K⁺ Excretion → K⁺ Returns to Normal
↓ Blood K⁺ → ↓ Aldosterone → ↓ K⁺ Excretion → K⁺ Conserved
This is a negative feedback loop.
STEP-BY-STEP UNDERSTANDING OF THE FIGURE
STEP 1: Blood Potassium Controls Aldosterone
Box 1
↑ Plasma K⁺
⬇️
Stimulates adrenal cortex (zona glomerulosa)
⬇️
↑ Aldosterone secretion
Easy Memory
Potassium is the boss of aldosterone.
STEP 2: Aldosterone Controls Potassium Excretion
Box 2
↑ Aldosterone
⬇️
Acts on principal cells of:
- Late distal tubule
- Cortical collecting duct
⬇️
↑ Potassium secretion into urine
⬇️
↑ Potassium excretion
Easy Memory
Aldosterone opens the exit door for potassium.
STEP 3: Potassium Intake and Potassium Excretion Are Compared
Circle (Σ) = Balance Center
The body constantly compares:
Potassium Intake
vs
Potassium Excretion
Normal State
Potassium intake ≈ Potassium excretion
Balance is maintained.xample
You eat extra bananas or a potassium-rich meal.
⬇️
Potassium intake increases.
Now:
Intake > Excretion
This creates a positive potassium balance.
STEP 4: Blood Potassium Rises
Box 4
When intake exceeds excretion:
Plasma K⁺ concentration increases
⬇️
This increased K⁺ goes back to:
Box 1
and stimulates more aldosterone secretion.
COMPLETE CYCLE
Eat More Potassium
⬇️
↑ K⁺ Intake
⬇️
↑ Plasma K⁺
⬇️
↑ Aldosterone Secretion
⬇️
↑ K⁺ Secretion by Kidneys
⬇️
↑ Urinary K⁺ Excretion
⬇️
Plasma K⁺ Returns to Normal
WHY IS THIS NEGATIVE FEEDBACK?
Because the original change is reversed.
Original Problem
↑ Plasma K⁺
Kidney Response
↑ Aldosterone
⬇️
↑ K⁺ Excretion
Result
↓ Plasma K⁺
The system corrects itself.
WHAT HAPPENS DURING LOW POTASSIUM INTAKE?
Low K⁺ Intake
⬇️
↓ Plasma K⁺
⬇️
↓ Aldosterone
⬇️
↓ K⁺ Secretion
⬇️
Kidneys conserve potassium
⬇️
Prevents hypokalemia
EASY ONE-LINE STORY
Potassium rises → Aldosterone rises → Kidney throws out potassium → Potassium becomes normal.
SUPER HIGH-YIELD EXAM FLOWCHART
↑ K⁺ Intake
↓
↑ Plasma K⁺
↓
↑ Aldosterone
↓
↑ Principal Cell Activity
↓
↑ K⁺ Secretion
↓
↑ Urinary K⁺ Excretion
↓
↓ Plasma K⁺ (Back to Normal)KEY CONCEPT
✅ Blood potassium concentration directly stimulates aldosterone secretion.
✅ Aldosterone increases potassium secretion by principal cells in the distal nephron.
✅ Increased potassium excretion lowers plasma potassium concentration.
✅ This forms a powerful negative feedback system.
✅ The purpose of the system is to keep extracellular fluid potassium concentration within a narrow normal range.
✅ ↑ K⁺ → ↑ Aldosterone → ↑ K⁺ Excretion → Normal K⁺.
✅ ↓ K⁺ → ↓ Aldosterone → ↓ K⁺ Excretion → Potassium conservation.
Blockade of Aldosterone Feedback System Greatly Impairs Potassium Regulation
- In the absence of adequate aldosterone secretion, renal potassium secretion is impaired.
- This occurs in patients with Addison disease.
- Impaired potassium secretion causes extracellular fluid potassium concentration to rise to dangerously high levels.
- Excess aldosterone secretion greatly increases potassium secretion.
- This occurs in conditions such as primary aldosteronism.
- Increased potassium secretion causes potassium loss by the kidneys.
- Potassium loss by the kidneys leads to hypokalemia.
- In addition to stimulating renal potassium secretion, aldosterone also increases cellular uptake of potassium.
- This effect contributes to the aldosterone-potassium feedback system.
- The quantitative importance of the aldosterone feedback system is demonstrated experimentally.
- In the experiment, potassium intake was increased almost 7-fold in dogs.
- The experiment was performed under two conditions.
- The first condition was normal.
- The second condition involved blocking the aldosterone feedback system.
- The aldosterone feedback system was blocked by removing the adrenal glands.
- The animals were then given a fixed rate of aldosterone infusion.
- Plasma aldosterone concentration was maintained at a normal level.
- Plasma aldosterone concentration could not increase or decrease when potassium intake changed.
- In normal animals, a 7-fold increase in potassium intake caused only a slight increase in plasma potassium concentration.
- Plasma potassium concentration increased from 4.2 to 4.3 mEq/L.
- When the aldosterone feedback system functions normally, potassium concentration is precisely controlled.
- Precise control occurs despite large changes in potassium intake.
- When the aldosterone feedback system was blocked, the same increase in potassium intake caused a much larger increase in plasma potassium concentration.
- Potassium concentration control becomes greatly impaired when the aldosterone feedback system is blocked.
- Similar impairment of potassium regulation occurs in people with poorly functioning aldosterone feedback systems.
- This impairment occurs in patients with primary aldosteronism.
- This impairment also occurs in patients with Addison disease.
KEY CONCEPT
- Aldosterone is essential for normal potassium regulation.
- Too little aldosterone causes potassium retention and hyperkalemia.
- Too much aldosterone causes excessive potassium loss and hypokalemia.
- The aldosterone feedback system keeps plasma potassium concentration stable despite large changes in potassium intake.
- Blocking this feedback system greatly impairs potassium control.
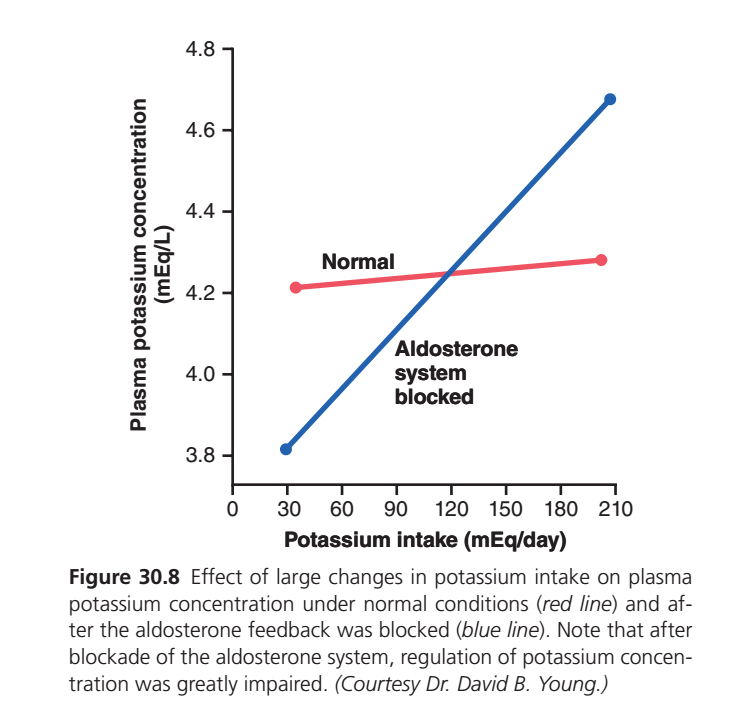
BLOCKADE OF ALDOSTERONE FEEDBACK SYSTEM GREATLY IMPAIRS POTASSIUM REGULATION (Figure 30.8)
BIG PICTURE
This graph answers an important question:
What happens if aldosterone cannot work?
👉 The body loses its ability to keep blood potassium (K⁺) stable.
This proves that:
Aldosterone is one of the most important hormones for potassium regulation.
Understanding the Graph
X-Axis
Potassium Intake (mEq/day)
- Left side = Low potassium intake
- Right side = High potassium intake
Y-Axis
Plasma Potassium Concentration (mEq/L)
This is the potassium level in the blood.
RED LINE = NORMAL ALDOSTERONE SYSTEM
What Happens?
Potassium intake increases greatly:
30 mEq/day → 200 mEq/day
But plasma potassium changes only slightly:
4.2 → 4.3 mEq/L
Almost no change!
Why?
Because the aldosterone feedback system is working.
High K⁺ Intake
⬇️
↑ Plasma K⁺ (slight increase)
⬇️
↑ Aldosterone
⬇️
↑ Renal K⁺ Excretion
⬇️
Extra K⁺ removed
⬇️
Plasma K⁺ remains nearly normal
Easy Memory
“Aldosterone acts like a potassium thermostat.”
BLUE LINE = ALDOSTERONE SYSTEM BLOCKED
What Happens?
Now aldosterone cannot respond.
As potassium intake rises:
30 mEq/day → 200 mEq/day
Plasma potassium rises dramatically:
3.8 → 4.7 mEq/L
Why?
Because the kidneys lose their major mechanism for removing excess potassium.
High K⁺ Intake
⬇️
↑ Plasma K⁺
⬇️
No Aldosterone Response
⬇️
Poor K⁺ Secretion
⬇️
Poor K⁺ Excretion
⬇️
Potassium Accumulates in Blood
Comparison
| Condition | Effect of Increased K⁺ Intake |
|---|---|
| Normal Aldosterone System | Plasma K⁺ remains almost constant |
| Aldosterone Blocked | Plasma K⁺ rises markedly |
Clinical Correlation
Addison Disease
In Addison disease:
- Adrenal cortex is destroyed
- Aldosterone production decreases
Result
- Reduced potassium secretion
- Reduced potassium excretion
- Hyperkalemia develops
Easy Memory
Addison = No Aldosterone = High Potassium
Why Is Aldosterone So Powerful?
Aldosterone acts on:
Principal Cells
in the:
- Late distal tubule
- Cortical collecting duct
It increases:
✅ Na⁺ reabsorption
✅ K⁺ secretion
✅ K⁺ excretion
Therefore, even large dietary potassium loads can be removed efficiently.
Conceptual Story
Normal Person
Eats 5 bananas 🍌🍌🍌🍌🍌
⬇️
K⁺ rises slightly
⬇️
Aldosterone increases
⬇️
Kidneys excrete extra K⁺
⬇️
Blood K⁺ remains normal
Person Without Aldosterone
Eats 5 bananas 🍌🍌🍌🍌🍌
⬇️
K⁺ rises
⬇️
No aldosterone response
⬇️
Kidneys cannot excrete enough K⁺
⬇️
Hyperkalemia develops
KEY CONCEPT
✅ Aldosterone is essential for maintaining normal plasma potassium concentration.
✅ When potassium intake increases, aldosterone secretion increases and stimulates renal potassium excretion.
✅ With a normal aldosterone system, plasma K⁺ changes very little despite large changes in potassium intake.
✅ Blocking aldosterone greatly impairs potassium regulation.
✅ Without aldosterone, potassium accumulates in the blood and hyperkalemia can occur.
✅ Normal: Large change in K⁺ intake → Small change in plasma K⁺.
✅ Aldosterone blocked: Large change in K⁺ intake → Large change in plasma K⁺.
✅ This graph demonstrates the importance of the aldosterone–potassium negative feedback system in maintaining potassium homeostasis.
Increased Distal Tubular Flow Rate Stimulates Potassium Secretion
- Increased distal tubular flow rate stimulates potassium secretion.
- Increased distal tubular flow rate occurs with volume expansion.
- Increased distal tubular flow rate occurs with high sodium intake.
- Increased distal tubular flow rate occurs with treatment using some diuretics.
- Decreased distal tubular flow rate reduces potassium secretion.
- Decreased distal tubular flow rate occurs with sodium depletion.
- The effect of tubular flow rate on potassium secretion is strongly influenced by potassium intake.
- When potassium intake is high, increased tubular flow rate causes a much greater increase in potassium secretion.
- When potassium intake is low, increased tubular flow rate has a smaller effect on potassium secretion.
Main Effect 1
- When potassium is secreted into the tubular fluid, luminal potassium concentration increases.
- Increased luminal potassium concentration reduces the driving force for potassium diffusion across the luminal membrane.
- With increased tubular flow rate, secreted potassium is continuously flushed down the tubule.
- Continuous flushing minimizes the rise in tubular potassium concentration.
- This increases net potassium secretion.
Main Effect 2
- A high tubular flow rate increases the number of high-conductance BK channels in the luminal membrane.
- BK channels are normally quiescent.
- BK channels become active when flow rate increases.
- Activation of BK channels greatly increases potassium conductance across the luminal membrane.
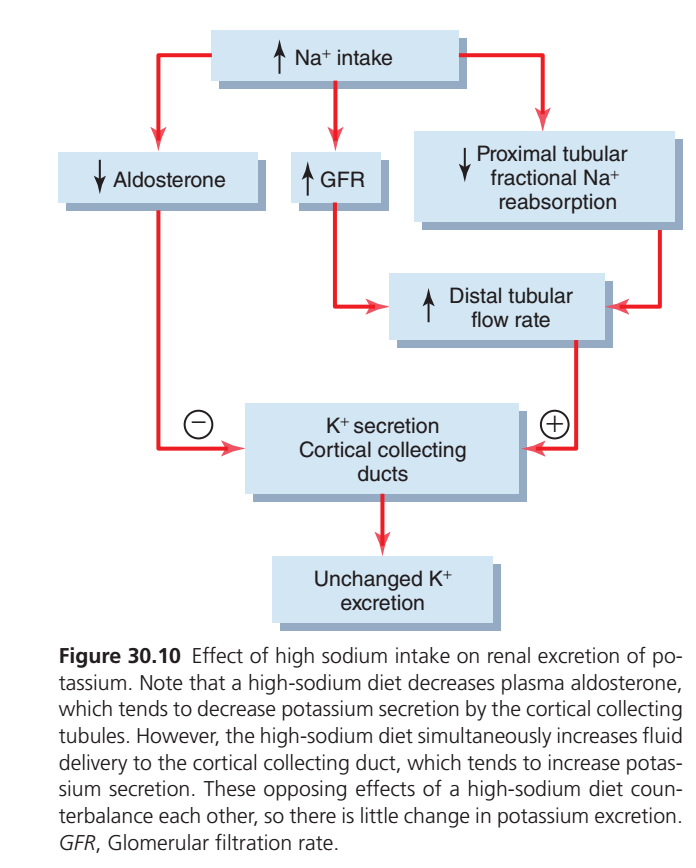
Importance During Changes in Sodium Intake
- The effect of increased tubular flow rate helps preserve normal potassium excretion during changes in sodium intake.
- With a high sodium intake, aldosterone secretion decreases.
- Decreased aldosterone secretion by itself tends to decrease potassium secretion.
- Decreased aldosterone secretion by itself tends to decrease urinary potassium excretion.
- High sodium intake also increases distal tubular flow rate.
- Increased distal tubular flow rate tends to increase potassium secretion.
- Decreased aldosterone secretion and increased tubular flow rate counterbalance each other.
- Therefore, high sodium intake causes little change in potassium excretion.
- With a low sodium intake, aldosterone secretion increases.
- With a low sodium intake, tubular flow rate decreases.
- Increased aldosterone secretion and decreased tubular flow rate counterbalance each other.
- Therefore, low sodium intake also causes little change in potassium excretion.
KEY CONCEPT
- Increased distal tubular flow rate increases potassium secretion.
- It increases potassium secretion by flushing potassium from the tubule and activating BK channels.
- The effect is stronger when potassium intake is high.
- Changes in aldosterone secretion and tubular flow rate balance each other during changes in sodium intake.
- As a result, potassium excretion changes very little with high or low sodium intake.
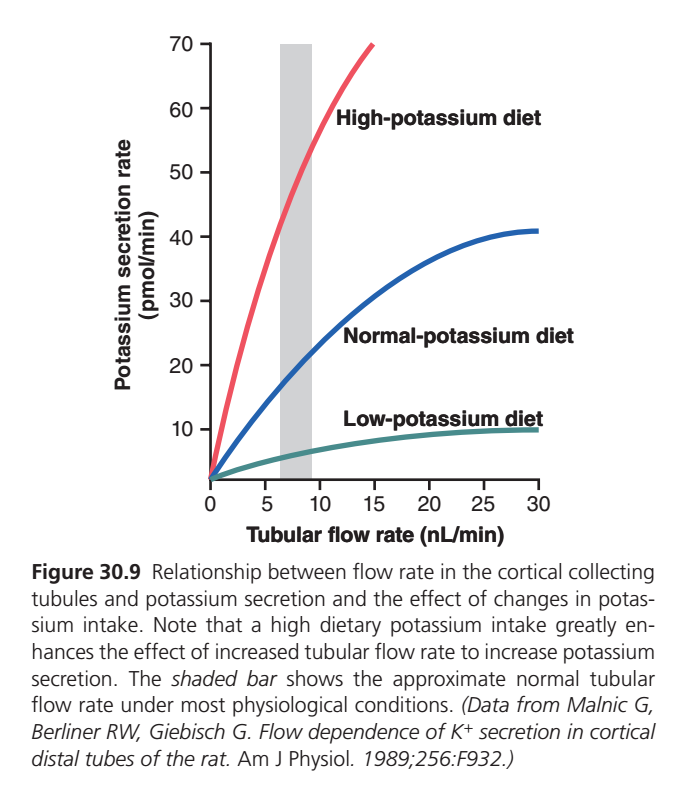
EFFECT OF TUBULAR FLOW RATE ON POTASSIUM SECRETION (Figure 30.9)
BIG PICTURE
This graph shows:
↑ Tubular Flow Rate
➡️ ↑ Potassium (K⁺) Secretion
The faster fluid flows through the cortical collecting duct, the more potassium is secreted into urine.
Understanding the Graph
X-Axis
Tubular Flow Rate (nL/min)
- Left = Slow flow
- Right = Fast flow
Y-Axis
Potassium Secretion Rate
Amount of potassium secreted into the tubule.
Main Observation
All three curves move upward.
This means:
Faster Tubular Flow
⬇️
More Potassium Secretion
regardless of potassium intake.
Why Does Increased Flow Increase Potassium Secretion?
Imagine a River
Slow Flowing River
Potassium accumulates near the tubular cells.
As K⁺ builds up in the tubular fluid:
- Concentration gradient decreases
- Less K⁺ leaves the cells
➡️ Potassium secretion slows.
Fast Flowing River
Tubular fluid continuously washes away secreted potassium.
So:
- K⁺ concentration in tubular fluid remains low
- Concentration gradient stays high
- More K⁺ diffuses out of principal cells
➡️ Potassium secretion increases.
EASY MEMORY
“Fast Flow Flushes Potassium Away”
The faster the tubular fluid moves,
the more potassium the kidney can dump into urine.
Effect of Different Potassium Diets
1. Low-Potassium Diet (Green Curve)
Situation
Body wants to conserve potassium.
Result
- Potassium secretion remains very low.
- Increasing flow causes only a small increase in secretion.
Easy Memory
Low K⁺ Diet = Save Potassium
2. Normal-Potassium Diet (Blue Curve)
Situation
Normal potassium balance.
Result
- Moderate potassium secretion.
- Increasing flow noticeably increases secretion.
3. High-Potassium Diet (Red Curve)
Situation
Body has excess potassium.
Result
- Potassium secretion becomes very high.
- Increased flow dramatically increases secretion.
Easy Memory
High K⁺ Diet + Fast Flow = Massive K⁺ Excretion
Gray Shaded Area
This represents:
Normal Physiological Tubular Flow Rate
The usual flow rates seen in everyday life.
Even within this normal range:
small increases in flow can significantly increase potassium secretion.
Clinical Importance
What Increases Distal Tubular Flow?
Volume Expansion
- Increased extracellular fluid volume
High Sodium Intake
- More Na⁺ delivered distally
- More water follows
Diuretics (Very Important)
Examples:
- Loop diuretics
- Thiazide diuretics
These increase:
⬆ Distal flow rate
⬇
⬆ Potassium secretion
⬇
⬆ Potassium loss in urine
Why Diuretics Cause Hypokalemia
Diuretic
⬇️
↑ Tubular Flow Rate
⬇️
↑ K⁺ Secretion
⬇️
↑ Urinary K⁺ Loss
⬇️
Hypokalemia
Guyton’s Core Concept
The late distal tubule and cortical collecting duct are the major sites of potassium regulation.
Potassium secretion here depends strongly on:
- Plasma potassium concentration
- Aldosterone
- Tubular flow rate
SUPER HIGH-YIELD FLOWCHART
↑ Tubular Flow
↓
K⁺ Washed Away From Tubule
↓
Low Luminal K⁺ Concentration
↓
Large Gradient for K⁺ Diffusion
↓
↑ K⁺ Secretion
↓
↑ Urinary K⁺ ExcretionKEY CONCEPT
✅ Increased distal tubular flow rate strongly stimulates potassium secretion.
✅ Fast flow continuously washes away secreted potassium, maintaining a favorable diffusion gradient.
✅ Higher flow = Greater potassium excretion.
✅ A high-potassium diet greatly enhances the effect of flow on potassium secretion.
✅ A low-potassium diet suppresses potassium secretion even when flow increases.
✅ Diuretics, volume expansion, and high sodium intake increase distal flow and therefore increase potassium loss.
✅ Fast Flow = More K⁺ Secretion = More K⁺ Excretion.
Acute Acidosis Decreases Potassium Secretion
- Acute increases in extracellular fluid hydrogen ion concentration (acidosis) reduce potassium secretion.
- Decreased hydrogen ion concentration (alkalosis) increases potassium secretion.
- Acid-base disturbances have complex effects on potassium excretion.
- One important mechanism is that increased hydrogen ion concentration reduces Na⁺-K⁺ ATPase pump activity.
- Reduced Na⁺-K⁺ ATPase activity decreases intracellular potassium concentration.
- Decreased intracellular potassium reduces passive diffusion of potassium into the tubular lumen.
- Acidosis may also reduce the number of potassium channels in the luminal membrane.
- In intercalated cells of the late distal and collecting tubules, acidosis stimulates hydrogen-ATPase.
- Acidosis also stimulates hydrogen-potassium ATPase.
- These effects enhance potassium reabsorption.
- Increased potassium reabsorption reduces net potassium secretion.
- Prolonged acidosis lasting several days increases urinary potassium excretion.
- Chronic acidosis reduces proximal tubular Na⁺-K⁺ ATPase activity.
- Reduced Na⁺-K⁺ ATPase activity inhibits sodium chloride and water reabsorption.
- Inhibition of reabsorption increases distal volume delivery.
- Increased distal volume delivery stimulates potassium secretion.
- This effect overrides the inhibitory effect of hydrogen ions on the Na⁺-K⁺ ATPase pump.
- Chronic acidosis causes potassium loss.
- Acute acidosis decreases potassium excretion.
Beneficial Effects of Diet High in Potassium and Low in Sodium Content
- For most of human history, diets were relatively low in sodium and high in potassium.
- This differs from the typical modern diet.
- Some isolated populations have maintained these traditional dietary patterns.
- The Yanomamo tribe of Northern Brazil is one example.
- Their sodium intake may be as low as 10 to 20 mmol/day.
- Their potassium intake may be as high as 200 mmol/day.
- Their diet contains large amounts of fruits and vegetables.
- Their diet contains no processed foods.
- Populations consuming this type of diet usually do not develop age-related increases in blood pressure.
- These populations also have a low incidence of cardiovascular diseases.
- Industrialization has increased the consumption of processed foods.
- Processed foods often contain high sodium and low potassium.
- Sodium intake has increased markedly with industrialization.
- Potassium intake has decreased markedly with industrialization.
- In most industrialized countries, potassium intake averages 30 to 70 mmol/day.
- In most industrialized countries, sodium intake averages 140 to 180 mmol/day.
- Experimental studies have shown that a high-sodium and low-potassium diet increases the risk of hypertension.
- This dietary pattern also increases the risk of cardiovascular disease.
- This dietary pattern also increases the risk of kidney disease.
- A potassium-rich diet helps protect against the harmful effects of a high-sodium diet.
- Increased potassium intake reduces blood pressure.
- Increased potassium intake reduces the risk of stroke.
- Increased potassium intake reduces the risk of coronary artery disease.
- Increased potassium intake reduces the risk of kidney disease.
- The beneficial effects of potassium are greatest when combined with a low-sodium diet.
- Dietary guidelines recommend reducing sodium chloride intake to about 65 to 100 mmol/day.
- This corresponds to 1.5–2.3 g/day of sodium.
- This corresponds to 3.8–5.8 g/day of sodium chloride.
- Dietary guidelines recommend increasing potassium intake to 120 mmol/day.
- This corresponds to 4.7 g/day of potassium for healthy adults.
KEY CONCEPT
- Acute acidosis decreases potassium secretion and excretion.
- Chronic acidosis increases potassium secretion and potassium loss.
- Diets high in potassium and low in sodium help maintain normal blood pressure.
- High-potassium diets reduce the risk of cardiovascular and kidney diseases.
- The greatest health benefits occur when high potassium intake is combined with low sodium intake.