


- Cells function normally only when they are surrounded by extracellular fluid with a relatively constant concentration of electrolytes and other solutes.
- The total concentration of solutes in extracellular fluid (osmolarity) must be carefully regulated.
- Proper osmolarity prevents cells from shrinking or swelling.
- Osmolarity depends on the amount of solute divided by the volume of extracellular fluid.
- Sodium chloride is the main solute that determines extracellular fluid osmolarity.
- Extracellular fluid osmolarity and sodium chloride concentration are mainly regulated by the amount of extracellular water.
- Total body water is controlled by fluid intake.
- Fluid intake is regulated by factors that determine thirst.
- Total body water is also controlled by renal water excretion.
- Renal water excretion is controlled by factors that affect glomerular filtration.
- Renal water excretion is also controlled by factors that affect tubular reabsorption.
- This chapter discusses how the kidneys eliminate excess water by excreting dilute urine.
- This chapter discusses how the kidneys conserve water by excreting concentrated urine.
- This chapter discusses feedback mechanisms that control extracellular fluid sodium concentration and osmolarity.
- This chapter discusses thirst and salt appetite mechanisms that regulate water and salt intake.
- Water and salt intake help control extracellular fluid volume.
- Water and salt intake help control extracellular fluid osmolarity.
- Water and salt intake help control extracellular fluid sodium concentration.
- Normal kidneys can greatly vary the proportions of solutes and water in the urine.
- When excess water is present and body fluid osmolarity decreases, the kidneys excrete very dilute urine.
- The osmolarity of dilute urine can be as low as 50 mOsm/L.
- This urine concentration is about one-sixth of normal extracellular fluid osmolarity.
- When body water is deficient and extracellular fluid osmolarity increases, the kidneys excrete highly concentrated urine.
- The osmolarity of concentrated urine can reach 1200–1400 mOsm/L.
- The kidneys can excrete a large volume of dilute urine without major changes in solute excretion.
- The kidneys can excrete a small volume of concentrated urine without major changes in solute excretion.
- Sodium excretion can remain relatively unchanged during these adjustments.
- Potassium excretion can remain relatively unchanged during these adjustments.
- The kidneys can regulate water excretion independently of solute excretion.
- This ability is essential for survival.
- This ability is especially important when fluid intake is limited.
KEY CONCEPT
- Cells require a stable extracellular fluid environment.
- Extracellular fluid osmolarity depends mainly on water balance.
- Thirst controls water intake.
- Kidneys control water excretion.
- Kidneys can produce very dilute or very concentrated urine.
- Water excretion can be regulated independently of solute excretion.
- This mechanism is vital for maintaining body fluid balance and survival.
ANTIDIURETIC HORMONE CONTROLS URINE CONCENTRATION
- The body has a powerful feedback system that regulates plasma osmolarity and sodium concentration.
- This feedback system works by changing renal water excretion independently of solute excretion.
- Antidiuretic hormone (ADH) is a major effector of this feedback system.
- ADH is also called vasopressin.
- When body fluid osmolarity rises above normal, body fluids become more concentrated.
- Increased osmolarity stimulates the posterior pituitary gland to secrete more ADH.
- Increased ADH raises the permeability of the distal tubules to water.
- Increased ADH raises the permeability of the collecting ducts to water.
- Increased water permeability causes more water to be reabsorbed.
- Increased water reabsorption decreases urine volume.
- Increased ADH does not markedly change the rate of solute excretion by the kidneys.
- When excess water is present in the body, extracellular fluid osmolarity decreases.
- Reduced extracellular fluid osmolarity decreases ADH secretion from the posterior pituitary gland.
- Reduced ADH lowers the permeability of the distal tubules to water.
- Reduced ADH lowers the permeability of the collecting ducts to water.
- Reduced water permeability causes less water to be reabsorbed.
- Less water reabsorption leads to excretion of larger amounts of dilute urine.
- The rate of ADH secretion largely determines whether the kidneys produce dilute urine.
- The rate of ADH secretion largely determines whether the kidneys produce concentrated urine.
KEY CONCEPT
- ADH (vasopressin) is the main hormone controlling urine concentration.
- High osmolarity increases ADH secretion.
- Increased ADH increases water reabsorption and decreases urine volume.
- Low osmolarity decreases ADH secretion.
- Decreased ADH causes excretion of large volumes of dilute urine.
- ADH determines whether urine is dilute or concentrated.
RENAL MECHANISMS FOR EXCRETING DILUTE URINE
- When there is a large excess of water in the body, the kidneys can excrete up to 20 L/day of dilute urine.
- The osmolarity of this dilute urine can be as low as 50 mOsm/L.
- The kidneys achieve this by continuing to reabsorb solutes.
- The kidneys do not reabsorb large amounts of water in the late distal tubule and collecting ducts.
- After ingestion of 1 liter of water, urine volume increases significantly.
- Urine volume rises to about six times the normal level within 45 minutes.
- The total amount of solute excreted remains relatively constant.
- The urine becomes more dilute after water ingestion.
- Urine osmolarity decreases from about 600 to 100 mOsm/L.
- After excess water intake, the kidneys remove the extra water from the body.
- The kidneys do not excrete substantially greater amounts of solutes.
- Cells require extracellular fluid with a relatively constant concentration of electrolytes and other solutes.
- Extracellular fluid osmolarity must be carefully regulated.
- Proper osmolarity prevents cells from shrinking.
- Proper osmolarity prevents cells from swelling.
- Osmolarity is determined by the amount of solute divided by the volume of extracellular fluid.
- Sodium chloride is the main solute contributing to extracellular fluid osmolarity.
- Extracellular fluid osmolarity is largely regulated by the amount of extracellular water.
- Sodium chloride concentration is also largely regulated by the amount of extracellular water.
- Total body water is controlled by fluid intake.
- Fluid intake is regulated by factors that determine thirst.
- Total body water is also controlled by renal water excretion.
- Renal water excretion is influenced by factors affecting glomerular filtration.
- Renal water excretion is influenced by factors affecting tubular reabsorption.
- This chapter discusses renal mechanisms for eliminating excess water through dilute urine formation.
- This chapter discusses renal mechanisms for conserving water through concentrated urine formation.
- This chapter discusses feedback mechanisms controlling extracellular fluid sodium concentration and osmolarity.
- This chapter discusses thirst and salt appetite mechanisms that regulate water and salt intake.
- Water and salt intake help control extracellular fluid volume.
- Water and salt intake help control extracellular fluid osmolarity.
- Water and salt intake help control extracellular fluid sodium concentration.
- Normal kidneys can greatly vary the proportions of water and solutes in urine.
- When excess water is present and body fluid osmolarity decreases, the kidneys produce very dilute urine.
- Dilute urine can have an osmolarity as low as 50 mOsm/L.
- This osmolarity is about one-sixth that of normal extracellular fluid.
- When body water is deficient and extracellular fluid osmolarity rises, the kidneys produce highly concentrated urine.
- Concentrated urine can have an osmolarity of 1200 to 1400 mOsm/L.
- The kidneys can excrete large volumes of dilute urine without major changes in solute excretion.
- The kidneys can excrete small volumes of concentrated urine without major changes in solute excretion.
- Sodium excretion can remain relatively unchanged during these adjustments.
- Potassium excretion can remain relatively unchanged during these adjustments.
- The kidneys regulate water excretion independently of solute excretion.
- This ability is essential for survival.
- This ability is especially important when fluid intake is limited.
- Glomerular filtrate is initially formed with an osmolarity of about 300 mOsm/L.
- The initial osmolarity of glomerular filtrate is approximately the same as plasma.
- To excrete excess water, the filtrate becomes diluted as it moves through the tubules.
- Filtrate dilution occurs because solutes are reabsorbed more than water.
- Dilution occurs only in specific segments of the tubular system.
KEY CONCEPT
- Excess body water leads to excretion of large volumes of dilute urine.
- Kidneys dilute urine by reabsorbing solutes without reabsorbing equivalent amounts of water.
- Urine osmolarity can decrease to as low as 50 mOsm/L.
- The kidneys remove excess water while keeping solute excretion relatively constant.
- Glomerular filtrate starts at about 300 mOsm/L and becomes diluted in specific nephron segments.
- Kidneys can regulate water excretion independently of solute excretion.
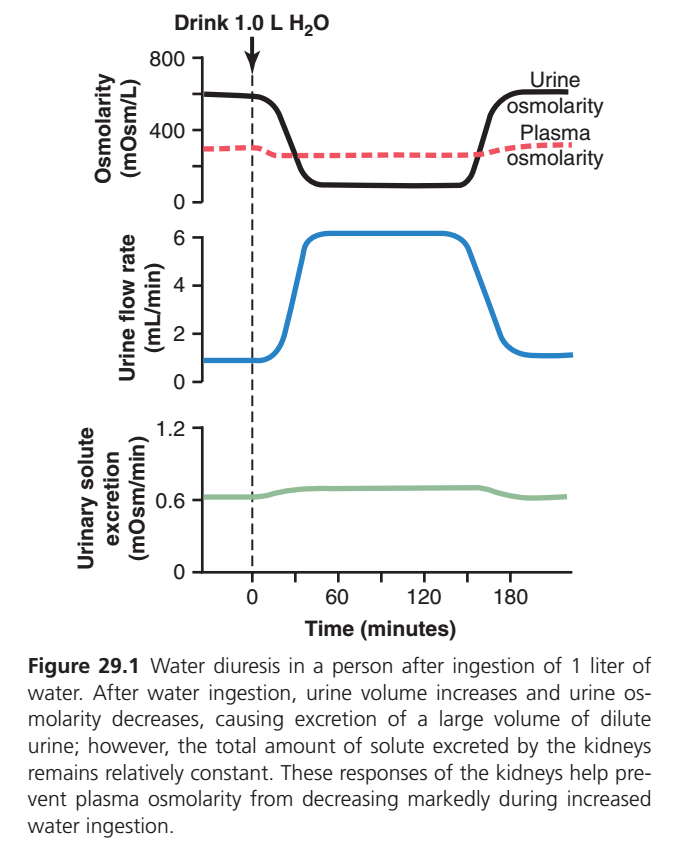
Figure 29.1 — What Happens After Drinking 1 Liter of Water?
This graph shows how the kidneys respond when a person drinks 1 liter of water at time 0 minutes.
The kidneys have one main goal:
✅ Remove extra water
✅ Keep body osmolarity almost normal
✅ Avoid losing important solutes (Na⁺, Cl⁻, etc.)
First Understand the Axes
X-axis (Horizontal)
Time (minutes)
- 0 = water is consumed
- Graph follows the body’s response for about 3 hours
TOP GRAPH: Osmolarity
Y-axis = Osmolarity (mOsm/L)
This graph has 2 lines:
🔴 Dotted Red Line = Plasma Osmolarity
⚫ Black Line = Urine Osmolarity
🔴 DOTTED RED LINE (Plasma Osmolarity)
This is the osmolarity of the blood plasma.
Normally ≈ 300 mOsm/L
Before Drinking Water
Plasma osmolarity is normal.
Think:
Normal amount of water + Normal amount of solute
≈ 300 mOsm/L
After Drinking 1 L Water
Extra water enters blood.
Now:
- Water increases
- Solutes stay same
Therefore plasma becomes slightly diluted.
Plasma osmolarity falls a little.
Example:
300 → 290 mOsm/L
Why Doesn’t It Fall Much More?
Because kidneys immediately start removing excess water.
So plasma osmolarity stays close to normal.
This is why the red dotted line only shows a small decrease.
Later
After excess water is excreted:
- Water balance returns
- Plasma osmolarity returns toward normal
Therefore the red dotted line rises back.
KEY IDEA OF RED DOTTED LINE
Blood osmolarity changes only slightly.
Because kidneys rapidly remove excess water.
⚫ BLACK LINE (Urine Osmolarity)
This is the concentration of urine.
Before Drinking Water
Urine is relatively concentrated.
≈ 600 mOsm/L
This means:
- Body is conserving water
- Urine contains lots of solutes relative to water
After Drinking 1 L Water
Body suddenly has excess water.
Hypothalamus senses:
↓ Plasma osmolarity
↓
ADH secretion decreases
↓
Collecting ducts become less permeable to water
↓
Less water reabsorbed
↓
More water stays in urine
Result
Urine becomes very dilute.
Urine osmolarity drops dramatically.
Approximately:
600 → 100 mOsm/L
The black line falls sharply.
During Water Diuresis
Urine remains very dilute.
The kidney is trying to get rid of excess water.
Later
Once extra water is removed:
- ADH returns
- Water reabsorption increases again
Urine becomes concentrated.
So the black line rises back toward 600 mOsm/L.
KEY IDEA OF BLACK LINE
Urine osmolarity changes A LOT.
Because kidneys dilute urine to remove excess water.
MIDDLE GRAPH: Urine Flow Rate (Blue Line)
Y-axis = mL/min
🔵 Blue Line = Urine Flow Rate
This tells us how much urine is produced every minute.
Before Drinking Water
Urine flow is low.
≈ 1 mL/min
Normal urine production.
After Drinking Water
ADH falls.
Less water reabsorbed.
Large amount of water remains in tubules.Result
Urine volume rises sharply.
≈ 1 → 6 mL/min
The blue line shoots upward.
During Water Diuresis
Large volume of dilute urine is excreted.
This is called:
Water Diuresis
Meaning:
Excretion of excess water without losing much solute.
Later
Excess water removed.
ADH rises back.
Urine flow decreases.
Blue line returns near baseline.
KEY IDEA OF BLUE LINE
More water in body → More urine produced.
BOTTOM GRAPH: Urinary Solute Excretion
Y-axis = mOsm/min
🟢 Green Line = Solute Excretion Rate
This shows how much dissolved material is excreted.
Examples:
- Sodium
- Chloride
- Potassium
- Urea
Before Drinking Water
About:
0.6 mOsm/min
After Drinking Water
Notice something important.
The green line changes very little.
It stays almost flat.
Why?
The kidneys are trying to remove:
❌ Water
NOT
❌ Sodium
NOT
❌ Other solutes
Therefore:
- Water excretion increases greatly
- Solute excretion remains almost unchanged
KEY IDEA OF GREEN LINE
The kidney removes extra water while conserving most solutes.
Putting All Lines Together
Step 1: Drink 1 Liter Water
↓
Step 2: Plasma becomes slightly diluted
🔴 Plasma osmolarity decreases a little
↓
Step 3: ADH secretion decreases
↓
Step 4: Collecting ducts reabsorb less water
↓
Step 5: Large amount of water enters urine
🔵 Urine flow increases greatly
↓
Step 6: Urine becomes dilute
⚫ Urine osmolarity decreases dramatically
↓
Step 7: Solute excretion remains almost unchanged
🟢 Green line stays nearly flat
↓
Step 8: Excess water leaves body
↓
Step 9: Plasma osmolarity returns toward normal
↓
Step 10: Urine flow and urine osmolarity return to baseline
One-Sentence Exam Concept
After drinking 1 liter of water, plasma osmolarity (🔴 dotted line) decreases only slightly, urine osmolarity (⚫ black line) decreases markedly, urine flow rate (🔵 blue line) increases greatly, and urinary solute excretion (🟢 green line) remains nearly constant because the kidneys excrete excess water without losing significant solutes.
Formation of Dilute Urine (When ADH is Very Low) – Easiest Concept
🎯 Main Idea
When ADH (Antidiuretic Hormone) is very low or absent, the kidneys:
✅ Reabsorb salt (NaCl)
❌ Do NOT reabsorb much water
As a result:
➡️ More water stays inside the tubule
➡️ Urine becomes very dilute (watery)
➡️ Large volume of urine is produced
Step-by-Step Journey of Tubular Fluid
1. Proximal Tubule
What happens?
- NaCl is reabsorbed
- Water is also reabsorbed
Both leave together.
Osmolarity
300 mOsm/L → remains 300 mOsm/L
Why?
Water follows sodium.
👉 Fluid concentration does not change.
Remember:
“Salt out + Water out = No change in concentration”
2. Descending Loop of Henle
What happens?
- Highly permeable to water
- Almost impermeable to NaCl
Water leaves the tubule.
Osmolarity Changes
- Start = 300
- Middle = 400
- Bottom = 600
Why?
Water is removed but salt remains.
So fluid becomes more concentrated.
Easy Memory
Descending limb = Water leaves
💧⬅️
Result:
300 → 400 → 600
3. Ascending Loop of Henle
What happens?
- NaCl leaves
- Water cannot follow
This is the “diluting segment.”
Osmolarity Changes
- Bottom = 600
- Upper ascending = 400
- Early distal tubule = 100
Why?
Salt is removed but water stays.
Fluid becomes increasingly dilute.
Easy Memory
Ascending limb = Salt leaves
🧂⬅️
Result:
600 → 400 → 100
Most Important Concept
At the start of the Distal Tubule
Tubular fluid is already very dilute:
= 100 mOsm/L
This is called:
⭐ Diluting Segment of Nephron
Because salt is removed without water.
4. Distal Tubule (ADH Low)
What happens?
- More NaCl is reabsorbed
- Water cannot be reabsorbed
Osmolarity
100 → around 80–70 mOsm/L
Fluid becomes even more dilute.
5. Collecting Duct (ADH Very Low)
What happens?
- Some additional NaCl reabsorbed
- Water channels (Aquaporins) are absent because ADH is low
Therefore:
❌ Water stays in tubule
✅ Salt leaves
Osmolarity
70 → 50 mOsm/L
Final Urine
Urine Osmolarity
≈ 50 mOsm/L
This is extremely dilute urine.
Urine Volume
Can be as much as:
✅ 15–20 liters/day
if excess water is present.
Understanding the Numbers in the Figure
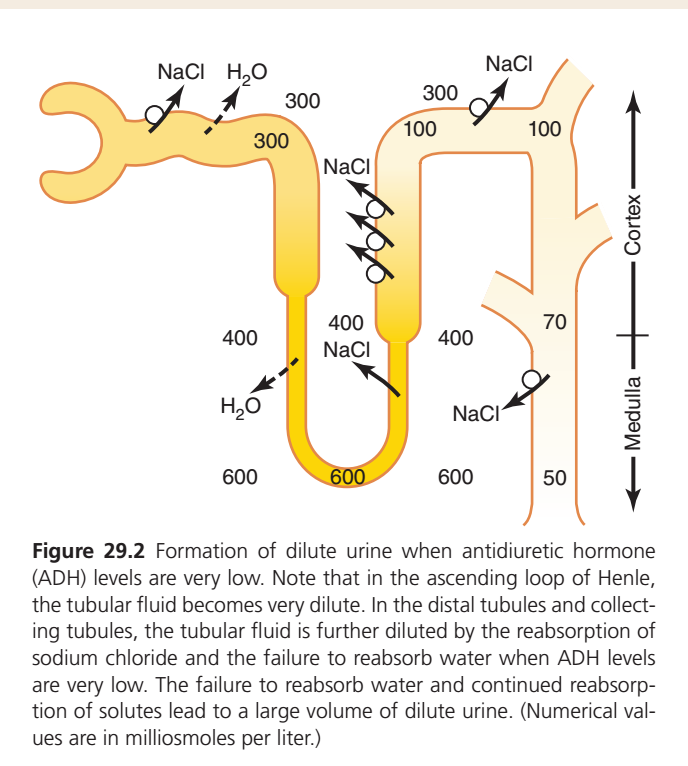
The numbers (300, 400, 600, 100, 70, 50) represent:
Osmolarity (mOsm/L)
Meaning:
How concentrated the tubular fluid is at that point.
| Number | Meaning |
|---|---|
| 300 | Normal body fluid concentration |
| 400 | More concentrated |
| 600 | Very concentrated |
| 100 | Dilute |
| 70 | More dilute |
| 50 | Extremely dilute urine |
What Do the Arrows Mean?
H₂O Arrows
💧
Water is leaving the tubule.
Seen mainly in:
- Proximal tubule
- Descending loop
NaCl Arrows
🧂
Salt is leaving the tubule.
Seen mainly in:
- Thick ascending limb
- Distal tubule
- Collecting duct
Cortex vs Medulla
The right-side arrow shows kidney regions.
Cortex (Upper Part)
- Osmolarity ≈ 300 mOsm/L
Medulla (Deeper Part)
- Osmolarity increases gradually
300 → 400 → 600
This concentrated medulla pulls water out of the descending limb.
One-Line Story of the Whole Figure
Low ADH = Salt removed + Water retained in tubule
Therefore:
300 → 600 → 100 → 70 → 50
and the kidney produces a large volume of very dilute urine (≈50 mOsm/L).
KEY CONCEPT
Descending limb loses water → fluid becomes concentrated (300→600).
Ascending limb loses salt but not water → fluid becomes dilute (600→100).
With low ADH, distal tubule and collecting duct continue removing salt but cannot remove water → urine becomes extremely dilute (100→70→50 mOsm/L).
Result = Large volume of dilute urine. 🚰💧
TUBULAR FLUID REMAINS ISOSMOTIC IN PROXIMAL TUBULES
- As fluid flows through the proximal tubule, solutes are reabsorbed.
- Water is also reabsorbed in the proximal tubule.
- Solutes and water are reabsorbed in equal proportions.
- Because solutes and water are reabsorbed equally, little change occurs in osmolarity.
- The fluid in the proximal tubule remains isosmotic with plasma.
- The osmolarity of proximal tubular fluid remains about 300 mOsm/L.
- As fluid moves down the descending loop of Henle, water is reabsorbed by osmosis.
- Water moves out of the tubule into the surrounding tissues.
- The tubular fluid reaches equilibrium with the surrounding renal medullary interstitial fluid.
- The interstitial fluid of the renal medulla is highly hypertonic.
- The osmolarity of the renal medullary interstitial fluid is about two to four times greater than the original glomerular filtrate.
- As more water leaves the descending loop, the tubular fluid becomes more concentrated.
- The tubular fluid continues to become more concentrated as it flows toward the inner medulla.
KEY CONCEPT
- In the proximal tubule, water and solutes are reabsorbed equally.
- Therefore, proximal tubular fluid remains isosmotic with plasma (~300 mOsm/L).
- In the descending loop of Henle, water is reabsorbed by osmosis.
- The renal medulla is highly hypertonic.
- Loss of water from the tubule makes the tubular fluid progressively more concentrated as it enters the inner medulla.
TUBULAR FLUID IS DILUTED IN THE ASCENDING LOOP OF HENLE
- In the ascending limb of the loop of Henle, sodium is actively reabsorbed.
- In the ascending limb of the loop of Henle, potassium is actively reabsorbed.
- In the ascending limb of the loop of Henle, chloride is actively reabsorbed.
- Reabsorption of these ions is especially strong in the thick ascending segment.
- The ascending limb is impermeable to water.
- Water cannot be reabsorbed from this segment.
- This impermeability to water remains even when large amounts of ADH are present.
- Solutes are removed from the tubular fluid without water following them.
- As a result, the tubular fluid becomes progressively more dilute.
- The tubular fluid becomes more dilute as it moves up the ascending loop of Henle.
- Dilution continues as the fluid enters the early distal tubule.
- The osmolarity of the tubular fluid gradually decreases.
- By the time the fluid reaches the early distal tubule, its osmolarity is about 100 mOsm/L.
- Fluid leaving the early distal tubule is hypo-osmotic.
- This occurs whether ADH is present or absent.
- The osmolarity of the fluid leaving the early distal tubule is about one-third that of plasma.
KEY CONCEPT
- The thick ascending limb actively reabsorbs sodium, potassium, and chloride.
- The ascending limb is impermeable to water, even in the presence of ADH.
- Solute reabsorption without water reabsorption dilutes the tubular fluid.
- Tubular fluid osmolarity falls to about 100 mOsm/L in the early distal tubule.
TUBULAR FLUID IN DISTAL AND COLLECTING TUBULES IS FURTHER DILUTED IN THE ABSENCE OF ADH
- Dilute fluid from the early distal tubule enters the late distal convoluted tubule.
- The fluid then passes into the cortical collecting duct.
- The fluid then passes into the medullary collecting duct.
- Additional sodium chloride is reabsorbed in these segments.
- In the absence of ADH, these tubular segments are impermeable to water.
- Water is not reabsorbed from these segments when ADH is absent.
- Sodium chloride continues to be reabsorbed.
- Continued solute reabsorption without water reabsorption makes the tubular fluid even more dilute.
- The osmolarity of the tubular fluid can decrease to as low as 50 mOsm/L.
- Failure to reabsorb water contributes to urine dilution.
- Continued reabsorption of solutes also contributes to urine dilution.
- These processes result in the formation of a large volume of dilute urine.
- The mechanism for forming dilute urine is continued solute reabsorption in the distal nephron.
- The mechanism for forming dilute urine also involves reduced water reabsorption.
- In healthy kidneys, fluid leaving the ascending loop of Henle is always dilute.
- In healthy kidneys, fluid leaving the early distal tubule is always dilute.
- This dilution occurs regardless of the level of ADH.
- In the absence of ADH, further dilution occurs in the late distal tubule.
- In the absence of ADH, further dilution occurs in the collecting ducts.
- A large volume of dilute urine is ultimately excreted.
KEY CONCEPT
- Late distal tubules and collecting ducts continue to reabsorb sodium chloride.
- Without ADH, these segments remain impermeable to water.
- Solute reabsorption without water reabsorption further dilutes the tubular fluid.
- Tubular fluid osmolarity can fall to as low as 50 mOsm/L.
- The absence of ADH results in excretion of a large volume of dilute urine.
- Dilute urine formation depends on continued solute reabsorption with reduced water reabsorption.
RENAL MECHANISMS FOR EXCRETING DILUTE URINE (SUMMARY ESSAY)
Imagine a person drinks a large amount of water. The body now has excess water that must be removed to keep the composition of body fluids normal. The kidneys solve this problem by producing a large volume of very dilute urine.
Normal kidneys can excrete up to 20 liters of dilute urine per day, and the urine osmolarity can fall as low as 50 mOsm/L. This means the urine contains very little solute and a lot of water.
The kidneys achieve this by continuing to reabsorb important solutes such as sodium and chloride while preventing large amounts of water from being reabsorbed in the later parts of the nephron. As a result, water is removed from the body while most solutes are conserved.
Example
Suppose a person drinks 1 liter of water quickly.
Within about 45 minutes, urine output may increase to nearly six times the normal rate. The kidneys remove the extra water by producing a larger volume of urine. However, the amount of solute excreted changes very little. Instead, the urine simply becomes more dilute, and its osmolarity falls from about 600 mOsm/L to 100 mOsm/L.
This allows the body to eliminate excess water without losing large amounts of important electrolytes.
Why Must the Body Regulate Water So Carefully?
Body cells function properly only when they are surrounded by extracellular fluid that has a relatively constant concentration of electrolytes and other solutes.
If extracellular fluid becomes too concentrated, water leaves the cells and they shrink.
If extracellular fluid becomes too dilute, water enters the cells and they swell.
Therefore, the body must carefully regulate osmolarity, which is determined by:
Osmolarity = Amount of Solute ÷ Volume of Water
Because sodium chloride is the major extracellular solute, extracellular fluid osmolarity depends mainly on the relationship between sodium and water.
The amount of body water is controlled by:
- Water intake (thirst)
- Water excretion by the kidneys
Together, these mechanisms keep extracellular fluid volume and osmolarity within normal limits.
How Does the Kidney Make Dilute Urine?
When glomerular filtrate is first formed, its osmolarity is approximately 300 mOsm/L, which is almost the same as plasma.
As this filtrate travels through different parts of the nephron, its concentration changes.
1. Proximal Tubule: No Change in Osmolarity
In the proximal tubule, water and solutes are reabsorbed in almost equal proportions.
Because water follows the solutes, the concentration of the tubular fluid changes very little.
Therefore, the tubular fluid remains isosmotic with plasma, with an osmolarity of about 300 mOsm/L.
Example
If 100 units of water and solute enter the proximal tubule, both are reabsorbed proportionally. Therefore, the concentration remains essentially unchanged.
2. Descending Loop of Henle: Fluid Becomes Concentrated
The surrounding renal medulla is highly concentrated (hypertonic).
As tubular fluid descends into this region, water leaves the tubule by osmosis.
Because water leaves while solutes remain behind, the tubular fluid becomes progressively more concentrated.
The deeper the fluid moves into the medulla, the more concentrated it becomes.
Example
Think of boiling soup. When water evaporates but salt remains, the soup becomes more concentrated. The same principle occurs here.
3. Ascending Loop of Henle: Fluid Becomes Dilute
The ascending limb works in the opposite way.
Here, sodium, potassium, and chloride are actively reabsorbed from the tubular fluid.
However, this segment is impermeable to water.
Therefore, solutes leave the tubule but water cannot follow.
As a result, the tubular fluid becomes progressively more dilute.
By the time it reaches the early distal tubule, osmolarity has fallen to about 100 mOsm/L.
Example
Imagine removing salt from a glass of water without removing any water. The remaining fluid becomes less concentrated. This is exactly what happens in the ascending limb.
4. Distal Tubule and Collecting Ducts Without ADH
The fluid entering the distal tubule is already dilute.
In the absence of ADH (Antidiuretic Hormone), the late distal tubule and collecting ducts remain almost impermeable to water.
However, sodium chloride continues to be reabsorbed.
Therefore, more solutes leave the tubular fluid while water remains inside.
This makes the tubular fluid even more dilute.
Its osmolarity may fall to as low as 50 mOsm/L.
Because water is not reabsorbed, a large volume of dilute urine is produced and excreted.
Example
Imagine filtering salty water and continuously removing salt while leaving the water behind. The remaining fluid becomes increasingly dilute. This is what occurs when ADH is absent.
Overall Sequence of Dilute Urine Formation
Glomerulus
→ Filtrate = 300 mOsm/L
Proximal Tubule
→ Water and solutes reabsorbed equally
→ Still 300 mOsm/L
Descending Loop
→ Water leaves
→ Fluid becomes concentrated
Ascending Loop
→ Solutes leave
→ Water cannot leave
→ Fluid becomes dilute (100 mOsm/L)
Late Distal Tubule & Collecting Ducts (No ADH)
→ More solutes reabsorbed
→ Water remains
→ Fluid becomes very dilute (50 mOsm/L)
Final Result
→ Large volume of dilute urine
KEY CONCEPT
- The kidney removes excess water by producing dilute urine.
- Filtrate starts at 300 mOsm/L in the glomerulus.
- The proximal tubule keeps the fluid isosmotic because water and solutes are reabsorbed equally.
- The descending loop concentrates the fluid because water leaves.
- The ascending loop dilutes the fluid because solutes leave but water cannot follow.
- In the absence of ADH, the distal tubule and collecting ducts continue removing solutes without reabsorbing water.
- Urine osmolarity can fall to 50 mOsm/L.
- The final result is a large volume of very dilute urine, allowing the body to eliminate excess water while conserving important solutes.