


- The glomerular filtration rate (GFR) depends on two factors. 337
- The first factor is the glomerular filtration coefficient (Kf).
- The second factor is the net filtration pressure across the glomerular capillaries.
GFR Formula
GFR = Kf × Net Filtration Pressure
- The net filtration pressure is the sum of forces that favor or oppose filtration across the glomerular capillaries.
Forces That Affect Filtration
1. Glomerular Hydrostatic Pressure (PG)
- This is the pressure inside the glomerular capillaries.
- It promotes filtration.
2. Bowman Capsule Hydrostatic Pressure (PB)
- This is the pressure inside the Bowman capsule.
- It opposes filtration.
3. Glomerular Capillary Colloid Osmotic Pressure (πG)
- This pressure is produced by plasma proteins in the glomerular capillaries.
- It opposes filtration.
4. Bowman Capsule Colloid Osmotic Pressure (πB)
- This pressure is produced by proteins in the Bowman capsule.
- It promotes filtration.
- Under normal conditions, the protein concentration in the glomerular filtrate is very low.
- Therefore, the colloid osmotic pressure in the Bowman capsule is considered to be zero.
Complete GFR Formula
GFR = Kf × (PG − PB − πG + πB)
Normal Forces Favoring Filtration
| Force | Value (mm Hg) |
|---|---|
| Glomerular Hydrostatic Pressure (PG) | 60 |
| Bowman Capsule Colloid Osmotic Pressure (πB) | 0 |
Total Favoring Force
60 + 0 = 60 mm Hg
Normal Forces Opposing Filtration
| Force | Value (mm Hg) |
|---|---|
| Bowman Capsule Hydrostatic Pressure (PB) | 18 |
| Glomerular Capillary Colloid Osmotic Pressure (πG) | 32 |
Total Opposing Force
18 + 32 = 50 mm Hg
Net Filtration Pressure Calculation
Net Filtration Pressure = Favoring Forces − Opposing Forces
= 60 − 18 − 32
= 42 − 32
= +10 mm Hg
Easy Concept
60 mm Hg pushes fluid out of the capillaries.
18 mm Hg pushes back from Bowman capsule.
32 mm Hg pulls fluid back into the capillaries because of plasma proteins.
Final pressure available for filtration = +10 mm Hg.
Changes in Filtration Forces
- Some of these forces can change significantly during different physiological conditions.
- Other forces change mainly during disease states.
KEY CONCEPT
GFR is determined by the filtration coefficient (Kf) and the net filtration pressure. Glomerular hydrostatic pressure promotes filtration, while Bowman capsule hydrostatic pressure and glomerular colloid osmotic pressure oppose filtration. Normally, the net filtration pressure is +10 mm Hg (60 − 18 − 32 = 10 mm Hg), which drives filtration across the glomerular capillaries.
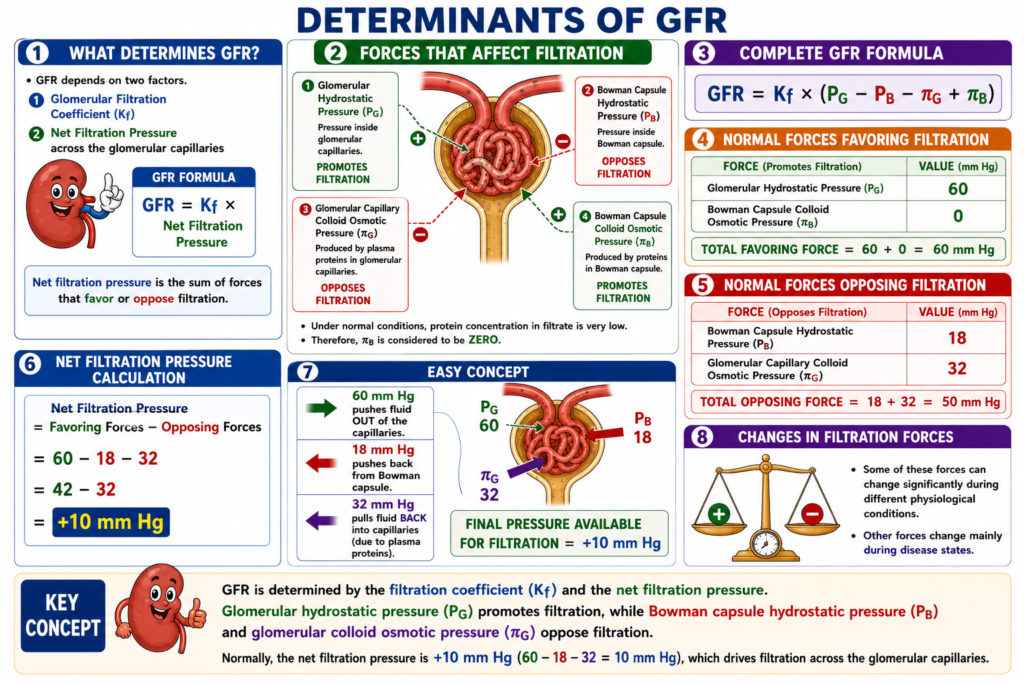
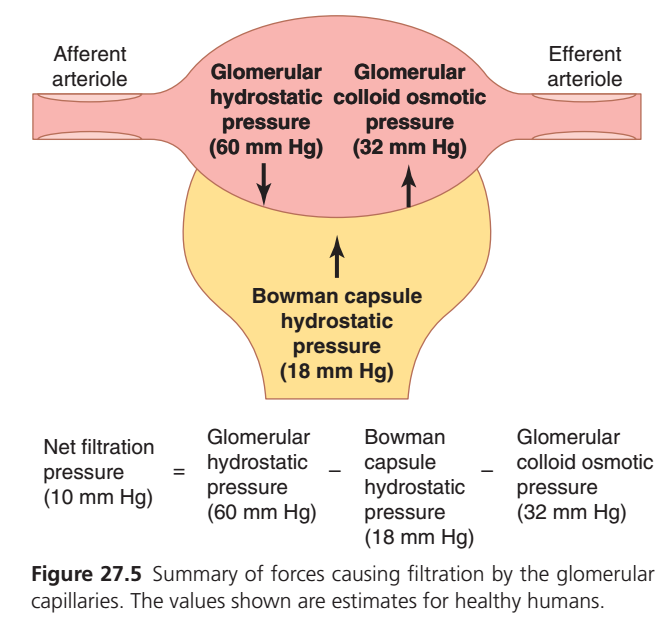
FIGURE 27.5 — FORCES DETERMINING GLOMERULAR FILTRATION
What Does This Figure Show?
- This figure shows the forces that promote and oppose filtration in the glomerulus.
- Filtration occurs when fluid moves from the glomerular capillaries into the Bowman capsule.
Force 1: Glomerular Hydrostatic Pressure (PG)
Value = 60 mm Hg
- This pressure is generated by the blood inside the glomerular capillaries.
- It pushes fluid out of the capillaries toward the Bowman capsule.
- It is the main force promoting filtration.
Direction
Glomerular capillaries
↓
Bowman capsule
✅ Promotes filtrationForce 2: Bowman Capsule Hydrostatic Pressure (PB)
Value = 18 mm Hg
- This pressure is produced by the fluid already present in the Bowman capsule.
- It pushes against the incoming filtrate.
- It acts in the opposite direction of filtration.
Direction
Bowman capsule
↑
Toward glomerular capillaries
❌ Opposes filtration
Force 3: Glomerular Colloid Osmotic Pressure (πG)
Value = 32 mm Hg
- Plasma proteins remain inside the glomerular capillaries.
- These proteins attract water back into the capillaries.
- This pulling force opposes filtration.
Direction
Bowman capsule
↑
Toward glomerular capillaries
❌ Opposes filtration
Understanding the Three Forces Together
Force Pushing Fluid Out
Glomerular Hydrostatic Pressure = 60 mm Hg
↓
Forces Pulling Fluid Back
Bowman Capsule Hydrostatic Pressure = 18 mm Hg
Glomerular Colloid Osmotic Pressure = 32 mm Hg
=
50 mm Hg
Net Filtration Pressure Calculation
Step 1
Force Favoring Filtration = 60 mm Hg
Step 2
Forces Opposing Filtration
= 18 + 32
= 50 mm Hg
Step 3
Net Filtration Pressure
= 60 − 18 − 32
= 42 − 32
= 10 mm Hg
Final Answer
Net Filtration Pressure = +10 mm Hg
Easy Memory Trick
“60 Pushes Out, 50 Pulls Back”
- 60 mm Hg pushes fluid out.
- 18 mm Hg pushes back.
- 32 mm Hg pulls back.
- Only 10 mm Hg remains to drive filtration.
Shortcut
60 − (18 + 32) = 10 mm Hg
KEY CONCEPT
Three forces determine glomerular filtration. Glomerular hydrostatic pressure (60 mm Hg) promotes filtration, while Bowman capsule hydrostatic pressure (18 mm Hg) and glomerular colloid osmotic pressure (32 mm Hg) oppose filtration. The net filtration pressure is 10 mm Hg (60 − 18 − 32 = 10 mm Hg), which drives fluid from the glomerular capillaries into the Bowman capsule.
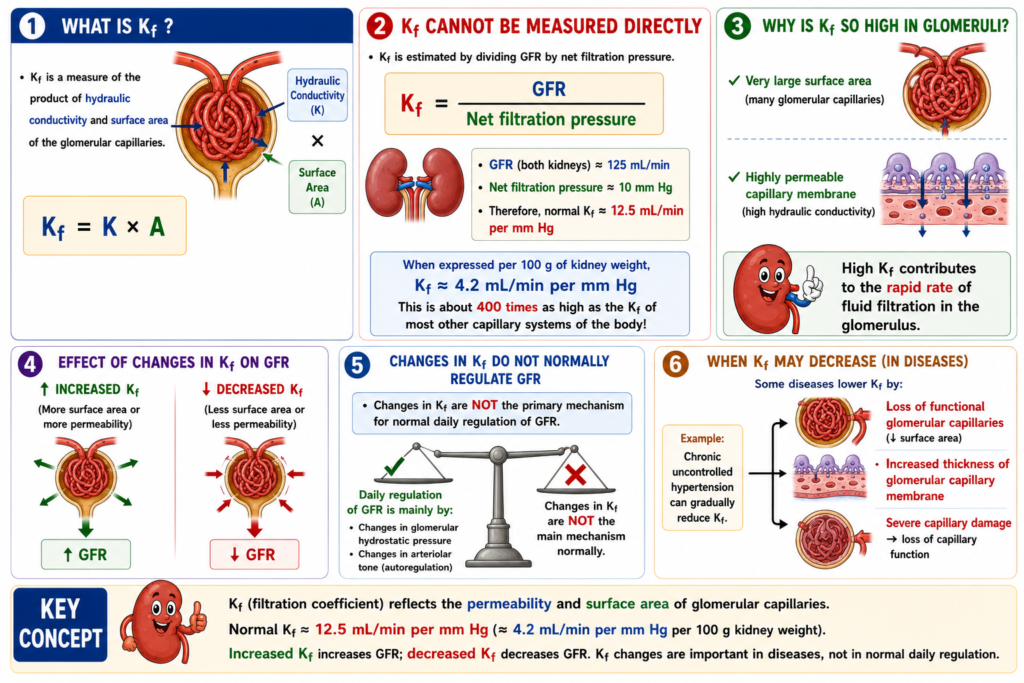
INCREASED GLOMERULAR CAPILLARY FILTRATION COEFFICIENT INCREASES GFR
- The filtration coefficient (Kf) is the product of the hydraulic conductivity and the surface area of the glomerular capillaries.
- Kf cannot be measured directly.
- It can be estimated experimentally by dividing the GFR by the net filtration pressure.
Kf Formula
Kf = GFR ÷ Net Filtration Pressure
Calculation of Normal Kf
- The total GFR of both kidneys is about 125 mL/min.
- The net filtration pressure is about 10 mm Hg.
Step-by-Step Calculation
Kf = GFR ÷ Net Filtration Pressure
Kf = 125 ÷ 10
Kf = 12.5 mL/min per mm Hg
Normal Value
Kf = 12.5 mL/min per mm Hg of filtration pressure
- When Kf is expressed per 100 grams of kidney weight, it averages about 4.2 mL/min per mm Hg.
- This value is about 400 times higher than the Kf of most other capillary systems in the body.
- The high Kf of the glomerular capillaries contributes to their rapid rate of fluid filtration.
Effect of Changes in Kf
- An increase in Kf increases the GFR.
- A decrease in Kf decreases the GFR.
- However, changes in Kf are not the primary mechanism for normal day-to-day regulation of GFR.
Diseases That Decrease Kf
- Some diseases reduce Kf.
- Kf may decrease when the number of functional glomerular capillaries decreases.
- This reduces the surface area available for filtration.
- Kf may also decrease when the glomerular capillary membrane becomes thicker.
- Increased membrane thickness reduces hydraulic conductivity.
Example: Chronic Uncontrolled Hypertension
- Chronic uncontrolled hypertension may gradually decrease Kf.
- It can increase the thickness of the glomerular capillary basement membrane.
- Over time, hypertension can severely damage the glomerular capillaries.
- This damage may eventually lead to loss of capillary function.
KEY CONCEPT
Kf is the product of glomerular capillary surface area and hydraulic conductivity. It can be calculated as Kf = GFR ÷ Net Filtration Pressure. Using GFR = 125 mL/min and Net Filtration Pressure = 10 mm Hg, Kf = 12.5 mL/min per mm Hg. A higher Kf increases GFR, while diseases such as chronic hypertension can decrease Kf by reducing filtration surface area or increasing membrane thickness.
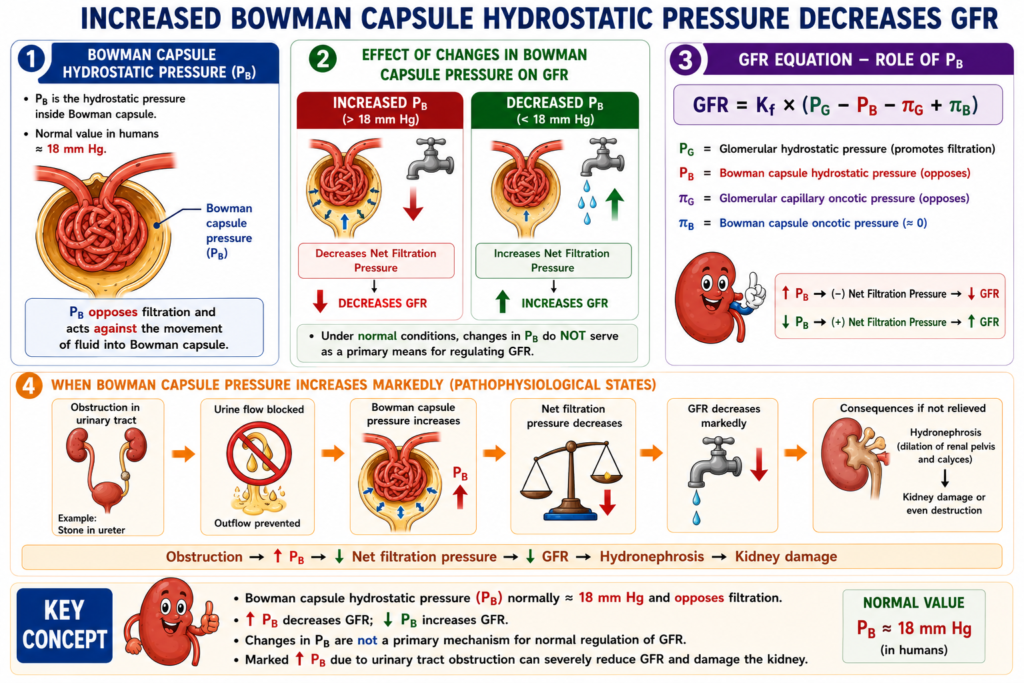
INCREASED BOWMAN CAPSULE HYDROSTATIC PRESSURE DECREASES GFR
- Direct measurements in experimental animals suggest that the normal Bowman capsule hydrostatic pressure in humans is about 18 mm Hg.
- Increasing the hydrostatic pressure in the Bowman capsule decreases GFR.
- Decreasing the hydrostatic pressure in the Bowman capsule increases GFR.
- Under normal conditions, changes in Bowman capsule pressure are not a primary mechanism for regulating GFR.
Effect of Increased Bowman Capsule Pressure
- In some pathological conditions, Bowman capsule pressure can increase greatly.
- A marked increase in Bowman capsule pressure causes a significant reduction in GFR.
Urinary Tract Obstruction
- Obstruction of the urinary tract can increase Bowman capsule pressure.
- Calcium crystals may precipitate and form stones.
- Uric acid may also precipitate and form stones.
- These stones may become lodged in the urinary tract.
- Stones often become lodged in the ureter.
- The obstruction blocks the outflow of urine.
- This blockage raises Bowman capsule pressure.
- The increased Bowman capsule pressure reduces GFR.
Consequences of Prolonged Obstruction
- Persistent obstruction can eventually cause hydronephrosis.
- Hydronephrosis means distention and dilation of the renal pelvis and calyces.
- If the obstruction is not relieved, kidney damage can occur.
- Severe obstruction may even destroy the kidney.
KEY CONCEPT
Normal Bowman capsule hydrostatic pressure is about 18 mm Hg. An increase in Bowman capsule pressure opposes filtration and decreases GFR, while a decrease in this pressure increases GFR. Urinary tract obstruction, such as kidney stones in the ureter, raises Bowman capsule pressure, reduces GFR, and may lead to hydronephrosis and kidney damage if not relieved.
INCREASED GLOMERULAR CAPILLARY COLLOID OSMOTIC PRESSURE DECREASES GFR
- As blood passes from the afferent arteriole through the glomerular capillaries to the efferent arteriole, the plasma protein concentration increases by about 20%.
- This increase occurs because about one-fifth of the fluid in the glomerular capillaries is filtered into the Bowman capsule.
- The plasma proteins are not filtered.
- Therefore, the plasma proteins become more concentrated in the glomerular capillaries.
- The normal colloid osmotic pressure of plasma entering the glomerular capillaries is about 28 mm Hg.
- By the time blood reaches the efferent end of the capillaries, the colloid osmotic pressure rises to about 36 mm Hg.
- The average glomerular capillary colloid osmotic pressure lies between 28 mm Hg and 36 mm Hg.
Calculation
Average Colloid Osmotic Pressure
= (28 + 36) ÷ 2
= 64 ÷ 2
= 32 mm Hg
- Therefore, the average glomerular capillary colloid osmotic pressure is about 32 mm Hg.
Factors Affecting Glomerular Capillary Colloid Osmotic Pressure
- Two factors influence the glomerular capillary colloid osmotic pressure.
- The first factor is the arterial plasma colloid osmotic pressure.
- The second factor is the filtration fraction.
- Increasing the arterial plasma colloid osmotic pressure increases the glomerular capillary colloid osmotic pressure.
- This increase tends to decrease GFR.
Effect of Filtration Fraction
- Increasing the filtration fraction concentrates the plasma proteins.
- This raises the glomerular capillary colloid osmotic pressure.
- The filtration fraction is defined as GFR divided by renal plasma flow.
Formula
Filtration Fraction = GFR ÷ Renal Plasma Flow
- The filtration fraction can increase if GFR increases.
- The filtration fraction can also increase if renal plasma flow decreases.
Example
- A reduction in renal plasma flow with no initial change in GFR increases the filtration fraction.
- The increased filtration fraction raises the glomerular capillary colloid osmotic pressure.
- The increased glomerular capillary colloid osmotic pressure tends to reduce GFR.
- Therefore, changes in renal blood flow can influence GFR independently of changes in glomerular hydrostatic pressure.
Effect of Increased Renal Blood Flow
- When renal blood flow increases, a smaller fraction of plasma is initially filtered from the glomerular capillaries.
- As a result, the glomerular capillary colloid osmotic pressure rises more slowly.
- The inhibitory effect of colloid osmotic pressure on GFR becomes less.
- Therefore, even when glomerular hydrostatic pressure remains constant, increased renal blood flow tends to increase GFR.
Effect of Decreased Renal Blood Flow
- When renal blood flow decreases, a larger fraction of plasma is initially filtered from the glomerular capillaries.
- As a result, the glomerular capillary colloid osmotic pressure rises more rapidly.
- The inhibitory effect of colloid osmotic pressure on GFR becomes greater.
- Therefore, even when glomerular hydrostatic pressure remains constant, decreased renal blood flow tends to decrease GFR.
KEY CONCEPT
Glomerular capillary colloid osmotic pressure opposes filtration and decreases GFR. As filtration occurs, plasma proteins become concentrated, causing colloid osmotic pressure to rise from 28 mm Hg to 36 mm Hg, with an average of 32 mm Hg. Increased arterial plasma protein concentration or increased filtration fraction raises glomerular colloid osmotic pressure and lowers GFR. Increased renal blood flow slows the rise in colloid osmotic pressure and increases GFR, whereas decreased renal blood flow speeds up the rise in colloid osmotic pressure and decreases GFR.
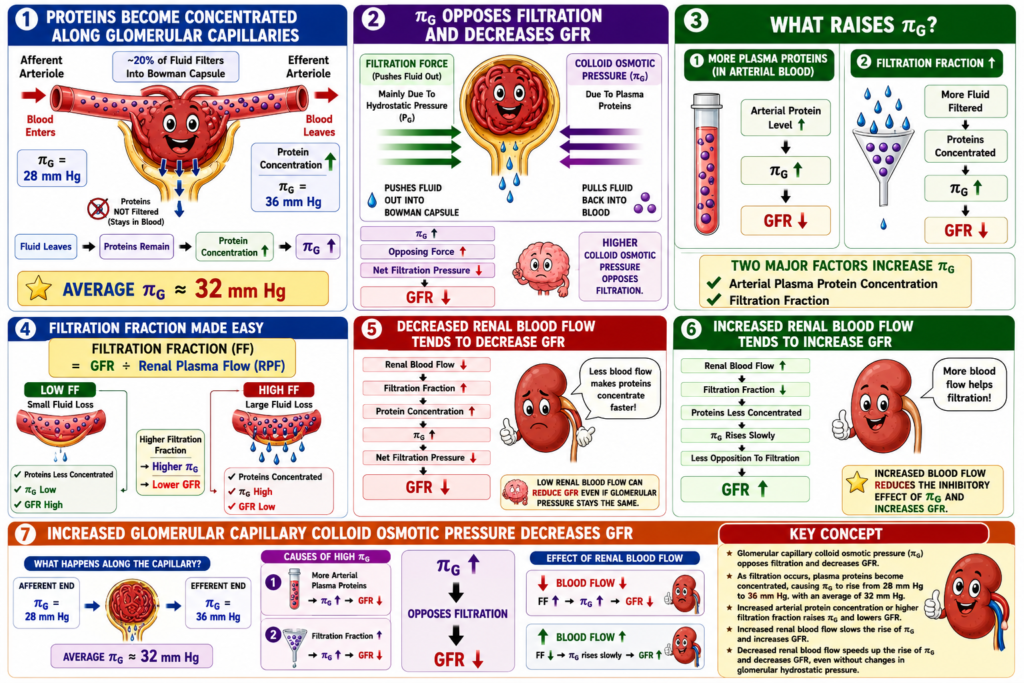
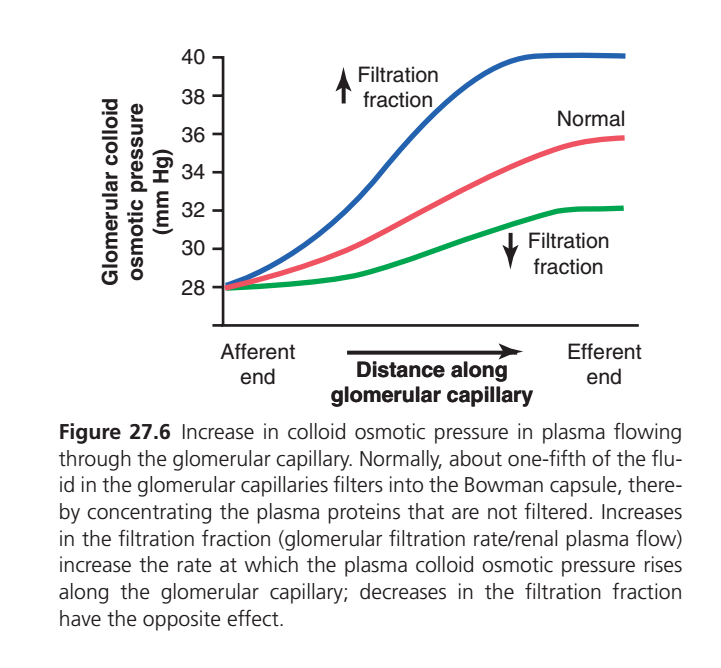
FIGURE 27.6 — EFFECT OF FILTRATION FRACTION ON GLOMERULAR COLLOID OSMOTIC PRESSURE
What Does This Graph Show?
- The graph shows how glomerular colloid osmotic pressure changes as blood flows from the afferent end to the efferent end of the glomerular capillary.
- The X-axis shows the distance along the glomerular capillary.
- The Y-axis shows the glomerular colloid osmotic pressure (mm Hg).
- At the afferent end, all three curves begin at about 28 mm Hg.
Red Line — Normal Filtration Fraction
- This is the normal situation.
- Blood enters the glomerulus with a colloid osmotic pressure of about 28 mm Hg.
- As filtration occurs, water leaves the capillaries.
- Plasma proteins remain in the capillaries.
- Therefore, the plasma proteins become progressively concentrated.
- The colloid osmotic pressure gradually increases.
- At the efferent end, it reaches about 36 mm Hg.
Meaning
✅ Normal filtration causes a gradual increase in plasma protein concentration.
✅ Colloid osmotic pressure rises from 28 → 36 mm Hg.
Blue Line — Increased Filtration Fraction
- This curve represents an increased filtration fraction.
- A larger fraction of plasma is filtered from the capillaries.
- More water leaves the capillaries.
- Plasma proteins become concentrated more rapidly.
- Therefore, colloid osmotic pressure rises more steeply.
- At the efferent end, it reaches about 40 mm Hg.
Meaning
✅ Increased filtration fraction causes a greater rise in plasma protein concentration.
✅ Higher colloid osmotic pressure produces a stronger opposition to filtration.
✅ GFR tends to decrease.
Green Line — Decreased Filtration Fraction
- This curve represents a decreased filtration fraction.
- A smaller fraction of plasma is filtered.
- Less water leaves the capillaries.
- Plasma proteins become concentrated more slowly.
- Therefore, colloid osmotic pressure rises more gradually.
- At the efferent end, it reaches only about 32 mm Hg.
Meaning
✅ Decreased filtration fraction causes less concentration of plasma proteins.
✅ Colloid osmotic pressure rises less.
✅ Opposition to filtration is reduced.
✅ GFR tends to increase.
Comparison of the Three Curves
Increased Filtration Fraction (Blue)
More filtration
→ More protein concentration
→ Higher colloid osmotic pressure
→ More opposition to filtration
→ ↓ GFR
Normal Filtration Fraction (Red)
Normal filtration
→ Normal protein concentration
→ Normal rise in colloid osmotic pressure
→ Normal GFR
Decreased Filtration Fraction (Green)
Less filtration
→ Less protein concentration
→ Lower colloid osmotic pressure
→ Less opposition to filtration
→ ↑ GFR
Easy Memory Trick
“More Filtration = More Protein Concentration”
↑ Filtration Fraction
→ ↑ Protein concentration
→ ↑ Colloid Osmotic Pressure
→ ↓ GFR
↓ Filtration Fraction
→ ↓ Protein concentration
→ ↓ Colloid Osmotic Pressure
→ ↑ GFR
KEY CONCEPT
As blood flows through the glomerular capillaries, filtration concentrates plasma proteins and increases glomerular colloid osmotic pressure. A higher filtration fraction causes a faster and greater rise in colloid osmotic pressure (up to about 40 mm Hg), which opposes filtration and tends to decrease GFR. A lower filtration fraction causes a smaller rise in colloid osmotic pressure (about 32 mm Hg), which reduces opposition to filtration and tends to increase GFR.
INCREASED GLOMERULAR CAPILLARY HYDROSTATIC PRESSURE INCREASES GFR
Normal Glomerular Hydrostatic Pressure
- The hydrostatic pressure inside glomerular capillaries is normally about 60 mm Hg.
- Changes in this pressure are the main way the body regulates GFR.
- When glomerular hydrostatic pressure increases, GFR increases.
- When glomerular hydrostatic pressure decreases, GFR decreases.
Factors That Determine Glomerular Hydrostatic Pressure
- Glomerular hydrostatic pressure depends on three controlled factors:
- Arterial pressure
- Afferent arteriolar resistance
- Efferent arteriolar resistance
Effect of Arterial Pressure
- Increased arterial pressure tends to increase glomerular hydrostatic pressure.
- Therefore, increased arterial pressure tends to increase GFR.
- This effect is reduced by autoregulatory mechanisms.
- These mechanisms help keep glomerular pressure relatively constant despite changes in arterial pressure.
Effect of Afferent Arteriolar Resistance
- Increased afferent arteriolar resistance decreases glomerular hydrostatic pressure.
- As a result, GFR decreases.
- Dilation of afferent arterioles increases glomerular hydrostatic pressure.
- Therefore, GFR increases.
Effect of Moderate Efferent Arteriolar Constriction
- Constriction of efferent arterioles increases resistance to blood leaving the glomerulus.
- This increases glomerular hydrostatic pressure.
- If renal blood flow is not reduced too much, GFR increases slightly.
Effect of Severe Efferent Arteriolar Constriction
- Efferent constriction also decreases renal blood flow.
- As efferent resistance increases, filtration fraction increases.
- Glomerular colloid osmotic pressure also increases.
- Severe constriction means more than about a 3-fold increase in efferent resistance.
- In severe constriction, the increase in colloid osmotic pressure becomes greater than the increase in hydrostatic pressure.
- The net filtration force decreases.
- As a result, GFR decreases.
Biphasic Effect of Efferent Arteriolar Constriction
- Efferent arteriolar constriction has a biphasic effect on GFR.
- Moderate constriction causes a slight increase in GFR.
- Severe constriction causes a decrease in GFR.
Why Severe Efferent Constriction Lowers GFR
- Severe efferent constriction progressively decreases renal plasma flow.
- Filtration fraction progressively increases.
- Glomerular plasma protein concentration progressively increases.
- Colloid osmotic pressure rises rapidly in a nonlinear manner.
- This rise occurs because of the Donnan effect.
- Higher protein concentration causes colloid osmotic pressure to rise more rapidly.
- Ions bound to plasma proteins also contribute to osmotic pressure.
Summary
- Constriction of afferent arterioles decreases GFR.
- Mild to moderate constriction of efferent arterioles increases GFR.
- Severe efferent arteriolar constriction decreases GFR.
- Severe constriction means more than about a 3-fold increase in efferent arteriolar resistance.
KEY CONCEPT
✅ GFR is mainly controlled by glomerular hydrostatic pressure.
✅ ↑ Arterial pressure → ↑ GFR
✅ Afferent constriction → ↓ GFR
✅ Afferent dilation → ↑ GFR
✅ Moderate efferent constriction → ↑ GFR
✅ Severe efferent constriction → ↓ GFR (because colloid osmotic pressure rises more than hydrostatic pressure)
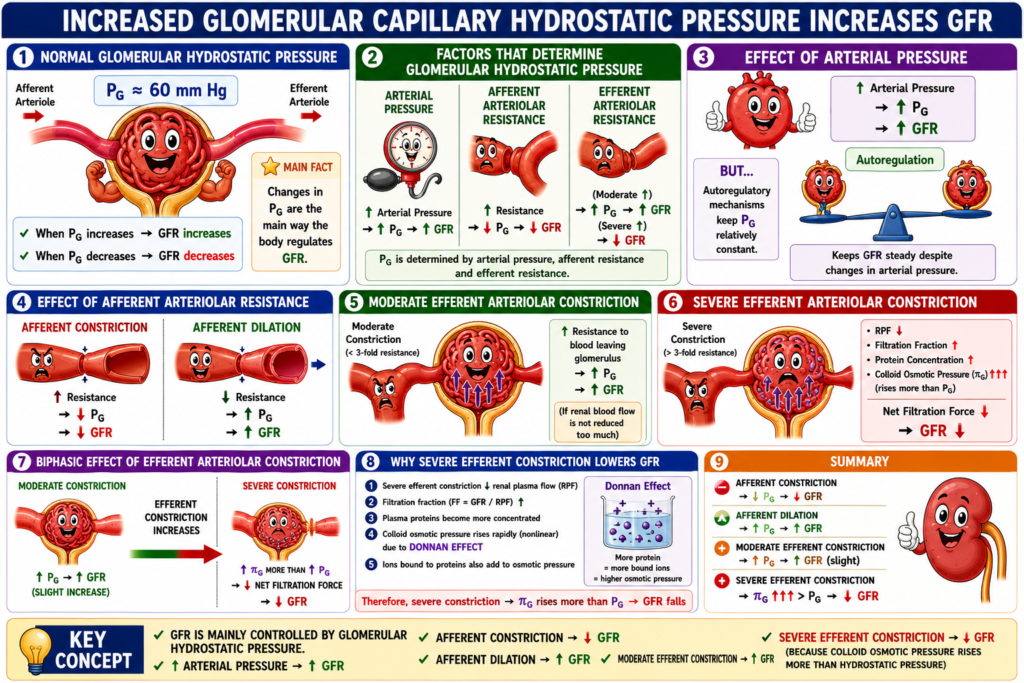
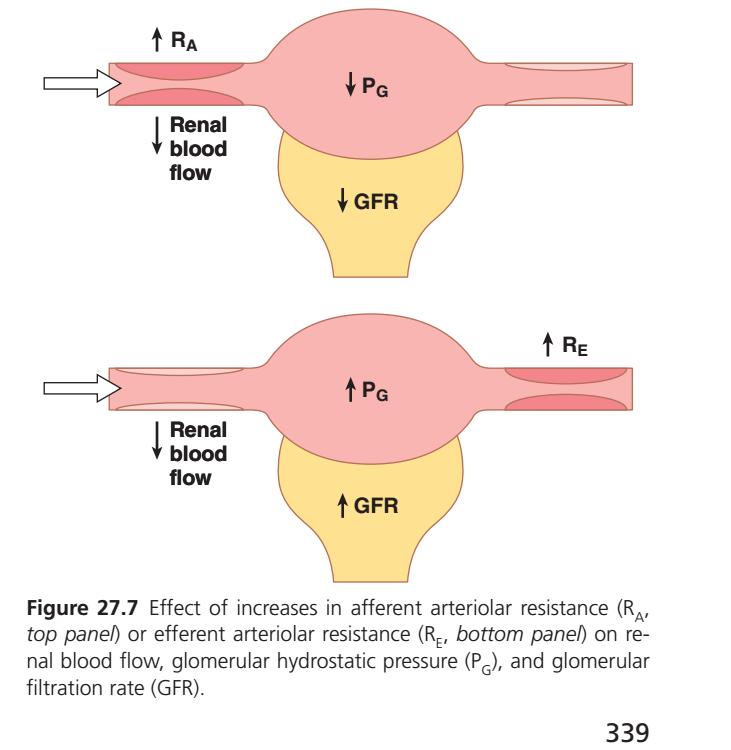
FIGURE 27.7: EFFECT OF AFFERENT AND EFFERENT ARTERIOLAR RESISTANCE ON GFR
Top Panel: Increased Afferent Arteriolar Resistance (↑ RA)
- The afferent arteriole becomes constricted.
- Less blood enters the glomerulus.
- Renal blood flow decreases (↓ Renal Blood Flow).
- Glomerular hydrostatic pressure decreases (↓ PG).
- Less fluid is filtered into Bowman’s capsule.
- GFR decreases (↓ GFR).
Easy Concept
Afferent arteriole = Entry pipe
- Narrow entry pipe → Less blood enters.
- Less pressure inside glomerulus.
- Less filtration occurs.
- GFR falls.
Bottom Panel: Increased Efferent Arteriolar Resistance (↑ RE)
- The efferent arteriole becomes constricted.
- Blood has more difficulty leaving the glomerulus.
- Renal blood flow decreases (↓ Renal Blood Flow).
- Blood backs up inside the glomerulus.
- Glomerular hydrostatic pressure increases (↑ PG).
- More filtration occurs.
- GFR increases (↑ GFR).
Easy Concept
Efferent arteriole = Exit pipe
- Narrow exit pipe → Blood cannot leave easily.
- Pressure builds up inside glomerulus.
- Filtration increases.
- GFR rises.
KEY CONCEPT
Afferent Constriction (↑ RA)
Narrow Entry Pipe
⬇ Blood enters glomerulus
⬇ Glomerular pressure (PG)
⬇ GFR
Efferent Constriction (↑ RE)
Narrow Exit Pipe
⬆ Blood trapped in glomerulus
⬆ Glomerular pressure (PG)
⬆ GFR (if constriction is moderate)
One-Line Memory Trick
Afferent Constriction = Less In → Less Filtered → ↓ GFR
Efferent Constriction = Less Out → More Pressure → ↑ GFR (moderate constriction)
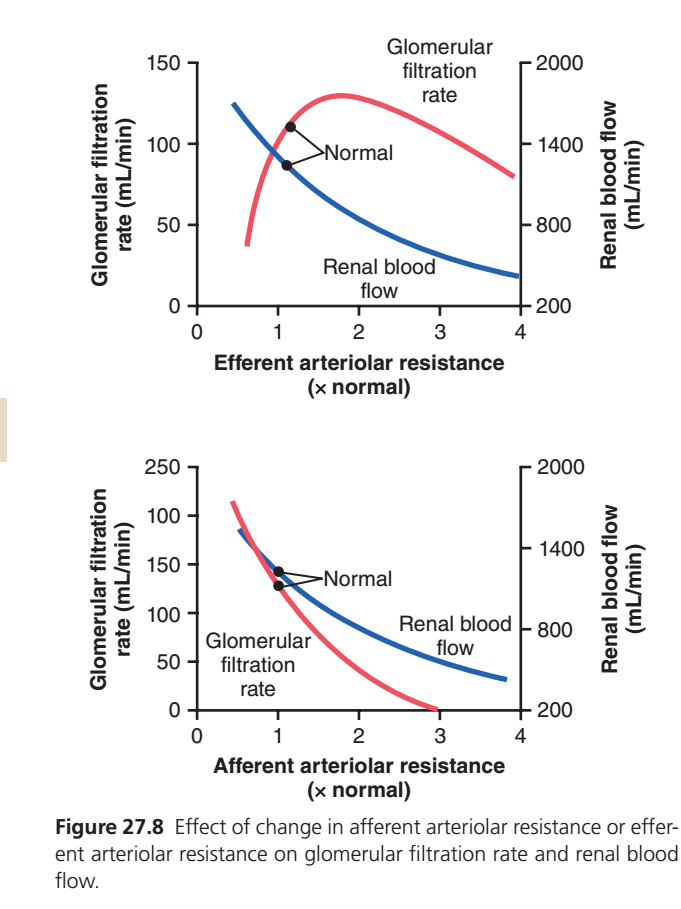
FIGURE 27.8: EFFECT OF AFFERENT AND EFFERENT ARTERIOLAR RESISTANCE ON GFR AND RENAL BLOOD FLOW
This figure shows how changing the diameter of the afferent or efferent arteriole affects:
- GFR (Glomerular Filtration Rate) → Red line
- Renal Blood Flow (RBF) → Blue line
The black dots labeled Normal represent normal kidney conditions.
TOP GRAPH: EFFECT OF EFFERENT ARTERIOLAR RESISTANCE
X-Axis
Efferent Arteriolar Resistance (× Normal)
Moving right means:
➡️ Increasing constriction of the efferent arteriole
➡️ The exit pipe is becoming narrower
Blue Line = Renal Blood Flow
As efferent resistance increases:
- Blood finds it harder to leave the glomerulus.
- Total renal blood flow decreases.
- Therefore the blue line continuously falls.
Easy Visualization
Normal Exit Pipe:
Blood →→→ exits easilyConstricted Exit Pipe:
Blood →→ (difficult exit)Result:
⬇ Renal Blood Flow
Red Line = GFR
Notice the red line first rises and then falls.
This is the most important concept in the graph.
Phase 1: Mild to Moderate Efferent Constriction
As the exit pipe narrows slightly:
- Blood gets trapped inside the glomerulus.
- Pressure inside glomerular capillaries increases.
- Glomerular hydrostatic pressure (PG) rises.
- More filtration occurs.
Result:
⬆ GFR
This explains why the red line rises at first.
Easy Analogy
Imagine a water balloon with a partially blocked outlet.
Water enters →→→
Outlet partly blockedPressure inside balloon rises.
More water is pushed through the filter.
Result:
⬆ GFR
Phase 2: Severe Efferent Constriction
As efferent constriction becomes very severe:
- Renal blood flow falls dramatically.
- Blood remains longer inside glomerular capillaries.
- More water leaves the blood.
- Plasma proteins become concentrated.
- Colloid osmotic pressure increases greatly.
Now proteins pull water back into capillaries.
This opposes filtration.
Result:
⬇ GFR
Therefore the red line begins to fall.
Why Does GFR Fall Despite High Pressure?
At severe constriction:
Hydrostatic pressure
VS
Protein osmotic pressureProtein osmotic pressure becomes stronger.
So net filtration decreases.
Result:
⬇ GFR
MEMORY POINT FROM TOP GRAPH
Moderate Efferent Constriction
↑ PG
↑ GFR
↓ RBFSevere Efferent Constriction
↓↓ RBF
↑↑ Protein concentration
↑↑ Colloid osmotic pressure
↓ GFRBOTTOM GRAPH: EFFECT OF AFFERENT ARTERIOLAR RESISTANCE
X-Axis
Afferent Arteriolar Resistance (× Normal)
Moving right means:
➡️ Increasing constriction of afferent arteriole
➡️ Entry pipe becomes narrower
Blue Line = Renal Blood Flow
As afferent resistance increases:
- Less blood enters the kidney.
- Renal blood flow decreases.
Therefore:
⬇ RBF
The blue line continuously falls.
Easy Visualization
Normal:
Blood →→→ enters glomerulusConstricted Afferent Arteriole:
Blood → (little entry)Result:
⬇ Renal Blood Flow
Red Line = GFR
As afferent resistance increases:
- Less blood enters glomerulus.
- Glomerular pressure decreases.
- Less fluid is filtered.
Result:
⬇ GFR
Therefore the red line continuously falls.
Why Does GFR Fall So Much?
The afferent arteriole is the entry gate.
If very little blood enters:
Less blood
↓
Less pressure
↓
Less filtration
↓
Lower GFRSo the red line falls sharply.
COMPARISON OF BOTH GRAPHS
| Change | Renal Blood Flow | GFR |
|---|---|---|
| Afferent Constriction | ↓ | ↓ |
| Mild Efferent Constriction | ↓ | ↑ |
| Severe Efferent Constriction | ↓↓ | ↓ |
SIMPLE PIPE TRICK
Afferent Arteriole = ENTRY PIPE
If entry pipe narrows:
Less blood enters
↓
Lower glomerular pressure
↓
Lower GFREfferent Arteriole = EXIT PIPE
If exit pipe narrows slightly:
Blood trapped
↓
Pressure rises
↓
Higher GFRIf exit pipe narrows too much:
Blood flow falls severely
↓
Proteins become concentrated
↓
Colloid osmotic pressure rises
↓
GFR fallsKEY CONCEPT
Afferent Constriction
Less In = Less Filtered = ↓ GFR
Mild Efferent Constriction
Less Out = More Pressure = ↑ GFR
Severe Efferent Constriction
Too Little Blood Flow + High Protein Concentration = ↓ GFR
One-Line Exam Formula
✅ Afferent constriction → ↓ RBF + ↓ GFR
✅ Moderate efferent constriction → ↓ RBF + ↑ GFR
✅ Severe efferent constriction → ↓↓ RBF + ↓ GFR
SUMMARY
The glomerular filtration rate (GFR) is the amount of fluid filtered from the glomerular capillaries into Bowman’s capsule each minute. It is one of the most important indicators of kidney function because it determines how effectively the kidneys filter blood and remove waste products. GFR depends on two major factors: the filtration coefficient (Kf) and the net filtration pressure acting across the glomerular capillaries.
The relationship can be expressed as:
GFR = Kf × Net Filtration Pressure
The net filtration pressure is determined by the balance between forces that favor filtration and forces that oppose filtration. The main force favoring filtration is the glomerular hydrostatic pressure (60 mm Hg), which pushes fluid out of the glomerular capillaries into Bowman’s capsule. Opposing this force are the Bowman capsule hydrostatic pressure (18 mm Hg) and the glomerular capillary colloid osmotic pressure (32 mm Hg), both of which resist filtration. Since the protein concentration in Bowman’s capsule is normally negligible, its colloid osmotic pressure is essentially zero. Therefore, the normal net filtration pressure is approximately 10 mm Hg, which drives filtration.
Another important determinant of GFR is the filtration coefficient (Kf), which reflects the permeability and surface area of the glomerular capillaries. The glomerular capillaries have an exceptionally high Kf compared with other capillary beds because they possess a large filtration surface area and a highly permeable filtration membrane. An increase in Kf increases GFR, whereas a decrease in Kf lowers GFR. Diseases such as chronic hypertension can reduce Kf by thickening the glomerular membrane and damaging capillaries, thereby reducing filtration efficiency.
The Bowman capsule hydrostatic pressure also influences GFR. An increase in this pressure opposes filtration and decreases GFR. Under normal conditions, Bowman capsule pressure remains relatively constant. However, urinary tract obstruction caused by kidney stones or other conditions can increase this pressure, resulting in a marked reduction in GFR. Prolonged obstruction may lead to hydronephrosis and kidney damage if left untreated.
The glomerular capillary colloid osmotic pressure is another force that opposes filtration. As plasma flows through the glomerular capillaries, water is filtered while proteins remain behind, causing protein concentration and colloid osmotic pressure to increase. This rise in osmotic pressure opposes further filtration. An increase in plasma protein concentration or filtration fraction raises colloid osmotic pressure and therefore decreases GFR. Conversely, increased renal blood flow slows the rise in protein concentration within the capillaries and tends to increase GFR.
The most important physiological regulator of GFR is the glomerular hydrostatic pressure. Increases in glomerular hydrostatic pressure increase GFR, whereas decreases reduce GFR. This pressure is determined mainly by arterial blood pressure and the resistance of the afferent and efferent arterioles. Dilation of the afferent arteriole allows more blood to enter the glomerulus, increasing hydrostatic pressure and GFR. In contrast, afferent arteriolar constriction decreases blood flow into the glomerulus and reduces GFR.
Changes in efferent arteriolar resistance have a more complex effect. Moderate constriction of the efferent arteriole increases glomerular hydrostatic pressure and slightly raises GFR. However, severe efferent constriction greatly reduces renal blood flow, causing plasma proteins to become highly concentrated within the glomerular capillaries. The resulting rise in colloid osmotic pressure eventually outweighs the increase in hydrostatic pressure, leading to a decrease in GFR. Therefore, efferent arteriolar constriction has a biphasic effect: moderate constriction increases GFR, whereas severe constriction decreases it.
The structure of the glomerular filtration membrane is essential for selective filtration. It consists of three layers: the fenestrated endothelium, the basement membrane, and the podocyte layer. Together, these structures allow rapid filtration of water and small solutes while preventing significant filtration of proteins and blood cells. The membrane is highly selective based on both molecular size and electrical charge. Small substances such as water, sodium, glucose, and inulin are freely filtered, whereas large proteins such as albumin are normally retained in the blood. Negatively charged molecules are filtered less readily because the filtration barrier itself carries strong negative charges that repel plasma proteins.
A clinical example of altered filtration is minimal-change nephropathy, in which damage to podocytes increases permeability to plasma proteins. As a result, proteins such as albumin leak into the urine, producing proteinuria or albuminuria. This condition demonstrates the importance of the filtration barrier in maintaining normal kidney function.
In summary, GFR is determined by the interaction of the filtration coefficient and the net filtration pressure across the glomerular capillaries. The major factors affecting GFR include glomerular hydrostatic pressure, Bowman capsule pressure, glomerular colloid osmotic pressure, and the filtration coefficient. Among these, glomerular hydrostatic pressure is the most important physiological regulator. Together, these factors ensure efficient filtration of blood while preserving essential proteins and maintaining normal fluid and electrolyte balance.