


- In the previous sections, we learned the basic principles of how water and solutes move across the tubular membrane.
- With this basic understanding, we can now study the special features of different nephron segments.
- Each tubular segment has unique characteristics that help it perform specific functions.
- We will discuss only the most important tubular transport functions.
- The main focus will be on the reabsorption of sodium, chloride, and water.
- In later chapters, we will discuss the reabsorption and secretion of other substances in different parts of the tubular system.
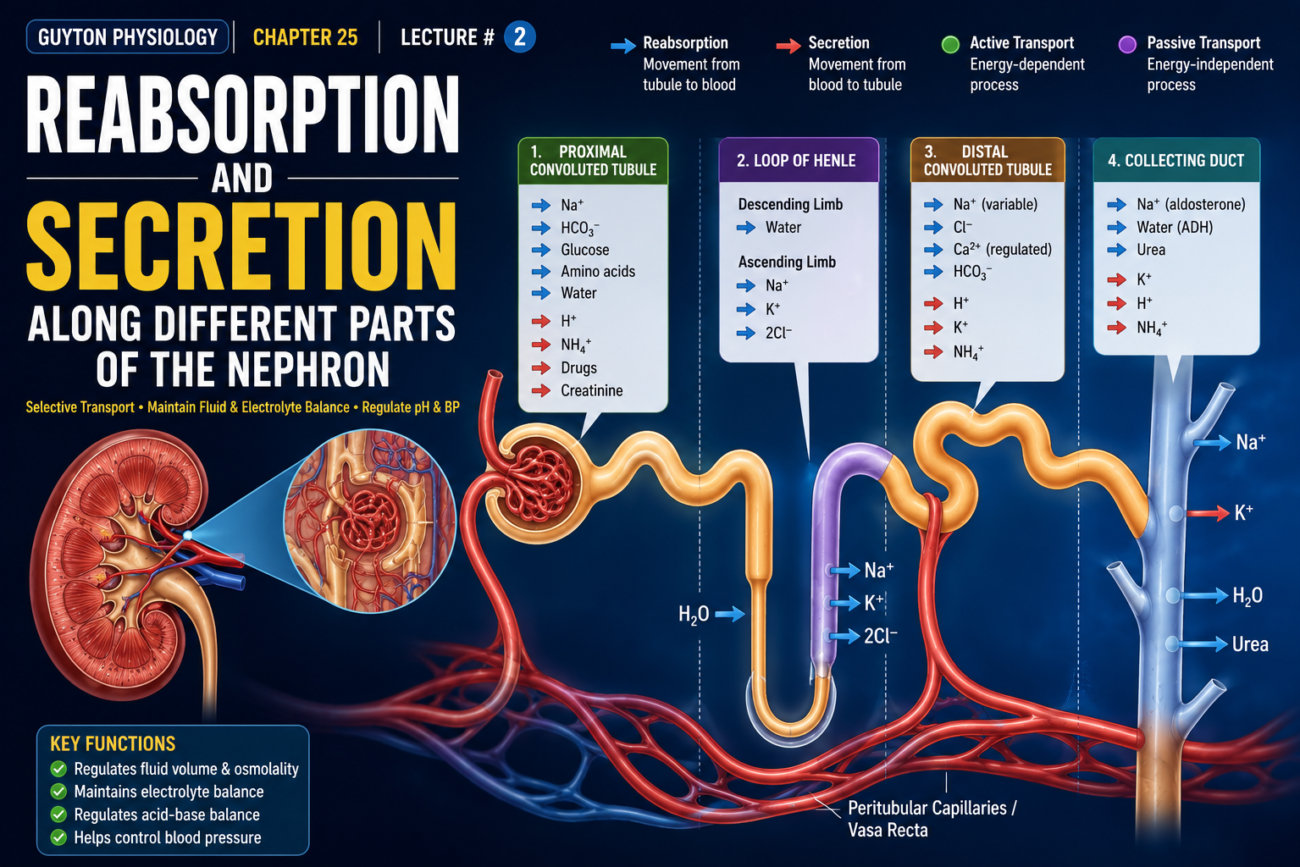
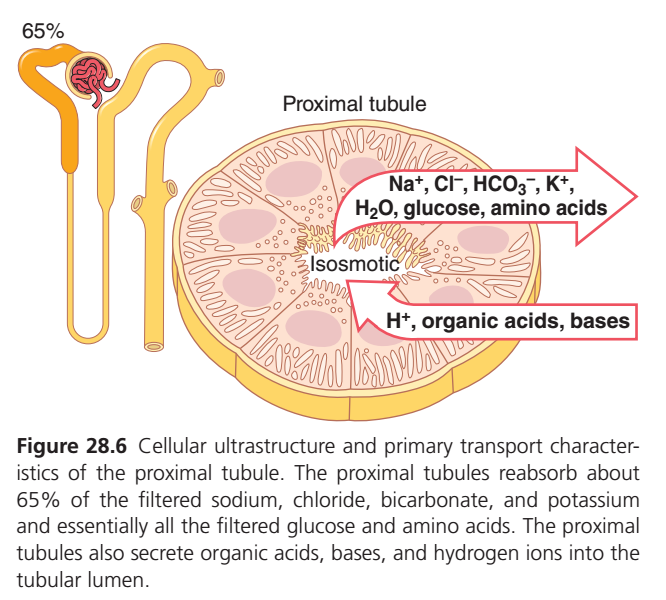
PROXIMAL TUBULAR REABSORPTION
- Normally, about 65% of the filtered sodium and water are reabsorbed by the proximal tubules before the filtrate reaches the loops of Henle.
- A slightly lower percentage of filtered chloride is also reabsorbed in the proximal tubules.
- These percentages can increase or decrease under different physiological conditions.
- The proximal tubule has a high capacity for both active and passive reabsorption.
- This high reabsorptive capacity is due to the special cellular features of the proximal tubule.
- Proximal tubular epithelial cells are highly metabolically active.
- These cells contain many mitochondria to support powerful active transport processes.
- The proximal tubular cells have an extensive brush border on the luminal (apical) side of the membrane.
- They also have extensive intercellular and basal channels.
- Together, these features provide a very large membrane surface area.
- This large surface area allows rapid transport of sodium ions and other substances.
- The brush border membrane contains many protein carrier molecules.
- These carrier proteins transport a large amount of sodium across the luminal membrane.
- Sodium is co-transported with organic nutrients such as glucose and amino acids.
- Additional sodium enters the cell through counter-transport mechanisms.
- These mechanisms reabsorb sodium while secreting other substances into the tubular lumen.
- Hydrogen ions are the main substances secreted by this process.
- Secretion of hydrogen ions into the tubular lumen is important for bicarbonate removal.
- Hydrogen ions combine with bicarbonate to form carbonic acid.
- Carbonic acid then breaks down into water and carbon dioxide.
- The Na⁺-K⁺ ATPase pump provides the main force for reabsorption of sodium, chloride, and water in the proximal tubule.
- The mechanisms of sodium and chloride transport differ between the early and late parts of the proximal tubule.
- In the first half of the proximal tubule, sodium is reabsorbed together with glucose, amino acids, and other solutes.
- In the second half of the proximal tubule, little glucose and few amino acids remain to be reabsorbed.
- Therefore, sodium is mainly reabsorbed with chloride ions in the second half of the proximal tubule.
- The chloride concentration is higher in the second half of the proximal tubule than in the first half.
- In the early proximal tubule, sodium is reabsorbed mainly with glucose, bicarbonate, and organic ions.
- This leaves behind tubular fluid with a higher chloride concentration.
- The higher chloride concentration promotes chloride diffusion from the tubular lumen into the renal interstitial fluid.
- Chloride diffuses through the intercellular junctions.
- Passive chloride reabsorption also occurs through solvent drag.
- Small amounts of chloride are reabsorbed through specific chloride channels in the proximal tubular cell membrane.
- The concentrations of different solutes change along the proximal tubule.
- The amount of sodium in the tubular fluid decreases markedly along the proximal tubule.
- However, sodium concentration remains relatively constant.
- Total osmolarity also remains relatively constant.
- Water reabsorption keeps pace with sodium reabsorption because the proximal tubule is highly permeable to water.
- Glucose, amino acids, and bicarbonate are reabsorbed more rapidly than water.
- Therefore, their concentrations decrease markedly along the proximal tubule.
- Solutes that are less permeable and not actively reabsorbed, such as creatinine, become more concentrated along the proximal tubule.
- Total solute concentration remains almost unchanged throughout the proximal tubule.
- This occurs because the proximal tubule has a high permeability to water.
- The proximal tubule is also an important site for secretion of organic acids and bases.
- Examples include bile salts, oxalate, urate, and catecholamines.
- Many of these substances are end products of metabolism.
- These substances must be removed rapidly from the body.
- Secretion into the proximal tubule, filtration by the glomerulus, and minimal tubular reabsorption together promote rapid urinary excretion.
- The kidneys also secrete many potentially harmful drugs and toxins into the tubules.
- This process rapidly clears these substances from the blood.
- Some drugs, such as penicillin and salicylates, are cleared very rapidly by the kidneys.
- Rapid clearance can make it difficult to maintain an effective therapeutic drug concentration.
- Para-aminohippuric acid (PAH) is another substance that is rapidly secreted by the proximal tubule.
- PAH is secreted so rapidly that about 90% of it is removed from plasma during passage through the kidneys.
- PAH is then excreted in the urine.
- Therefore, PAH clearance can be used to estimate renal plasma flow (RPF).
KEY CONCEPT
- Proximal tubules reabsorb about 65% of filtered sodium and water.
- Large surface area and many mitochondria support rapid reabsorption.
- Sodium is reabsorbed with glucose and amino acids early, and mainly with chloride later.
- Water reabsorption closely follows sodium reabsorption.
- The proximal tubule also secretes hydrogen ions, organic acids, bases, drugs, and toxins.
- PAH clearance is used to estimate renal plasma flow (RPF).
PROXIMAL TUBULE (PCT) — THE KIDNEY’S “BULK REABSORPTION FACTORY”
Main Idea
After blood is filtered in the glomerulus, a large amount of useful substances enters the nephron.
The proximal tubule immediately takes back most of these valuable substances so they are not lost in urine.
What Does the Proximal Tubule Reabsorb?
About 65% of the filtered load is reabsorbed here.
It takes back:
✅ Sodium (Na⁺)
✅ Chloride (Cl⁻)
✅ Bicarbonate (HCO₃⁻)
✅ Potassium (K⁺)
✅ Water (H₂O)
✅ Almost all glucose
✅ Almost all amino acids
What Does the Proximal Tubule Secrete?
The proximal tubule also moves some substances from blood into the tubule for removal.
It secretes:
➡️ Hydrogen ions (H⁺)
➡️ Organic acids
➡️ Organic bases
These substances will eventually leave the body in urine.
Why is “Isosmotic” Written in the Figure?
Easy Concept
The proximal tubule removes:
- Water
- Sodium
in almost equal proportions.
Therefore:
✔ Water follows sodium.
✔ Fluid concentration does not change much.
✔ Osmolarity remains nearly the same.
This process is called:
ISOSMOTIC REABSORPTION
Meaning:
Water and solutes are reabsorbed together, so the tubular fluid remains nearly the same concentration.
Simple Story
Imagine a Shopping Bag
After filtration, the nephron bag contains:
🧂 Salt
💧 Water
🍬 Glucose
🥩 Amino acids
⚡ Potassium
The proximal tubule acts like a careful worker:
✔ Takes back most useful items
✔ Returns them to the blood
✔ Throws unwanted acids and H⁺ into the urine
KEY CONCEPT
- Proximal tubule is the major reabsorptive segment of the nephron.
- It reabsorbs about 65% of filtered Na⁺, Cl⁻, HCO₃⁻, K⁺, and water.
- It reabsorbs almost all glucose and amino acids.
- It secretes H⁺, organic acids, and organic bases.
- Reabsorption is isosmotic, meaning water follows solutes and osmolarity stays nearly unchanged.
- Think of the proximal tubule as the kidney’s “recycling and recovery center.”
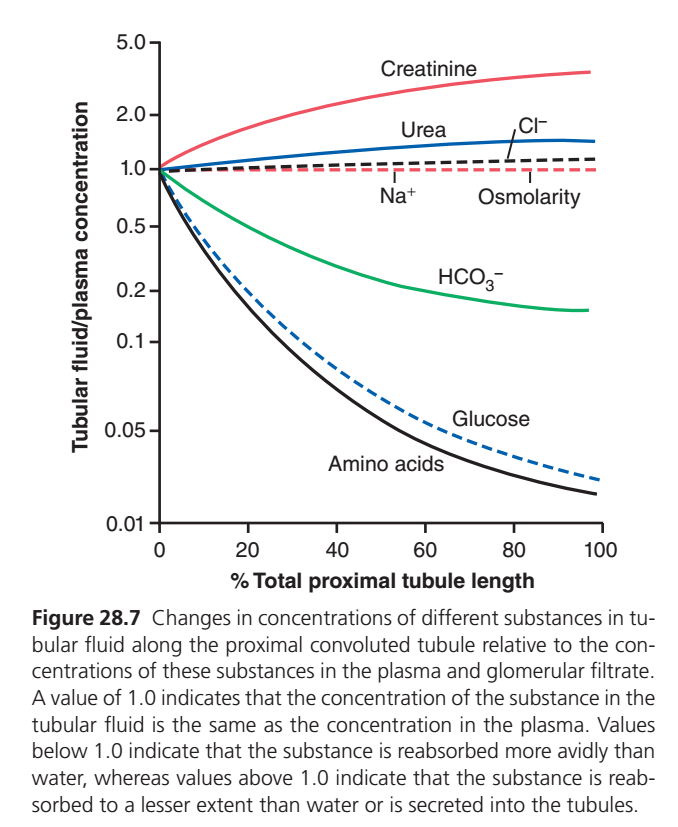
FIGURE 28.7 — WHAT HAPPENS TO DIFFERENT SUBSTANCES AS FLUID MOVES THROUGH THE PROXIMAL TUBULE?
This graph is one of the most important proximal tubule graphs in Guyton.
The secret to understanding it is:
What is on the Y-axis?
Tubular Fluid / Plasma Concentration Ratio (TF/P)TF/P=Concentration in plasmaConcentration in tubular fluid
Meaning of TF/P Values
TF/P = 1
Substance concentration in tubular fluid = concentration in plasma
➡ No relative change
TF/P < 1
Concentration falls in tubular fluid
➡ Substance is being reabsorbed faster than water
TF/P > 1
Concentration rises in tubular fluid
➡ Substance is reabsorbed slower than water
OR
➡ Substance is secreted into tubule
FIRST UNDERSTAND THE REFERENCE LINES
🔴 Red Horizontal Dotted Line (TF/P = 1)
This is the most important reference line.
It means:
“No relative change compared with plasma”
If a substance stays on this line:
- Water and that substance are removed equally.
- Concentration does not change.
Think:
Water and solute are running at the same speed.
⚫ Black Horizontal Dotted Line (Osmolarity)
Notice it stays very close to 1.
This tells us:
The proximal tubule performs ISOSMOTIC REABSORPTION.
Water follows sodium almost perfectly.
Therefore:
- Water leaves
- Solutes leave
at nearly the same rate.
So osmolarity hardly changes.
NOW EACH CURVE
1. Na⁺ LINE
(Almost on the red dotted line)
What happens?
About 65% of filtered sodium is reabsorbed.
BUT
About 65% of water is also reabsorbed.
Therefore sodium concentration remains almost unchanged.
Why?
Whenever sodium leaves:
💧 Water follows.
Thus concentration stays almost the same.
Easy Memory
Sodium and water are best friends.
They move together.
Therefore:
TF/P ≈ 1
2. Cl⁻ LINE (Blue Line Rising Slightly)
Notice chloride slowly rises above 1.
Why does chloride concentration increase?
Early proximal tubule:
Na⁺ and water are reabsorbed rapidly.
Bicarbonate is removed rapidly.
Chloride initially remains behind.
Therefore chloride becomes slightly concentrated.ater
The accumulated chloride is then reabsorbed.
So the rise is only mild.
Easy Memory
Chloride is a “late passenger.”
It stays behind initially.
Concentration rises slightly.
3. UREA LINE
(Rises above 1)
What happens?
Water is reabsorbed faster than urea.
As water leaves:
Remaining urea becomes concentrated.
Example
Start:
100 mL water + 100 urea
Half water removed
50 mL water + 100 urea
Concentration doubles.
Easy Memory
Urea is left behind while water escapes.
Therefore concentration increases.
4. CREATININE LINE
(Rises highest of all)
Why?
Creatinine is:
✔ Filtered
✔ Almost not reabsorbed
Some may even be secreted.
Meanwhile huge amounts of water are removed.esult
Creatinine becomes more and more concentrated.
Therefore TF/P rises dramatically.
Easy Memory
Water leaves.
Creatinine stays.
Concentration shoots upward.
5. HCO₃⁻ (BICARBONATE) LINE
(Green line falling)
What happens?
Bicarbonate is reabsorbed very efficiently.
Much faster than water.
Result
Tubular concentration rapidly decreases.
Therefore TF/P falls below 1.
Easy Memory
Kidney wants to save bicarbonate.
So bicarbonate disappears from tubule quickly.
6. GLUCOSE LINE
(Blue dashed line falling sharply)
What happens?
Glucose is reabsorbed almost completely.
Very early in proximal tubule.Result
Very little glucose remains in tubular fluid.
Concentration approaches zero.
Easy Memory
Normal urine should contain almost no glucose.
Kidney grabs glucose immediately.
7. AMINO ACID LINE
(Black line falling most steeply)
What happens?
Amino acids are reabsorbed even more completely and rapidly.
Result
Their concentration becomes almost zero.
The curve drops fastest.
Easy Memory
Kidney hates wasting amino acids.
They are taken back almost immediately.
WHY SOME LINES GO UP AND OTHERS GO DOWN?
Lines Going UP (>1)
Water is removed faster than the substance
Examples:
- Creatinine
- Urea
- Chloride (slightly)
Think:
Water leaves → substance left behind → concentration rises.
Lines Going DOWN (<1)
Substance is removed faster than water
Examples:
- Glucose
- Amino acids
- Bicarbonate
Think:
Substance disappears from tubule faster than water.
THE ENTIRE GRAPH IN ONE SENTENCE
As filtrate moves through the proximal tubule, water and sodium are reabsorbed together (isosmotic reabsorption), glucose and amino acids are reabsorbed almost completely, bicarbonate is strongly reabsorbed, chloride and urea become slightly concentrated because water leaves faster than they do, and creatinine becomes highly concentrated because it is hardly reabsorbed at all.
KEY CONCEPT
- Red dotted line (TF/P = 1): no relative concentration change.
- Black dotted line (Osmolarity): shows isosmotic reabsorption.
- Na⁺: stays near 1 because water follows sodium.
- Cl⁻: rises slightly because it lags behind early.
- Urea: rises because water leaves faster.
- Creatinine: rises most because it is not reabsorbed.
- HCO₃⁻: falls because it is strongly reabsorbed.
- Glucose: falls sharply because almost all is reabsorbed.
- Amino acids: fall most rapidly because they are reabsorbed almost completely very early.
SOLUTE AND WATER TRANSPORT IN LOOPS OF HENLE
- The loop of Henle has three functionally different segments: the thin descending segment, thin ascending segment, and thick ascending segment.
- The thin descending and thin ascending segments have thin epithelial membranes.
- These segments do not have brush borders.
- These segments contain few mitochondria.
- These segments have very low metabolic activity.
- About 20% of the filtered water is reabsorbed in the loop of Henle.
- Almost all of this water reabsorption occurs in the thin descending limb.
- The thin descending limb is highly permeable to water.
- Water is reabsorbed passively through AQP-1 water channels.
- The ascending limb, including both thin and thick portions, is almost impermeable to water.
- This property is important for concentrating urine.
- The thick ascending segment begins about halfway up the ascending limb.
- The thick ascending segment contains thick epithelial cells.
- These cells have high metabolic activity.
- These cells can actively reabsorb sodium, chloride, and potassium.
- About 25% of the filtered sodium, chloride, and potassium are reabsorbed in the loop of Henle.
- Most of this reabsorption occurs in the thick ascending limb.
- Significant amounts of calcium, bicarbonate, and magnesium are also reabsorbed in the thick ascending limb.
- The thin ascending limb has a much lower reabsorptive capacity than the thick ascending limb.
- The thin descending limb does not reabsorb significant amounts of these solutes.
- An important part of solute reabsorption in the thick ascending limb is the Na⁺-K⁺ ATPase pump.
- This pump is located in the basolateral membrane of epithelial cells.
- Reabsorption of many other solutes depends on the activity of the Na⁺-K⁺ ATPase pump.
- The pump keeps intracellular sodium concentration low.
- The low intracellular sodium concentration creates a favorable gradient for sodium entry from the tubular fluid into the cell.
- In the thick ascending limb, sodium movement across the luminal membrane occurs mainly through the NKCC2 co-transporter.
- The NKCC2 transporter carries 1 sodium, 2 chloride, and 1 potassium ion together.
- This transporter uses the energy from sodium movement into the cell.
- This energy drives potassium reabsorption against its concentration gradient.
- The thick ascending limb is the site of action of loop diuretics.
- Furosemide, ethacrynic acid, and bumetanide act on this segment.
- These drugs inhibit the NKCC2 co-transporter.
- The thick ascending limb also contains a sodium-hydrogen counter-transporter in the luminal membrane.
- This transporter reabsorbs sodium and secretes hydrogen ions.
- Significant paracellular reabsorption of cations also occurs in the thick ascending limb.
- These cations include magnesium, calcium, sodium, and potassium.
- This reabsorption occurs because the tubular lumen has a slight positive charge compared with the interstitial fluid.
- The NKCC2 co-transporter moves equal amounts of cations and anions into the cell.
- Some potassium leaks back into the tubular lumen through potassium channels.
- This potassium backleak creates a positive charge of about +8 millivolts in the tubular lumen.
- The positive luminal charge drives cations such as magnesium and calcium through the paracellular pathway into the interstitial fluid.
- The thick ascending limb is almost impermeable to water.
- Therefore, most of the water entering this segment remains inside the tubule.
- Large amounts of solutes are reabsorbed despite little water reabsorption.
- As fluid moves through the ascending limb, it becomes increasingly dilute.
- The dilute fluid then flows toward the distal tubule.
- This feature helps the kidneys dilute or concentrate urine under different conditions.
KEY CONCEPT
- The loop of Henle has thin descending, thin ascending, and thick ascending segments.
- Water is mainly reabsorbed in the thin descending limb.
- The ascending limb is nearly impermeable to water.
- The thick ascending limb actively reabsorbs sodium, chloride, and potassium.
- NKCC2 is the main transporter in the thick ascending limb.
- Loop diuretics block NKCC2.
- The thick ascending limb dilutes tubular fluid and helps regulate urine concentration.
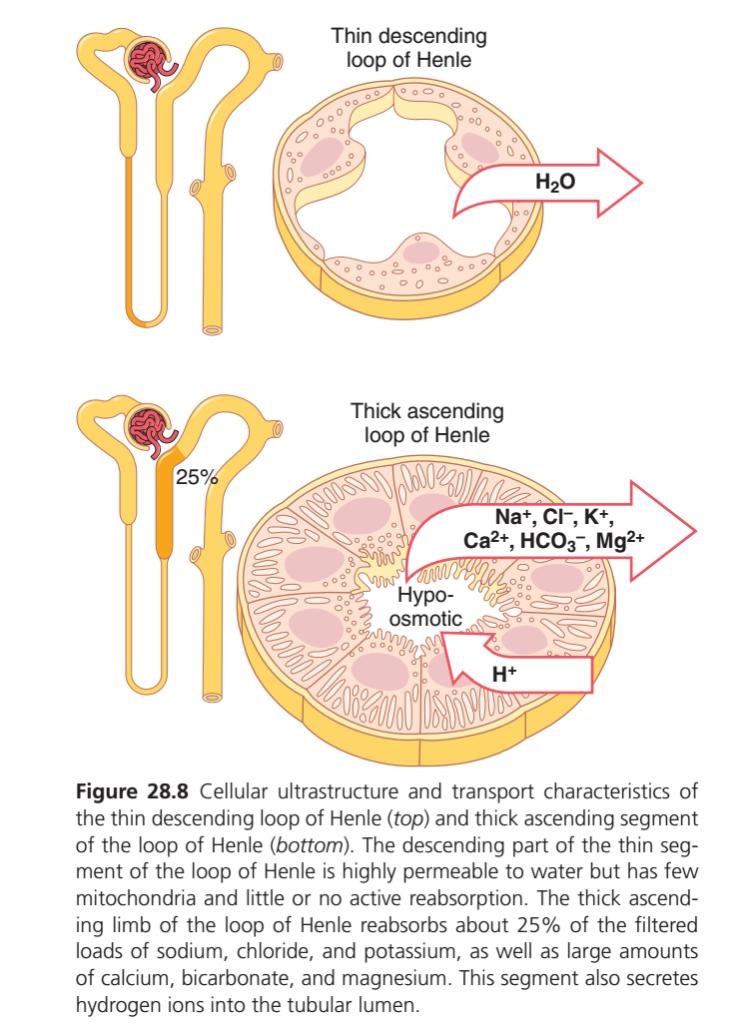
LOOP OF HENLE — THE KIDNEY’S “CONCENTRATING SYSTEM”
This figure shows the two very different parts of the Loop of Henle:
- Thin Descending Limb
- Thick Ascending Limb
The easiest way to remember them is:
Descending Limb
💧 Water leaves
Ascending Limb
🧂 Salt leaves
PART 1: THIN DESCENDING LIMB
What Happens Here?
The wall is:
✅ Highly permeable to water
❌ Almost impermeable to salts
❌ Very little active transport
Main Event
Water moves out of the tubule into the kidney medulla.
H₂O → OUT
Why Does Water Leave?
The surrounding kidney medulla is very concentrated (hyperosmotic).
Water always moves:
From dilute area → concentrated area
Therefore water leaves the tubule.
What Happens to Tubular Fluid?
As water leaves:
- Less water remains
- Solutes remain behind
Therefore tubular fluid becomes:
MORE CONCENTRATED
HYPEROSMOTIC
Easy Story
Imagine a bucket containing:
🧂 Salt
💧 Water
If you remove only water:
The remaining fluid becomes very salty.
This is exactly what happens in the descending limb.
THIN DESCENDING LIMB IN ONE SENTENCE
“Water leaves, solutes stay, tubular fluid becomes concentrated.”
PART 2: THICK ASCENDING LIMB
This part does the exact opposite.
What Leaves Here?
Reabsorbed into Blood
✅ Na⁺
✅ Cl⁻
✅ K⁺
✅ Ca²⁺
✅ Mg²⁺
✅ HCO₃⁻
About 25% of filtered sodium is reabsorbed here.
This is why the figure shows:
25%
What Is Secreted?
H⁺
Hydrogen ions move into the tubular lumen.
MOST IMPORTANT FEATURE
Is Water Reabsorbed Here?
NO
The thick ascending limb is:
❌ Nearly impermeable to water
What Happens Then?
Salts leave
BUT
Water cannot follow
Result
Tubular fluid becomes:
MORE DILUTE
HYPO-OSMOTIC
This is why the center of the figure says:
HYPO-OSMOTIC
Why Is It Called the “Diluting Segment”?
Because:
🧂 Salt leaves
💧 Water stays
Therefore the remaining fluid becomes dilute.
Easy Story
Imagine a bucket containing:
🧂 Salt
💧 Water
Now remove only salt.
The remaining fluid becomes less salty.
Exactly what happens in the thick ascending limb.
COMPARISON OF BOTH LIMBS
| Feature | Thin Descending Limb | Thick Ascending Limb |
|---|---|---|
| Water permeability | Very high | Very low |
| Salt transport | Minimal | Very high |
| Water movement | Out | No significant movement |
| NaCl movement | Little | Out |
| Tubular fluid becomes | Concentrated | Dilute |
| Osmolarity | Hyperosmotic | Hypo-osmotic |
| Nickname | Water-losing segment | Diluting segment |
THE BIG CONCEPT
The two limbs work together:
Descending Limb
💧 Water leaves
⬆ Osmolarity increases
⬆ Fluid becomes concentrated
Ascending Limb
🧂 Salt leaves
⬇ Osmolarity decreases
⬇ Fluid becomes dilute
SUPER EASY MEMORY TRICK
DESCENDING = WATER DOWN
Think:
D = Descending = Drinks out water
💧 Water leaves
ASCENDING = SALT AWAY
Think:
A = Ascending = Active salt transport
🧂 Salt leaves
KEY CONCEPT
- Thin descending limb: highly permeable to water, very little active transport.
- Water leaves the tubule, making tubular fluid more concentrated (hyperosmotic).
- Thick ascending limb: actively reabsorbs Na⁺, Cl⁻, K⁺, Ca²⁺, Mg²⁺, and HCO₃⁻.
- About 25% of filtered sodium is reabsorbed here.
- H⁺ is secreted into the lumen.
- Water cannot follow the reabsorbed salts.
- Therefore tubular fluid becomes dilute (hypo-osmotic).
- Descending limb = water out.
- Ascending limb = salt out.
- Together they create the kidney’s powerful urine-concentrating mechanism.
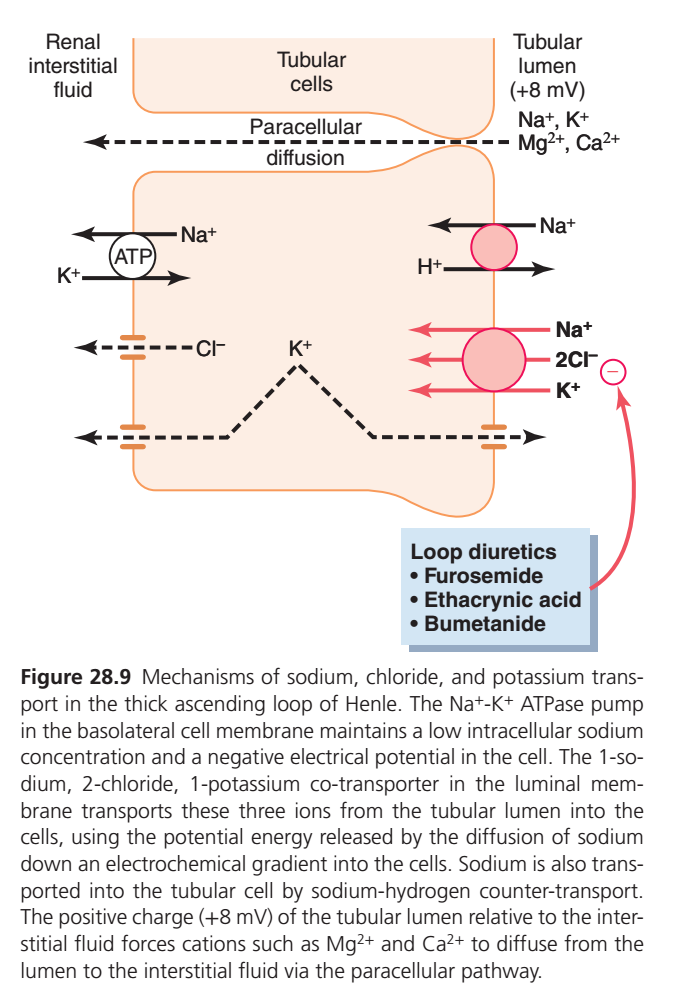
Mechanism of Solute Transport in the Thick Ascending Limb of the Loop of Henle
The thick ascending limb of the Loop of Henle is a specialized segment of the nephron that plays a crucial role in the reabsorption of sodium, chloride, potassium, calcium, and magnesium. Because this segment reabsorbs large amounts of solutes while allowing very little water to pass, it is commonly known as the diluting segment of the nephron. The transport processes occurring here help regulate body fluid composition and contribute to the kidney’s ability to produce concentrated urine.
The process begins with the Na⁺-K⁺ ATPase pump located on the basolateral membrane of the tubular cell. This pump uses energy from ATP to transport sodium out of the cell into the renal interstitial fluid while moving potassium into the cell. By continuously removing sodium from the cell, the pump keeps intracellular sodium concentration low. This creates a strong gradient that favors the movement of sodium from the tubular lumen into the tubular cell.
On the luminal membrane, sodium enters the cell through the Na⁺-K⁺-2Cl⁻ cotransporter (NKCC2). This transporter simultaneously carries one sodium ion, one potassium ion, and two chloride ions from the tubular lumen into the cell. The energy for this transport is provided indirectly by the sodium gradient established by the Na⁺-K⁺ ATPase pump. As a result, large quantities of sodium, chloride, and potassium are reabsorbed from the tubular fluid.
After entering the cell, sodium is actively pumped into the interstitial fluid by the Na⁺-K⁺ ATPase pump, while chloride diffuses out of the cell through chloride channels into the interstitial fluid. Potassium, however, behaves differently. Much of the potassium that enters the cell through the NKCC2 transporter leaks back into the tubular lumen through potassium channels. This process is known as potassium recycling.
Potassium recycling has an important consequence. As positively charged potassium ions move back into the lumen, they create a positive electrical potential of approximately +8 mV within the tubular lumen. This positive luminal voltage becomes a driving force for the movement of other positively charged ions.
Because the lumen is positively charged, cations such as calcium (Ca²⁺) and magnesium (Mg²⁺) are pushed through the spaces between adjacent tubular cells into the interstitial fluid. This movement occurs through the paracellular pathway, meaning the ions pass between cells rather than through them. Thus, the positive luminal potential promotes the passive reabsorption of calcium and magnesium.
Another transport mechanism present in this segment is the Na⁺-H⁺ exchanger, which allows sodium to enter the tubular cell while hydrogen ions are secreted into the tubular lumen. This process contributes both to sodium reabsorption and to the regulation of acid-base balance.
A unique feature of the thick ascending limb is that it is almost impermeable to water. Therefore, although large amounts of sodium, chloride, potassium, calcium, magnesium, and bicarbonate are reabsorbed, water cannot follow these solutes. Consequently, the tubular fluid becomes progressively more dilute as it moves upward through the loop. This is why the thick ascending limb is called the diluting segment.
The clinical importance of this segment is highlighted by the action of loop diuretics, including furosemide, bumetanide, and ethacrynic acid. These drugs block the NKCC2 cotransporter, preventing the reabsorption of sodium, potassium, and chloride. As a result, more salt remains in the tubular fluid, water follows the retained solutes, and large volumes of urine are produced. For this reason, loop diuretics are among the most powerful diuretic drugs used in clinical medicine.
KEY CONCEPT
The thick ascending limb functions as the kidney’s major salt-reabsorbing segment. The Na⁺-K⁺ ATPase pump drives sodium transport, the NKCC2 cotransporter reabsorbs sodium, potassium, and chloride, and potassium recycling creates a positive luminal voltage that promotes calcium and magnesium reabsorption. Because water cannot follow these solutes, the tubular fluid becomes dilute, making this segment the diluting segment of the nephron.
EARLY DISTAL TUBULE
- The next part of the distal tubule is highly convoluted.
- This segment has many reabsorptive properties similar to the thick ascending limb of the loop of Henle.
- It actively reabsorbs most ions, including sodium, potassium, and chloride.
- It is almost impermeable to water.
- It is also almost impermeable to urea.
- Because water cannot follow the reabsorbed solutes, this segment dilutes the tubular fluid.
- Therefore, it is called the diluting segment.
- Approximately 5% of the filtered sodium chloride is reabsorbed in the early distal tubule.
- Sodium and chloride enter the tubular cell through the sodium-chloride co-transporter.
- The Na⁺-K⁺ ATPase pump transports sodium out of the cell across the basolateral membrane.
- Chloride leaves the cell through chloride channels in the basolateral membrane.
- Thiazide diuretics inhibit the sodium-chloride co-transporter.
- These drugs are commonly used to treat hypertension and heart failure.
KEY CONCEPT
- The early distal tubule resembles the thick ascending limb in function.
- It reabsorbs sodium, potassium, and chloride.
- It is almost impermeable to water and urea.
- About 5% of filtered sodium chloride is reabsorbed here.
- Sodium-chloride co-transporters mediate sodium and chloride reabsorption.
- Thiazide diuretics block the sodium-chloride co-transporter.
- This segment dilutes tubular fluid and is called the diluting segment.
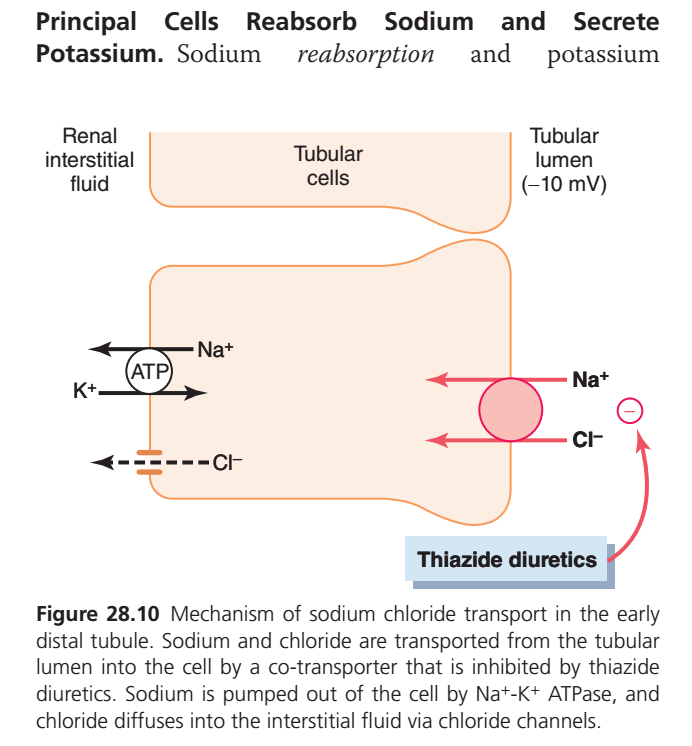
Sodium Chloride Reabsorption in the Early Distal Tubule
The early distal convoluted tubule (DCT) is an important segment of the nephron that continues the process of salt reabsorption after the filtrate leaves the Loop of Henle. Its primary function is to reabsorb sodium (Na⁺) and chloride (Cl⁻) from the tubular fluid while remaining relatively impermeable to water. Because solutes are removed without significant water reabsorption, this segment also contributes to the dilution of tubular fluid.
The transport process begins on the luminal side of the tubular cell, where sodium and chloride enter together through a sodium-chloride cotransporter (NCC). This transporter moves one sodium ion and one chloride ion from the tubular lumen into the cell. The movement of these ions is driven by the low intracellular sodium concentration that is maintained by the Na⁺-K⁺ ATPase pump.
On the basolateral membrane, the Na⁺-K⁺ ATPase pump uses ATP to actively transport sodium out of the cell into the renal interstitial fluid while bringing potassium into the cell. This pump keeps intracellular sodium levels low and serves as the major driving force for sodium reabsorption throughout the nephron.
After entering the tubular cell through the sodium-chloride cotransporter, chloride ions leave the cell through chloride channels located on the basolateral membrane and diffuse into the interstitial fluid. Thus, both sodium and chloride are ultimately reabsorbed into the blood.
As sodium is removed from the tubular lumen, the lumen becomes slightly negatively charged (about −10 mV) relative to the interstitial fluid. This electrical gradient influences the movement of other ions in the distal nephron and contributes to later potassium and hydrogen ion secretion in downstream segments.
A clinically important feature of the early distal tubule is the presence of the sodium-chloride cotransporter (NCC), which is the target of thiazide diuretics. Drugs such as hydrochlorothiazide, chlorthalidone, and indapamide block this transporter, preventing sodium and chloride reabsorption. As a result, more sodium remains in the tubular fluid, water follows osmotically, and urine output increases. This is why thiazide diuretics are commonly used in the treatment of hypertension and mild edema.
Another important characteristic of the early distal tubule is its low permeability to water. Therefore, sodium and chloride are reabsorbed without significant water reabsorption. As solutes leave while water remains in the tubular fluid, the tubular fluid becomes progressively more dilute. For this reason, the early distal tubule, like the thick ascending limb of the Loop of Henle, is considered part of the nephron’s diluting segment.
Key Concept
The early distal tubule primarily reabsorbs sodium and chloride through the Na⁺-Cl⁻ cotransporter (NCC). The Na⁺-K⁺ ATPase pump provides the energy that drives this process by maintaining a low intracellular sodium concentration. Chloride diffuses into the interstitial fluid through chloride channels, and because water does not follow these solutes, the tubular fluid becomes more dilute. Thiazide diuretics block the NCC transporter, reducing sodium reabsorption and increasing urine formation. Thus, the early distal tubule serves as an important salt-reabsorbing and diluting segment of the nephron.
LATE DISTAL TUBULES AND CORTICAL COLLECTING TUBULES
- The second half of the distal tubule and the cortical collecting tubule have similar functional characteristics.
- These segments contain two main types of cells: principal cells and intercalated cells.
- Principal cells reabsorb sodium from the tubular lumen.
- Principal cells also reabsorb water from the tubular lumen.
- Principal cells secrete potassium ions into the tubular lumen.
- There are two types of intercalated cells.
- Type A intercalated cells reabsorb potassium ions.
- Type A intercalated cells also reabsorb bicarbonate ions.
- Type A intercalated cells secrete hydrogen ions into the tubular lumen.
- Type B intercalated cells have the opposite effects.
- Sodium reabsorption by principal cells depends on the Na⁺-K⁺ ATPase pump in the basolateral membrane.
- Potassium secretion by principal cells also depends on the Na⁺-K⁺ ATPase pump.
- This pump keeps the intracellular sodium concentration low.
- The low intracellular sodium concentration promotes sodium diffusion into the cell through sodium channels.
- Potassium secretion occurs in two steps.
- First, potassium enters the cell through the action of the Na⁺-K⁺ ATPase pump.
- This pump maintains a high intracellular potassium concentration.
- Second, potassium diffuses out of the cell through potassium channels in the luminal membrane.
- Potassium then enters the tubular fluid down its concentration gradient.
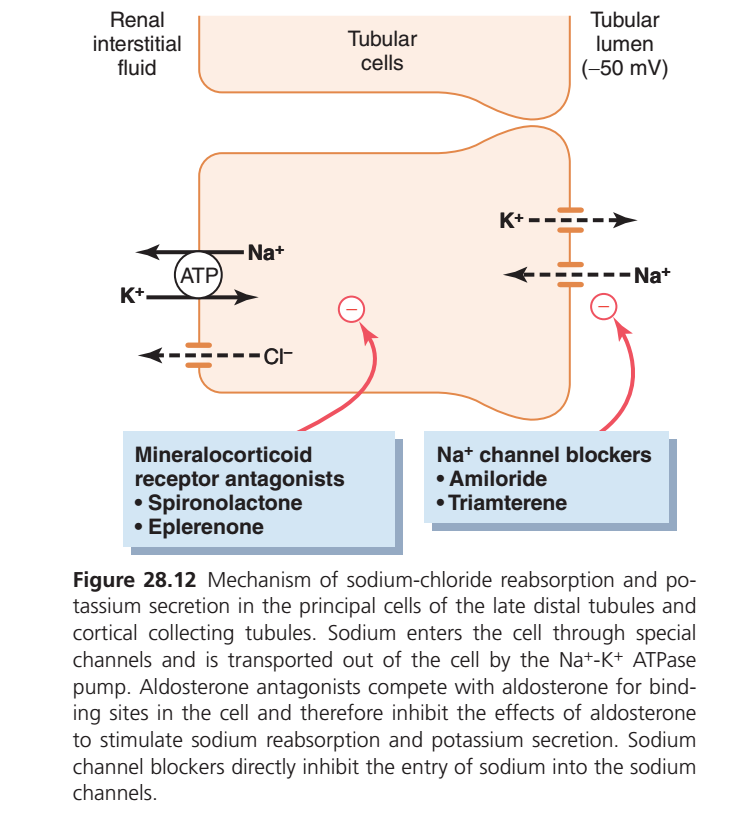
- Principal cells are the main sites of action of potassium-sparing diuretics.
- Potassium-sparing diuretics include spironolactone, eplerenone, amiloride, and triamterene.
- Spironolactone and eplerenone are mineralocorticoid receptor antagonists.
- These drugs compete with aldosterone for receptor sites in principal cells.
- Therefore, they inhibit the effects of aldosterone on sodium reabsorption.
- They also inhibit the effects of aldosterone on potassium secretion.
- Amiloride and triamterene are sodium channel blockers.
- These drugs directly block sodium entry through luminal sodium channels.
- As a result, less sodium enters the principal cells.
- This reduces the amount of sodium transported by the Na⁺-K⁺ ATPase pump.
- Reduced sodium transport decreases potassium transport into the cells.
- This ultimately decreases potassium secretion into the tubular fluid.
- Sodium channel blockers decrease urinary potassium excretion.
- Aldosterone antagonists also decrease urinary potassium excretion.
- Therefore, both groups of drugs act as potassium-sparing diuretics.
KEY CONCEPT
- Late distal tubules and cortical collecting tubules contain principal cells and intercalated cells.
- Principal cells reabsorb sodium and water and secrete potassium.
- Type A intercalated cells reabsorb potassium and bicarbonate and secrete hydrogen ions.
- Type B intercalated cells have opposite functions.
- Na⁺-K⁺ ATPase drives sodium reabsorption and potassium secretion.
- Spironolactone and eplerenone block aldosterone action.
- Amiloride and triamterene block sodium channels.
- These drugs reduce potassium loss and act as potassium-sparing diuretics.
Transport Functions of the Distal Tubule and Collecting Tubule
The distal tubule and collecting tubule represent the final segments of the nephron where the kidney makes its last adjustments to the composition of urine. These segments play a critical role in regulating sodium, potassium, hydrogen ions, bicarbonate, calcium, magnesium, and water. Unlike earlier nephron segments that perform bulk reabsorption, the distal tubule and collecting tubule provide fine control over electrolyte balance, acid-base balance, and body water content.
The early distal tubule functions similarly to the thick ascending limb of the Loop of Henle. It reabsorbs sodium (Na⁺), chloride (Cl⁻), calcium (Ca²⁺), and magnesium (Mg²⁺) from the tubular fluid into the blood. However, this segment is almost impermeable to water and urea. As solutes are reabsorbed without accompanying water movement, the tubular fluid becomes progressively more dilute. Therefore, the early distal tubule is considered part of the kidney’s diluting segment.
The late distal tubule and cortical collecting tubule contain two important cell types: principal cells and intercalated cells. Each cell type performs a specific function in maintaining the body’s internal environment.
Principal Cells
Principal cells are mainly responsible for regulating sodium, potassium, and water balance. These cells reabsorb sodium and chloride from the tubular lumen into the blood. At the same time, they secrete potassium (K⁺) into the tubular fluid. This process helps maintain normal potassium levels in the body.
Principal cells are also the primary site where antidiuretic hormone (ADH) acts. In the presence of ADH, the cell membranes become highly permeable to water, allowing water to move from the tubular fluid into the surrounding interstitial fluid and eventually back into the bloodstream. As a result, water is conserved and urine becomes more concentrated. When ADH levels are low, little water is reabsorbed, resulting in the production of larger volumes of dilute urine.
Type A Intercalated Cells
Type A intercalated cells are specialized for regulating the body’s acid-base balance. These cells secrete hydrogen ions (H⁺) into the tubular lumen while reabsorbing bicarbonate (HCO₃⁻) and potassium (K⁺) into the blood. By removing hydrogen ions from the body and conserving bicarbonate, these cells help correct acidosis and maintain normal blood pH.
Thus, while principal cells primarily control sodium, potassium, and water balance, intercalated cells mainly control acid-base balance.
The interaction of these two cell types allows the kidney to precisely regulate the final composition of urine. By the time the filtrate leaves the collecting tubule, the body has adjusted its sodium concentration, potassium concentration, acid-base status, and water content according to physiological needs.
Simple Concept
Think of the nephron as a factory:
- Early distal tubule = removes extra salt and minerals while keeping water behind.
- Principal cells = save sodium and water, throw away potassium.
- Type A intercalated cells = save bicarbonate, remove acid (H⁺).
- ADH = the “water-saving hormone” that determines how much water is reabsorbed.
KEY CONCEPT
The early distal tubule reabsorbs sodium, chloride, calcium, and magnesium and is almost impermeable to water, making it a diluting segment. The late distal tubule and cortical collecting tubule contain principal cells, which reabsorb sodium and water (under the influence of ADH) and secrete potassium, and Type A intercalated cells, which reabsorb bicarbonate and potassium while secreting hydrogen ions. Together, these segments provide the final regulation of electrolyte balance, acid-base balance, and water conservation before urine is excreted.
Sodium Reabsorption and Potassium Secretion by Principal Cells
The principal cells of the late distal tubule and cortical collecting tubule are responsible for the final regulation of sodium and potassium balance in the body. These cells determine how much sodium is retained and how much potassium is excreted in the urine. Their activity is strongly influenced by the hormone aldosterone, making them a key site for maintaining extracellular fluid volume and electrolyte balance.
The process begins when sodium (Na⁺) enters the principal cell from the tubular lumen through special sodium channels located on the luminal membrane. Because the intracellular sodium concentration is kept low, sodium readily moves from the lumen into the cell.
Once sodium enters the cell, it is actively transported out across the basolateral membrane by the Na⁺-K⁺ ATPase pump. This pump uses ATP to move sodium into the renal interstitial fluid while simultaneously transporting potassium into the cell. By continuously removing sodium from the cell, the pump maintains a low intracellular sodium concentration, which promotes further sodium entry from the tubular lumen.
As potassium accumulates inside the cell, it diffuses through potassium channels on the luminal membrane and enters the tubular fluid. Thus, principal cells perform two opposite functions simultaneously:
- Reabsorb sodium into the blood
- Secrete potassium into the urine
Because sodium is removed from the tubular lumen while negatively charged ions remain behind, the tubular lumen becomes electrically negative, reaching approximately −50 mV relative to the interstitial fluid. This negative luminal potential further favors the secretion of positively charged potassium ions into the tubular fluid.
Aldosterone greatly enhances these transport processes. It increases the number and activity of sodium channels and Na⁺-K⁺ ATPase pumps, leading to increased sodium reabsorption and increased potassium secretion. Therefore, aldosterone helps conserve sodium and water while promoting potassium excretion.
Several important drugs act on principal cells. Mineralocorticoid receptor antagonists, such as spironolactone and eplerenone, block the action of aldosterone. As a result, sodium reabsorption decreases and potassium secretion is reduced. Because they prevent excessive potassium loss, these drugs are known as potassium-sparing diuretics.
Another group of potassium-sparing diuretics includes amiloride and triamterene. These drugs directly block the luminal sodium channels through which sodium enters the principal cell. When sodium entry is reduced, less sodium is reabsorbed and the driving force for potassium secretion decreases. Consequently, potassium is retained in the body.
Simple Concept
Think of the principal cell as a sodium-potassium exchange station:
- Sodium enters the cell from the urine and is returned to the blood.
- Potassium enters the cell from the blood and is released into the urine.
- Aldosterone makes this exchange station work faster.
- Spironolactone and eplerenone block aldosterone’s effects.
- Amiloride and triamterene block sodium entry into the cell.
- Both groups of drugs reduce potassium loss and are therefore called potassium-sparing diuretics.
KEY CONCEPT
Principal cells of the late distal tubule and cortical collecting tubule reabsorb sodium and secrete potassium. Sodium enters through luminal sodium channels and is pumped into the blood by the Na⁺-K⁺ ATPase pump, while potassium moves into the tubular lumen through potassium channels. Aldosterone stimulates both sodium reabsorption and potassium secretion. Spironolactone and eplerenone block aldosterone action, whereas amiloride and triamterene block sodium channels. Both types of drugs decrease potassium secretion and are therefore classified as potassium-sparing diuretics.
INTERCALATED CELLS CAN SECRETE OR REABSORB HYDROGEN, BICARBONATE, AND POTASSIUM IONS
- Intercalated cells play a major role in acid-base regulation.
- Intercalated cells make up about 30% to 40% of the cells in the collecting tubules and collecting ducts.
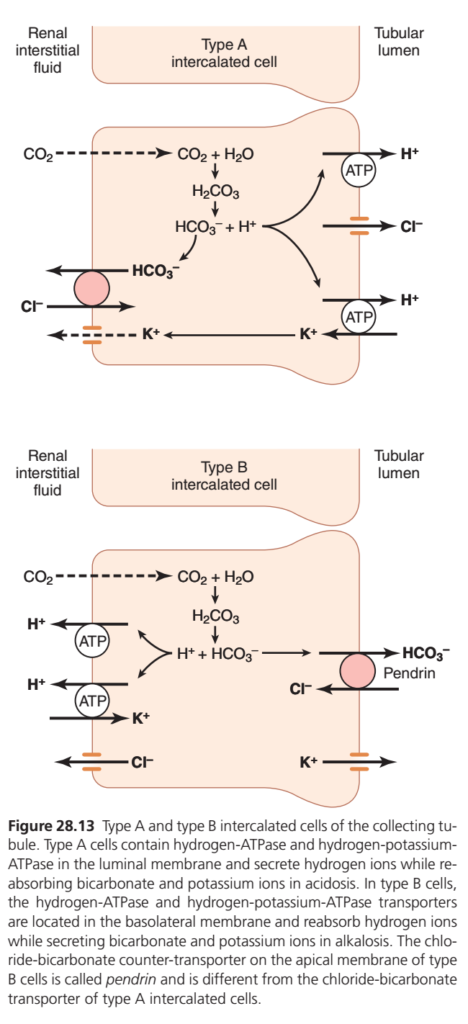
- Type A intercalated cells secrete hydrogen ions through a hydrogen-ATPase transporter.
- Type A intercalated cells also secrete hydrogen ions through a hydrogen-potassium-ATPase transporter.
- Hydrogen ions are produced inside the cell from water and carbon dioxide.
- Carbonic anhydrase converts water and carbon dioxide into carbonic acid.
- Carbonic acid then dissociates into hydrogen ions and bicarbonate ions.
- Hydrogen ions are secreted into the tubular lumen.
- For each hydrogen ion secreted, one bicarbonate ion becomes available for reabsorption across the basolateral membrane.
- Type A intercalated cells are especially important during acidosis.
- In acidosis, Type A intercalated cells remove hydrogen ions and reabsorb bicarbonate.
- Type B intercalated cells have functions opposite to those of Type A cells.
- Type B intercalated cells secrete bicarbonate into the tubular lumen.
- Type B intercalated cells reabsorb hydrogen ions during alkalosis.
- Type B intercalated cells have hydrogen and bicarbonate transporters on opposite sides of the cell compared with Type A cells.
- The chloride-bicarbonate counter-transporter in Type B cells is called pendrin.
- Pendrin is different from the chloride-bicarbonate transporter found in Type A cells.
- Hydrogen ions are actively transported out of Type B cells through a hydrogen-ATPase pump on the basolateral membrane.
- Bicarbonate is secreted into the tubular lumen by Type B cells.
- This process helps remove excess bicarbonate from the body during alkalosis.
- Chronic metabolic alkalosis increases the number of Type B intercalated cells.
- Increased Type B cells promote greater bicarbonate excretion.
- Acidosis increases the number of Type A intercalated cells.
- A more detailed explanation of this mechanism is discussed later.
- Intercalated cells can also reabsorb or secrete potassium ions.
- The late distal tubule and cortical collecting tubule are almost completely impermeable to urea.
- This characteristic is similar to the early distal tubule diluting segment.
- Most urea entering these segments passes into the collecting duct.
- The urea is eventually excreted in the urine or reabsorbed in the medullary collecting ducts.
- The late distal tubule and cortical collecting tubule reabsorb sodium ions.
- The late distal tubule and cortical collecting tubule reabsorb chloride ions.
- The late distal tubule and cortical collecting tubule reabsorb bicarbonate ions.
- The rate of reabsorption is controlled by hormones.
- Aldosterone is the most important hormone controlling this process.
- These segments also secrete potassium ions into the tubular lumen.
- These segments also secrete hydrogen ions into the tubular lumen.
- Aldosterone helps regulate potassium and hydrogen ion secretion.
- Potassium and hydrogen ion concentrations in body fluids also influence this process.
- Type A intercalated cells can actively secrete large amounts of hydrogen ions during acidosis.
- This secretion occurs through a hydrogen-ATPase mechanism.
- This mechanism differs from hydrogen ion secretion in the proximal tubule.
- Type A intercalated cells can secrete hydrogen ions against a very large concentration gradient.
- The gradient can be as high as 1000:1.
- The proximal tubule can create only a small hydrogen ion gradient.
- The proximal tubule usually achieves a gradient of about 4- to 10-fold.
- During alkalosis, Type B intercalated cells secrete bicarbonate.
- During alkalosis, Type B intercalated cells actively reabsorb hydrogen ions.
- Intercalated cells play a key role in acid-base regulation of body fluids.
- Water permeability of the late distal tubule and cortical collecting duct is controlled by ADH.
- ADH is also called vasopressin.
- When ADH levels are high, these segments become permeable to water.
- When ADH is absent, these segments are almost impermeable to water.
- This property helps control urine dilution and urine concentration.
KEY CONCEPT
- Intercalated cells regulate acid-base balance.
- Type A cells secrete hydrogen ions and reabsorb bicarbonate during acidosis.
- Type B cells secrete bicarbonate and reabsorb hydrogen ions during alkalosis.
- Intercalated cells can also reabsorb or secrete potassium.
- Late distal tubules and cortical collecting tubules reabsorb sodium, chloride, and bicarbonate.
- Aldosterone regulates sodium reabsorption and potassium/hydrogen secretion.
- These segments are almost impermeable to urea.
- ADH controls water permeability and helps regulate urine concentration.
TYPE A & TYPE B INTERCALATED CELLS — THE KIDNEY’S “ACID-BASE CORRECTION TEAM”
The collecting tubule contains special cells called intercalated cells. Their main job is to keep the body’s pH (acid-base balance) normal.
Think of them as two opposite workers:
- Type A cells = Fight Acidosis (Too Much Acid)
- Type B cells = Fight Alkalosis (Too Much Base)
They work like a thermostat that automatically corrects acid-base disturbances.
1. TYPE A INTERCALATED CELL
“REMOVE ACID, SAVE BICARBONATE”
When Does It Work?
Type A cells become active during:
✅ Acidosis
This means:
- Blood contains excess H⁺ ions
- Body fluids become too acidic
- pH falls below normal
The kidney must remove acid and restore pH.
What Happens Inside the Cell?
Carbon dioxide (CO₂) enters the cell from blood.
Inside the cell:
CO₂ + H₂O
↓
H₂CO₃ (carbonic acid)
↓
H⁺ + HCO₃⁻
The cell produces:
- Hydrogen ion (H⁺)
- Bicarbonate ion (HCO₃⁻)
What Happens to H⁺?
The cell actively pumps H⁺ into the tubular lumen using:
1. H⁺-ATPase Pump
Uses ATP energy
H⁺ → Urine
2. H⁺-K⁺ ATPase Pump
Moves:
- H⁺ into urine
- K⁺ into cell
Result:
More acid leaves the body.
What Happens to Bicarbonate?
The newly formed bicarbonate is transported into the blood.
Result:
Blood gains bicarbonate.
Since bicarbonate is the body’s major buffer, this helps neutralize excess acid.
Potassium Handling
The H⁺-K⁺ ATPase pump brings potassium into the cell.
Potassium is then returned to the blood.
Therefore Type A cells:
✅ Reabsorb potassium
Final Effect of Type A Cells
Urine
↑ H⁺ secretion
(more acidic urine)
Blood
↑ HCO₃⁻
↑ K⁺
↓
Acidosis corrected
EASY MEMORY
TYPE A = ACID OUT
A = Acidosis
Type A cells:
- Secrete H⁺
- Reabsorb HCO₃⁻
- Reabsorb K⁺
Purpose:
👉 Remove acid from the body
2. TYPE B INTERCALATED CELL
“REMOVE BICARBONATE, SAVE ACID”
Type B cells are almost the mirror image of Type A cells.
When Does It Work?
Type B cells become active during:
✅ Alkalosis
This means:
- Blood has too much bicarbonate
- Blood is too alkaline
- pH rises above normal
The kidney must reduce alkalinity.
What Happens Inside the Cell?
Just like Type A cells:
CO₂ + H₂O
↓
H₂CO₃
↓
H⁺ + HCO₃⁻
Again, hydrogen and bicarbonate are produced.
But now they move in the opposite direction.
What Happens to Bicarbonate?
Type B cells secrete bicarbonate into urine.
This occurs through a special transporter called:
Pendrin
Pendrin exchanges:
HCO₃⁻ out to urine
↓
Cl⁻ into cell
So the body loses bicarbonate.
What Happens to H⁺?
Hydrogen ions are transported into blood.
This helps restore acidity.
Potassium Handling
Potassium is secreted into the tubular lumen.
Therefore Type B cells:
✅ Secrete potassium
Final Effect of Type B Cells
Urine
↑ HCO₃⁻
↑ K⁺
Blood
↑ H⁺
↓
Alkalosis corrected
EASY MEMORY
TYPE B = BASE OUT
B = Base (Bicarbonate) Out
Type B cells:
- Secrete HCO₃⁻
- Reabsorb H⁺
- Secrete K⁺
Purpose:
👉 Remove excess bicarbonate from the body
THE BIG CONCEPT
The kidney has two opposite acid-base specialists:
| Type A Cell | Type B Cell |
|---|---|
| Active in Acidosis | Active in Alkalosis |
| Secretes H⁺ | Reabsorbs H⁺ |
| Reabsorbs HCO₃⁻ | Secretes HCO₃⁻ |
| Reabsorbs K⁺ | Secretes K⁺ |
| Makes urine acidic | Makes urine alkaline |
| Corrects Acidosis | Corrects Alkalosis |
SMART CLINICAL STORY
Imagine blood pH as a room temperature:
Blood Too Acidic (Acidosis)
Type A cell says:
“There is too much acid. Throw H⁺ into urine and save bicarbonate!”
Result:
✔ Acid removed
✔ Bicarbonate preserved
✔ pH rises toward normal
Blood Too Alkaline (Alkalosis)
Type B cell says:
“There is too much bicarbonate. Dump bicarbonate into urine and keep hydrogen ions!”
Result:
✔ Bicarbonate removed
✔ Acidity restored
✔ pH falls toward normal
KEY CONCEPT
Intercalated cells are the kidney’s acid-base regulators.
- Type A intercalated cells work during acidosis, secreting H⁺ while reabsorbing HCO₃⁻ and K⁺.
- Type B intercalated cells work during alkalosis, secreting HCO₃⁻ and K⁺ while reabsorbing H⁺.
- Together they keep body pH within the normal range and maintain acid-base homeostasis.
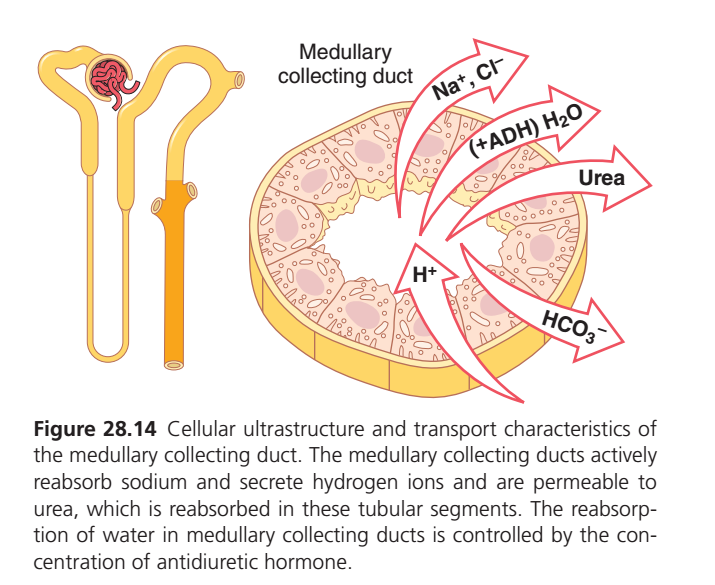
MEDULLARY COLLECTING DUCTS
- The medullary collecting ducts usually reabsorb less than 5% of the filtered water.
- The medullary collecting ducts usually reabsorb less than 5% of the filtered sodium.
- The medullary collecting ducts are the final site for processing urine.
- Therefore, they play a critical role in determining the final excretion of water and solutes.
- The epithelial cells of the collecting ducts are nearly cuboidal in shape.
- These cells have smooth surfaces.
- These cells contain relatively few mitochondria.
- The permeability of the medullary collecting duct to water is controlled by ADH.
- High levels of ADH cause water to be reabsorbed into the medullary interstitium.
- Water reabsorption reduces urine volume.
- Water reabsorption also concentrates solutes in the urine.
- Unlike the cortical collecting tubule, the medullary collecting duct is permeable to urea.
- Special urea transporters facilitate urea diffusion across the luminal membrane.
- Special urea transporters also facilitate urea diffusion across the basolateral membrane.
- Some tubular urea is reabsorbed into the medullary interstitium.
- Urea reabsorption increases the osmolality of the renal medulla.
- This helps the kidneys produce concentrated urine.
- The medullary collecting duct can secrete hydrogen ions against a large concentration gradient.
- This ability is similar to that of the cortical collecting tubule.
- Therefore, the medullary collecting duct plays an important role in acid-base regulation.
KEY CONCEPT
- Medullary collecting ducts reabsorb less than 5% of filtered water and sodium.
- They are the final site for urine processing.
- ADH controls water permeability in this segment.
- High ADH increases water reabsorption and concentrates urine.
- The medullary collecting duct is permeable to urea.
- Urea reabsorption increases medullary osmolality and helps concentrate urine.
- This segment can actively secrete hydrogen ions.
- Medullary collecting ducts contribute to acid-base regulation.
MEDULLARY COLLECTING DUCT (MCD)
30-Second Conceptual Summary
Think of the Medullary Collecting Duct as the kidney’s final urine adjustment station.
Before urine leaves the kidney, this segment makes the last important changes.
What Goes BACK to Blood? ✅
🧂 Na⁺ and Cl⁻
→ Reabsorbed
→ Body saves salt
💧 Water (H₂O)
→ Reabsorbed only when ADH is present
→ Concentrates urine
🧪 Urea
→ Reabsorbed into the medulla
→ Helps create a concentrated kidney medulla
🛡️ HCO₃⁻ (Bicarbonate)
→ Reabsorbed
→ Helps maintain normal blood pH
What Goes INTO Urine? ❌
🧨 H⁺ (Hydrogen ions)
→ Secreted into urine
→ Removes excess acid from the body
EASY MEMORY DIAGRAM
BLOOD
↑
Na+, Cl− ↑
H2O (ADH) ↑
Urea ↑
HCO3− ↑
--------------------------------
MEDULLARY COLLECTING DUCT
--------------------------------
↓
H+
↓
URINEBIG PICTURE
The Medullary Collecting Duct:
✅ Saves salt
✅ Saves water (under ADH control)
✅ Saves bicarbonate
✅ Reabsorbs urea
✅ Removes acid (H⁺)
✅ Determines final urine concentration
EXAM PEARL
“ADH acts mainly on the collecting ducts to increase water reabsorption and produce concentrated urine.”
KEY CONCEPT
The Medullary Collecting Duct is the kidney’s final urine-processing segment. It reabsorbs Na⁺, Cl⁻, water (with ADH), urea, and bicarbonate, while secreting H⁺. Therefore, it plays a major role in urine concentration and acid–base regulation.
SUMMARY OF CONCENTRATIONS OF DIFFERENT SOLUTES IN DIFFERENT TUBULAR SEGMENTS
- Whether a solute becomes concentrated in the tubular fluid depends on its reabsorption relative to water reabsorption.
- If a greater percentage of water is reabsorbed, the solute becomes more concentrated.
- If a greater percentage of the solute is reabsorbed, the solute becomes more diluted.
- The concentration of different substances changes in different parts of the renal tubule.
- The values shown represent the tubular fluid concentration divided by the plasma concentration of a substance.
- If the plasma concentration remains constant, changes in the tubular fluid/plasma ratio reflect changes in tubular fluid concentration.
- As filtrate moves through the tubular system, the concentration ratio increases above 1.0 if more water is reabsorbed than solute.
- The concentration ratio also increases if there is net secretion of the solute into the tubular fluid.
- If the concentration ratio decreases below 1.0, more solute has been reabsorbed relative to water.
- Substances such as creatinine become highly concentrated in the urine.
- These substances are generally not needed by the body.
- The kidneys reabsorb these substances very little or not at all.
- Some of these substances may also be secreted into the tubules.
- As a result, large amounts are excreted in the urine.
- Substances such as glucose and amino acids are strongly reabsorbed.
- These substances are important for the body and must be conserved.
- Therefore, almost none of these substances are lost in the urine.
- Inulin can be used to assess water reabsorption by the renal tubules.
- Inulin is a polysaccharide used to measure GFR.
- Inulin is neither reabsorbed nor secreted by the renal tubules.
- Therefore, changes in inulin concentration reflect changes in the amount of water in the tubular fluid.
- At the end of the proximal tubule, the tubular fluid/plasma concentration ratio for inulin is about 3.0.
- This means that the concentration of inulin in tubular fluid is three times higher than in plasma and glomerular filtrate.
- Because inulin is neither reabsorbed nor secreted, this ratio reflects water reabsorption.
- A ratio of 3.0 means that only one-third of the filtered water remains in the tubule.
- This also means that about two-thirds of the filtered water has been reabsorbed in the proximal tubule.
- At the end of the collecting ducts, the tubular fluid/plasma concentration ratio for inulin is about 125.
- This means that only 1/125 of the filtered water remains in the tubule.
- Therefore, more than 99% of the filtered water has been reabsorbed.
KEY CONCEPT
- Solute concentration depends on solute reabsorption relative to water reabsorption.
- More water reabsorption increases solute concentration.
- More solute reabsorption decreases solute concentration.
- Creatinine becomes highly concentrated because it is minimally reabsorbed.
- Glucose and amino acids are strongly reabsorbed and rarely appear in urine.
- Inulin is neither reabsorbed nor secreted and is used to assess water reabsorption.
- An inulin ratio of 3.0 indicates about 67% water reabsorption.
- An inulin ratio of 125 indicates more than 99% water reabsorption.
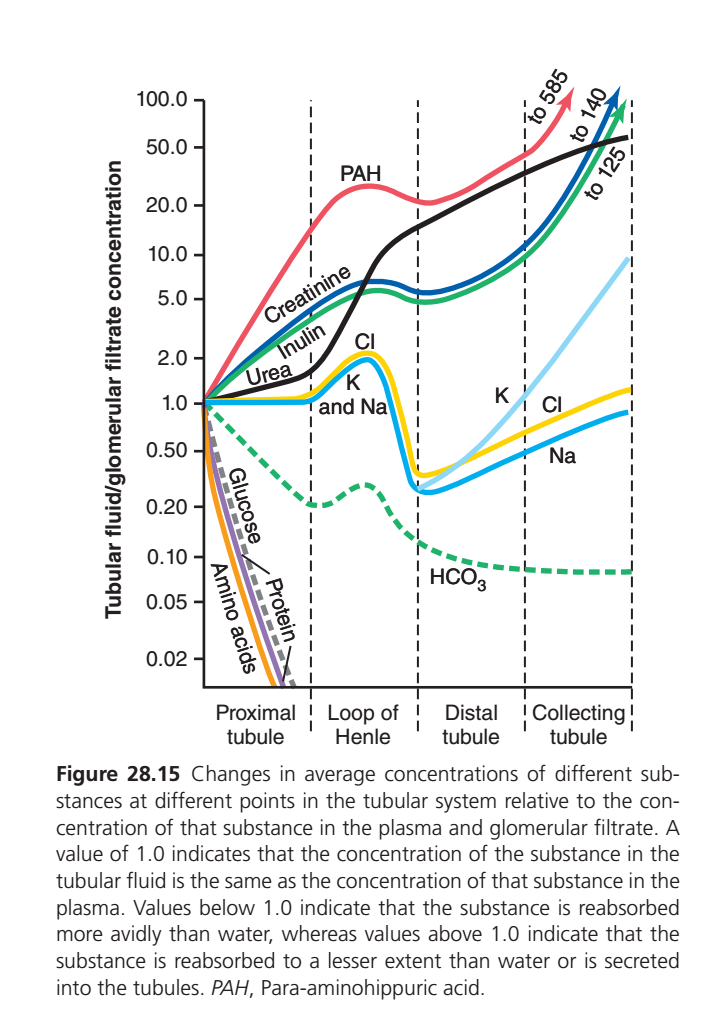
This graph shows:
Tubular Fluid Concentration ÷ Glomerular Filtrate Concentration (TF/P ratio)
Simple Rule
🔹 Ratio = 1
= Concentration in tubular fluid is same as plasma.
🔹 Ratio > 1
= Substance becomes more concentrated in tubule.
This happens when:
- Water is removed faster than the substance, OR
- The substance is secreted into the tubule.
🔹 Ratio < 1
= Substance becomes diluted in tubule.
This happens when:
1. PAH (RED LINE)
Highest line on graph
PAH = Para-aminohippuric acid
What happens?
Kidney:
- Filters PAH
- Also actively secretes PAH from blood into tubule
So PAH is continuously added into tubular fluid.
Result
Concentration rises dramatically:
1 → 10 → 20 → 50 → 85
Key Concept
✅ Filtration + Massive Secretion
Therefore PAH concentration becomes extremely high.
2. CREATININE (BLACK LINE)
What happens?
Creatinine:
- Freely filtered
- Almost not reabsorbed
- Slight secretion
Meanwhile water is being reabsorbed.
Result
Creatinine becomes progressively concentrated.
1 → 2 → 10 → 20 → 40 → 60
Key Concept
✅ Water leaves tubule
❌ Creatinine stays behind
Therefore concentration rises.
3. INULIN (GREEN SOLID LINE)
Most important reference substance
Inulin:
- Filtered
- Not reabsorbed
- Not secreted
Only water is removed.
Result
Concentration continuously increases.
1 → 2 → 5 → 20 → 50
Key Concept
✅ Perfect marker of water reabsorption
Whatever increase occurs is due only to water removal.
4. UREA (BLUE LINE)
What happens?
Urea is:
- Filtered
- Partially reabsorbed
But water is reabsorbed even more rapidly.
Result
Concentration rises initially.
1 → 2 → 5
Later some urea handling occurs in Loop of Henle and collecting ducts.
Finally concentration rises again.
Key Concept
✅ Reabsorbed
BUT
✅ Water removed faster
Therefore concentration still increases.
5. CHLORIDE (YELLOW LINE)
Proximal Tubule
Initially chloride is reabsorbed slower than water.
Water leaves first.
So chloride concentration rises slightly.
1 → 2
Thick Ascending Limb
Large NaCl reabsorption occurs.
Now chloride concentration falls sharply.
2 → 0.3
Collecting Duct
Water reabsorption increases chloride concentration again.
0.3 → 1.2
Key Concept
Initially water leaves faster.
Later chloride leaves faster.
6. SODIUM (BLUE-CYAN LINE)
What happens?
Sodium reabsorption closely follows water.
Therefore concentration stays near 1 in proximal tubule.
Loop of Henle
Large Na reabsorption occurs.
Concentration falls sharply.
1 → 0.25
Collecting Duct
Water removal causes slight increase.
0.25 → 0.8
Key Concept
✅ Sodium concentration usually changes little because water follows sodium.
7. POTASSIUM (LIGHT BLUE LINE)
Proximal Tubule
Potassium reabsorption parallels water.
Ratio remains around 1.
Thick Ascending Limb
Potassium reabsorbed.
Ratio falls.
Distal Tubule & Collecting Tubule
Principal cells secrete potassium.
Now concentration rises dramatically.
0.3 → 1 → 10
Key Concept
Early = Reabsorption
Late = Secretion
Therefore sharp upward rise.
8. BICARBONATE (GREEN DOTTED LINE)
Only DOTTED LINE
HCO₃⁻ is avidly reabsorbed.
Especially in:
- Proximal tubule
- Thick ascending limb
Result
Concentration steadily falls.
1 → 0.2 → 0.1 → 0.08
Key Concept
✅ Reabsorbed much faster than water
Therefore concentration becomes very low.
9. GLUCOSE (BLACK SOLID LINE GOING DOWN)
What happens?
Almost all glucose is reabsorbed in proximal tubule.
Result
1 → 0 very rapidly
By end of proximal tubule:
Almost none remains.
Key Concept
✅ Complete reabsorption
Normal urine contains no glucose.
10. AMINO ACIDS (PURPLE LINE)
What happens?
Almost 100% reabsorbed in proximal tubule.
Result
Rapid fall to near zero.
Key Concept
✅ Complete reabsorption
Normally absent in urine.
11. PROTEINS (GRAY DOTTED LINE)
What happens?
Very little protein is filtered.
Whatever small amount enters tubule is reabsorbed.
Result
Concentration falls rapidly toward zero.
Key Concept
✅ Filtered proteins are reclaimed.
Normally urine contains almost no protein.
WHO GOES UP AND WHO GOES DOWN?
Strong Upward Rise ↑
- PAH ↑↑↑ (secretion)
- Creatinine ↑
- Inulin ↑
- Urea ↑
- Potassium ↑ late
Strong Downward Fall ↓
- Glucose ↓↓↓
- Amino acids ↓↓↓
- Proteins ↓↓↓
- Bicarbonate ↓↓
Rise Then Fall Then Rise
- Sodium
- Chloride
- Potassium
because different nephron segments reabsorb or secrete them differently.UPER-FAST EXAM MEMORY
| Substance | Main Reason for Curve |
|---|---|
| PAH | Filtered + Secreted |
| Creatinine | Water removed, not reabsorbed |
| Inulin | Water removed only |
| Urea | Partly reabsorbed but water removed faster |
| Na⁺ | Reabsorbed with water |
| Cl⁻ | Initially lags behind water, later reabsorbed |
| K⁺ | Reabsorbed early, secreted late |
| HCO₃⁻ | Strongly reabsorbed |
| Glucose | Completely reabsorbed |
| Amino acids | Completely reabsorbed |
| Proteins | Reabsorbed after filtration |
KEY CONCEPT
Think of every line as answering one question:
“Compared with water, is this substance being reabsorbed faster, slower, or secreted?”
- Line goes UP → Substance remains in tubule or is secreted.
- Line goes DOWN → Substance is reabsorbed faster than water.
- Line stays near 1 → Substance and water are reabsorbed at similar rates.