Edema
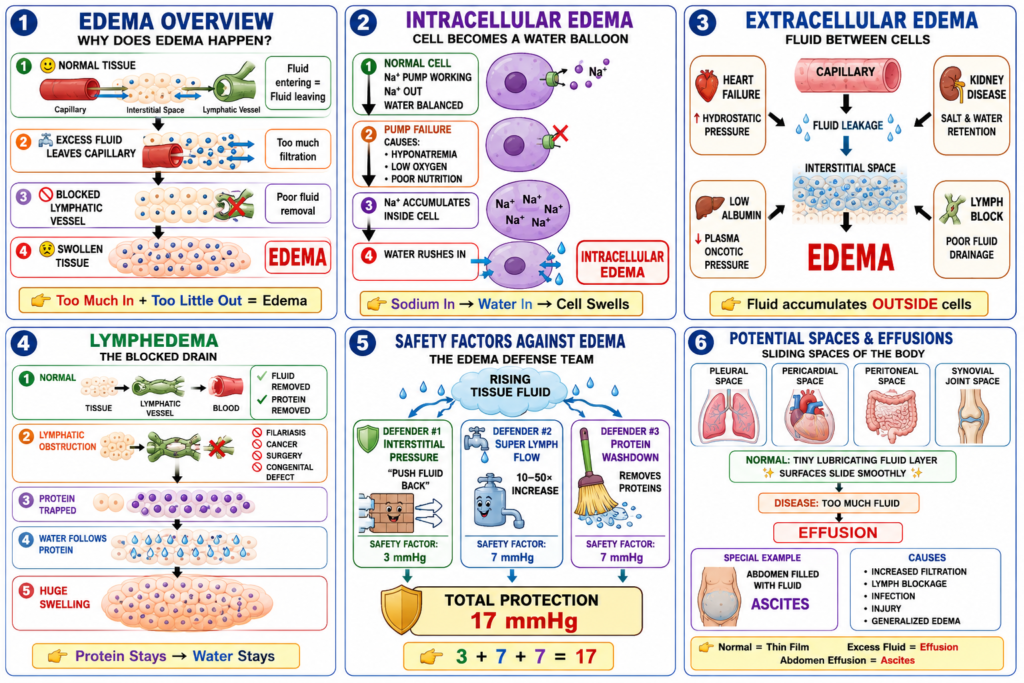
- Edema means there is too much fluid in the body tissues.
- In most cases, edema occurs in the extracellular fluid (ECF) compartment.
- Edema can also occur because of fluid accumulation inside the cells (intracellular fluid).
Key Concept: Edema = Excess fluid in body tissues, usually in the extracellular fluid, but it can also occur inside cells.
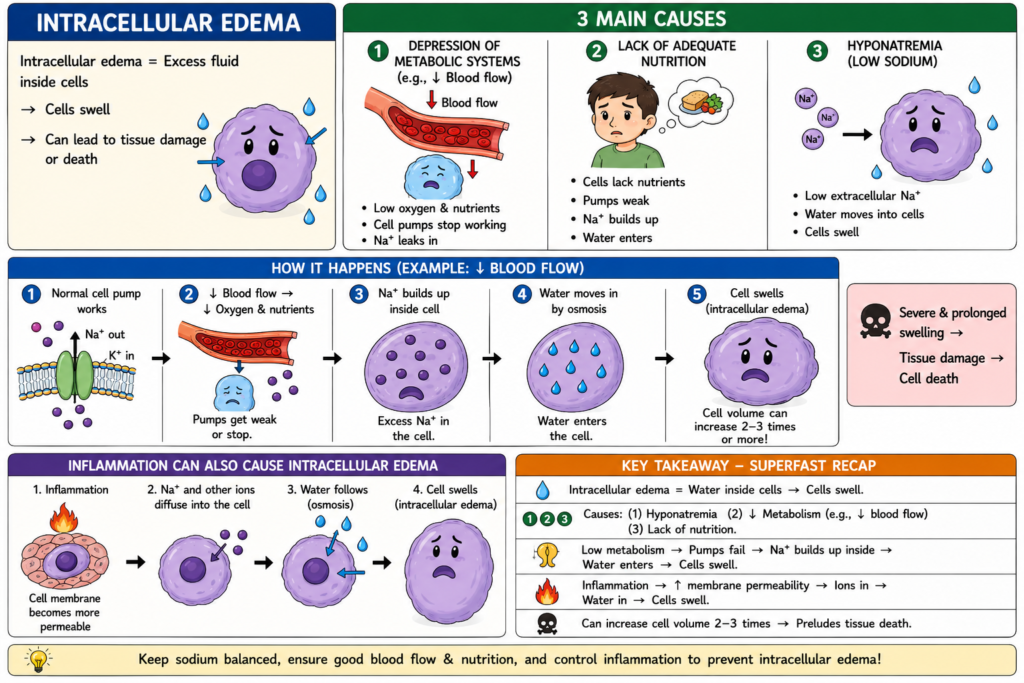
Intracellular Edema
- Three conditions commonly cause intracellular swelling:
- Hyponatremia.
- Depression of tissue metabolic systems.
- Lack of adequate nutrition to the cells.
- When blood flow to a tissue decreases, the supply of oxygen and nutrients also decreases.
- If blood flow becomes too low, normal tissue metabolism cannot be maintained.
- The cell membrane ionic pumps become depressed.
- Sodium ions normally leak into the cells.
- These sodium ions can no longer be pumped out of the cells.
- Excess sodium accumulates inside the cells.
- The increased intracellular sodium causes water to move into the cells by osmosis.
- This process can increase the intracellular volume of a tissue area.
- In some cases, the volume of an entire ischemic leg can increase to two to three times normal.
- A large increase in intracellular volume is usually a sign that tissue death may occur.
- Intracellular edema can also occur in inflamed tissues.
- Inflammation usually increases the permeability of the cell membrane.
- Sodium and other ions diffuse into the cells more easily.
- Water then moves into the cells by osmosis.
Key Concept: Intracellular edema occurs when sodium accumulates inside cells, causing water to enter the cells by osmosis and produce cell swelling.
Extracellular Edema
- Extracellular edema occurs when excess fluid accumulates in the extracellular spaces.
- There are two general causes of extracellular edema:
- Abnormal leakage of fluid from the plasma into the interstitial spaces through the capillaries.
- Failure of the lymphatic system to return fluid from the interstitial space back to the blood.
- Failure of lymphatic drainage is often called lymphedema.
- The most common clinical cause of interstitial fluid accumulation is excessive capillary fluid filtration.
Key Concept: Extracellular edema occurs when fluid accumulates in the extracellular space because of increased capillary fluid leakage or impaired lymphatic drainage.
Factors That Can Increase Capillary Filtration
- To understand the causes of excessive capillary filtration, it is important to review the factors that determine capillary filtration.
- The capillary filtration rate can be expressed mathematically as:
Filtration=Kf(Pc−Pif−πc+πif)
- Kf is the capillary filtration coefficient.
- Kf depends on the permeability and surface area of the capillaries.
- Pc is the capillary hydrostatic pressure.
- Pif is the interstitial fluid hydrostatic pressure.
- πc is the capillary plasma colloid osmotic pressure.
- πif is the interstitial fluid colloid osmotic pressure.
- From this equation, any of the following changes can increase the capillary filtration rate:
- Increased capillary filtration coefficient.
- Increased capillary hydrostatic pressure.
- Decreased plasma colloid osmotic pressure.
Key Concept: Capillary filtration increases when the capillary filtration coefficient increases, capillary hydrostatic pressure increases, or plasma colloid osmotic pressure decreases.
Solving the Filtration Equation (Easy Method)
Filtration=Kf(Pc−Pif−πc+πif)
Step 1: Understand Each Factor
- Kf = Capillary filtration coefficient
- Pc = Capillary hydrostatic pressure (pushes fluid out)
- Pif = Interstitial fluid hydrostatic pressure (opposes fluid movement out)
- πc = Plasma colloid osmotic pressure (pulls fluid into capillary)
- πif = Interstitial colloid osmotic pressure (pulls fluid out of capillary)
Step 2: Remember the Simple Rule
Forces that move fluid OUT of capillaries:
- Pc
- πif
Forces that move fluid INTO capillaries:
- − Pif
- − πc
Step 3: Calculate Net Filtration Pressure
Net Filtration Pressure (NFP) = Pc − Pif − πc + πif
Example
Suppose:
- Pc = 30 mmHg
- Pif = 2 mmHg
- πc = 25 mmHg
- πif = 5 mmHg
- Kf = 1
Then:
NFP = 30 − 2 − 25 + 5
NFP = 8 mmHg
Now multiply by Kf:
Filtration = 1 × 8 = 8
Filtration = 8 units
Super-Easy Memory Trick
OUT forces − IN forces
= (Pc + πif) − (Pif + πc)
= Net Filtration Pressure
Then:
Filtration = Kf × Net Filtration Pressure
Key Concept: First calculate the net force pushing fluid out of the capillary [(Pc + πif) − (Pif + πc)], then multiply by Kf to get the filtration rate.
Lymphedema—Failure of Lymph Vessels to Return Fluid and Protein to the Blood
- Lymphedema occurs when lymphatic function is greatly impaired.
- This may happen because of blockage or loss of lymph vessels.
- Edema can become very severe in these conditions.
- Plasma proteins that leak into the interstitial fluid cannot be removed.
- The protein concentration in the interstitial fluid increases.
- The increased protein concentration raises the interstitial fluid colloid osmotic pressure.
- This higher colloid osmotic pressure draws more fluid out of the capillaries.
- Blockage of lymph flow can occur with infections of the lymph nodes.
- One example is infection by filarial nematodes (Wuchereria bancrofti).
- These are microscopic threadlike worms.
- Adult worms live in the human lymphatic system.
- They spread from person to person through mosquitoes.
- People with filarial infection can develop severe lymphedema.
- They can also develop elephantiasis.
- Men may develop swelling of the scrotum, called hydrocele.
- Lymphatic filariasis affects millions of people in tropical and subtropical regions.
- Preventive chemotherapy has greatly reduced lymphatic filariasis over the past 20 years.
- Lymphedema can also occur in people with certain types of cancer.
- It can also occur after surgery that removes or blocks lymph vessels.
- During a radical mastectomy, many lymph vessels are removed.
- This reduces the removal of protein and fluid from the breast and arm regions.
- As a result, edema and tissue swelling can occur.
- Some lymph vessels regrow after surgery.
- Therefore, the interstitial edema is usually temporary.
Key Concept: Lymphedema occurs when lymphatic drainage is impaired, causing protein accumulation in the interstitial fluid, which increases interstitial colloid osmotic pressure and draws excess fluid into the tissues.
Summary of Causes of Extracellular Edema
I. Increased Capillary Hydrostatic Pressure
A. Excessive Kidney Retention of Salt and Water
- Acute kidney failure.
- Chronic kidney failure.
- Mineralocorticoid excess.
B. High Venous Pressure and Venous Constriction
- Heart failure.
- Venous obstruction.
- Failure of venous pumps:
- Paralysis of muscles.
- Immobilization of body parts.
- Failure of venous valves.
C. Decreased Arteriolar Resistance
- Excessive body heat.
- Insufficiency of the sympathetic nervous system.
- Vasodilator drugs.
II. Decreased Plasma Proteins
A. Loss of Proteins in Urine
- Nephrotic syndrome.
B. Loss of Plasma Proteins From Denuded Skin Areas
- Burns.
- Wounds.
C. Failure to Produce Plasma Proteins
- Liver disease (e.g., cirrhosis).
- Serious protein or caloric malnutrition.
III. Increased Capillary Permeability
- Immune reactions that release histamine and other immune products.
- Toxins.
- Bacterial infections.
- Vitamin deficiency, especially vitamin C.
- Prolonged ischemia.
- Burns.
IV. Blockage of Lymph Return
- Cancer.
- Infections (e.g., filarial nematodes).
- Surgery.
- Congenital absence or abnormality of lymphatic vessels.
Key Concept: Extracellular edema is caused by increased capillary hydrostatic pressure, decreased plasma proteins, increased capillary permeability, or blockage of lymphatic drainage.
Edema Caused by Heart Failure
- Heart failure is one of the most common and serious causes of edema.
- In heart failure, the heart cannot pump blood normally from the veins into the arteries.
- This increases venous pressure and capillary pressure.
- Increased capillary pressure causes increased capillary filtration.
- Arterial pressure tends to decrease.
- Decreased arterial pressure reduces the excretion of salt and water by the kidneys.
- The retained salt and water cause more edema.
- Blood flow to the kidneys is reduced in heart failure.
- Reduced kidney blood flow stimulates renin secretion.
- Renin increases the formation of angiotensin II.
- Angiotensin II increases aldosterone secretion.
- Angiotensin II and aldosterone cause additional salt and water retention by the kidneys.
- In advanced heart failure, ADH secretion increases.
- ADH increases water reabsorption by the renal tubules.
- This can lead to hyponatremia.
- Hyponatremia can cause intracellular edema.
- Increased water retention also contributes to extracellular edema.
- All of these factors together can cause severe generalized edema in untreated heart failure.
- In left-sided heart failure, the right ventricle pumps blood into the lungs normally.
- Blood cannot leave the lungs easily through the pulmonary veins to the left side of the heart.
- This occurs because the left side of the heart is greatly weakened.
- Pulmonary vascular pressures increase.
- Pulmonary capillary pressure also increases.
- Increased pulmonary capillary pressure causes pulmonary edema.
- Pulmonary edema is serious and life-threatening.
- If untreated, fluid can rapidly accumulate in the lungs.
- Death may occur within a few hours.
Key Concept: Heart failure causes edema by increasing capillary hydrostatic pressure and promoting salt and water retention by the kidneys, leading to generalized edema and, in left-sided heart failure, life-threatening pulmonary edema.
Edema Caused by Decreased Kidney Excretion of Salt and Water
- Most sodium chloride added to the blood remains in the extracellular fluid (ECF).
- Only a small amount of sodium chloride enters the cells.
- In kidney diseases, urinary excretion of salt and water may be impaired.
- As a result, excessive sodium chloride and water accumulate in the extracellular fluid.
- Most of the retained salt and water leak from the blood into the interstitial spaces.
- Some of the retained fluid remains in the blood.
- The main effects are:
- Widespread increase in interstitial fluid volume (extracellular edema).
- Hypertension due to increased blood volume.
- In acute glomerulonephritis, the renal glomeruli are damaged by inflammation.
- Damaged glomeruli cannot filter adequate amounts of fluid.
- This leads to retention of salt and water.
- Serious extracellular edema usually develops.
- Hypertension also usually develops.
Key Concept: Impaired kidney excretion of salt and water causes retention of sodium chloride and water, leading to extracellular edema and increased blood volume that produces hypertension.
Edema Caused by Decreased Plasma Proteins
- Failure to produce normal amounts of plasma proteins can decrease plasma protein levels.
- Leakage of proteins from the plasma can also decrease plasma protein levels.
- Decreased plasma proteins lower the plasma colloid osmotic pressure.
- Lower plasma colloid osmotic pressure increases capillary filtration throughout the body.
- Increased capillary filtration causes extracellular edema.
- Large amounts of protein may be lost in the urine in certain kidney diseases.
- This condition is called nephrotic syndrome.
- Various kidney diseases can damage the glomerular membranes.
- Damaged glomerular membranes become leaky to plasma proteins.
- Large quantities of plasma proteins can pass into the urine.
- Plasma protein concentration decreases when protein loss exceeds protein synthesis.
- Serious generalized edema occurs when plasma protein concentration falls below 2.5 g/100 mL.
- Cirrhosis of the liver is associated with damage to many liver parenchymal cells.
- Damaged liver cells are replaced by scar tissue (fibrosis).
- The liver becomes less able to produce sufficient plasma proteins.
- Albumin production is especially reduced.
- Reduced plasma proteins lower plasma colloid osmotic pressure.
- This causes the generalized edema associated with cirrhosis.
- Cirrhosis can also cause edema by compressing the portal venous drainage vessels.
- Fibrosis may obstruct blood flow through the liver.
- This increases portal venous pressure (portal hypertension).
- Increased portal venous pressure raises capillary hydrostatic pressure in the gastrointestinal area.
- Increased capillary hydrostatic pressure increases fluid filtration from the plasma.
- The combination of low plasma protein concentration and high portal capillary pressure causes large amounts of fluid and protein to move into the abdominal cavity.
- This condition is called ascites.
Key Concept: Decreased plasma proteins lower plasma colloid osmotic pressure, causing increased capillary filtration and edema. In cirrhosis, both reduced albumin production and portal hypertension contribute to edema and ascites.
Safety Factors That Normally Prevent Edema
- Many disturbances can cause edema.
- However, the abnormality usually must be severe before serious edema develops.
- Three major safety factors help prevent excessive fluid accumulation in the interstitial spaces.
1. Low Compliance of the Interstitium
- The interstitium has low compliance when interstitial fluid pressure is in the negative pressure range.
- This helps prevent excessive fluid accumulation.
2. Increased Lymph Flow
- Lymph flow can increase 10- to 50-fold.
- Increased lymph flow helps remove excess fluid from the interstitial spaces.
3. Washdown of Interstitial Fluid Proteins
- Increased capillary filtration reduces the concentration of proteins in the interstitial fluid.
- This process is called washdown.
- Reduced interstitial protein concentration lowers interstitial fluid colloid osmotic pressure.
- Lower interstitial colloid osmotic pressure helps reduce further fluid accumulation.
Key Concept: Edema is normally prevented by low interstitial compliance, greatly increased lymph flow, and washdown of interstitial proteins, all of which limit excess fluid accumulation in the interstitial spaces.
Safety Factor Caused by Low Compliance of the Interstitium in the Negative Pressure Range
- Interstitial fluid hydrostatic pressure in loose subcutaneous tissues is normally slightly below atmospheric pressure.
- The average interstitial fluid hydrostatic pressure is about −3 mm Hg.
- This slight suction helps hold the tissues together.
- When interstitial fluid pressure is in the negative range, small changes in interstitial fluid volume cause relatively large changes in interstitial fluid hydrostatic pressure.
- Therefore, tissue compliance is low in the negative pressure range.
- Compliance is defined as the change in volume per mm Hg change in pressure.
- Low tissue compliance acts as a safety factor against edema.
- When interstitial fluid hydrostatic pressure increases, it opposes further capillary filtration.
- As long as interstitial fluid pressure remains negative, a small increase in interstitial fluid volume causes a relatively large increase in interstitial fluid pressure.
- The increased interstitial pressure opposes further movement of fluid into the tissues.
- The normal interstitial fluid hydrostatic pressure is about −3 mm Hg.
- Interstitial pressure must increase by about 3 mm Hg before large amounts of fluid begin to accumulate in the tissues.
- Therefore, the safety factor against edema provided by this mechanism is about 3 mm Hg.
- In the positive pressure range, tissue compliance increases greatly.
- When tissue compliance increases, this safety factor against edema is lost.
Key Concept: Low compliance of the interstitium in the negative pressure range causes small increases in tissue fluid volume to produce large increases in interstitial pressure, which opposes further capillary filtration and helps prevent edema (safety factor ≈ 3 mm Hg).
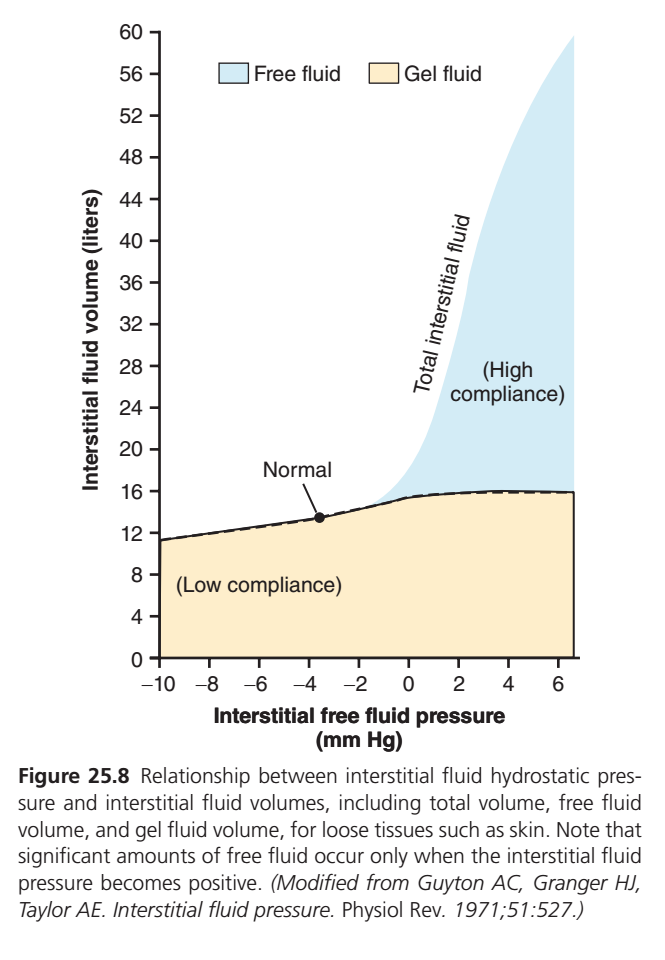
Importance of Interstitial Gel in Preventing Fluid Accumulation in the Interstitium
- In normal tissues with negative interstitial fluid pressure, almost all interstitial fluid is present in gel form.
- The fluid is bound within a proteoglycan meshwork.
- There are virtually no free fluid spaces larger than a few hundredths of a micrometer in diameter.
- The interstitial gel prevents fluid from flowing easily through the tissues.
- The proteoglycan filaments act as a barrier to fluid movement.
- When interstitial fluid pressure becomes more negative, the gel does not contract very much.
- The proteoglycan meshwork provides elastic resistance to compression.
- In the negative pressure range, interstitial fluid volume changes very little.
- This occurs whether the pressure is only a few mm Hg below zero or 10 to 20 mm Hg below zero.
- Therefore, tissue compliance is very low in the negative pressure range.
- When interstitial fluid pressure rises into the positive pressure range, free fluid begins to accumulate in the tissues.
- In this range, the tissues become more compliant.
- Large amounts of fluid can accumulate with only small increases in interstitial fluid pressure.
- Most of the extra fluid accumulates as free fluid.
- The free fluid pushes the proteoglycan filaments apart.
- As a result, the fluid can move freely through the tissue spaces.
- The fluid is no longer in gel form.
- When free fluid accumulates, the edema is called pitting edema.
- Pressing a thumb against the swollen tissue pushes the fluid away from that area.
- After the thumb is removed, a pit remains in the skin for a few seconds.
- The pit disappears when fluid flows back from the surrounding tissues.
- Pitting edema is different from nonpitting edema.
- Nonpitting edema occurs when tissue cells swell instead of the interstitium.
- It can also occur when interstitial fluid becomes clotted with fibrinogen.
- In these conditions, the fluid cannot move freely through the tissue spaces.
Key Concept: Interstitial gel normally prevents free fluid accumulation and limits fluid movement through tissues. When interstitial pressure becomes positive, free fluid accumulates, tissue compliance increases, and pitting edema develops.
Importance of Proteoglycan Filaments as a Spacer for Cells and in Preventing Rapid Flow of Fluid in Tissues
- Proteoglycan filaments and collagen fibrils act as spacers between cells.
- Nutrients and ions do not diffuse readily through cell membranes.
- Adequate spacing between cells is necessary for rapid exchange of substances.
- This spacing allows nutrients and electrolytes to move between blood capillaries and cells.
- It also allows waste products to move from cells to the blood.
- Proteoglycan filaments prevent fluid from flowing too easily through the tissue spaces.
- Without proteoglycan filaments, fluid would move freely through the interstitium.
- Simply standing upright would cause large amounts of interstitial fluid to move from the upper body to the lower body.
- When excessive fluid accumulates in the interstitium, as occurs in edema, large fluid channels are formed.
- These channels allow fluid to flow more easily through the interstitial spaces.
- In severe leg edema, fluid accumulation can often be reduced by elevating the legs.
- Although proteoglycan filaments restrict bulk fluid flow, they do not greatly interfere with diffusion.
- Different substances within the fluid can diffuse through the tissues at least 95% as easily as normal.
- Nutrients can still diffuse efficiently to the cells.
- Waste products can still be removed efficiently from the cells.
- Therefore, normal exchange of substances is not significantly impaired by the proteoglycan filaments of the interstitium.
Key Concept: Proteoglycan filaments act as spacers between cells, prevent rapid bulk flow of interstitial fluid, and help maintain tissue fluid distribution, while still allowing nearly normal diffusion of nutrients and waste products.
Increased Lymph Flow as a Safety Factor Against Edema
- A major function of the lymphatic system is to return fluid and proteins from the interstitium back to the circulation.
- These fluid and proteins are continuously filtered from the capillaries into the interstitial spaces.
- The lymphatic system returns them to the blood.
- Without this continuous return of fluid and proteins:
- Plasma volume would rapidly decrease.
- Interstitial edema would develop.
- The lymphatic system acts as a major safety factor against edema.
- When fluid begins to accumulate in the tissues, lymph flow can increase 10- to 50-fold.
- Increased lymph flow removes large amounts of fluid from the interstitial spaces.
- Increased lymph flow also removes large amounts of proteins from the interstitium.
- This response occurs when capillary filtration increases.
- The increased lymphatic drainage helps prevent excessive fluid accumulation in the tissues.
- It also prevents interstitial fluid pressure from rising into the positive pressure range.
- The safety factor provided by increased lymph flow is about 7 mm Hg.
Key Concept: Increased lymph flow is a major safety factor against edema because it can increase 10- to 50-fold to remove excess interstitial fluid and proteins, preventing excessive fluid accumulation (safety factor ≈ 7 mm Hg).
Washdown of Interstitial Fluid Protein as a Safety Factor Against Edema
- When increased amounts of fluid are filtered into the interstitium, interstitial fluid pressure rises.
- Increased interstitial fluid pressure causes increased lymph flow.
- In most tissues, interstitial protein concentration decreases as lymph flow increases.
- This occurs because the lymphatic system removes proteins faster than proteins are filtered out of the capillaries.
- Capillaries are relatively impermeable to proteins compared with lymph vessels.
- Therefore, proteins are washed out of the interstitial fluid as lymph flow increases.
- The proteins in the interstitial fluid create interstitial colloid osmotic pressure.
- Interstitial colloid osmotic pressure tends to draw fluid out of the capillaries.
- When interstitial protein concentration decreases, interstitial colloid osmotic pressure also decreases.
- Lower interstitial colloid osmotic pressure reduces the net filtration force across the capillaries.
- This helps prevent further accumulation of fluid in the tissues.
- The safety factor provided by this mechanism is about 7 mm Hg.
Key Concept: Increased lymph flow washes proteins out of the interstitial fluid, lowering interstitial colloid osmotic pressure and reducing capillary filtration, thereby helping prevent edema (safety factor ≈ 7 mm Hg).
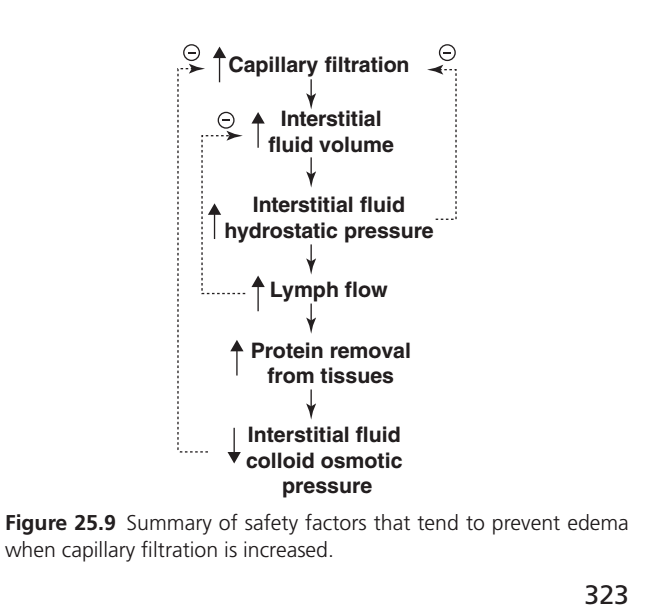
Summary of Safety Factors That Prevent Edema
- When capillary filtration tends to increase, several safety factors help prevent edema.
1. Low Tissue Compliance and Increased Interstitial Fluid Hydrostatic Pressure
- The safety factor caused by low tissue compliance in the negative pressure range is about 3 mm Hg.
2. Increased Lymph Flow
- The safety factor caused by increased lymph flow is about 7 mm Hg.
3. Washdown of Interstitial Proteins
- The safety factor caused by washdown of proteins from the interstitial spaces is about 7 mm Hg.
- This decreases interstitial fluid colloid osmotic pressure.
Total Safety Factor Against Edema
- Total safety factor = 3 mm Hg + 7 mm Hg + 7 mm Hg
- Total safety factor = 17 mm Hg
- Therefore, capillary pressure in peripheral tissues can theoretically increase by about 17 mm Hg before marked edema develops.
- This increase is approximately double the normal capillary pressure.
Key Concept: The total safety factor against edema is about 17 mm Hg, consisting of low tissue compliance (3 mm Hg), increased lymph flow (7 mm Hg), and protein washdown (7 mm Hg), which together help prevent excessive fluid accumulation in tissues.
Fluids in Potential Spaces of the Body
- Potential spaces are spaces in the body that normally contain only a small amount of fluid.
- Examples of potential spaces include:
- Pleural cavity.
- Pericardial cavity.
- Peritoneal cavity.
- Synovial cavities.
- Joint cavities.
- Bursae.
- In these spaces, the surfaces almost touch each other.
- Only a thin layer of fluid is present between the surfaces.
- The surfaces slide over each other during movement.
- A viscous protein-containing fluid lubricates the surfaces.
- This lubrication helps the surfaces slide smoothly over each other.
Fluid Is Exchanged Between Capillaries and Potential Spaces
- The surface membrane of a potential space offers little resistance to the movement of fluids.
- Electrolytes move easily between the potential space and the surrounding interstitial fluid.
- Proteins also move relatively easily between these areas.
- Fluid continuously moves back and forth between the potential space and surrounding tissues.
- Fluid from nearby capillaries diffuses into the interstitial fluid.
- Fluid from nearby capillaries also diffuses into the potential space.
Lymphatic Vessels Drain Protein From the Potential Spaces
- Proteins leak out of capillaries into the potential spaces.
- This process is similar to protein accumulation in the interstitial spaces.
- These proteins must be removed and returned to the circulation.
- Removal occurs through lymphatic vessels or other drainage channels.
- Every potential space is directly or indirectly connected to lymphatic vessels.
- In the pleural cavity, large lymphatic vessels arise directly from the cavity.
- In the peritoneal cavity, large lymphatic vessels also arise directly from the cavity.
Edema Fluid in the Potential Spaces Is Called Effusion
- When edema develops in tissues near a potential space, fluid often accumulates in the potential space as well.
- This fluid accumulation is called effusion.
- Lymphatic blockage can cause effusion.
- Excessive capillary filtration can also cause effusion.
- These mechanisms are similar to those that cause interstitial edema.
- The abdominal cavity is especially prone to fluid accumulation.
- Effusion in the abdominal cavity is called ascites.
- In severe cirrhosis, 20 liters or more of ascitic fluid may accumulate.
- The pleural cavity can become swollen during generalized edema.
- The pericardial cavity can also become swollen during generalized edema.
- Joint spaces may also become swollen during generalized edema.
- Local injury in a cavity may block lymphatic drainage.
- Local infection in a cavity may also block lymphatic drainage.
- Blocked lymphatic drainage can cause isolated swelling of that cavity.
Fluid Pressure in Potential Spaces
- Fluid exchange in the pleural cavity is representative of fluid exchange in other potential spaces.
- In the normal nonedematous state, fluid pressure in most potential spaces is negative.
- This negative pressure is similar to the negative pressure in loose subcutaneous tissue.
- Normal fluid pressure in the pleural cavity is about −7 to −8 mm Hg.
- Normal fluid pressure in joint spaces is about −3 to −5 mm Hg.
- Normal fluid pressure in the pericardial cavity is about −5 to −6 mm Hg.
Key Concept: Potential spaces normally contain a thin lubricating fluid layer. Fluid and proteins move freely between capillaries, interstitial fluid, and these spaces, while lymphatics remove excess protein and fluid. Excess fluid accumulation in a potential space is called effusion, and abdominal effusion is called ascites.
SUMMARY
Edema, Safety Factors Against Edema, and Fluids in Potential Spaces
Edema is the accumulation of excess fluid in the body tissues. It may occur in the intracellular compartment (intracellular edema) or in the extracellular compartment (extracellular edema). Intracellular edema commonly results from hyponatremia, impaired cellular metabolism, or inadequate cellular nutrition. These conditions depress cellular ion pumps, causing sodium to accumulate inside cells and water to enter by osmosis, leading to cell swelling. Inflammation can also increase cell membrane permeability, allowing sodium and water to enter cells and produce intracellular edema.
Extracellular edema occurs when excess fluid accumulates in the interstitial spaces. The two major causes are excessive capillary filtration and impaired lymphatic drainage (lymphedema). Capillary filtration increases when the capillary filtration coefficient increases, capillary hydrostatic pressure rises, plasma colloid osmotic pressure falls, or interstitial colloid osmotic pressure rises.
Lymphedema develops when lymphatic vessels fail to return fluid and proteins from the interstitial space back to the circulation. Protein accumulation in the interstitium increases interstitial colloid osmotic pressure, which attracts additional fluid and worsens edema. Common causes include lymphatic obstruction from infections such as filariasis, cancer, surgery, or congenital lymphatic abnormalities.
Major causes of extracellular edema include increased capillary hydrostatic pressure, decreased plasma proteins, increased capillary permeability, and blockage of lymphatic drainage. Increased hydrostatic pressure may occur in heart failure, kidney disease, venous obstruction, or venous valve failure. Decreased plasma proteins may result from nephrotic syndrome, liver cirrhosis, burns, wounds, or severe malnutrition. Increased capillary permeability can occur with inflammation, infections, toxins, burns, vitamin C deficiency, and prolonged ischemia.
Heart failure is one of the most important causes of edema. Reduced cardiac pumping increases venous and capillary pressures, promoting capillary filtration. Decreased renal perfusion activates the renin-angiotensin-aldosterone system, causing salt and water retention. Increased ADH secretion further promotes water retention. Together, these mechanisms cause generalized edema. Left-sided heart failure may produce pulmonary edema because blood accumulates in the lungs and pulmonary capillary pressure rises.
Kidney diseases that impair sodium and water excretion also cause edema. Retained sodium chloride remains mainly in the extracellular fluid, increasing interstitial fluid volume and blood volume. This leads to extracellular edema and hypertension. Acute glomerulonephritis is a classic example.
Decreased plasma proteins lower plasma colloid osmotic pressure and increase capillary filtration. In nephrotic syndrome, protein loss in urine may exceed protein synthesis, causing severe generalized edema. In liver cirrhosis, reduced albumin production lowers plasma oncotic pressure. Portal hypertension further increases capillary hydrostatic pressure, causing accumulation of fluid in the abdominal cavity known as ascites.
Several important safety factors normally prevent edema. The first is the low compliance of the interstitium when interstitial pressure is negative. Small increases in fluid volume produce relatively large increases in interstitial pressure, which opposes further filtration. This provides a safety factor of approximately 3 mm Hg.
The second safety factor is increased lymph flow. When tissue fluid begins to accumulate, lymph flow can increase 10- to 50-fold, removing excess fluid and proteins from the interstitium. This contributes a safety factor of about 7 mm Hg.
The third safety factor is washdown of interstitial proteins. Increased lymph flow removes proteins from the interstitial fluid, lowering interstitial colloid osmotic pressure and reducing the tendency for fluid to leave the capillaries. This mechanism also provides a safety factor of about 7 mm Hg.
Together, these mechanisms provide a total safety factor against edema of approximately 17 mm Hg. Therefore, capillary pressure can nearly double before significant edema develops.
The interstitial space contains a proteoglycan gel that normally binds most interstitial fluid. This gel prevents free fluid accumulation and restricts fluid movement through tissues. When interstitial pressure becomes positive, free fluid accumulates, tissue compliance increases, and pitting edema develops. Proteoglycan filaments also act as spacers between cells, facilitating nutrient delivery and waste removal while preventing excessive bulk fluid movement through tissues.
Potential spaces of the body include the pleural, pericardial, peritoneal, synovial, joint, and bursal cavities. These spaces normally contain only a thin layer of lubricating proteinaceous fluid that allows adjacent surfaces to slide smoothly over one another. Fluids, electrolytes, and proteins move readily between capillaries, interstitial fluid, and potential spaces. Lymphatic vessels continuously remove excess proteins and fluid from these spaces.
When excess fluid accumulates in a potential space, it is called an effusion. Fluid accumulation in the abdominal cavity is known as ascites. Effusions may result from increased capillary filtration, impaired lymphatic drainage, generalized edema, local infection, or injury. Under normal conditions, fluid pressure within most potential spaces remains negative, helping prevent excessive fluid accumulation.
In summary, edema develops when fluid movement into tissues exceeds the capacity of lymphatic drainage and protective mechanisms. The balance among capillary hydrostatic pressure, plasma colloid osmotic pressure, interstitial forces, lymphatic function, and tissue compliance determines whether fluid remains in the circulation or accumulates in tissues and potential spaces.