


- The kidneys can make concentrated urine.
- This ability is essential for the survival of land mammals, including humans.
- Water is continuously lost from the body.
- Water is lost through the lungs during breathing.
- Water is lost through the gastrointestinal tract in feces.
- Water is lost through the skin by evaporation and sweating.
- Water is lost through the kidneys in urine.
- Fluid intake must replace the water that is lost.
- The kidneys can reduce water loss by producing a small volume of concentrated urine.
- This decreases the amount of water that must be consumed.
- This function is especially important when water is scarce.
- When the body has a water deficit, the kidneys produce concentrated urine.
- The kidneys continue to excrete solutes.
- The kidneys increase water reabsorption.
- The kidneys decrease urine volume.
- Human kidneys can concentrate urine up to 1200–1400 mOsm/L.
- This is about 4–5 times the osmolarity of plasma.
- Some desert animals can concentrate urine much more than humans.
- The Australian hopping mouse can concentrate urine up to 10,000 mOsm/L.
- This allows the mouse to survive in the desert without drinking water.
- The mouse obtains enough water from food.
- Additional water is produced during metabolism of food.
- Animals that live in freshwater environments have a limited ability to concentrate urine.
- Beavers can concentrate urine only up to about 500 mOsm/L.
KEY CONCEPT
- Kidneys conserve water by increasing water reabsorption and producing concentrated urine.
- Concentrated urine helps maintain body fluid balance when water is limited.
- Humans can concentrate urine up to 1200–1400 mOsm/L.
- Desert animals have a much greater urine-concentrating ability than freshwater animals.
OBLIGATORY URINE VOLUME
- The maximum urine-concentrating ability of the kidney determines the minimum urine volume that must be excreted each day.
- This urine is needed to remove metabolic waste products and ingested electrolytes from the body.
- A 70-kg person on a normal diet must excrete about 600 mOsm of solute each day.
- If the maximum urine concentration is 1200 mOsm/L, the minimum urine volume can be calculated.
- 600 mOsm/day ÷ 1200 mOsm/L = 0.5 L/day
- This minimum urine volume is called the obligatory urine volume.
- This unavoidable urine loss contributes to dehydration when drinking water is unavailable.
- Additional water is also lost through the skin.
- Water is lost through the respiratory tract.
- Water is lost through the gastrointestinal tract.
- The human kidney can concentrate urine only up to about 1200 mOsm/L.
- This limited concentrating ability explains why drinking seawater causes severe dehydration.
- The sodium chloride concentration of seawater is about 3.0% to 3.5%.
- The osmolarity of seawater is about 1000–1200 mOsm/L.
- Drinking 1 liter of seawater with an osmolarity of 1200 mOsm/L provides 1200 mOsm of sodium chloride.
- If the kidney can concentrate urine to 1200 mOsm/L, 1 liter of urine would be needed to excrete 1200 mOsm of sodium chloride.
- However, drinking seawater still causes dehydration.
- The kidney must also excrete other solutes.
- Urea is an important additional solute.
- When urine is maximally concentrated, other solutes contribute about 600 mOsm/L.
- Therefore, the maximum sodium chloride concentration that can be excreted by the kidneys is about 600 mOsm/L.
- For every liter of seawater consumed, the kidneys must excrete 1200 mOsm of sodium chloride.
- The kidneys must also excrete 600 mOsm of other solutes such as urea.
- A total of 1800 mOsm must be excreted.
- To excrete 1800 mOsm at a maximum urine concentration of 1200 mOsm/L, 1.5 liters of urine are required.
- Thus, drinking 1 liter of seawater leads to the production of 1.5 liters of urine.
- This causes a net loss of 0.5 liter of body fluid.
- This explains the rapid dehydration that occurs in people who drink seawater after a shipwreck.
KEY CONCEPT
- Obligatory urine volume = minimum urine volume required to excrete daily solutes.
- For a normal person: 600 mOsm/day ÷ 1200 mOsm/L = 0.5 L/day.
- Drinking seawater increases solute load beyond what the kidneys can efficiently remove.
- Excreting seawater salt requires more water than is gained from the seawater.
- Therefore, seawater consumption causes net water loss and dehydration.
URINE SPECIFIC GRAVITY
- Urine specific gravity is commonly used in clinical practice.
- It provides a quick estimate of urine solute concentration.
- The more concentrated the urine, the higher the urine specific gravity.
- In most cases, urine specific gravity increases as urine osmolarity increases.
- Urine specific gravity measures the weight of solutes in a given volume of urine.
- Urine specific gravity depends on:
- The number of solute molecules.
- The size of solute molecules.
- Osmolarity depends only on the number of solute molecules in a given volume.
- Urine specific gravity is usually expressed in grams per milliliter (g/mL).
- In humans, normal urine specific gravity ranges from 1.002 to 1.028 g/mL.
- Urine specific gravity increases by about 0.001 for every 35–40 mOsm/L increase in urine osmolarity.
- The relationship between urine specific gravity and osmolarity can change when large molecules are present in the urine.
- Examples of large molecules include:
- Glucose.
- Radiocontrast media used for diagnostic tests.
- Some antibiotics.
- In these situations, urine specific gravity may falsely indicate highly concentrated urine.
- This false increase can occur even when urine osmolality is normal.
- Dipsticks can be used to estimate urine specific gravity.
- Most laboratories measure urine specific gravity using a refractometer.
KEY CONCEPT
- Urine specific gravity is a quick clinical indicator of urine concentration.
- Higher urine concentration usually means higher specific gravity.
- Specific gravity depends on both the number and size of solute molecules.
- Osmolarity depends only on the number of solute molecules.
- Large molecules in urine can falsely increase specific gravity without increasing urine osmolality significantly.
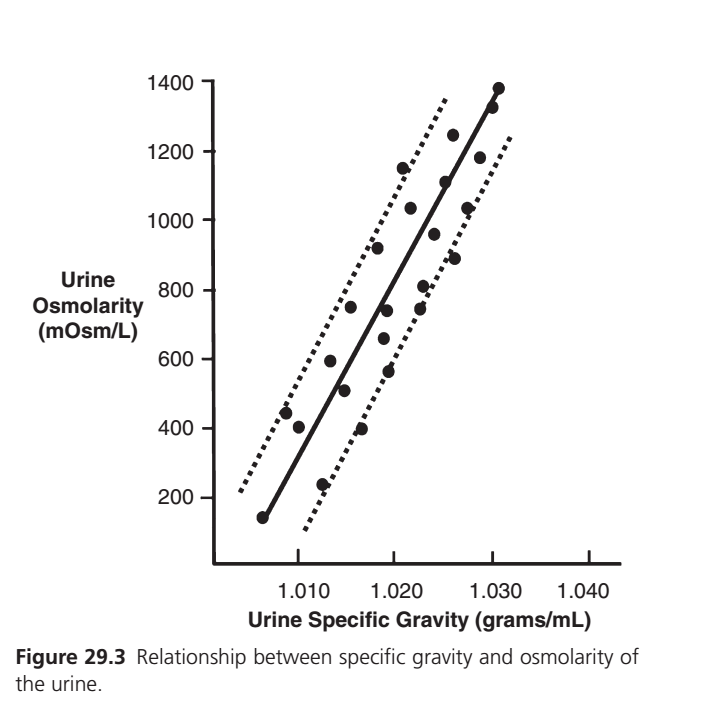
Figure 29.3 — Relationship Between Urine Specific Gravity and Urine Osmolarity
This graph shows a very important renal physiology concept:
As urine becomes more concentrated, both urine osmolarity and urine specific gravity increase.
In simple words:
Concentrated urine = More dissolved particles = Higher osmolarity + Higher specific gravity
Step 1: Understand the Axes
Y-Axis (Vertical)
Urine Osmolarity (mOsm/L)
This measures:
Number of dissolved particles in urine
Examples:
- Sodium
- Chloride
- Potassium
- Urea
Low Osmolarity
Example:
100 mOsm/L
Means:
✅ Few solute particles
✅ Dilute urine
✅ Lots of waterHigh Osmolarity
Example:
1200–1400 mOsm/L
Means:
✅ Many solute particles
✅ Concentrated urine
✅ Little water
X-Axis (Horizontal)
Urine Specific Gravity (g/mL)
Specific gravity compares:
Weight of urine
vs
Weight of pure water
Pure Water
Specific gravity = 1.000
Dilute Urine
Specific gravity ≈ 1.005–1.010
Almost like water.
Concentrated Urine
Specific gravity ≈ 1.025–1.030
Contains many dissolved substances.
Therefore heavier than water.
WHAT ARE THE BLACK CIRCLES? ⚫
The black circles are:
Actual Urine Samples
Each circle represents:
One urine measurement from a person
For each sample:
- Specific gravity was measured
- Osmolarity was measured
Then plotted on the graph.
Example
One urine sample:
Specific gravity = 1.010
Osmolarity = 400 mOsm/L
↓
One black dot appears there.
Another sample:
Specific gravity = 1.025
Osmolarity = 1000 mOsm/L
↓
Another black dot appears there.
Why Are Dots Scattered?
Because urine composition differs between people.
Some urine contains:
- More urea
- More glucose
- More protein
- Different electrolytes
Therefore:
The relationship is not perfectly identical in every sample.
KEY IDEA OF BLACK CIRCLES
Each black circle = one real urine sample.
The dots show actual experimental data.
WHAT IS THE SOLID BLACK LINE? ─
This is the most important line.
It is called:
Best-Fit Line (Regression Line)
It shows the average relationship between:
- Specific gravity
- Osmolarity
What Does It Tell Us?
As specific gravity increases:
Urine osmolarity also increases.
Example
Specific gravity:
1.010
↓
Osmolarity about:
300–400 mOsm/L
Specific gravity:
1.020
↓
Osmolarity about:
700–800 mOsm/L
Specific gravity:
1.030
↓
Osmolarity about:
1300–1400 mOsm/L
KEY IDEA OF SOLID BLACK LINE
Higher specific gravity = Higher urine osmolarity.
This is why clinicians can estimate urine concentration using specific gravity.
WHAT ARE THE DOTTED LINES? ⋯⋯⋯
The two dotted lines form a band around the solid line.
These are:
Normal Variation Limits
(or confidence/prediction limits)
They show the expected range where most urine samples will fall.
Upper Dotted Line
Represents:
Higher-than-average osmolarity for a given specific gravity.
Lower Dotted Line
Represents:
Lower-than-average osmolarity for a given specific gravity.
Why Are They Needed?
Because not all urine samples behave exactly the same.
Example
Specific Gravity = 1.020
Average osmolarity from solid line:
≈ 750 mOsm/L
But actual samples may be:
- 650 mOsm/L
- 800 mOsm/L
- 900 mOsm/L
Therefore the dotted lines show:
“Most samples should fall somewhere in this range.”
KEY IDEA OF DOTTED LINES
They show biological variation around the average relationship.
How to Read This Graph Clinically
Suppose urine specific gravity is:
1.010
Follow upward to the solid line.
Estimated urine osmolarity:
≈ 300–400 mOsm/L
Suppose urine specific gravity is:
1.020
Estimated osmolarity:
≈ 700–800 mOsm/L
Suppose urine specific gravity is:
1.030
Estimated osmolarity:
≈ 1300–1400 mOsm/L
Why Do Doctors Use Specific Gravity?
Because it is:
✅ Quick
✅ Cheap
✅ Easy
✅ Available in routine urinalysis
Measuring osmolarity directly requires laboratory equipment.
Specific gravity provides a rapid estimate.
Important Guyton Concept
Urine specific gravity generally increases linearly with urine osmolarity because:
The more solute particles present in urine, the heavier and more concentrated the urine becomes.
Therefore:
↑ Urine osmolarity
→ ↑ Urine specific gravity
↓
Dilute urine:
- Low osmolarity
- Low specific gravity
↓
Concentrated urine:
- High osmolarity
- High specific gravity
One-Line Exam Concept
The black circles represent actual urine samples, the solid black line represents the average (best-fit) relationship between urine specific gravity and urine osmolarity, and the dotted lines represent the normal range of variation around this relationship; as urine specific gravity increases, urine osmolarity increases almost linearly.
EXCRETING CONCENTRATED URINE REQUIRES HIGH ADH LEVELS AND HYPEROSMOTIC RENAL MEDULLA
- Two basic requirements are necessary to form concentrated urine.
- The first requirement is a high level of ADH.
- ADH increases the permeability of the distal tubules to water.
- ADH increases the permeability of the collecting ducts to water.
- Increased water permeability allows these tubular segments to reabsorb large amounts of water.
- The second requirement is a high osmolarity of the renal medullary interstitial fluid.
- The high osmolarity creates the osmotic gradient needed for water reabsorption.
- This osmotic gradient is effective when ADH levels are high.
- The renal medullary interstitium surrounding the collecting ducts is normally hyperosmotic.
- When ADH levels are high, water moves out of the tubules by osmosis.
- Water passes through the tubular membrane into the renal interstitium.
- Water is then carried away by the vasa recta.
- The vasa recta returns the reabsorbed water to the blood.
- The kidney’s ability to concentrate urine depends on the level of ADH.
- The kidney’s ability to concentrate urine also depends on the degree of hyperosmolarity in the renal medulla.
- The renal medullary interstitial fluid becomes hyperosmotic through a specific process.
- This process is called the countercurrent multiplier mechanism.
KEY CONCEPT
- Concentrated urine requires:
- High ADH levels.
- A hyperosmotic renal medulla.
- ADH allows more water to be reabsorbed from distal tubules and collecting ducts.
- The hyperosmotic renal medulla provides the osmotic force for water reabsorption.
- Water moves from the tubules → renal interstitium → vasa recta → blood.
- The countercurrent multiplier mechanism creates the hyperosmotic renal medulla.
SUMMARY
EXCRETING CONCENTRATED URINE REQUIRES HIGH ADH LEVELS AND A HYPEROSMOTIC RENAL MEDULLA
The kidneys can conserve water by producing a small volume of concentrated urine. This ability is extremely important when the body is losing water or when water intake is low. To make concentrated urine, two conditions must be present: a high level of Antidiuretic Hormone (ADH) and a hyperosmotic (highly concentrated) renal medulla.
ADH acts on the distal tubules and collecting ducts of the kidneys. When ADH levels are high, these tubular segments become highly permeable to water. As a result, large amounts of water move out of the tubular fluid and are reabsorbed back into the body. This decreases urine volume and makes the urine more concentrated.
However, ADH alone is not enough. There must also be a strong osmotic force to pull water out of the tubules. This force is provided by the hyperosmotic renal medulla. The interstitial fluid in the renal medulla contains a very high concentration of solutes compared with the fluid inside the tubules.
Because of this concentration difference, water moves by osmosis from the collecting ducts into the renal medullary interstitium whenever ADH is present. After leaving the tubules, the reabsorbed water enters the vasa recta and is carried back into the bloodstream.
Therefore, the kidney’s ability to produce concentrated urine depends on two factors:
- High ADH levels that make the tubules permeable to water.
- A hyperosmotic renal medulla that provides the osmotic gradient needed for water reabsorption.
The hyperosmotic renal medulla is created by a special process known as the countercurrent multiplier mechanism, which establishes and maintains a high solute concentration in the renal medulla.
Example 1: Dehydration
Suppose a person is lost in a desert and cannot drink water. The body becomes dehydrated, causing ADH secretion to increase. ADH makes the collecting ducts highly permeable to water. Because the renal medulla is hyperosmotic, water is pulled out of the collecting ducts and returned to the blood. As a result, only a small amount of highly concentrated urine is produced, helping conserve body water.
Example 2: Drinking Very Little Water
If a person drinks very little water during the day, ADH levels rise. More water is reabsorbed from the distal tubules and collecting ducts. Urine volume decreases and becomes dark yellow and concentrated because less water is lost.
Example 3: Lack of ADH
If ADH is absent or very low, the collecting ducts become poorly permeable to water. Even if the renal medulla is hyperosmotic, water cannot be reabsorbed effectively. Large amounts of dilute urine are excreted.
KEY CONCEPT
- Concentrated urine formation requires:
- High ADH levels.
- A hyperosmotic renal medulla.
- ADH makes distal tubules and collecting ducts highly permeable to water.
- The hyperosmotic renal medulla provides the osmotic force that pulls water out of the tubules.
- Reabsorbed water enters the renal interstitium and then the vasa recta before returning to the blood.
- The more ADH and the greater the medullary hyperosmolarity, the more concentrated the urine becomes.
- The hyperosmotic renal medulla is produced by the countercurrent multiplier mechanism.