LEC # 8 PAGE # 318 GUYTON PHYSIOLOGY 15th Ed:
Plasma Sodium Concentration and Fluid Status
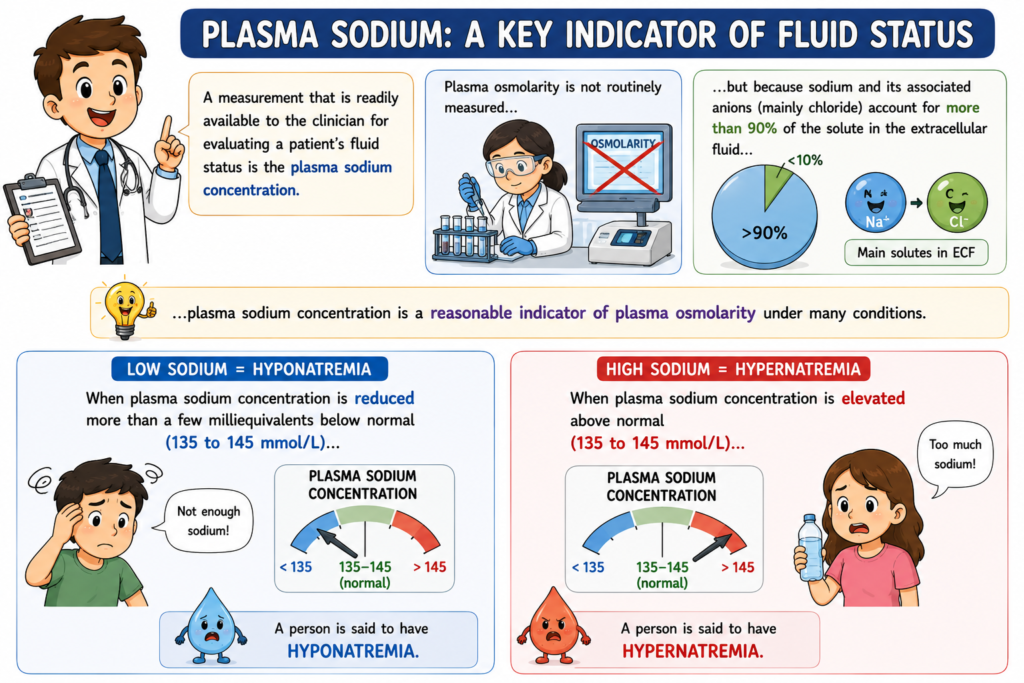
- Plasma sodium concentration is a measurement that is easily available to clinicians.
- It is used to assess a patient’s fluid status.
- Plasma osmolarity is not routinely measured.
- Sodium and its associated anions (mainly chloride) make up more than 90% of the solutes in the extracellular fluid (ECF).
- Therefore, plasma sodium concentration is a useful indicator of plasma osmolarity in many situations.
- Normal plasma sodium concentration is 135–145 mmol/L.
- When plasma sodium concentration falls more than a few milliequivalents below normal, the condition is called hyponatremia.
- Hyponatremia = Low plasma sodium concentration.
- When plasma sodium concentration rises above the normal range, the condition is called hypernatremia.
- Hypernatremia = High plasma sodium concentration.
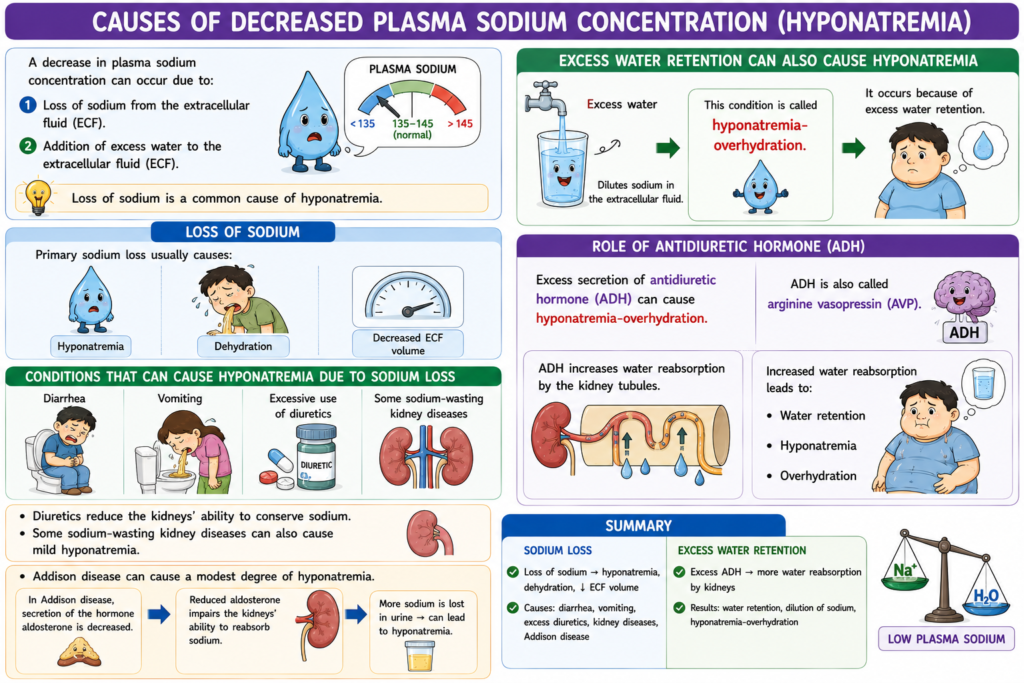
Causes of Hyponatremia: Excess Water or Loss of Sodium (Hyponatremia)
- A decrease in plasma sodium concentration can occur due to:
- Loss of sodium from the extracellular fluid (ECF).
- Addition of excess water to the extracellular fluid (ECF).
- Loss of sodium is a common cause of hyponatremia.
- Primary sodium loss usually causes:
- Hyponatremia.
- Dehydration.
- Decreased extracellular fluid (ECF) volume.
- Conditions that can cause hyponatremia due to sodium loss include:
- Diarrhea.
- Vomiting.
- Excessive use of diuretics can cause hyponatremia.
- Diuretics reduce the kidneys’ ability to conserve sodium.
- Some sodium-wasting kidney diseases can also cause mild hyponatremia.
- Addison disease can cause a modest degree of hyponatremia.
- In Addison disease, secretion of the hormone aldosterone is decreased.
- Reduced aldosterone impairs the kidneys’ ability to reabsorb sodium.
- Hyponatremia can also occur because of excess water retention.
- Excess water dilutes sodium in the extracellular fluid.
- This condition is called hyponatremia-overhydration.
- Excess secretion of antidiuretic hormone (ADH) can cause hyponatremia-overhydration.
- ADH is also called arginine vasopressin (AVP).
- ADH increases water reabsorption by the kidney tubules.
- Increased water reabsorption leads to:
- Water retention.
- Hyponatremia.
- Overhydration.
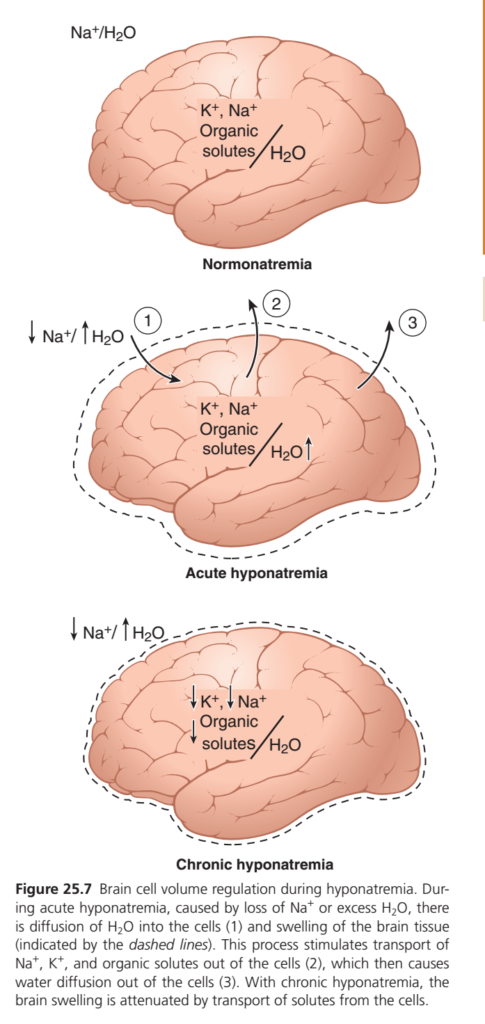
Hyponatremia Causes Cell Edema.Effects of Hyponatremia on Cells and the Brain
- Rapid changes in cell volume due to hyponatremia can seriously affect tissue and organ function.
- The brain is especially sensitive to these changes.
- A rapid decrease in plasma sodium concentration can cause brain cell edema.
- Brain cell edema means swelling of brain cells.
- Rapid hyponatremia can cause neurological symptoms, including:
- Headache.
- Nausea.
- Lethargy.
- Disorientation.
- If plasma sodium concentration rapidly falls below 115–120 mmol/L, severe brain swelling may occur.
- Severe brain swelling can lead to:
- Seizures.
- Coma.
- Permanent brain damage.
- Death.
- The skull is rigid and cannot expand.
- The brain can increase its volume by only about 10% before herniation occurs.
- Herniation means brain tissue is forced into a space where it normally does not belong.
- Brain tissue may be pushed through the foramen magnum.
- The foramen magnum is an opening at the base of the skull.
- The spinal cord connects with the brain through the foramen magnum.
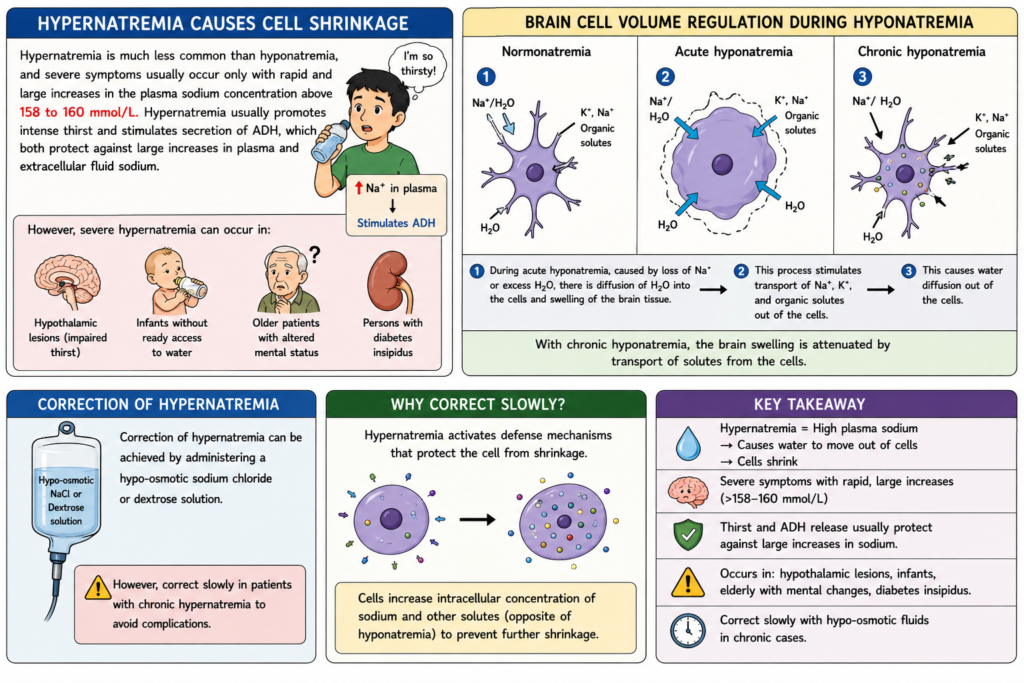
Adaptation to Slowly Developing Hyponatremia
- When hyponatremia develops slowly over several days, the brain and other tissues begin to adapt.
- Cells transport solutes from inside the cell to the extracellular fluid.
- Solutes moved out of the cells include:
- Sodium.
- Chloride.
- Potassium.
- Organic solutes such as glutamate.
- This adaptation reduces the osmotic movement of water into the cells.
- Reduced water entry helps prevent excessive cell swelling.
- As a result, tissue swelling is decreased.
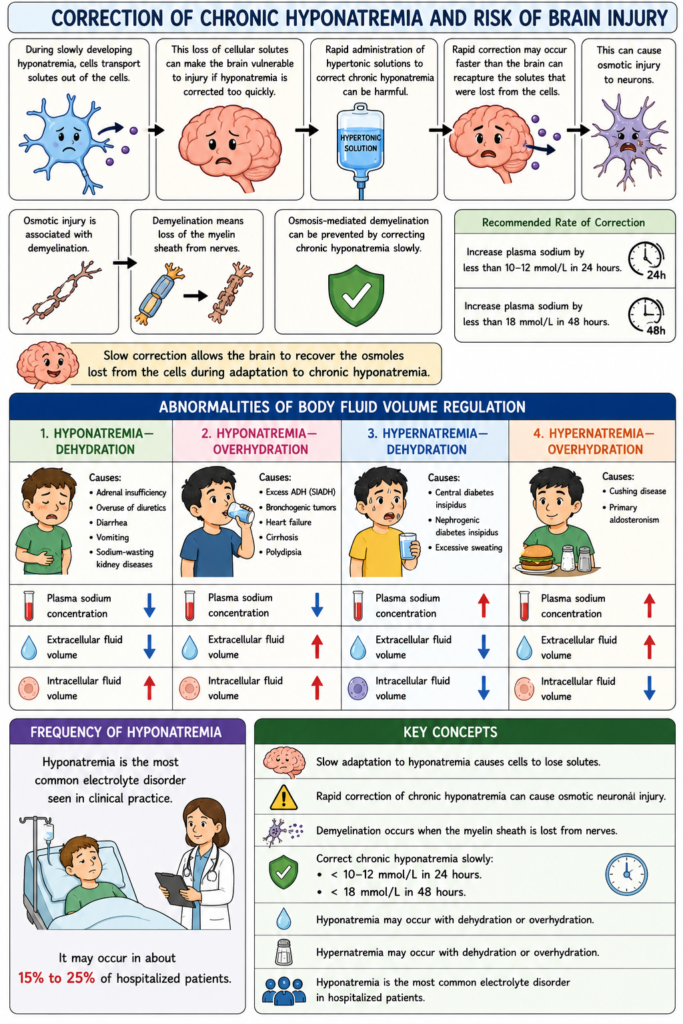
Correction of Chronic Hyponatremia and Risk of Brain Injury
- During slowly developing hyponatremia, cells transport solutes out of the cells.
- This loss of cellular solutes can make the brain vulnerable to injury if hyponatremia is corrected too quickly.
- Rapid administration of hypertonic solutions to correct chronic hyponatremia can be harmful.
- Rapid correction may occur faster than the brain can recapture the solutes that were lost from the cells.
- This can cause osmotic injury to neurons.
- Osmotic injury is associated with demyelination.
- Demyelination means loss of the myelin sheath from nerves.
- Osmosis-mediated demyelination can be prevented by correcting chronic hyponatremia slowly.
- Plasma sodium concentration should be increased by less than 10–12 mmol/L in 24 hours.
- Plasma sodium concentration should be increased by less than 18 mmol/L in 48 hours.
- Slow correction allows the brain to recover the osmoles lost from the cells during adaptation to chronic hyponatremia.
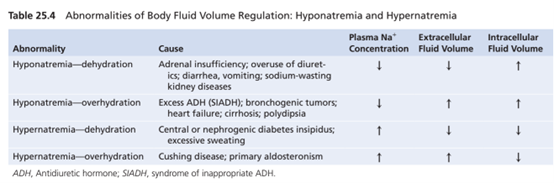
Abnormalities of Body Fluid Volume Regulation
Hyponatremia—Dehydration
- Causes:
- Adrenal insufficiency.
- Overuse of diuretics.
- Diarrhea.
- Vomiting.
- Sodium-wasting kidney diseases.
- Plasma sodium concentration: ↓
- Extracellular fluid volume: ↓
- Intracellular fluid volume: ↑
Hyponatremia—Overhydration
- Causes:
- Excess ADH (SIADH).
- Bronchogenic tumors.
- Heart failure.
- Cirrhosis.
- Polydipsia.
- Plasma sodium concentration: ↓
- Extracellular fluid volume: ↑
- Intracellular fluid volume: ↑
Hypernatremia—Dehydration
- Causes:
- Central diabetes insipidus.
- Nephrogenic diabetes insipidus.
- Excessive sweating.
- Plasma sodium concentration: ↑
- Extracellular fluid volume: ↓
- Intracellular fluid volume: ↓
Hypernatremia—Overhydration
- Causes:
- Cushing disease.
- Primary aldosteronism.
- Plasma sodium concentration: ↑
- Extracellular fluid volume: ↑
- Intracellular fluid volume: ↓
Frequency of Hyponatremia
- Hyponatremia is the most common electrolyte disorder seen in clinical practice.
- It may occur in about 15% to 25% of hospitalized patients.
Key Concepts
- Slow adaptation to hyponatremia causes cells to lose solutes.
- Rapid correction of chronic hyponatremia can cause osmotic neuronal injury.
- Demyelination occurs when the myelin sheath is lost from nerves.
- Correct chronic hyponatremia slowly:
- < 10–12 mmol/L in 24 hours.
- < 18 mmol/L in 48 hours.
- Hyponatremia may occur with dehydration or overhydration.
- Hypernatremia may occur with dehydration or overhydration.
- Hyponatremia is the most common electrolyte disorder in hospitalized patients.
Causes of Hypernatremia: Water Loss or Excess Sodium
- An increase in plasma sodium concentration causes an increase in plasma osmolarity.
- Increased plasma sodium concentration can occur due to:
- Loss of water from the extracellular fluid (ECF).
- Excess sodium in the extracellular fluid (ECF).
- Loss of water from the extracellular fluid concentrates the sodium ions.
- Primary loss of water from the extracellular fluid causes:
- Hypernatremia.
- Dehydration.
- Hypernatremia can occur when the body is unable to secrete ADH.
- ADH is required for the kidneys to conserve water.
- In the absence of ADH, the kidneys excrete large amounts of dilute urine.
- This disorder is called central diabetes insipidus.
- Central diabetes insipidus is also called AVP-deficiency.
- Excessive loss of dilute urine causes:
- Dehydration.
- Increased concentration of sodium chloride in the extracellular fluid.
- In some kidney diseases, the kidneys cannot respond to ADH.
- This condition causes a type of nephrogenic diabetes insipidus.
- Nephrogenic diabetes insipidus is also called AVP-resistance.
- A common cause of hypernatremia with decreased extracellular fluid volume is simple dehydration.
- Simple dehydration occurs when water intake is less than water loss.
- This can happen during prolonged heavy exercise with excessive sweating.
Key Concepts
Simple dehydration occurs when water loss exceeds water intake.
Hypernatremia = Increased plasma sodium concentration.
Hypernatremia increases plasma osmolarity.
Hypernatremia can result from:
Water loss.
Excess sodium.
Water loss from the ECF causes hypernatremia and dehydration.
Lack of ADH causes central diabetes insipidus (AVP-deficiency).
Failure of the kidneys to respond to ADH causes nephrogenic diabetes insipidus (AVP-resistance).
Excessive loss of dilute urine leads to dehydration and hypernatremia.
Hypernatremia Due to Excess Sodium Retention
- Hypernatremia can occur when excessive sodium chloride is added to the extracellular fluid (ECF).
- Excess sodium chloride in the ECF often causes hypernatremia-overhydration.
- Excess sodium chloride retention is usually associated with some degree of water retention by the kidneys.
- Excessive secretion of aldosterone can cause a mild degree of hypernatremia.
- Excessive aldosterone can also cause overhydration.
- Aldosterone is a sodium-retaining hormone.
- Hypernatremia is usually not severe in this condition.
- Sodium retention stimulates the secretion of ADH.
- ADH causes the kidneys to reabsorb greater amounts of water.
- Increased water reabsorption helps limit the rise in plasma sodium concentration.
- The sodium-retaining effects of excess aldosterone are often opposed by compensatory mechanisms.
- One compensatory mechanism is a decrease in other antinatriuretic hormones, such as angiotensin II.
- Another compensatory mechanism is an increase in blood pressure.
- Increased blood pressure causes pressure natriuresis.
Evaluation of Plasma Sodium Abnormalities
- When analyzing abnormalities of plasma sodium concentration, the cause should be identified first.
- Determine whether the abnormality is due to:
- A primary loss of sodium.
- A primary gain of sodium.
- A primary loss of water.
- A primary gain of water.
- Proper therapy depends on identifying the primary cause of the abnormality.
Key Concepts
- Excess sodium chloride in the ECF can cause hypernatremia.
- Excess sodium retention is usually accompanied by water retention.
- Hypernatremia with sodium retention often causes hypernatremia-overhydration.
- Excess aldosterone causes sodium retention, mild hypernatremia, and overhydration.
- Sodium retention stimulates ADH secretion.
- ADH increases water reabsorption by the kidneys.
- Water retention helps prevent severe hypernatremia.
- Compensatory mechanisms include:
- Decreased angiotensin II.
- Increased blood pressure.
- Pressure natriuresis.
- Correct evaluation requires determining whether the primary problem is sodium loss/gain or water loss/gain.
Hypernatremia Causes Cell Shrinkage
Hypernatremia: Clinical Features
- Hypernatremia is much less common than hyponatremia.
- Severe symptoms usually occur only when plasma sodium concentration increases rapidly and markedly.
- Severe symptoms are usually seen when plasma sodium concentration rises above 158–160 mmol/L.
- Hypernatremia usually stimulates intense thirst.
- Hypernatremia also stimulates secretion of ADH.
- Thirst and ADH secretion help protect against large increases in plasma sodium concentration.
- Thirst and ADH secretion also help protect against large increases in extracellular fluid sodium concentration.
- Severe hypernatremia can occur in patients with hypothalamic lesions.
- Hypothalamic lesions may impair the sensation of thirst.
- Severe hypernatremia can occur in infants who may not have easy access to water.
- Severe hypernatremia can occur in older patients with altered mental status.
- Severe hypernatremia can also occur in persons with diabetes insipidus.
Key Concepts
- Hypernatremia is less common than hyponatremia.
- Severe symptoms usually occur with rapid and large increases in plasma sodium concentration.
- Severe symptoms are typically seen when plasma sodium exceeds 158–160 mmol/L.
- Hypernatremia stimulates:
- Intense thirst.
- ADH secretion.
- Thirst and ADH help prevent excessive increases in plasma sodium concentration.
- Severe hypernatremia may occur in:
- Patients with hypothalamic lesions.
- Infants with limited access to water.
- Older patients with altered mental status.
- Persons with diabetes insipidus.
Correction of Hypernatremia
- Hypernatremia can be corrected by administering a hypo-osmotic sodium chloride solution.
- Hypernatremia can also be corrected by administering a dextrose solution.
- Hypernatremia should be corrected slowly in patients with chronic increases in plasma sodium concentration.
- Chronic hypernatremia activates defense mechanisms that protect cells from changes in volume.
- These defense mechanisms help cells adapt to hypernatremia.
- The defense mechanisms in hypernatremia are opposite to those seen in hyponatremia.
- These mechanisms increase the intracellular concentration of sodium.
- These mechanisms also increase the intracellular concentration of other solutes.
Key Concepts
- Hypernatremia can be treated with:
- Hypo-osmotic sodium chloride solution.
- Dextrose solution.
- Chronic hypernatremia should be corrected slowly.
- Hypernatremia activates cellular defense mechanisms.
- These defenses protect cells from volume changes.
- The adaptive response is opposite to that seen in hyponatremia.
- Adaptation increases intracellular sodium and other solutes.