

- Gases move from one place to another by diffusion.
- Diffusion always occurs because of a difference in partial pressure.
- Oxygen (O₂) diffuses from the alveoli into the pulmonary capillary blood because:
- Alveolar PO₂ is higher than pulmonary capillary blood PO₂.
- In the body tissues:
- Capillary blood PO₂ is higher than tissue PO₂.
- Therefore, O₂ diffuses from the blood into the body cells.
- Inside the cells:
- O₂ is used for metabolism.
- This produces carbon dioxide (CO₂).
- As CO₂ is formed:
- Intracellular PCO₂ increases.
- CO₂ diffuses from the cells into the tissue capillaries.
- When the blood reaches the lungs:
- Pulmonary capillary blood PCO₂ is higher than alveolar PCO₂.
- Therefore, CO₂ diffuses from the blood into the alveoli.
- Thus, the transport of O₂ and CO₂ in the body depends on:
- Diffusion
- Blood flow
- The following sections explain these factors in more detail.
KEY CONCEPT
- O₂ always diffuses from a region of higher PO₂ to lower PO₂, while CO₂ diffuses from a region of higher PCO₂ to lower PCO₂. Efficient gas transport depends on both diffusion and continuous blood flow.
DIFFUSION OF OXYGEN FROM ALVEOLI TO PULMONARY CAPILLARY BLOOD
- Oxygen (O₂) diffuses from the alveoli into the pulmonary capillary blood.
- This occurs because alveolar PO₂ is higher than pulmonary capillary blood PO₂.
Fig. 41.1
- Fig. 41.1 shows:
- A pulmonary alveolus next to a pulmonary capillary.
- O₂ diffusing from the alveolus into the blood.
- The average alveolar PO₂ is 104 mm Hg.
- The venous blood entering the pulmonary capillary has a PO₂ of 40 mm Hg.
- This blood has a lower PO₂ because much of its oxygen was used by the body tissues.
- Therefore, the pressure difference driving oxygen diffusion is: 104 − 40 = 64 mm Hg
Easy Concept of the Calculation
- Alveolar PO₂ = 104 mm Hg
- Venous blood PO₂ = 40 mm Hg
Pressure difference:
104 − 40 = 64 mm Hg
- This 64 mm Hg difference is the driving force that pushes oxygen from the alveolus into the blood.
- As blood flows through the pulmonary capillary:
- Oxygen rapidly diffuses into the blood.
- Blood PO₂ increases quickly.
- By the time the blood has traveled about one-third of the capillary length, its PO₂ has almost reached the alveolar PO₂ (104 mm Hg).
KEY CONCEPT
- Oxygen moves from the alveoli to the pulmonary blood because alveolar PO₂ (104 mm Hg) is higher than venous blood PO₂ (40 mm Hg). The 64 mm Hg pressure difference drives rapid diffusion, allowing blood to become almost fully oxygenated within the first one-third of the pulmonary capillary.
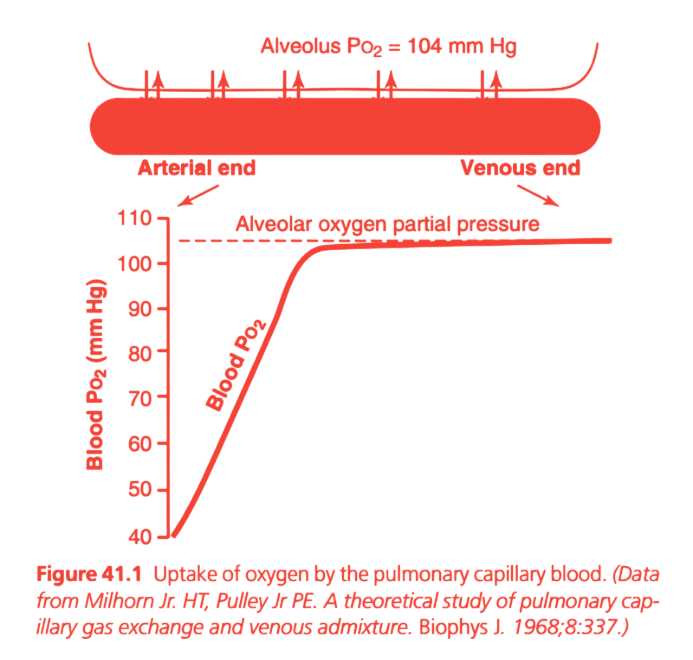
This is Figure 41.1 from Guyton Physiology, and it explains how oxygen moves from the alveoli into the pulmonary capillary blood. This is one of the most important MBBS physiology graphs because it explains why oxygenation is normally completed within the first one-third of the pulmonary capillary.Figure 41.1: Uptake of Oxygen by Pulmonary Capillary Blood
⭐ One-Line Concept
As blood flows through the pulmonary capillary, oxygen diffuses rapidly from the alveolus into the blood until both have the same PO₂ (104 mmHg).
In simple words:
Alveolus has high oxygen → Blood has low oxygen → Oxygen diffuses into blood until both become equal.
PART 1: Upper Diagram
This upper figure shows oxygen diffusion between the alveolus and pulmonary capillary.
Alveolus
PO₂ = 104 mmHg
───────────────────
↓ ↓ ↓ ↓ ↓ ↓
=========================
Pulmonary Capillary
=========================The downward arrows represent
Oxygen moving from the alveolus into the blood.
Why Does Oxygen Move Downward?
Because gases always diffuse
from higher partial pressure to lower partial pressure.
Here,
| Location | PO₂ |
|---|---|
| Alveolus | 104 mmHg |
| Blood entering capillary | 40 mmHg |
Since
104 > 40
oxygen naturally moves
Alveolus → Blood
No pump is required.
This is simple diffusion.
Understanding the Pulmonary Capillary
Notice the long pink tube.
This represents one pulmonary capillary.
Blood enters from one side
↓
Flows through the capillary
↓
Leaves from the other side.
Why Is One End Called “Arterial End”?
This confuses many students.
Remember:
This capillary belongs to the pulmonary circulation, not the systemic circulation.
Blood entering this capillary comes from the pulmonary artery.
Pulmonary arteries carry deoxygenated blood.
Therefore,
The beginning of the pulmonary capillary is called the
Arterial End
because it receives blood from the pulmonary artery.
PO₂ at the Arterial End = 40 mmHg
This blood has just returned from the body.
Body tissues have already used much of its oxygen.
Therefore,
Mixed venous blood has
PO₂ ≈40 mmHg
This is the starting oxygen pressure.
As Blood Flows Forward…
Blood is continuously exposed to alveolar oxygen.
Oxygen keeps diffusing into blood.
Blood PO₂ rises rapidly.
PO₂ at the Venous End = 104 mmHg
By the time blood reaches the end of the capillary,
its PO₂ becomes
104 mmHg
Exactly the same as the alveolus.
Why?
Because diffusion stops when
partial pressures become equal.
No pressure difference
↓
No diffusion.
Very Important Rule
Diffusion does not stop because oxygen disappears.
It stops because
the pressure difference disappears.
PART 2: Lower Graph
Now let’s understand the graph.
X-Axis (Horizontal)
This does NOT represent time directly.
It represents
Position of blood along the pulmonary capillary.
Left side
↓
Blood just entered.
Right side
↓
Blood is leaving.
So moving right means
Blood has traveled farther.
Y-Axis (Vertical)
Blood PO₂ (mmHg)
Shows
Oxygen pressure inside the blood.
Bottom
↓
Little oxygen.
Top
↓
High oxygen.
Why Does the Red Curve Start at 40 mmHg?
Because mixed venous blood enters the lungs with
PO₂ = 40 mmHg
The body tissues have already extracted oxygen.
Therefore,
Blood starts with low oxygen.
Why Does the Red Curve Rise?
Because oxygen is continuously diffusing into blood.
As blood moves along the capillary,
more oxygen enters,
so blood PO₂ increases.
Why Is the Rise So Steep Initially?
Look carefully.
The curve rises very rapidly at the beginning.
Why?
Initially,
Pressure difference is huge.
Alveolus
104 mmHg
Blood
40 mmHg
Difference
64 mmHg
Large pressure difference
↓
Very rapid diffusion.
As Blood Gains Oxygen…
Blood PO₂ rises.
Now
Alveolus
104
Blood
90
Difference
Only 14 mmHg.
Smaller pressure difference
↓
Slower diffusion.
Therefore,
The curve begins to flatten.
Why Does the Curve Become Flat?
Eventually,
Blood PO₂ becomes
104 mmHg.
Now
Alveolus
104
Blood
104
Difference
0
No diffusion.
Therefore,
The curve becomes horizontal.
Dashed Horizontal Line
This line represents
Alveolar PO₂
=
104 mmHg.
Blood PO₂ can never rise above this value while breathing room air.
Because diffusion only continues until both sides are equal.
Why Does Blood Reach 104 mmHg So Early?
This is the most important concept.
Look carefully.
Blood reaches
104 mmHg
within about
the first one-third of the pulmonary capillary.
The remaining two-thirds are called the
Diffusion Reserve (Safety Factor).
What Is Diffusion Reserve?
Normally,
blood remains in the pulmonary capillary for about 0.75 seconds at rest.
However,
oxygenation is completed in only about 0.25 seconds.
That means:
0.75 seconds available
|----0.25 sec----|--------0.50 sec--------|
Oxygenation Reserve
CompleteSo even if blood flows faster, there is still enough time for complete oxygenation.
Why Is This Important During Exercise?
During exercise,
blood moves much faster through the lungs.
Transit time may decrease to about 0.25 seconds.
Even then,
oxygenation is usually still completed because the lungs have a built-in safety reserve.
Clinical Correlation
1. Pulmonary Fibrosis
The respiratory membrane becomes thick.
Oxygen diffuses more slowly.
Blood may not reach 104 mmHg before leaving the capillary.
Result:
Hypoxemia (low arterial oxygen).
2. Pulmonary Edema
Fluid accumulates around alveoli.
Diffusion distance increases.
Oxygen transfer slows.
Again,
blood may leave before becoming fully oxygenated.
3. Exercise
Blood moves faster,
but diffusion capacity also increases because:
- More capillaries open.
- Surface area increases.
Therefore,
oxygenation usually remains complete.
Easy Analogy
Imagine a dry sponge placed in water.
At first:
The sponge absorbs water very quickly because it is very dry.
As it becomes wet,
absorption slows.
Finally,
when fully soaked,
it cannot absorb more water.
Exactly the same happens with blood:
- Blood enters with low PO₂ (40 mmHg) → absorbs oxygen rapidly.
- As blood PO₂ rises, the pressure difference decreases → diffusion slows.
- At 104 mmHg, blood and alveolar PO₂ are equal → diffusion stops.
Step-by-Step Journey of One Red Blood Cell
BODY TISSUES
│
│ Oxygen used by tissues
▼
Mixed Venous Blood
PO₂ = 40 mmHg
│
▼
Pulmonary Capillary Begins
│
▼
Large pressure difference
(104 − 40 = 64 mmHg)
│
▼
Rapid oxygen diffusion
│
▼
Blood PO₂ rises
40 → 60 → 80 → 95 → 104 mmHg
│
▼
Pressure difference becomes zero
│
▼
Blood leaves lung
PO₂ = 104 mmHgHigh-Yield MBBS Viva Points
- Alveolar PO₂ ≈ 104 mmHg.
- Mixed venous blood enters the pulmonary capillary with PO₂ ≈ 40 mmHg.
- Oxygen diffuses from the alveolus to the blood because PO₂ is higher in the alveolus.
- Blood PO₂ reaches 104 mmHg within the first one-third of the pulmonary capillary under normal conditions.
- Diffusion stops when alveolar and blood PO₂ become equal.
- The remaining two-thirds of the capillary provide a diffusion reserve (safety factor), allowing complete oxygenation even during exercise.
Super Easy Memory Trick
Imagine filling an empty bottle from a water tap:
- 🚰 Tap = Alveolus (PO₂ = 104 mmHg).
- 🍼 Bottle = Blood entering with PO₂ = 40 mmHg.
At first, the bottle fills very quickly because it is almost empty.
As the bottle becomes full, filling slows down.
When the bottle is completely full, no more water enters.
Likewise:
- Low blood PO₂ (40 mmHg) → rapid oxygen diffusion.
- Blood PO₂ rises → diffusion gradually slows.
- Blood PO₂ reaches 104 mmHg → no pressure difference remains, so oxygen diffusion stops.
Key MBBS takeaway: The lungs are so efficient that blood becomes fully oxygenated in only the first one-third of the pulmonary capillary, leaving a two-thirds diffusion reserve that protects oxygenation during exercise and mild lung stress.
Uptake of Oxygen By the Pulmonary Blood During Exercise
- During strenuous exercise, the body may need up to 20 times more oxygen than at rest.
- During exercise, cardiac output increases.
- Because blood flows faster, it remains in the pulmonary capillaries for less than half the normal time.
- Even with this shorter time, the blood still becomes almost fully saturated with oxygen before leaving the pulmonary capillaries.
- This happens for two main reasons:
- The diffusing capacity for O₂ increases about 3 times during exercise.
- More pulmonary capillaries open and participate in gas exchange.
- The surface area available for oxygen diffusion increases.
- The ventilation-perfusion (V̇A/Q̇) ratio becomes closer to ideal, especially in the upper lungs.
- Under resting conditions, oxygenation is completed very early.
- As shown in Fig. 41.1, blood becomes almost fully oxygenated after passing through about one-third of the pulmonary capillary.
- During the remaining two-thirds of the capillary, very little additional oxygen enters the blood.
- Therefore, at rest, blood stays in the pulmonary capillaries about three times longer than needed for full oxygenation.
- During exercise, although blood spends less time in the capillaries, it is still oxygenated almost completely.
Fig. 41.1
- Fig. 41.1 shows that:
- Blood PO₂ rises rapidly as it flows through the pulmonary capillary.
- Blood becomes almost fully oxygenated within the first one-third of the capillary.
- The remaining two-thirds provide a large safety margin for oxygen uptake.
KEY CONCEPT
- During exercise, blood flows faster through the lungs, but oxygenation remains almost complete because the lung diffusing capacity increases about threefold and blood normally becomes fully oxygenated within the first one-third of the pulmonary capillary. This provides a large safety factor for oxygen uptake.
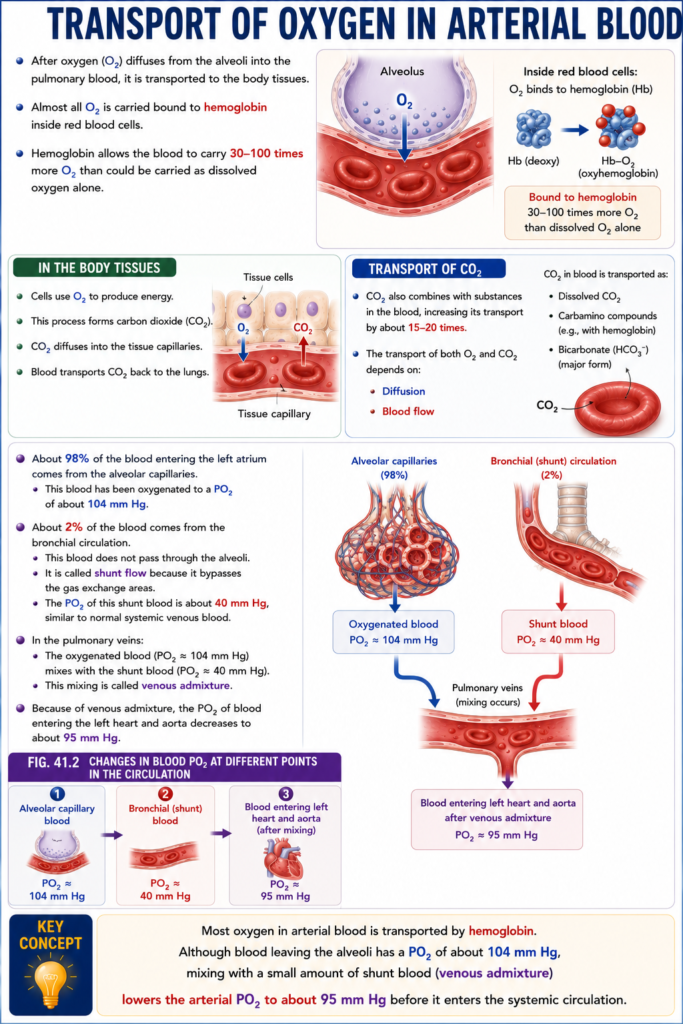
TRANSPORT OF OXYGEN IN ARTERIAL BLOOD
- After oxygen (O₂) diffuses from the alveoli into the pulmonary blood, it is transported to the body tissues.
- Almost all O₂ is carried bound to hemoglobin inside red blood cells.
- Hemoglobin allows the blood to carry 30–100 times more O₂ than could be carried as dissolved oxygen alone.
- In the body tissues:
- Cells use O₂ to produce energy.
- This process forms carbon dioxide (CO₂).
- CO₂ diffuses into the tissue capillaries.
- Blood transports CO₂ back to the lungs.
- CO₂ also combines with substances in the blood, increasing its transport by about 15–20 times.
- The transport of both O₂ and CO₂ depends on:
- Diffusion
- Blood flow
- About 98% of the blood entering the left atrium comes from the alveolar capillaries.
- This blood has been oxygenated to a PO₂ of about 104 mm Hg.
- About 2% of the blood comes from the bronchial circulation.
- This blood does not pass through the alveoli.
- It is called shunt flow because it bypasses the gas exchange areas.
- The PO₂ of this shunt blood is about 40 mm Hg, similar to normal systemic venous blood.
- In the pulmonary veins:
- The oxygenated blood (PO₂ ≈ 104 mm Hg) mixes with the shunt blood (PO₂ ≈ 40 mm Hg).
- This mixing is called venous admixture.
- Because of venous admixture, the PO₂ of blood entering the left heart and aorta decreases to about 95 mm Hg.
Fig. 41.2
- Fig. 41.2 shows the changes in blood PO₂ at different points in the circulation:
- Alveolar capillary blood: 104 mm Hg
- Bronchial (shunt) blood: 40 mm Hg
- Blood entering the left heart and aorta after mixing: 95 mm Hg
KEY CONCEPT
- Most oxygen in arterial blood is transported by hemoglobin. Although blood leaving the alveoli has a PO₂ of about 104 mm Hg, mixing with a small amount of shunt blood (venous admixture) lowers the arterial PO₂ to about 95 mm Hg before it enters the systemic circulation.
This is Figure 41.2 from Guyton Physiology, and it explains the complete journey of oxygen (PO₂) in the blood as it circulates through the lungs → arteries → tissues → veins → lungs again.
It also explains an extremely important concept:
Why is arterial PO₂ about 95 mmHg instead of 104 mmHg, even though blood leaves the pulmonary capillary with a PO₂ of 104 mmHg?
The answer is physiological shunt (venous admixture).
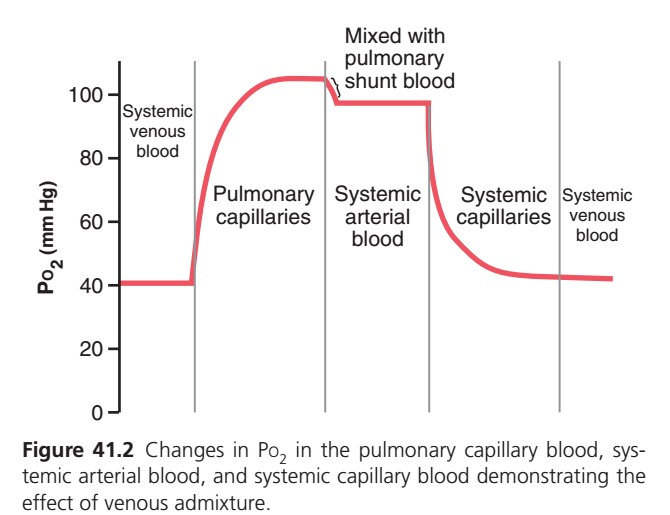
Figure 41.2: Changes in PO₂ During One Complete Circulation
⭐ One-Line Concept
Blood starts with low PO₂ (40 mmHg), becomes oxygenated in the lungs (104 mmHg), slightly decreases to about 95 mmHg after mixing with shunt blood, then loses oxygen in the tissues and returns to 40 mmHg.
This is one complete oxygen cycle.
Step 1: Understand the Axes
Y-Axis (Vertical)
PO₂ (mmHg)
This represents
Partial pressure of oxygen in the blood.
Higher value
↓
More oxygen
Lower value
↓
Less oxygen
X-Axis (Horizontal)
The X-axis does NOT represent time.
Instead, it represents different parts of the circulation.
From left to right:
Systemic veins
↓
Pulmonary capillaries
↓
Systemic arteries
↓
Systemic capillaries
↓
Systemic veins againThe graph follows one drop of blood as it travels around the body.
Region 1: Systemic Venous Blood
(Left side)
Look at the graph.
PO₂
=
40 mmHg
Why Is It 40 mmHg?
This blood has just returned from the tissues.
The tissues have used oxygen for metabolism.
Therefore,
Blood contains much less oxygen.
This blood is called
Mixed venous blood.
Easy Analogy
Imagine a delivery truck.
It started with many oxygen cylinders.
After delivering oxygen to hospitals (body tissues),
only a few cylinders remain.
This is venous blood.
Region 2: Pulmonary Capillaries
Now blood enters the lungs.
Look at the curve.
It rises rapidly.
Why Does It Rise?
Because
Alveolar PO₂
=
104 mmHg
Blood PO₂
=
40 mmHg
Large pressure difference
↓
Rapid oxygen diffusion.
Blood quickly gains oxygen.
Why Does the Curve Flatten?
Eventually,
Blood PO₂ reaches
104 mmHg.
Now
Blood PO₂
=
Alveolar PO₂
No pressure difference remains.
Diffusion stops.
Important Point
Blood becomes fully oxygenated
before leaving the pulmonary capillary.
Region 3: “Mixed with Pulmonary Shunt Blood”
This is the most important part of the graph.
Notice something unusual.
Blood PO₂ suddenly drops.
From
104
↓
About
95 mmHg.
Question
Why did oxygen decrease?
Did the lungs remove oxygen?
❌ No.
The lungs added oxygen.
The decrease occurs after leaving the lungs.
The Reason
Some blood bypasses the alveoli.
This blood remains deoxygenated.
Later,
It mixes with oxygenated blood.
This is called
Venous admixture
or
Physiological shunt.
What Is Pulmonary Shunt Blood?
Not every drop of blood passes through ventilated alveoli.
Some blood comes from:
Bronchial circulation
These veins drain directly into the pulmonary veins.
Their blood has lower PO₂.
Small Thebesian veins
These veins drain directly into the left side of the heart.
Again,
They contain less oxygen.
When these small amounts of deoxygenated blood mix with fully oxygenated blood,
arterial PO₂ falls slightly.
Therefore
Pulmonary capillary blood
↓
104 mmHg
After mixing
↓
Systemic arterial blood
↓
≈95 mmHg
Easy Analogy
Imagine
100 glasses contain pure juice.
Now add
2 glasses of plain water.
The juice becomes slightly diluted.
Exactly the same.
Oxygenated blood
Small amount of deoxygenated blood
↓
Slightly lower PO₂.
Region 4: Systemic Arterial Blood
Now blood travels through arteries.
PO₂
≈95 mmHg.
This is the blood supplying every organ.
Why Not 104 mmHg?
Because of
Physiological shunt.
This is an extremely common MBBS viva question.
Region 5: Systemic Capillaries
Now blood reaches tissues.
Observe the graph.
PO₂ falls steeply.
Why?
Cells continuously consume oxygen.
They use oxygen for ATP production.
Therefore,
Oxygen diffuses
Blood
↓
Tissues.
Blood gradually loses oxygen.
What Happens?
Blood PO₂ decreases
95
↓
80
↓
60
↓
50
↓
40 mmHg.
Why Does the Curve Become Flat Again?
Eventually,
Blood leaves the tissues.
Mixed venous blood now has
PO₂
≈40 mmHg.
This completes one circulation.
Complete Journey of One Red Blood Cell
BODY TISSUES
PO₂ = 40 mmHg
│
▼
Pulmonary Artery
│
▼
Pulmonary Capillary
40 → 60 → 80 → 104 mmHg
│
▼
Pulmonary Vein
104 mmHg
│
▼
Mixes with Physiological Shunt Blood
│
▼
Systemic Artery
≈95 mmHg
│
▼
Body Tissues
95 → 70 → 50 → 40 mmHg
│
▼
Systemic Veins
40 mmHgWhy Doesn’t Arterial PO₂ Stay at 104 mmHg?
This is one of the highest-yield questions.
The lungs oxygenate blood perfectly to 104 mmHg.
However,
before reaching the body,
this blood mixes with a small amount of deoxygenated blood.
This physiological shunt lowers arterial PO₂ to about 95 mmHg.
Clinical Correlation
1. Physiological Shunt
Normally,
2–5% of cardiac output bypasses alveolar gas exchange.
This causes the normal difference between:
- Pulmonary capillary PO₂ = 104 mmHg
- Systemic arterial PO₂ ≈95 mmHg
This difference contributes to the normal alveolar–arterial (A–a) oxygen gradient.
2. Right-to-Left Cardiac Shunt
Examples:
- Tetralogy of Fallot
- Eisenmenger syndrome
Much more deoxygenated blood enters systemic circulation.
Arterial PO₂ falls markedly.
3. Pneumonia
Some alveoli are filled with fluid.
Blood passes them without adequate oxygenation.
This increases shunt,
causing hypoxemia.
High-Yield MBBS Viva Points
| Location | PO₂ |
|---|---|
| Mixed venous blood | 40 mmHg |
| Alveolar air | 104 mmHg |
| Pulmonary capillary blood (end-capillary) | 104 mmHg |
| Systemic arterial blood | ≈95 mmHg |
| Systemic venous blood | 40 mmHg |
Summary of Every Region
| Region | What Happens? | PO₂ Change | Reason |
|---|---|---|---|
| Systemic venous blood | Blood returns from tissues | 40 mmHg | Oxygen has been used by tissues |
| Pulmonary capillaries | Oxygen diffuses into blood | 40 → 104 mmHg | Alveolar PO₂ is higher than blood PO₂ |
| Pulmonary shunt mixing | Small amount of deoxygenated blood mixes with oxygenated blood | 104 → ≈95 mmHg | Physiological shunt (venous admixture) |
| Systemic arterial blood | Oxygen-rich blood travels to organs | ≈95 mmHg | Blood after shunt mixing |
| Systemic capillaries | Oxygen diffuses into tissues | 95 → 40 mmHg | Cellular oxygen consumption |
Super Easy Memory Story
Imagine a delivery truck carrying oxygen cylinders:
🚚 Step 1: Returning from the city (Systemic venous blood)
The truck has delivered most of its cylinders.
➡️ PO₂ = 40 mmHg
🏭 Step 2: Oxygen factory (Pulmonary capillaries)
The truck is refilled completely.
➡️ PO₂ = 104 mmHg
🚰 Step 3: Small dilution (Physiological shunt)
Before leaving, a small amount of water is mixed with the load.
The load is still almost full, but slightly diluted.
➡️ PO₂ falls to ≈95 mmHg
🏘️ Step 4: Delivering to the body (Systemic capillaries)
The truck delivers oxygen to tissues.
Its oxygen supply gradually decreases.
➡️ PO₂ falls from 95 → 40 mmHg
🔁 Step 5: Returns to the factory
The truck reaches the lungs nearly empty again.
The cycle repeats.
MBBS Golden Rule
- Mixed venous blood enters the lungs with PO₂ ≈ 40 mmHg.
- Pulmonary capillary blood becomes fully oxygenated to PO₂ ≈ 104 mmHg.
- After mixing with physiological shunt blood, systemic arterial PO₂ becomes ≈ 95 mmHg.
- As blood passes through systemic tissues, oxygen diffuses into cells, and PO₂ falls back to ≈ 40 mmHg.
This single graph summarizes the entire oxygen journey through the body, from deoxygenated venous blood to oxygenated arterial blood and back again.
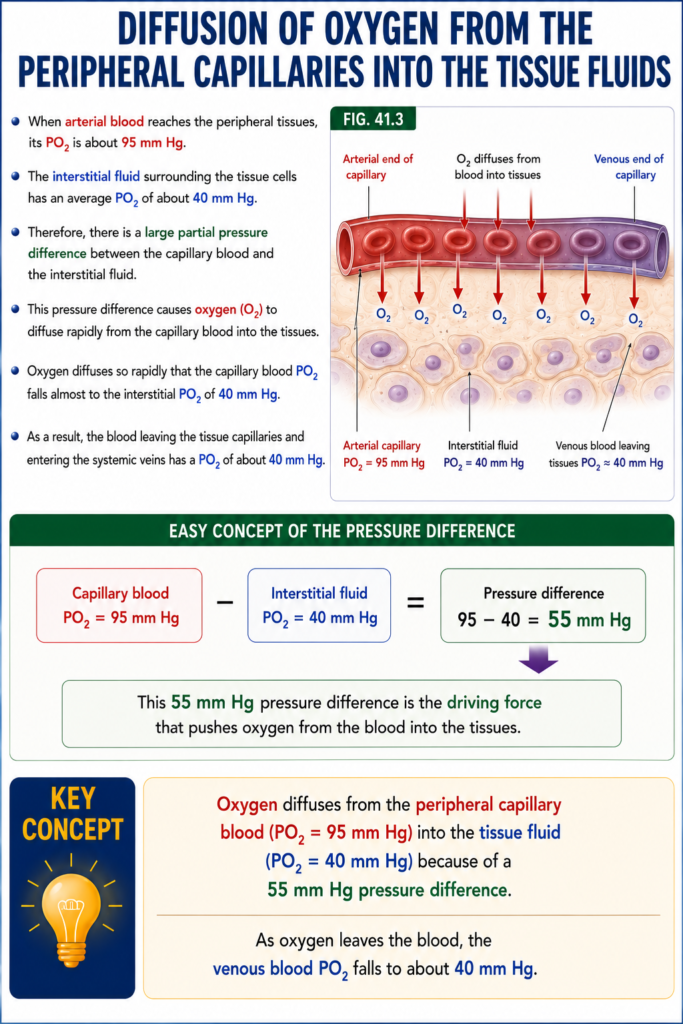
DIFFUSION OF OXYGEN FROM THE PERIPHERAL CAPILLARIES INTO THE TISSUE FLUIDS
- When arterial blood reaches the peripheral tissues, its PO₂ is about 95 mm Hg.
- The interstitial fluid surrounding the tissue cells has an average PO₂ of about 40 mm Hg.
- Therefore, there is a large partial pressure difference between the capillary blood and the interstitial fluid.
- This pressure difference causes oxygen (O₂) to diffuse rapidly from the capillary blood into the tissues.
- Oxygen diffuses so rapidly that the capillary blood PO₂ falls almost to the interstitial PO₂ of 40 mm Hg.
- As a result, the blood leaving the tissue capillaries and entering the systemic veins has a PO₂ of about 40 mm Hg.
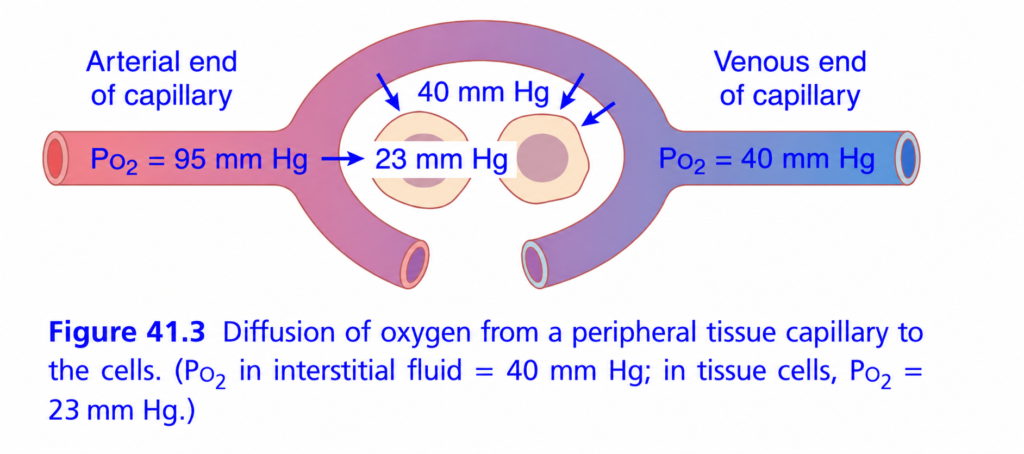
Fig. 41.3
- Fig. 41.3 shows:
- Arterial capillary PO₂ = 95 mm Hg
- Interstitial fluid PO₂ = 40 mm Hg
- O₂ diffusing from the blood into the tissues
- Venous blood leaving the tissues with a PO₂ of about 40 mm Hg
Easy Concept of the Pressure Difference
- Capillary blood PO₂ = 95 mm Hg
- Interstitial fluid PO₂ = 40 mm Hg
Pressure difference:
95 − 40 = 55 mm Hg
- This 55 mm Hg pressure difference is the driving force that pushes oxygen from the blood into the tissues.
KEY CONCEPT
- Oxygen diffuses from the peripheral capillary blood (PO₂ = 95 mm Hg) into the tissue fluid (PO₂ = 40 mm Hg) because of a 55 mm Hg pressure difference. As oxygen leaves the blood, the venous
- blood PO₂ falls to about 40 mm Hg.
Diffusion of Oxygen from Blood to Body Cells (Guyton Fig. 41.3) – Easiest Concept for MBBS Students
🎯 One-Line Concept
Oxygen always moves from HIGH partial pressure (PO₂) → LOW partial pressure (PO₂).
Think of oxygen like water flowing downhill.
It naturally moves from an area where it is more concentrated to an area where it is less concentrated.
Step 1: Arterial Blood Arrives (Rich in Oxygen)
🔴 Arterial end of capillary
PO₂ = 95 mm Hg
This blood has just come from the lungs, so it contains plenty of oxygen.
Blood
PO₂ = 95 mm Hg👉 Oxygen is “loaded” and ready to deliver to tissues.
Step 2: Interstitial Fluid Has Less Oxygen
Around every body cell is interstitial fluid.
Its oxygen pressure is only:
PO₂ = 40 mm Hg
Blood = 95
Interstitial fluid = 40Difference:
95 → 40
Because oxygen always moves from high → low pressure, oxygen leaves the blood.
➡ Blood → Interstitial fluid
Step 3: Body Cells Have Even Less Oxygen
Inside tissue cells,
PO₂ = 23 mm Hg
Interstitial fluid = 40
Cell = 23Again,
40 → 23
Oxygen moves into the cells.
➡ Interstitial fluid → Cell
Step 4: Why Is Cell PO₂ So Low?
Because cells are constantly using oxygen to make ATP (energy).
As oxygen is consumed,
PO₂ remains low.
This continuously pulls more oxygen into the cell.
Think of it as:
Cells are continuously “burning” oxygen, so they never become full of oxygen.
The Complete Oxygen Journey
Lungs
↓
Arterial Blood
PO₂ = 95
↓
Interstitial Fluid
PO₂ = 40
↓
Body Cell
PO₂ = 23
↓
Mitochondria
(Oxygen used to produce ATP)Why Does Venous Blood Have Only 40 mm Hg?
Initially,
Blood PO₂ = 95 mm Hg
As oxygen leaves the blood,
95
↓
80
↓
65
↓
50
↓
40By the time blood reaches the venous end of the capillary,
its PO₂ becomes
40 mm Hg
This is why the figure shows:
🔵 Venous blood = PO₂ 40 mm Hg
Easy Memory Trick
95 → 40 → 23
- 95 = Arterial blood
- 40 = Interstitial fluid (and venous blood)
- 23 = Tissue cells
👉 Oxygen always moves:
95 → 40 → 23
Never the opposite.
Everyday Analogy
Imagine three water tanks connected together.
Tank A = Full (95)
Tank B = Half Full (40)
Tank C = Almost Empty (23)Water naturally flows
Tank A
↓
Tank B
↓
Tank COxygen behaves exactly the same way.
Why Is This Gradient Important?
Without this pressure difference:
- ❌ Oxygen would not leave the blood.
- ❌ Cells would not receive oxygen.
- ❌ ATP production would stop.
- ❌ Cells would die.
The PO₂ gradient is therefore the driving force for oxygen delivery to tissues.
MBBS Exam Concept
Question: Why does oxygen diffuse from blood into tissues?
Answer:
Because arterial blood has a higher PO₂ (95 mm Hg) than interstitial fluid (40 mm Hg) and tissue cells (23 mm Hg). Oxygen always diffuses from higher partial pressure to lower partial pressure, so it moves from blood → interstitial fluid → tissue cells.
⭐ Super Memory Summary
Arterial Blood
PO₂ = 95 mm Hg
↓
(High → Low)
↓
Interstitial Fluid
PO₂ = 40 mm Hg
↓
(High → Low)
↓
Tissue Cells
PO₂ = 23 mm Hg
↓
O₂ used to make ATP
↓
Venous Blood leaves with
PO₂ = 40 mm HgGolden Rule
Oxygen always diffuses from HIGH PO₂ to LOW PO₂.
Mnemonic: “95 → 40 → 23” = Blood → Tissue Fluid → Cell
Increasing Blood Flow Raises Interstitial Fluid PO₂
- If blood flow to a tissue increases, more oxygen (O₂) is delivered to that tissue.
- As a result, the interstitial fluid PO₂ increases.
- Fig. 41.4 shows this effect.
- When blood flow increases to 400% of normal:
- Interstitial PO₂ rises from 40 mm Hg (Point A) to 66 mm Hg (Point B).
- Even with the maximum blood flow, interstitial PO₂ cannot rise above 95 mm Hg.
- This is because 95 mm Hg is the PO₂ of arterial blood.
- If blood flow decreases, the interstitial PO₂ also decreases, as shown at Point C.
Increasing Tissue Metabolism Decreases Interstitial Fluid PO₂
- If tissue cells use more oxygen for metabolism, the interstitial PO₂ decreases.
- Fig. 41.4 shows that:
- Higher oxygen consumption lowers interstitial PO₂.
- Lower oxygen consumption raises interstitial PO₂.
- Therefore, interstitial PO₂ depends on the balance between:
- The amount of oxygen delivered by the blood
- The amount of oxygen used by the tissues
Fig. 41.4
- Point A: Normal blood flow → Interstitial PO₂ = 40 mm Hg
- Point B: Blood flow = 400% of normal → Interstitial PO₂ = 66 mm Hg
- Maximum possible interstitial PO₂ = 95 mm Hg (equal to arterial PO₂)
- Point C: Reduced blood flow → Lower interstitial PO₂
KEY CONCEPT
- More blood flow delivers more oxygen and raises interstitial PO₂, while increased tissue metabolism uses more oxygen and lowers interstitial PO₂. Tissue PO₂ is determined by the balance between oxygen delivery and oxygen consumption.
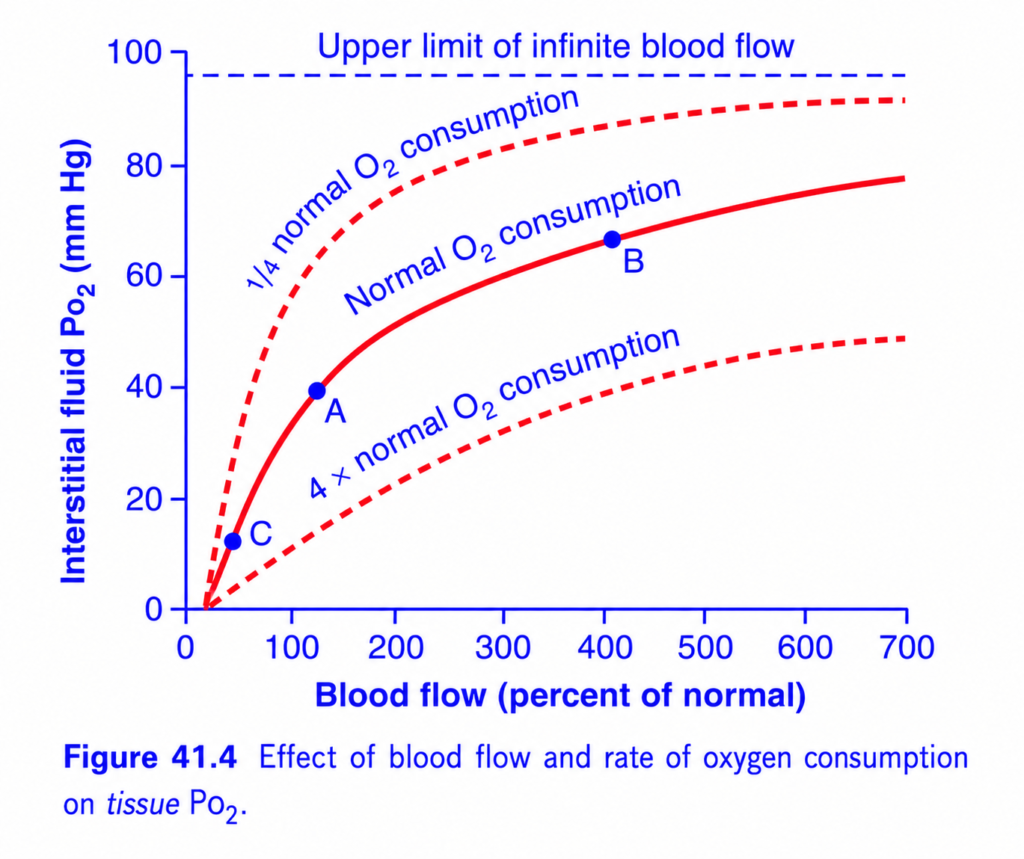
This is Figure 41.4 from Guyton Physiology, and it explains how tissue oxygen (interstitial PO₂) changes when blood flow or oxygen consumption changes.
This is one of the most important physiology graphs because it explains why tissues become hypoxic when blood flow decreases or oxygen consumption increases.
Figure 41.4: Effect of Blood Flow and Oxygen Consumption on Tissue PO₂
⭐ One-Line Concept
Tissue (interstitial) PO₂ depends on the balance between oxygen delivery (blood flow) and oxygen use (oxygen consumption).
- ↑ Blood flow → ↑ Tissue PO₂
- ↓ Blood flow → ↓ Tissue PO₂
- ↑ Oxygen consumption → ↓ Tissue PO₂
- ↓ Oxygen consumption → ↑ Tissue PO₂
Think of it as:
Tissue PO₂
=
Oxygen Supply (Blood Flow)
-
Oxygen Demand (Consumption)Step 1: Understand the Axes
X-Axis (Horizontal)
Blood Flow (% of Normal)
This shows how much blood reaches the tissue.
- 0% = No blood flow
- 100% = Normal blood flow
- 400% = Four times normal blood flow
- 700% = Seven times normal blood flow
👉 Moving to the right means more oxygen delivery.
Y-Axis (Vertical)
Interstitial PO₂ (mmHg)
This is oxygen pressure in the tissue fluid around the cells.
It is not blood PO₂.
Think of it as the oxygen available to tissue cells.
Higher PO₂ = More oxygen available.
Lower PO₂ = Less oxygen available.
What Are the Three Curves?
The graph shows three different oxygen consumption rates.
🔺 Upper Dashed Curve
¼ Normal Oxygen Consumption
The tissue uses very little oxygen.
Examples:
What Happens?
Blood delivers oxygen faster than the tissue uses it.
Therefore,
interstitial PO₂ becomes high.
Example
At normal blood flow (100%),
Tissue PO₂ is about
60 mmHg
instead of 40 mmHg.
Easy Memory
Small oxygen use
↓
Lots of oxygen remains
↓
High tissue PO₂
🔴 Middle Solid Curve
Normal Oxygen Consumption
This is the normal resting condition.
The tissue uses oxygen at the normal rate.
Point A
Look at Point A.
Blood flow
=
100% (Normal)
Tissue PO₂
≈40 mmHg
This is the normal operating point.
Meaning of Point A
Normal blood flow
Normal oxygen use
=
Normal tissue PO₂
≈40 mmHg
This is the normal value found in most tissues.
Point B
Now move to the right.
Blood flow increases to about 400%.
Tissue PO₂ rises to about 65–70 mmHg.
Why?
More blood arrives.
More oxygen is delivered.
The tissue still consumes oxygen at the same rate.
Therefore,
more oxygen remains in the interstitial fluid.
Easy Analogy
Imagine delivering water to a village.
If:
- 10 tankers arrive
- The village uses only 5
Water accumulates.
Exactly the same.
More blood
↓
More oxygen delivery
↓
Higher tissue PO₂.
🔻 Lower Dashed Curve
Four Times Normal Oxygen Consumption
Now the tissue is using oxygen four times faster.
Examples
- Heavy exercise
- Contracting skeletal muscle
- Severe fever
- Hyperthyroidism
What Happens?
Blood delivers oxygen,
but the cells consume it very rapidly.
Therefore,
very little oxygen remains in the tissue fluid.
Interstitial PO₂ becomes low.
Example
At normal blood flow (100%),
PO₂ is only about
10–15 mmHg.
Easy Memory
Very high oxygen use
↓
Oxygen disappears quickly
↓
Low tissue PO₂
Understanding Point C
Look at Point C.
Blood flow is very low.
Interstitital PO₂ is only about 10 mmHg.
Why?
Very little blood reaches the tissue.
Very little oxygen is delivered.
Cells continue consuming oxygen.
Therefore,
oxygen pressure falls sharply.
Clinical Examples
- Shock
- Arterial blockage
- Severe hypotension
- Ischemia
All produce
↓
Low tissue PO₂.
Why Do All Curves Rise?
As blood flow increases,
more oxygen reaches the tissue.
Therefore,
interstitial PO₂ increases.
Simple.
Why Do the Curves Flatten?
Look carefully.
Initially,
Increasing blood flow causes a large rise in tissue PO₂.
Later,
Further increases produce only small changes.
Why?
Because tissue PO₂ cannot exceed arterial oxygen pressure.
Eventually,
oxygen delivery reaches its maximum useful limit.
Dashed Horizontal Line
Upper Limit of Infinite Blood Flow
This line is around
95 mmHg.
Why 95 mmHg?
Arterial blood entering tissues has
PO₂ ≈95 mmHg.
Even with infinite blood flow,
tissue PO₂ can never exceed arterial PO₂.
Because oxygen always diffuses
Blood
↓
Tissues.
Never the opposite.
Compare All Three Curves
| Curve | Oxygen Consumption | Tissue PO₂ |
|---|---|---|
| Upper dashed | ¼ normal | Highest |
| Middle solid | Normal | Intermediate |
| Lower dashed | 4× normal | Lowest |
Understanding Every Point
Point A
Blood Flow
100%
Oxygen Consumption
Normal
↓
Tissue PO₂
≈40 mmHg
Normal tissue.
Point B
Blood Flow
400%
Oxygen Consumption
Normal
↓
Tissue PO₂
≈67 mmHg
Excellent oxygen supply.
Point C
Blood Flow
Very low
Oxygen Consumption
Normal
↓
Tissue PO₂
≈10 mmHg
Severe hypoxia.
Easy Daily-Life Analogy
Imagine a city receiving food.
Blood Flow
=
Food trucks.
Oxygen
=
Food.
Cells
=
People eating.
Situation 1
Many trucks
Few people eating
↓
Food accumulates.
High tissue PO₂.
Situation 2
Normal trucks
Normal eating
↓
Balanced.
Normal tissue PO₂.
Situation 3
Few trucks
Many hungry people
↓
Food disappears quickly.
Very little remains.
Low tissue PO₂.
Exactly like oxygen.
Clinical Correlation
1. Exercise
Muscles consume much more oxygen.
If blood flow does not increase enough,
tissue PO₂ falls.
This contributes to fatigue.
2. Shock
Blood flow decreases.
Even normal oxygen consumption can quickly lower tissue PO₂.
This leads to tissue hypoxia and organ dysfunction.
3. Hyperthyroidism
Cells consume oxygen rapidly.
Unless blood flow increases,
interstitial PO₂ decreases.
4. Reactive Hyperemia
After temporary ischemia,
blood flow increases several-fold.
Tissue PO₂ rapidly rises toward normal.
High-Yield MBBS Viva Points
- Normal interstitial PO₂ ≈40 mmHg (Point A).
- Increasing blood flow raises tissue PO₂.
- Increasing oxygen consumption lowers tissue PO₂.
- Maximum tissue PO₂ cannot exceed arterial PO₂ (~95 mmHg).
- Low blood flow or high oxygen consumption can both produce tissue hypoxia.
Super Easy Memory Trick
Imagine a classroom:
- 🚚 Blood flow = Students bringing lunch boxes (oxygen).
- 🍽️ Cells = Hungry children eating the lunch (oxygen consumption).
- 📦 Lunch boxes left in the room = Interstitial PO₂.
Three situations:
- ¼ Normal oxygen consumption (Upper dashed curve): Children eat very little → Many lunch boxes remain → High tissue PO₂.
- Normal oxygen consumption (Middle curve): Eating and delivery are balanced → Normal tissue PO₂ (~40 mmHg at Point A).
- 4× Normal oxygen consumption (Lower dashed curve): Children eat much faster than lunch arrives → Very few lunch boxes remain → Low tissue PO₂.
🎯 MBBS Golden Rule
| Change | Effect on Tissue PO₂ |
|---|---|
| ↑ Blood Flow | ↑ Tissue PO₂ |
| ↓ Blood Flow | ↓ Tissue PO₂ |
| ↑ Oxygen Consumption | ↓ Tissue PO₂ |
| ↓ Oxygen Consumption | ↑ Tissue PO₂ |
Remember this balance:
Tissue oxygen depends on how much oxygen is delivered by the blood versus how much oxygen is consumed by the cells. This is the central message of Figure 41.4.
DIFFUSION OF OXYGEN FROM PERIPHERAL CAPILLARIES TO TISSUE CELLS
- Oxygen (O₂) is continuously used by the body cells.
- Therefore, the intracellular PO₂ is always lower than the PO₂ in the peripheral capillaries.
- In many tissues, there is also a distance between the capillaries and the cells.
- Because of these factors, the normal intracellular PO₂ ranges:
- From 5 mm Hg to 40 mm Hg
- Average = 23 mm Hg
- The chemical processes inside the cells need only 1–3 mm Hg of O₂ pressure for full activity.
- Therefore, the average intracellular PO₂ of 23 mm Hg is more than enough to support normal cellular metabolism.
- This provides a large safety factor for oxygen supply.
Easy Concept
- Capillary PO₂ = 95 mm Hg
- Interstitial fluid PO₂ = 40 mm Hg
- Cell PO₂ = Average 23 mm Hg
- Oxygen always moves from higher PO₂ to lower PO₂:
Capillary (95 mm Hg)
↓
Interstitial Fluid (40 mm Hg)
↓
Cell (23 mm Hg)
↓
Mitochondria (1–3 mm Hg needed)- As long as this pressure gradient exists, oxygen keeps diffusing into the cells.
KEY CONCEPT
- Cells continuously consume oxygen, so their PO₂ remains lower than the surrounding capillaries. Oxygen diffuses from capillaries (95 mm Hg) → interstitial fluid (40 mm Hg) → cells (average 23 mm Hg), while only 1–3 mm Hg is needed for normal cellular metabolism, providing a large safety margin.
DIFFUSION OF CO₂ FROM PERIPHERAL TISSUE CELLS INTO CAPILLARIES AND FROM PULMONARY CAPILLARIES INTO ALVEOLI
- When oxygen (O₂) is used by the cells, it is converted into carbon dioxide (CO₂).
- This increases the intracellular PCO₂.
- Because intracellular PCO₂ is higher, CO₂ diffuses from the cells into the tissue capillaries.
- The blood carries CO₂ to the lungs.
- In the lungs, CO₂ diffuses from the pulmonary capillaries into the alveoli.
- CO₂ is then expired during breathing.
- At every step of gas transport:
- CO₂ diffuses in the opposite direction to O₂.
- However, there is one important difference:
- CO₂ diffuses about 20 times faster than O₂.
- Therefore, much smaller pressure differences are needed for CO₂ diffusion than for O₂ diffusion.
- The CO₂ pressure differences are:
- Between tissue cells and interstitial fluid
- Intracellular PCO₂ = 46 mm Hg
- Interstitial PCO₂ = 45 mm Hg
- Pressure difference = 46 − 45 = 1 mm Hg
- This small difference is enough for CO₂ to diffuse from the cells into the interstitial fluid.
- Between arterial blood and venous blood in the tissues
- Arterial blood PCO₂ = 40 mm Hg
- Venous blood PCO₂ = 45 mm Hg
- As blood passes through the tissue capillaries, its PCO₂ rises to about 45 mm Hg.
- This means the capillary blood almost completely equilibrates with the interstitial fluid.
- Between pulmonary capillary blood and alveolar air
- Pulmonary capillary blood PCO₂ = 45 mm Hg
- Alveolar PCO₂ = 40 mm Hg
- Pressure difference = 45 − 40 = 5 mm Hg
- This 5 mm Hg difference is enough to move all the required CO₂ from the blood into the alveoli.
- As shown in Fig. 41.6:
- The pulmonary capillary PCO₂ falls rapidly.
- It becomes almost equal to the alveolar PCO₂ (40 mm Hg) after the blood has traveled about one-third of the pulmonary capillary.
Fig. 41.5
- Intracellular PCO₂ = 46 mm Hg
- Interstitial PCO₂ = 45 mm Hg
- Arterial blood PCO₂ = 40 mm Hg
- Venous blood PCO₂ = 45 mm Hg
Fig. 41.6
- Pulmonary capillary blood PCO₂ = 45 mm Hg
- Alveolar PCO₂ = 40 mm Hg
- Blood PCO₂ falls to about 40 mm Hg within the first one-third of the pulmonary capillary.
KEY CONCEPT
- CO₂ always diffuses from higher PCO₂ to lower PCO₂, opposite to O₂ diffusion. Because CO₂ diffuses about 20 times faster than O₂, only very small pressure differences (1–5 mm Hg) are needed for rapid and efficient CO₂ exchange.
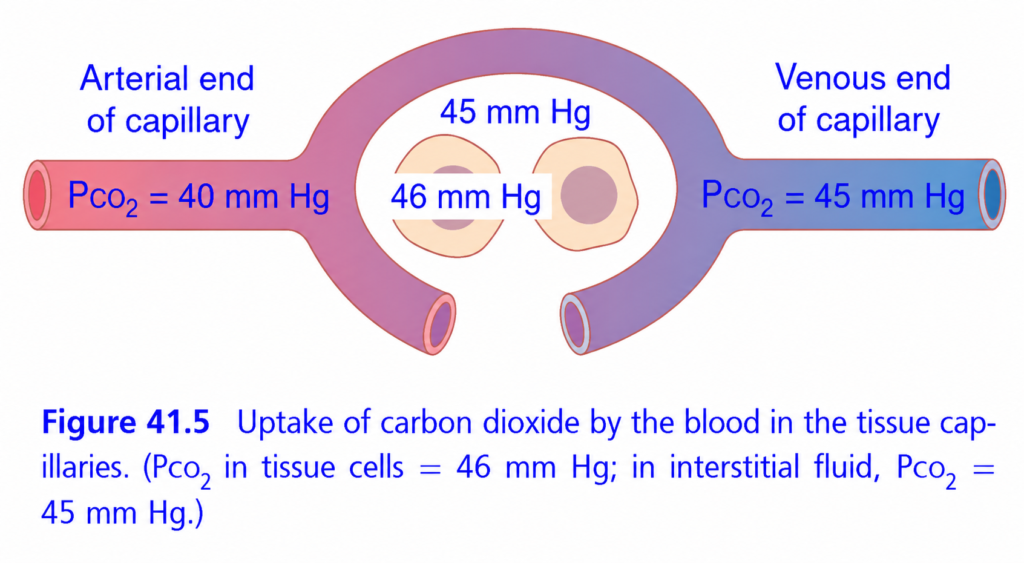
Diffusion of Carbon Dioxide (CO₂) from Body Cells into Blood (Guyton Fig. 41.5) – Easiest Concept
🎯 One-Line Concept
Carbon dioxide (CO₂) always moves from HIGH PCO₂ → LOW PCO₂.
Think of CO₂ as garbage produced by cells. It must be removed by the blood and carried to the lungs.
Step 1: Tissue Cells Produce CO₂
Every body cell continuously produces CO₂ during cellular respiration while making ATP.
Therefore, tissue cells have the highest CO₂ pressure.
PCO₂ = 46 mm Hg
Tissue Cell
PCO₂ = 46 mm Hg👉 This is the starting point of CO₂ movement.
Step 2: Interstitial Fluid Has Slightly Less CO₂
The fluid around the cells (interstitial fluid) has
PCO₂ = 45 mm Hg
Cell = 46
Interstitial fluid = 45Since
46 > 45
CO₂ diffuses
➡ Cell → Interstitial FluidStep 3: Arterial Blood Has Even Less CO₂
Blood arriving from the lungs contains
PCO₂ = 40 mm Hg
Blood = 40
Interstitial fluid = 45Since
45 > 40
CO₂ diffuses
➡ Interstitial Fluid → Blood
Step 4: Blood Picks Up CO₂
As blood flows through the capillary, it continuously receives CO₂ from the tissues.
Its PCO₂ gradually rises.
40
↑
41
↑
42
↑
43
↑
44
↑
45By the time blood reaches the venous end,
Venous Blood PCO₂ = 45 mm Hg
This is exactly what the figure shows.
Complete CO₂ Journey
Body Cell
PCO₂ = 46 mm Hg
↓
Interstitial Fluid
PCO₂ = 45 mm Hg
↓
Arterial Blood
PCO₂ = 40 mm Hg
↓
Venous Blood
PCO₂ = 45 mm Hg
↓
Lungs
↓
CO₂ ExhaledWhy Doesn’t Blood Reach 46 mm Hg?
Many students wonder:
If the cells have a PCO₂ of 46 mm Hg, why is venous blood only 45 mm Hg?
Simple Answer
CO₂ diffuses until the pressure difference becomes very small.
Blood does not need to reach exactly 46 mm Hg. By the time it reaches about 45 mm Hg, diffusion has slowed enough that the blood leaves the capillary and carries the CO₂ to the lungs.
Everyday Analogy
Imagine a room with smoke.
The room has lots of smoke.
Outside air has less smoke.
When you open the door,
the smoke naturally moves outside.
Exactly the same happens here.
Cell (46)
↓
Interstitial Fluid (45)
↓
Blood (40)CO₂ always moves toward the area with lower PCO₂.
Easy Memory Trick
Remember these numbers:
46 → 45 → 40
- 46 = Tissue cells
- 45 = Interstitial fluid (and venous blood)
- 40 = Arterial blood
CO₂ always moves:
46 → 45 → 40
Compare Oxygen and Carbon Dioxide
| Oxygen (O₂) | Carbon Dioxide (CO₂) |
|---|---|
| Arterial blood = 95 mm Hg | Tissue cells = 46 mm Hg |
| Interstitial fluid = 40 mm Hg | Interstitial fluid = 45 mm Hg |
| Tissue cells = 23 mm Hg | Arterial blood = 40 mm Hg |
| Moves from blood → cells | Moves from cells → blood |
Key Difference
- Oxygen is delivered to the tissues.
- Carbon dioxide is removed from the tissues.
Why Is This Important?
If CO₂ is not removed:
- ❌ CO₂ accumulates inside cells.
- ❌ Blood becomes more acidic (↓ pH).
- ❌ Cellular function is impaired.
The bloodstream continuously carries CO₂ to the lungs, where it is exhaled.
MBBS Exam Concept
Question: Why does CO₂ diffuse from tissue cells into the blood?
Answer:
Because tissue cells have the highest PCO₂ (46 mm Hg), interstitial fluid has 45 mm Hg, and arterial blood has the lowest PCO₂ (40 mm Hg). CO₂ always diffuses from higher partial pressure to lower partial pressure, so it moves from tissue cells → interstitial fluid → blood. Super Memory Summary
Body Cells
PCO₂ = 46 mm Hg
↓
(High → Low)
↓
Interstitial Fluid
PCO₂ = 45 mm Hg
↓
(High → Low)
↓
Arterial Blood
PCO₂ = 40 mm Hg
↓
Blood picks up CO₂
↓
Venous Blood leaves with
PCO₂ = 45 mm Hg
↓
Lungs → CO₂ is exhaled💡 Golden Rule
Carbon dioxide always diffuses from HIGH PCO₂ to LOW PCO₂.
Mnemonic: “46 → 45 → 40” = Cell → Tissue Fluid → Blood
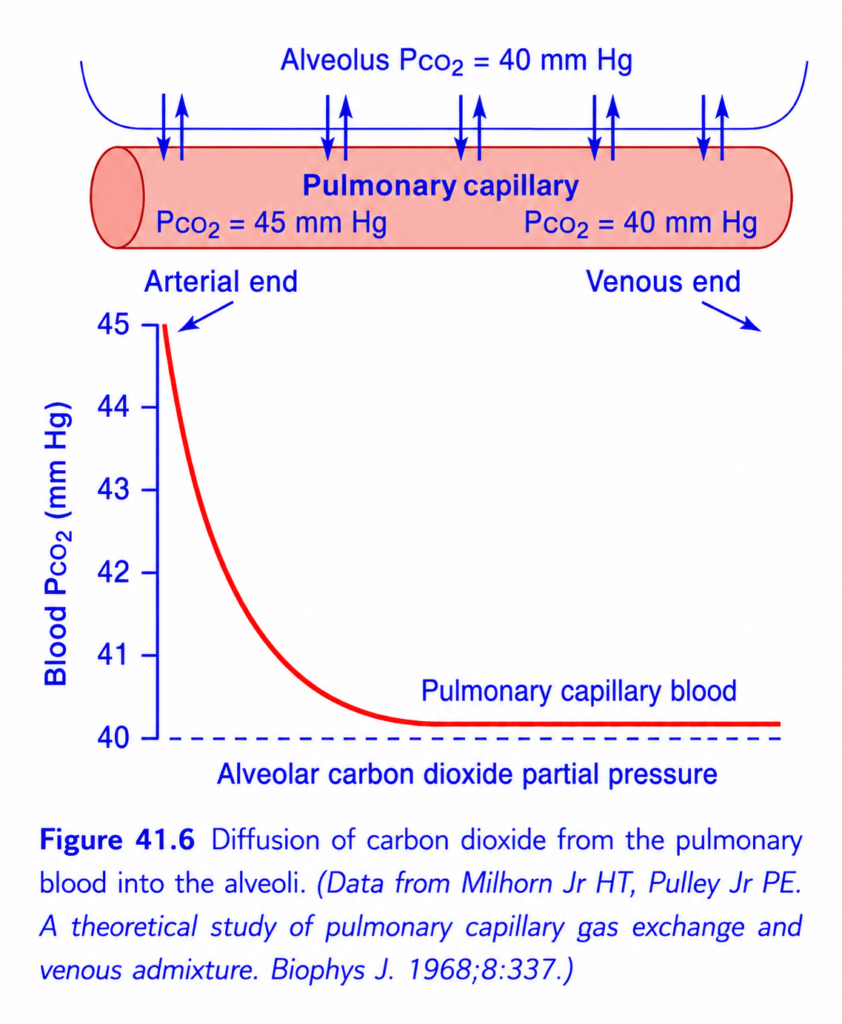
This is Figure 41.6 from Guyton Physiology, and it explains how carbon dioxide (CO₂) diffuses from pulmonary capillary blood into the alveoli.
This figure is the CO₂ counterpart of Figure 41.1 (oxygen uptake).
- Figure 41.1: O₂ moves Alveoli → Blood
- Figure 41.6: CO₂ moves Blood → Alveoli
Although CO₂ has only a 5 mmHg pressure difference (45 → 40 mmHg) compared with oxygen’s 64 mmHg (104 → 40 mmHg), CO₂ still diffuses just as rapidly because it is about 20 times more soluble (diffusible) than oxygen.
Figure 41.6: Diffusion of CO₂ from Pulmonary Blood into the Alveoli
⭐ One-Line Concept
Mixed venous blood enters the pulmonary capillary with a PCO₂ of 45 mmHg. CO₂ rapidly diffuses into the alveoli (PCO₂ = 40 mmHg) until blood PCO₂ also becomes 40 mmHg within the first one-third of the pulmonary capillary.
PART 1: Upper Diagram
What is shown?
Alveolus
PCO₂ = 40 mmHg
────────────────────────
↑ ↑ ↑ ↑ ↑ ↑
========================
Pulmonary Capillary
========================
PCO₂ = 45 → 40 mmHgThe upward arrows represent
CO₂ moving from blood into the alveolus.
Why Does CO₂ Move Upward?
Remember the basic diffusion rule:
Gas always diffuses from higher partial pressure to lower partial pressure.
Here,
| Location | PCO₂ |
|---|---|
| Pulmonary capillary blood | 45 mmHg |
| Alveolus | 40 mmHg |
Since
45 > 40
CO₂ naturally diffuses
Blood → Alveolus
No energy or pump is required.
This is simple diffusion.
Why Is Blood PCO₂ Initially 45 mmHg?
Blood entering the lungs comes from the body tissues.
The tissues continuously produce CO₂ during metabolism.
Therefore,
mixed venous blood returning to the lungs has
PCO₂ ≈45 mmHg.
Why Is Alveolar PCO₂ Only 40 mmHg?
The alveoli are continuously ventilated.
Every breath removes CO₂ from the alveoli.
Therefore,
alveolar CO₂ remains around
40 mmHg.
Pressure Gradient
This is the driving force for diffusion.
Blood = 45 mmHg
Alveolus = 40 mmHg
Difference = 5 mmHgEven though the gradient is only 5 mmHg, diffusion is still rapid.
Why Is Such a Small Gradient Enough?
This is the most important concept in this figure.
Many students ask:
“Oxygen needs a 64 mmHg gradient. Why does CO₂ need only 5 mmHg?”
The answer:
CO₂ is much more diffusible than O₂.
CO₂ diffuses approximately
20 times faster than oxygen
because it is much more soluble in the respiratory membrane.
So,
- Small pressure difference
- Very high diffusibility
↓
Rapid CO₂ transfer.Understanding the Pulmonary Capillary
Blood enters from the
Arterial End
Remember,
This is pulmonary circulation.
Pulmonary arteries carry
deoxygenated blood
with
PCO₂ = 45 mmHg.
Blood travels through the capillary.
CO₂ leaves continuously.
By the end,
Blood PCO₂ becomes
40 mmHg.
This end is called the
Venous End
because blood now enters the pulmonary veins.
PART 2: Lower Graph
Now let’s understand the graph.
X-Axis
The graph does NOT represent time directly.
It represents
Position of blood along the pulmonary capillary.
Left
↓
Blood entering
Right
↓
Blood leavingY-Axis
Blood PCO₂ (mmHg)
Shows
CO₂ pressure inside blood.
Top
↓
High CO₂
Bottom
↓
Low CO₂
Why Does the Curve Start at 45 mmHg?
Mixed venous blood arrives from body tissues.
The tissues have added CO₂.
Therefore,
Blood starts with
45 mmHg.
Why Does the Curve Fall?
Because
CO₂ diffuses into the alveolus.
As blood loses CO₂,
its PCO₂ decreases.
Simple.
Why Is the Fall Very Steep Initially?
Initially,
The pressure difference is largest.
Blood = 45
Alveolus = 40
Difference = 5 mmHgAlthough the gradient is small, CO₂ diffuses extremely rapidly because of its high diffusibility.
Therefore,
blood PCO₂ falls quickly.
Why Does the Curve Flatten?
Eventually,
Blood PCO₂ becomes
40 mmHg.
Now
Blood
=
Alveolus
No pressure difference remains.
Diffusion stops.
Therefore,
the graph becomes horizontal.
Dashed Horizontal Line
This line represents
Normal Alveolar PCO₂
=
40 mmHg
Blood can never fall below alveolar PCO₂ while breathing room air.
Why Does Equilibrium Occur So Early?
Look carefully.
Blood reaches
40 mmHg
within about the
first one-third of the pulmonary capillary.
Exactly like oxygen.
This means
CO₂ exchange finishes very early.
The remaining capillary length acts as a
diffusion reserve (safety factor).
Compare Oxygen and Carbon Dioxide
| Feature | Oxygen | Carbon Dioxide |
|---|---|---|
| Direction | Alveolus → Blood | Blood → Alveolus |
| Starting blood pressure | 40 mmHg | 45 mmHg |
| Alveolar pressure | 104 mmHg | 40 mmHg |
| Pressure gradient | 64 mmHg | 5 mmHg |
| Diffusibility | Lower | ~20× higher |
| Equilibrium | First one-third of capillary | First one-third of capillary |
Why Does CO₂ Diffuse So Easily?
Imagine
Two students crossing a muddy field.
Student 1 (Oxygen)
Walks slowly.
Needs a large push (large pressure gradient).
Student 2 (CO₂)
Slides easily on the mud.
Needs only a tiny push.
Exactly the same.
CO₂ moves across the respiratory membrane much more easily than oxygen.
Clinical Correlation
1. Exercise
During exercise,
CO₂ production increases.
However,
ventilation also increases.
Therefore,
alveolar and arterial PCO₂ usually remain around
40 mmHg.
2. Pulmonary Fibrosis
The respiratory membrane becomes thicker.
Both O₂ and CO₂ diffusion slow.
However,
CO₂ is less affected initially because it diffuses much more easily than oxygen.
That is why hypoxemia (low O₂) usually appears before hypercapnia (high CO₂) in many diffuse lung diseases.3. Severe Lung Disease
Only in advanced disease does CO₂ retention become significant.
Step-by-Step Journey of One CO₂ Molecule
BODY TISSUES
Produce CO₂
│
▼
Mixed Venous Blood
PCO₂ = 45 mmHg
│
▼
Pulmonary Capillary Begins
│
▼
Blood PCO₂ > Alveolar PCO₂
(45 > 40)
│
▼
CO₂ diffuses into alveolus
│
▼
Blood PCO₂ falls
45 → 43 → 42 → 41 → 40 mmHg
│
▼
Blood leaves lungs
PCO₂ = 40 mmHg
│
▼
CO₂ is exhaledHigh-Yield MBBS Viva Points
- Mixed venous blood enters the pulmonary capillary with PCO₂ ≈45 mmHg.
- Normal alveolar PCO₂ ≈40 mmHg.
- CO₂ diffuses from blood to alveoli because blood PCO₂ is higher than alveolar PCO₂.
- Blood PCO₂ reaches 40 mmHg within the first one-third of the pulmonary capillary.
- CO₂ requires only a 5 mmHg pressure gradient because it is about 20 times more diffusible than oxygen.
- CO₂ exchange is usually preserved until lung disease becomes advanced.
Super Easy Memory Trick
Imagine a crowded room with smoke:
- 🏠 Room = Blood
- 🌬️ Open window = Alveolus
- 🌫️ Smoke = CO₂
At first:
- The room has more smoke (45 mmHg).
- Outside (alveolus) has less smoke (40 mmHg).
As soon as you open the window:
- Smoke rushes out quickly.
- Soon, the smoke level inside equals the smoke level outside (40 mmHg).
- Once both are equal, smoke stops moving.
Exactly the same happens with CO₂ in the lungs.
🎯 MBBS Golden Rule
| Oxygen (Fig. 41.1) | Carbon Dioxide (Fig. 41.6) |
|---|---|
| Moves from alveolus → blood | Moves from blood → alveolus |
| Blood PO₂: 40 → 104 mmHg | Blood PCO₂: 45 → 40 mmHg |
| Large pressure gradient (64 mmHg) | Small pressure gradient (5 mmHg) |
| Lower diffusibility | ~20× higher diffusibility |
| Equilibrium in first one-third of capillary | Equilibrium in first one-third of capillary |
The key message of Figure 41.6: CO₂ is removed from pulmonary capillary blood extremely efficiently because it diffuses much more readily than oxygen, allowing complete equilibration with alveolar gas very early in the pulmonary capillary.
Effect of Tissue Metabolism and Tissue Blood Flow Rate on Interstitial PCO₂
- Tissue blood flow and tissue metabolism affect interstitial PCO₂.
- Their effects are exactly opposite to their effects on interstitial PO₂.
Fig. 41.7
1. Effect of Blood Flow
- At Point A (normal blood flow):
- Interstitial PCO₂ = 45 mm Hg
- If blood flow decreases to one-quarter of normal (Point B):
- Less CO₂ is removed from the tissues.
- Interstitial PCO₂ increases from 45 mm Hg to 60 mm Hg.
- If blood flow increases to six times normal (Point C):
- More CO₂ is removed from the tissues.
- Interstitial PCO₂ decreases from 45 mm Hg to 41 mm Hg.
- This value becomes almost equal to the arterial blood PCO₂ of 40 mm Hg.
2. Effect of Tissue Metabolism
- If tissue metabolism increases 10 times:
- Cells produce much more CO₂.
- Interstitial PCO₂ increases at all blood flow rates.
- If tissue metabolism decreases to one-quarter of normal:
- Cells produce much less CO₂.
- Interstitial PCO₂ decreases to about 41 mm Hg.
- This value becomes very close to the arterial blood PCO₂ of 40 mm Hg.
Easy Concept
Blood Flow Controls CO₂ Removal
- More blood flow → More CO₂ removed → Lower interstitial PCO₂
- Less blood flow → Less CO₂ removed → Higher interstitial PCO₂
Tissue Metabolism Controls CO₂ Production
- More metabolism → More CO₂ produced → Higher interstitial PCO₂
- Less metabolism → Less CO₂ produced → Lower interstitial PCO₂
Fig. 41.7 Summary
| Condition | Interstitial PCO₂ |
|---|---|
| Point A: Normal blood flow | 45 mm Hg |
| Point B: Blood flow = 25% of normal | 60 mm Hg |
| Point C: Blood flow = 600% of normal | 41 mm Hg |
| 10× metabolism | PCO₂ increases |
| ¼ metabolism | PCO₂ decreases to ~41 mm Hg |
KEY CONCEPT
- Interstitial PCO₂ depends on the balance between CO₂ production and CO₂ removal. Increased tissue metabolism raises PCO₂ by producing more CO₂, while increased blood flow lowers PCO₂ by removing CO₂ more rapidly. These effects are opposite to those seen with tissue PO₂.
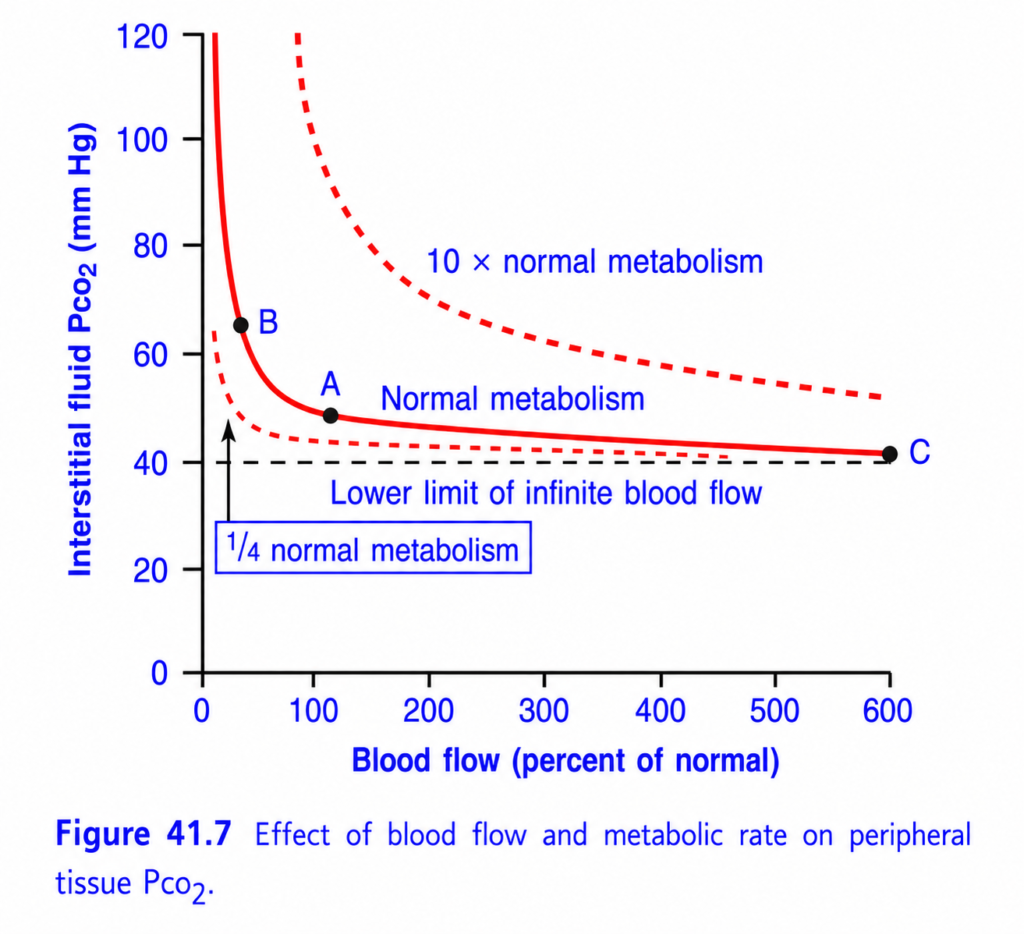
This is Figure 41.7 from Guyton Physiology, and it is the CO₂ version of Figure 41.4.
- Figure 41.4: Blood flow & metabolism affect Tissue PO₂
- Figure 41.7: Blood flow & metabolism affect Tissue PCO₂
The two graphs are exact opposites.
- More blood flow → PO₂ increases, but PCO₂ decreases.
- More metabolism → PO₂ decreases, but PCO₂ increases.
Figure 41.7: Effect of Blood Flow and Metabolic Rate on Tissue PCO₂
⭐ One-Line Concept
Tissue PCO₂ depends on the balance between CO₂ production (metabolism) and CO₂ removal (blood flow).
Simply,
- More metabolism → More CO₂ produced → Higher tissue PCO₂
- More blood flow → More CO₂ washed away → Lower tissue PCO₂
Think of it as:
Tissue PCO₂
=
CO₂ Produced (Metabolism)
-
CO₂ Removed (Blood Flow)Step 1: Understand the Axes
X-Axis (Horizontal)
Blood Flow (% of Normal)
This shows how much blood reaches the tissue.
Examples
- 0% = No blood flow
- 100% = Normal blood flow
- 300% = Three times normal
- 600% = Six times normal
👉 Moving to the right means more blood flow.
Y-Axis (Vertical)
Interstitial Fluid PCO₂ (mmHg)
This is the CO₂ pressure in the tissue fluid surrounding the cells.
It is not blood PCO₂.
Higher value
↓
More CO₂ accumulated in tissues.
Lower value
↓
Less CO₂ in tissues.
First Understand What Determines Tissue PCO₂
Every tissue cell continuously produces CO₂.
Blood continuously removes CO₂.
So tissue PCO₂ depends on two things:
CO₂ enters tissue
✔ Cellular metabolism
CO₂ leaves tissue
✔ Blood flow
The Three Curves
The graph shows three different metabolic rates.
🔻 Lower Dashed Curve
¼ Normal Metabolism
The tissue produces very little CO₂.
Examples
- Resting muscle
- Sleeping person
- Low metabolic activity
What Happens?
Very little CO₂ is produced.
Blood removes it easily.
Therefore,
Tissue PCO₂ remains low.
At Normal Blood Flow (100%)
PCO₂
≈42 mmHg
Very close to normal arterial PCO₂.
Easy Memory
Little CO₂ produced
↓
Little CO₂ remains
↓
Low tissue PCO₂
🔴 Middle Solid Curve
Normal Metabolism
This represents
Normal resting tissue.
Point A
Look at Point A.
Blood flow
=
100%
Metabolism
=
Normal
↓
Tissue PCO₂
≈45 mmHg
This is the normal operating point.
Meaning
Normal CO₂ production
Normal blood flow
=
Normal tissue PCO₂
≈45 mmHg
Point B
Now move left.
Blood flow becomes very low.
PCO₂ rises to about
60–65 mmHg.
Why?
Cells continue making CO₂.
But little blood is available to remove it.
Therefore,
CO₂ accumulates.
Clinical Examples
- Shock
- Arterial obstruction
- Severe hypotension
- Ischemia
All cause
↓
High tissue PCO₂.
Point C
Move to the far right.
Blood flow
≈600%
PCO₂
↓
40 mmHg
Why?
Large amounts of blood wash away CO₂ almost immediately.
Therefore,
Very little CO₂ remains.
🔺 Upper Dashed Curve
10× Normal Metabolism
Now the tissue produces
10 times more CO₂.
Examples
- Very intense exercise
- Severe muscle contractions
- Extreme metabolic activity
What Happens?
Cells produce enormous amounts of CO₂.
Even with increased blood flow,
large amounts of CO₂ remain.
Therefore,
Tissue PCO₂ stays high.
Example
At normal blood flow
PCO₂
≈70 mmHg
Much higher than normal.
Easy Memory
Huge CO₂ production
↓
Blood cannot remove all of it
↓
High tissue PCO₂
Understanding Every Point
Point A
Blood Flow
100%
Normal metabolism
↓
PCO₂
≈45 mmHg
Normal tissue.
Point B
Blood Flow
Very low
Normal metabolism
↓
PCO₂
≈60–65 mmHg
CO₂ accumulates because blood flow is insufficient.
Point C
Blood Flow
Very high
Normal metabolism
↓
PCO₂
≈40 mmHg
Blood removes CO₂ very efficiently.
Why Do All Curves Fall?
As blood flow increases,
more CO₂ is carried away.
Therefore,
less CO₂ remains in tissues.
Hence,
PCO₂ decreases.
Why Are the Curves Steep Initially?
Look carefully.
Increasing blood flow
from
20%
↓
100%
causes a huge fall in tissue PCO₂.
Later,
Increasing blood flow
from
400%
↓
600%
causes only a tiny decrease.
Why?
Because most CO₂ has already been removed.
Removing the remaining small amount produces only a slight effect.
Dashed Horizontal Line
Lower Limit of Infinite Blood Flow
Notice the dashed line at about
40 mmHg.
Why 40 mmHg?
Arterial blood entering tissues has
PCO₂ ≈40 mmHg.
Even with infinite blood flow, tissue PCO₂ cannot fall below the arterial PCO₂ because CO₂ cannot be removed to a value lower than the blood that is arriving.
Therefore,
40 mmHg
is the lowest possible tissue PCO₂.
Compare All Three Curves
| Curve | Metabolism | Tissue PCO₂ |
|---|---|---|
| Lower dashed | ¼ normal | Lowest |
| Middle solid | Normal | Intermediate |
| Upper dashed | 10× normal | Highest |
Compare Figure 41.4 and Figure 41.7
| Situation | Tissue PO₂ (Fig. 41.4) | Tissue PCO₂ (Fig. 41.7) |
|---|---|---|
| ↑ Blood flow | ↑ PO₂ | ↓ PCO₂ |
| ↓ Blood flow | ↓ PO₂ | ↑ PCO₂ |
| ↑ Metabolism | ↓ PO₂ | ↑ PCO₂ |
| ↓ Metabolism | ↑ PO₂ | ↓ PCO₂ |
These two graphs are mirror images of each other.
Easy Daily-Life Analogy
Imagine a city producing garbage.
- Cells = Factories producing garbage (CO₂).
- Blood flow = Garbage trucks removing garbage.
Situation 1
Few factories
Many garbage trucks
↓
Very little garbage remains.
↓
Low tissue PCO₂.
Situation 2
Normal factories
Normal trucks
↓
Balanced.
↓
Normal tissue PCO₂.Situation 3
Many factories
Few trucks
↓
Garbage accumulates.
↓
High tissue PCO₂.
Exactly like CO₂.
Clinical Correlation
1. Shock
Blood flow decreases.
CO₂ cannot be removed efficiently.
Tissue PCO₂ rises.
This is one reason poor tissue perfusion causes metabolic problems.
2. Exercise
Muscles produce much more CO₂.
Blood flow also increases greatly.
If blood flow increases proportionally, tissue PCO₂ rises only slightly.
3. Ischemia
Blood supply falls dramatically.
CO₂ accumulates rapidly in tissues.
This contributes to local acidosis and tissue dysfunction.
High-Yield MBBS Viva Points
- Normal tissue (interstitial) PCO₂ ≈45 mmHg (Point A).
- Increasing blood flow lowers tissue PCO₂ by washing out CO₂.
- Decreasing blood flow raises tissue PCO₂ because CO₂ accumulates.
- Increasing metabolism raises tissue PCO₂ by producing more CO₂.
- The lowest possible tissue PCO₂ approaches arterial PCO₂ (~40 mmHg) even with very high blood flow.
Super Easy Memory Trick
Imagine a room with smoke:
- 🏭 Factories = Cells producing CO₂.
- 🚛 Garbage trucks = Blood flow removing CO₂.
- 🌫️ Smoke = Tissue PCO₂.
Three situations:
- ¼ Normal metabolism (Lower dashed curve): Few factories produce little smoke → Trucks easily clear it → Low tissue PCO₂.
- Normal metabolism (Middle curve): Smoke production and removal are balanced → Normal tissue PCO₂ (~45 mmHg at Point A).
- 10× Normal metabolism (Upper dashed curve): Huge smoke production overwhelms removal → High tissue PCO₂.
🎯 MBBS Golden Rule
| Change | Effect on Tissue PCO₂ |
|---|---|
| ↑ Blood Flow | ↓ Tissue PCO₂ |
| ↓ Blood Flow | ↑ Tissue PCO₂ |
| ↑ Metabolism | ↑ Tissue PCO₂ |
| ↓ Metabolism | ↓ Tissue PCO₂ |
Final Rule to Remember
- Oxygen (PO₂): More blood flow adds oxygen, so PO₂ increases.
- Carbon dioxide (PCO₂): More blood flow removes CO₂, so PCO₂ decreases.
This opposite behavior of PO₂ and PCO₂ is the central physiological message of Figures 41.4 and 41.7 and is a favorite concept in MBBS exams and vivas.