Social Protection Programs
- Financial incentives improve:
- Healthcare access
- Poverty reduction
- Child health services
- Widely used to support poor and vulnerable families.
- COVID-19 greatly expanded social protection programs.
- Pandemic experience strengthened support systems for vulnerable children and families.
Types of Financial Incentives
- Unconditional Cash Transfers
- Given to eligible families without any conditions.
- Based on the belief that families use the money for their children’s needs.
- Conditional Cash Transfers
- Financial support is provided only when families meet specific health or education requirements.
Common Health-Related Conditions
- Attend breastfeeding education sessions.
- Visit health clinics for:
- Child vaccination
- Growth monitoring
- Participate in deworming programs.
- Ensure children receive:
- Vitamin A supplementation
- Iron supplementation
Education-Related Conditions
- Child school enrollment.
- Regular school attendance.
- Sometimes linked to academic performance.
Benefits of Social Protection Programs
- Reduce financial barriers to healthcare.
- Improve healthcare service delivery.
- Support child health and nutrition.
- Promote preventive healthcare.
- Encourage school participation.
Other Financial Incentive Programs
- Microcredit
- Vouchers
- Removal of user fees
- Health insurance
Technology-Based Innovations
- Mobile cash transfer systems improved delivery of financial support.
- Data and technology help identify families most in need.
- Continued international support is important for vulnerable communities.
KEY CONCEPT
- Social protection programs use conditional and unconditional cash transfers to reduce poverty, improve healthcare access, promote child health, and encourage education. COVID-19 accelerated the expansion of these programs and highlighted the value of technology-based financial support.
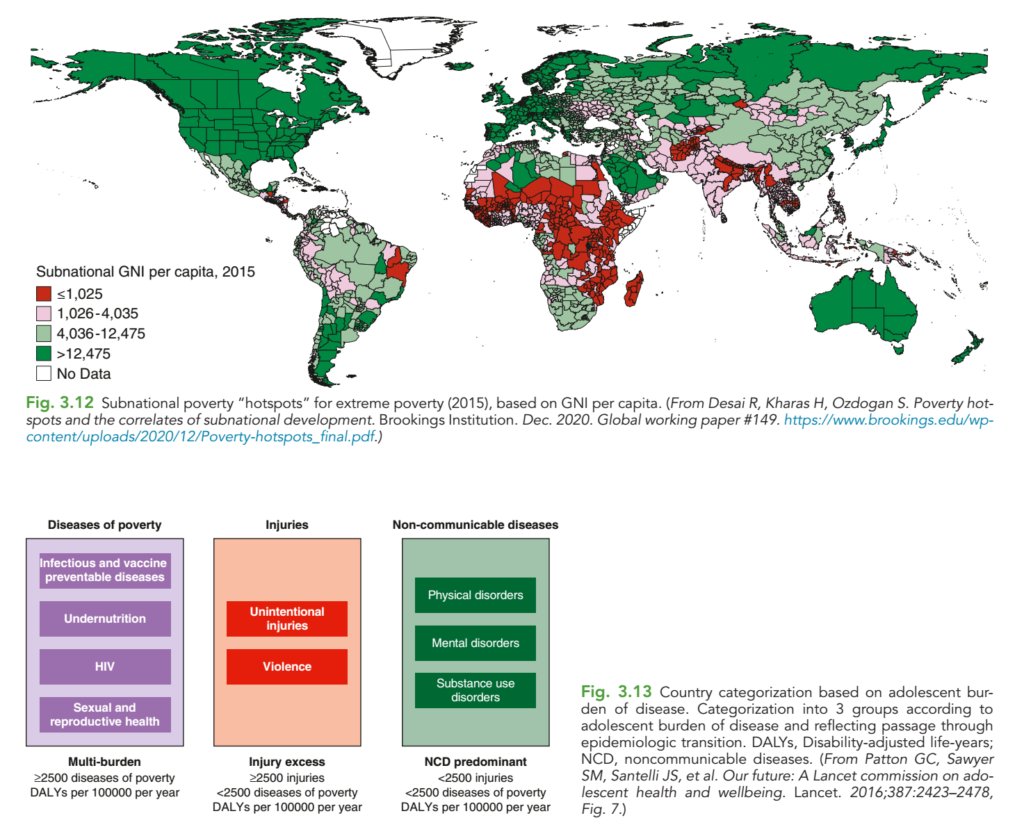
Figure Mentioned in Source: Fig. 3.12
Detailed Conceptual Explanation of the Nelson Textbook Figures (Fig. 3.12 and Fig. 3.13)
Topic: Global Poverty Hotspots and Adolescent Burden of Disease
Level: Pediatric Postgraduate Residents (PGR), FCPS, MD Pediatrics, MRCPCH, DCH
These two figures from Nelson Textbook of Pediatrics explain one of the most important concepts in Global Child Health:
Where children are born largely determines the diseases they develop, the health services they receive, and ultimately their chances of survival.
The figures demonstrate that poverty, geography, socioeconomic development, and epidemiologic transition determine the health problems of children and adolescents across the world.
FIGURE 3.12
Global Subnational Poverty Hotspots (GNI per Capita)
This map is not simply a country map.
It is a subnational map, meaning that it shows different regions or provinces inside each country.
Example:
Pakistan does not have one income level.
- Islamabad has much higher income.
- Interior Sindh has lower income.
- South Punjab differs from Central Punjab.
- Balochistan differs from Karachi.
Similarly,
India contains
- Kerala (higher income)
- Bihar (lower income)
Brazil contains
- São Paulo (rich)
- Amazon region (poor)
Therefore,
Health planning cannot be based only on country averages.
What is GNI per capita?
GNI = Gross National Income
Per capita means
Average income earned by one person in one year.
It estimates the economic status of people living in an area.
Higher GNI generally means
- Better nutrition
- Better sanitation
- Better education
- Better vaccination
- Better hospitals
- Better survival
Lower GNI generally means
- Poverty
- Malnutrition
- Poor healthcare
- High infectious diseases
- High maternal mortality
- High child mortality
Color Coding
Dark Green (> $12,475)
These are high-income regions.
Examples
- USA
- Canada
- Western Europe
- Japan
- Australia
- South Korea
Characteristics
✔ Excellent healthcare
✔ High vaccination
✔ Good sanitation
✔ High life expectancy
✔ Low infant mortality
Children usually die from
- congenital diseases
- cancers
- trauma
- obesity-related disorders
rather than infectious diseases.
Light Green ($4,036–12,475)
These represent
Upper-middle-income regions
Examples
- China (many regions)
- Brazil
- Turkey
- Malaysia
- South Africa (urban)
Characteristics
Rapid economic development
Improving hospitals
Falling infectious diseases
Increasing obesity
Increasing diabetes
Increasing hypertension
These countries are undergoing
Epidemiologic transition
Pink ($1,026–4,035)
These are
Lower-middle-income areas.
Examples
- Pakistan
- India
- Bangladesh
- Nepal
- Nigeria (some areas)
Characteristics
Double burden of disease
Children still suffer
- diarrhea
- pneumonia
- malnutrition
Adults increasingly develop
- diabetes
- hypertension
Therefore
Both communicable and noncommunicable diseases coexist.
Red (≤ $1,025)
These are
Extreme poverty hotspots.
Mostly
Sub-Saharan Africa
Parts of Afghanistan
Some areas of Yemen
Central African countries
Characteristics
Very limited healthcare
Poor nutrition
Unsafe drinking water
Low vaccination
High neonatal mortality
High maternal mortality
Frequent epidemics
Children die mainly from
- pneumonia
- diarrhea
- malaria
- measles
- malnutrition
rather than chronic diseases.
Why are some regions inside one country different?
Example
India
Kerala
- Better literacy
- Better vaccination
- Lower infant mortality
Bihar
- Higher poverty
- Lower female education
- Higher malnutrition
Same country
Different child health outcomes.
This explains why Nelson emphasizes
Subnational health planning.
Clinical Importance for Pediatricians
Suppose a child presents with fever.
Your differential diagnosis changes depending on where the child lives.
Rich country
Think
- leukemia
- autoimmune disease
- viral illness
Poor region
Think first
- malaria
- typhoid
- tuberculosis
- malnutrition
- HIV
Thus
Geography influences clinical reasoning.
Poverty Produces a Disease Cycle
Low income
↓
Poor education
↓
Poor sanitation
↓
Unsafe water
↓
Malnutrition
↓
Weak immunity
↓
Repeated infections
↓
School absence
↓
Lower earning capacity
↓
Persistent poverty
This is called the
Cycle of Poverty and Disease.
FIGURE 3.13
Country Categorization Based on Adolescent Burden of Disease
This figure explains the epidemiologic transition.
As countries become richer,
their disease patterns change.
Instead of infectious diseases,
people begin suffering mainly from
- obesity
- hypertension
- diabetes
- depression
This transition occurs gradually.
Nelson divides countries into three major categories.
Group 1
Diseases of Poverty
(Multi-burden Countries)
These countries still have
Infectious diseases
Examples
- Measles
- Tuberculosis
- Pneumonia
- Malaria
- Diarrhea
These diseases remain major killers.
Vaccine-preventable diseases
Examples
- Polio
- Measles
- Pertussis
- Diphtheria
These persist because vaccination coverage is incomplete.
Undernutrition
Children suffer
- wasting
- stunting
- micronutrient deficiency
Malnutrition worsens infections.
HIV
Many adolescents continue to develop
- HIV infection
- opportunistic infections
especially in parts of Sub-Saharan Africa.
Sexual and reproductive health problems
Examples
Teenage pregnancy
Unsafe abortion
STIs
Maternal deaths
Why is it called Multi-burden?
Because
one adolescent may simultaneously have
Malnutrition
Tuberculosis
Anemia
HIV
School dropout
This is multiple disease burden occurring together.
DALY
The figure mentions DALY.
DALY means
Disability-Adjusted Life Year.
It measures total health loss.
Formula
DALY = Years of Life Lost (YLL) + Years Lived with Disability (YLD)
Example
A child dies at age 5 instead of an expected lifespan of 70:
YLL = 65 years.
Another adolescent survives with paralysis for 20 years:
YLD accounts for those years lived with disability.
DALYs therefore capture both premature death and reduced quality of life.
Higher DALYs indicate a greater burden of disease in a population.
Group 2
Injury Excess Countries
These countries have fewer infectious diseases.
Instead,
injuries dominate.
Two major categories
Unintentional injuries
Examples
Road traffic accidents
Drowning
Falls
Burns
Poisoning
Electrical injuries
Violence
Examples
War
Firearm injuries
Child abuse
Gang violence
Interpersonal violence
Suicide
Adolescents are especially vulnerable because of
- increased independence
- risk-taking behavior
- substance use
- peer influence
Group 3
Noncommunicable Disease (NCD)-Predominant Countries
These are highly developed countries.
Infectious diseases have become relatively uncommon.
Instead,
the leading health problems are chronic conditions.
Physical disorders
Examples
Obesity
Type 2 diabetes
Asthma
Hypertension
Cancer
Inflammatory bowel disease
Mental disorders
Examples
Depression
Anxiety
ADHD
Eating disorders
Autism spectrum disorder
Self-harm
Mental health disorders often account for a large share of adolescent disability.
Substance use disorders
Examples
Alcohol misuse
Smoking
Nicotine dependence
Cannabis
Opioid misuse
Other substance abuse
These conditions contribute to long-term morbidity rather than immediate mortality.
Epidemiologic Transition
The figures together illustrate the progression from one disease pattern to another as socioeconomic conditions improve.
| Stage | Main Problems | Examples |
|---|---|---|
| Low-income | Infectious diseases, malnutrition, maternal deaths | Malawi, Niger |
| Lower-middle-income | Mixed burden (infectious + chronic diseases) | Pakistan, India, Bangladesh |
| Upper-middle-income | Increasing obesity, diabetes, trauma | China, Brazil, Turkey |
| High-income | Chronic diseases, mental illness, aging-related conditions | USA, Canada, Japan, Western Europe |
Pediatric Examples
Child in Rural Niger
Likely problems:
- Severe acute malnutrition
- Measles
- Malaria
- Pneumonia
- Vitamin A deficiency
Child in Rural Pakistan
Possible problems:
- Diarrhea
- Pneumonia
- Thalassemia
- Malnutrition
- Congenital heart disease
Child in Urban China
Possible problems:
- Childhood obesity
- Asthma
- Myopia
- Anxiety
- Road traffic injuries
Child in the United States
More common concerns include:
- Obesity
- Type 2 diabetes
- Depression
- ADHD
- Sports injuries
Key Examination Points for PGR
- Subnational analysis is more informative than national averages because disease burden varies widely within countries.
- GNI per capita is a strong indicator of access to nutrition, education, sanitation, and healthcare.
- Poverty is associated with infectious diseases, malnutrition, maternal mortality, and vaccine-preventable illnesses.
- As countries develop, they undergo an epidemiologic transition from communicable diseases to injuries and then to noncommunicable diseases (NCDs).
- DALY (Disability-Adjusted Life Year) is the standard metric for measuring total disease burden by combining premature mortality and disability.
- Many low- and middle-income countries, including Pakistan, experience a double burden of disease, where communicable diseases persist while NCDs are rapidly increasing.
- Effective pediatric practice requires understanding both the clinical presentation and the social determinants of health, as socioeconomic conditions strongly influence disease patterns, outcomes, and healthcare priorities.
Conceptual Summary
The central message of these Nelson textbook figures is that child and adolescent health is shaped by socioeconomic development. Poor regions predominantly face infectious diseases, undernutrition, and maternal-child health challenges. As economies improve, injuries become more prominent, and in high-income settings, chronic physical illnesses, mental health disorders, and substance use dominate. For pediatricians and PGR trainees, recognizing this transition is essential for disease prevention, diagnosis, public health planning, and resource allocation.
CHALLENGES IN GLOBAL HEALTH
Adolescent Health
- Adolescent health is a priority for achieving Sustainable Development Goals (SDGs).
- Investing in adolescents helps:
- Break the intergenerational cycle of poverty.
- Improve national productivity and economic growth.
- Major challenges:
- Limited health data, especially for adolescents aged 10–14 years.
- Need for greater youth participation in identifying health priorities.
- Key strategy:
- Improve completion of secondary school education, especially among girls.
- Education helps adolescents:
- Become economically independent.
- Become positive contributors to society.
- Break the cycle of poverty.
📌 Figure Mentioned: Fig. 3.13 (Major threats to adolescent health)
Major Threats to Adolescent Health
- Mental health disorders.
- Substance abuse.
- Sexual and reproductive health problems.
- Noncommunicable diseases (NCDs), such as obesity.
- Increased adolescent pregnancy emphasizes the need for:
- Sexual education.
- Reproductive health services.
Promoting Healthy Behaviors
- Interventions should:
- Promote healthy lifestyles.
- Improve individual behaviors and attitudes.
- Major concerns:
- Mental health disorders.
- Depression.
- Suicide.
- Effective management requires:
- Multidisciplinary approaches.
- Continued research.
Climate Change
- Climate change is a major long-term threat to child health.
- Results in:
- Environmental degradation.
- Loss of natural resources.
- Reduced food and water supplies.
- Poor child health and nutrition.
- Reducing greenhouse gas emissions is essential.
📌 Figure Mentioned: Fig. 3.14 (Children during conflict, emergencies, and migration)
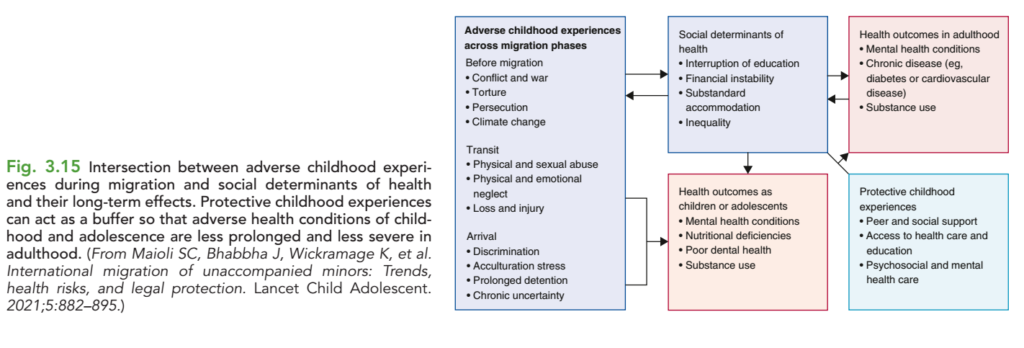
Conflict, Emergency Situations, and Migration
- Children, adolescents, and women are the most vulnerable during crises.
- Major consequences:
- Disease and injuries.
- Food shortages.
- Poor water and sanitation.
- Interrupted education.
- Family separation and displacement.
- Migrant children are at increased risk of:
- Discrimination.
- Exploitation.
- A rights-based approach should:
- Protect migrant children.
- Address long-term health and social consequences.
- Reduce root causes such as poverty, inequality, instability, and discrimination.
- Support vulnerable children and families.
📌 Figure Mentioned: Fig. 3.15 (Policies and support for migrant and vulnerable children)
Health Information and Communications Technology (HICT)
- HICT has transformed healthcare delivery.
- Social media and mobile applications help:
- Increase health awareness.
- Improve health education.
- Major barriers:
- Poor health data infrastructure.
- Limited internet and electricity.
- Lack of trained workforce.
- Inadequate funding.
- Technology not suited to local healthcare needs.
- Key priorities:
- Ensure privacy and data security.
- Standardize health data.
- Improve health information sharing.
- Strengthen collaboration between healthcare and technology sectors.
KEY CONCEPT
- Major global health challenges include adolescent health, climate change, conflict and migration, and health information and communications technology (HICT). Addressing these challenges requires investment in education, healthy lifestyles, protection of vulnerable populations, stronger health systems, and effective use of technology.
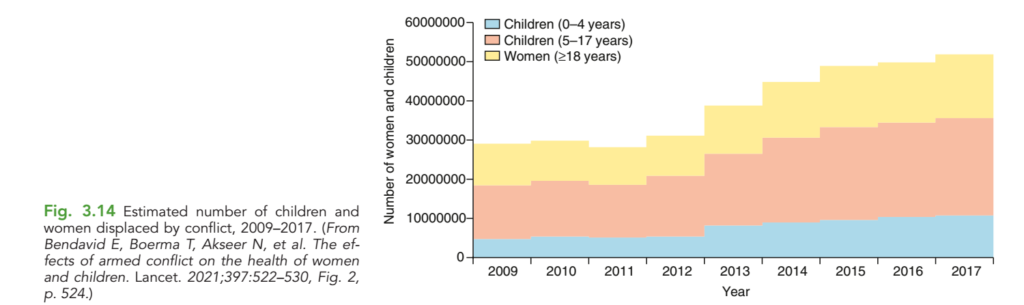
Detailed Conceptual Explanation of Nelson Textbook Figure 3.14
Estimated Number of Women and Children Displaced by Armed Conflict (2009–2017)
Level: Pediatric Postgraduate Residents (PGR), FCPS, MD Pediatrics, MRCPCH, DCH, Public Healthhe Main Message of This Figure
This figure demonstrates that:
Armed conflict is not only a military or political issue—it is one of the largest global pediatric and maternal health emergencies.
Every war creates a large population of:
- displaced infants
- displaced children
- displaced adolescents
- displaced mothers
- pregnant women
- newborns
These people often lose access to:
- Food
- Shelter
- Clean water
- Hospitals
- Vaccination
- Schools
- Medicines
- Maternal care
As conflicts increase, the number of displaced women and children rises dramatically, leading to major health crises.
What Does “Displaced” Mean?
A displaced person is someone who is forced to leave their home because it is no longer safe.
They may leave due to:
- War
- Civil conflict
- Terrorism
- Bombing
- Ethnic violence
- Political instability
Displacement can occur:
1. Internally Displaced Persons (IDPs)
These individuals remain within their own country.
Example:
A family moves from one city to another within Sudan due to fighting.
2. Refugees
These individuals cross an international border to seek safety.
Example:
A Syrian family relocates to Turkey or Jordan.
Understanding the Graph
The graph covers:
Years: 2009–2017
The Y-axis represents the estimated number of displaced women and children.
The graph is stacked, meaning each colored section contributes to the total.
Color Coding
Blue
Children (0–4 years)
These are:
- Neonates
- Infants
- Toddlers
- Preschool children
This is the most medically vulnerable group.
Pink
Children (5–17 years)
This includes:
- School-age children
- Adolescents
They form the largest proportion of displaced children.
Yellow
Women (≥18 years)
This group includes:
- Mothers
- Pregnant women
- Breastfeeding women
- Female caregivers
Their health directly affects the survival and well-being of children.
What Trend Does the Graph Show?
2009–2011
The total number of displaced women and children remains relatively stable at approximately 28–30 million.
Although conflicts existed during this period, the overall burden was lower than in later years.
2012
A slight increase is observed.
This period coincides with escalating conflicts in several regions.
2013
A sharp rise occurs, with the total approaching 40 million displaced women and children.
This increase reflects the intensification of multiple humanitarian crises.
2014–2015
The graph continues to climb, reaching around 45–48 million.
This indicates that prolonged conflicts are displacing more families over time.
2016–2017
The total exceeds 50 million, the highest value shown.
This means that by 2017:
- More than 50 million women and children had been displaced due to armed conflict.
Why Does the Number Increase Over Time?
Armed conflicts often become prolonged rather than ending quickly.
Examples during this period include:
- Civil wars
- Political instability
- Ethnic violence
- Terrorism
- International conflicts
As conflicts continue:
- Homes are destroyed.
- Schools close.
- Hospitals are damaged.
- Families flee repeatedly.
Thus, displacement accumulates year after year.
Why Are Children the Most Vulnerable?
Children have limited physiological reserves and depend on caregivers for survival.
During displacement, they face:
Nutritional Problems
- Acute malnutrition
- Stunting
- Micronutrient deficiencies
- Growth failure
Example:
A two-year-old living in a refugee camp receives only one meal per day and develops severe acute malnutrition.
Infectious Diseases
Overcrowded shelters facilitate disease transmission.
Common illnesses include:
- Measles
- Pneumonia
- Diarrhea
- Tuberculosis
- Cholera
- Malaria (in endemic areas)
Example:
Ten families sharing one tent with poor sanitation can rapidly spread respiratory and gastrointestinal infections.
Interrupted Vaccination
Conflict disrupts immunization programs.
Consequences include outbreaks of:
- Measles
- Polio
- Diphtheria
- Pertussis
Clinical Example:
A child who missed routine vaccines develops measles in a refugee camp.
Mental Health Effects
Children exposed to violence may experience:
- Anxiety
- Depression
- Post-traumatic stress disorder (PTSD)
- Sleep disturbances
- Behavioral regression
Example:
A child who witnessed bombing develops nightmares and refuses to attend school.
Educational Disruption
Displacement often interrupts schooling for months or years.
This affects:
- Literacy
- Cognitive development
- Future employment opportunities
Why Are Women Especially Vulnerable?
Women face unique health challenges during conflict.
Pregnancy
Many pregnant women lose access to:
- Antenatal care
- Skilled birth attendants
- Emergency obstetric services
This increases the risk of:Delivery
Without hospitals, childbirth may occur:
- At home
- In tents
- During migration
Complications such as postpartum hemorrhage or obstructed labor become life-threatening.Breastfeeding Challenges
Stress, food insecurity, and lack of privacy can impair breastfeeding.
Infants may then require unsafe alternatives, increasing the risk of malnutrition and infection.
Gender-Based Violence
Conflict settings increase the risk of:
- Sexual violence
- Human trafficking
- Exploitation
- Forced marriage
These have profound physical and psychological consequences.
Why Is the 0–4 Year Age Group Highlighted Separately?
Young children have:
- Immature immune systems
- Higher metabolic demands
- Greater susceptibility to dehydration
- Complete dependence on caregivers
Even brief interruptions in food, water, or healthcare can rapidly become life-threatening.
Why Is the 5–17 Year Group the Largest?
This age group includes:
- School-age children
- Adolescents
They often represent the largest proportion of displaced families because they constitute a significant share of the population in many conflict-affected countries.
Health issues include:
- Interrupted education
- Trauma
- Injury
- Recruitment into armed groups (in some settings)
- Early marriage
- Substance use
- Mental health disorders
Pediatric Perspective
For pediatricians, displacement is associated with a predictable spectrum of disease:
| Health Domain | Common Problems |
|---|---|
| Nutrition | Severe acute malnutrition, anemia, micronutrient deficiencies |
| Infectious diseases | Measles, pneumonia, diarrhea, tuberculosis, malaria |
| Vaccination | Missed immunizations and outbreaks of vaccine-preventable diseases |
| Mental health | PTSD, anxiety, depression, behavioral disorders |
| Development | Growth failure, developmental delay, learning difficulties |
| Child protection | Abuse, neglect, trafficking, exploitation |
Public Health Perspective
Conflict affects every component of the health system:
- Hospitals are destroyed or inaccessible.
- Healthcare workers may flee or be injured.
- Medicine supplies become limited.
- Vaccination campaigns are interrupted.
- Disease surveillance weakens.
- Safe water and sanitation deteriorate.
The result is a higher burden of preventable illness and death.Real-World Examples
Syria
Millions of women and children were displaced during the civil war.
Health consequences included:
- Interrupted vaccination
- Measles outbreaks
- Malnutrition
- Mental health disorders
Ukraine
Large-scale displacement disrupted:
- Maternal healthcare
- Neonatal services
- Childhood immunization
- Chronic disease management
Sudan
Conflict has resulted in:
- Severe food insecurity
- Cholera outbreaks
- Acute malnutrition
- Limited access to maternal and pediatric care
Afghanistan
Children have faced:
- Malnutrition
- Interrupted education
- Vaccine access challenges
- Increased maternal and infant health risks
Why Is This Figure Important for Pediatricians?
This figure emphasizes that armed conflict is a major determinant of child health, not just a political event. Displacement increases the risk of malnutrition, infectious diseases, interrupted immunization, psychological trauma, and maternal complications. Pediatricians working in humanitarian settings must therefore integrate clinical care with nutrition, vaccination, mental health support, child protection, and public health interventions.
High-Yield Examination Points (PGR/FCPS/MRCPCH)
- Armed conflict is a major social determinant of child and maternal health.
- Displacement may be internal (IDPs) or across international borders (refugees).
- Children aged 0–4 years are the most medically vulnerable because of immature immunity, rapid nutritional needs, and complete dependence on caregivers.
- Common health consequences include malnutrition, infectious diseases, interrupted immunization, mental health disorders, developmental delays, and increased child mortality.
- Women are at increased risk of maternal complications, unsafe childbirth, poor antenatal care, gender-based violence, and breastfeeding difficulties.
- Rising displacement from 2009 to 2017 reflects the growing impact of prolonged armed conflicts on global child health.
- Pediatricians should recognize that protecting child health in conflict settings requires both clinical management and humanitarian public health measures, including nutrition programs, immunization campaigns, safe water and sanitation, maternal care, and psychosocial support.