Skip to content
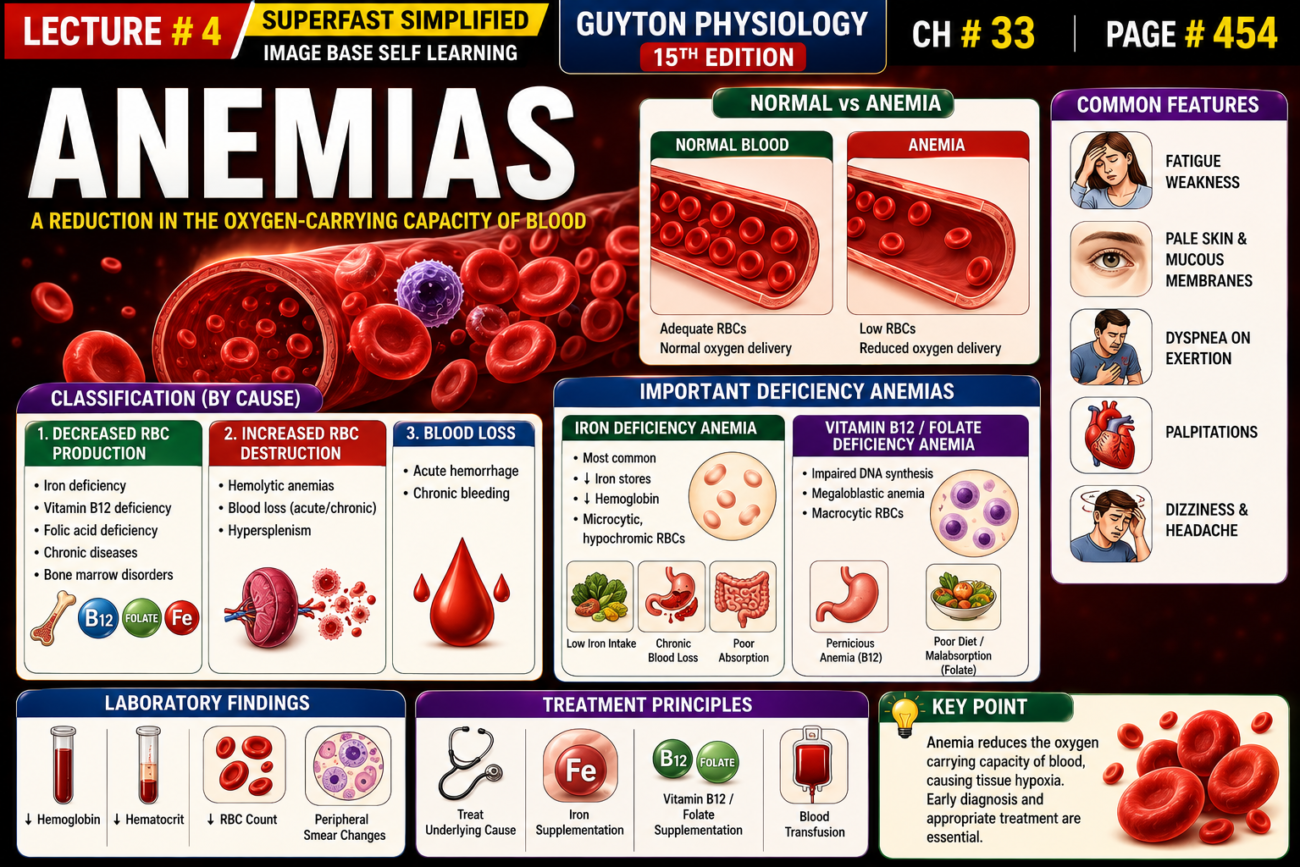
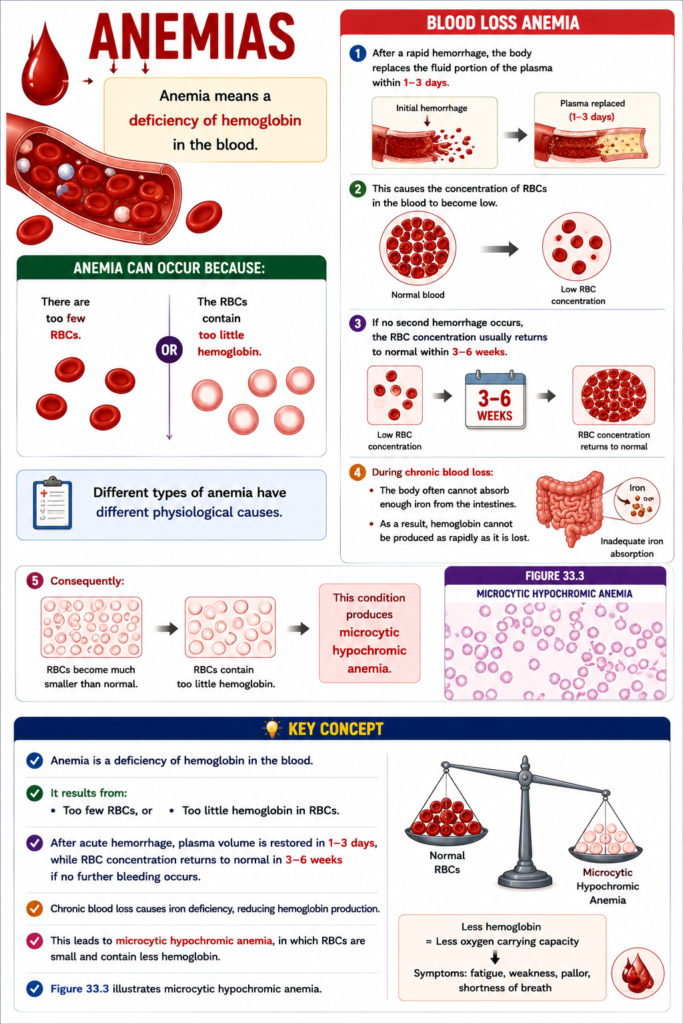
Anemia means a deficiency of hemoglobin in the blood .
Anemia can occur because:
There are too few RBCs .
The RBCs contain too little hemoglobin .
Different types of anemia have different physiological causes.
Blood Loss Anemia
After a rapid hemorrhage, the body replaces the fluid portion of the plasma within 1–3 days .
This causes the concentration of RBCs in the blood to become low .
If no second hemorrhage occurs:
The RBC concentration usually returns to normal within 3–6 weeks .
During chronic blood loss :
The body often cannot absorb enough iron from the intestines.
As a result, hemoglobin cannot be produced as rapidly as it is lost.
Consequently:
RBCs become much smaller than normal .
RBCs contain too little hemoglobin .
This condition produces microcytic hypochromic anemia .
Figure 33.3 shows microcytic hypochromic anemia .
KEY CONCEPT
Anemia is a deficiency of hemoglobin in the blood.
It results from:
Too few RBCs, or
Too little hemoglobin in RBCs.
After acute hemorrhage , plasma volume is restored in 1–3 days , while RBC concentration returns to normal in 3–6 weeks if no further bleeding occurs.
Chronic blood loss causes iron deficiency, reducing hemoglobin production.This leads to microcytic hypochromic anemia , in which RBCs are small and contain less hemoglobin .
Figure 33.3 illustrates microcytic hypochromic anemia.
ANEMIAS
Aplastic anemia is caused by bone marrow dysfunction .Bone marrow aplasia means lack of functioning bone marrow .Exposure to high-dose radiation can damage bone marrow stem cells .
Chemotherapy for cancer treatment can also damage bone marrow stem cells.A few weeks after stem cell damage, anemia develops .
High doses of certain toxic chemicals can also damage the bone marrow.
Examples include:
Insecticides
Benzene in gasoline
These toxic chemicals can produce the same effect as radiation and chemotherapy.
In autoimmune disorders , the immune system attacks healthy cells.
In lupus erythematosus , the immune system may attack bone marrow stem cells .
This can lead to aplastic anemia .
In about half of all aplastic anemia cases , the cause is unknown .
This condition is called idiopathic aplastic anemia .
People with severe aplastic anemia usually die if they are not treated.
Blood transfusions can temporarily increase the number of RBCs.Bone marrow transplantation is another treatment option.
KEY CONCEPT
Aplastic anemia results from bone marrow dysfunction .
Bone marrow aplasia means non-functioning bone marrow .
Causes include:
High-dose radiation
Chemotherapy
Toxic chemicals (insecticides, benzene)
Autoimmune disorders such as lupus erythematosus
About 50% of cases are idiopathic (cause unknown).
Severe aplastic anemia requires treatment with blood transfusions or bone marrow transplantation .
ANEMIAS
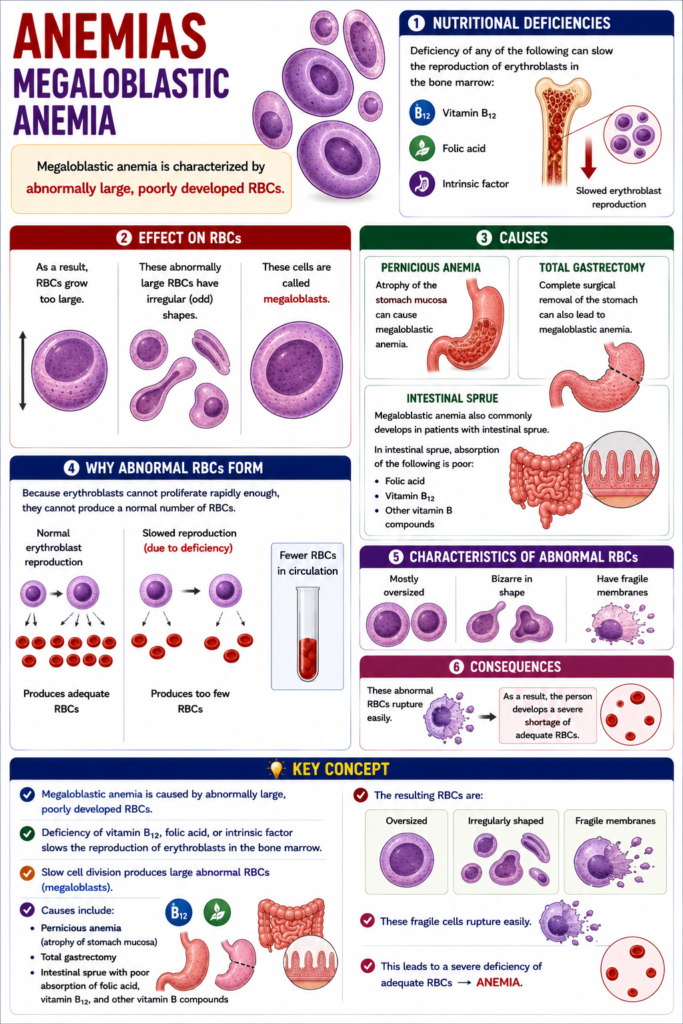
Megaloblastic anemia is characterized by abnormally large, poorly developed RBCs .Deficiency of any of the following can slow the reproduction of erythroblasts in the bone marrow:
Vitamin B12
Folic acid
Intrinsic factor
As a result, RBCs grow too large .
These abnormally large RBCs have irregular (odd) shapes .
These cells are called megaloblasts .
Atrophy of the stomach mucosa , as seen in pernicious anemia , can cause megaloblastic anemia.Total gastrectomy (complete surgical removal of the stomach) can also lead to megaloblastic anemia.Megaloblastic anemia also commonly develops in patients with intestinal sprue .
In intestinal sprue, absorption of the following is poor:
Folic acid
Vitamin B12
Other vitamin B compounds
Because erythroblasts cannot proliferate rapidly enough, they cannot produce a normal number of RBCs.
The RBCs that are produced are:
Mostly oversized
Bizarre in shape
Have fragile membranes
These abnormal RBCs rupture easily.
As a result, the person develops a severe shortage of adequate RBCs.
KEY CONCEPT
Megaloblastic anemia is caused by abnormally large, poorly developed RBCs .
Deficiency of vitamin B12 , folic acid , or intrinsic factor slows erythroblast reproduction.
Slow cell division produces large abnormal RBCs (megaloblasts) .
Causes include:
Pernicious anemia (atrophy of the stomach mucosa)Total gastrectomy Intestinal sprue with poor absorption of folic acid, vitamin B12, and other vitamin B compounds
The resulting RBCs are oversized , irregularly shaped , and have fragile membranes .
These fragile cells rupture easily, leading to anemia.
ANEMIAS
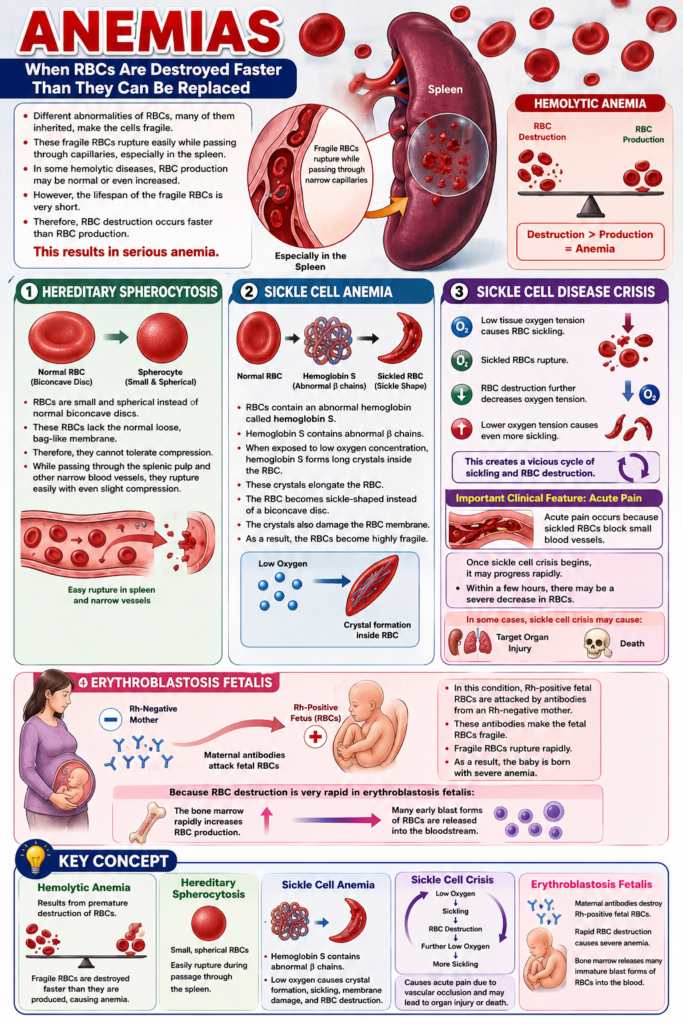
Hemolytic anemia occurs when RBCs are destroyed faster than they can be replaced.Different abnormalities of RBCs, many of them inherited , make the cells fragile.
These fragile RBCs rupture easily while passing through capillaries, especially in the spleen .
In some hemolytic diseases, RBC production may be normal or even increased .
However, the lifespan of the fragile RBCs is very short.
Therefore, RBC destruction occurs faster than RBC production.
This results in serious anemia .
Hereditary spherocytosis
RBCs are small and spherical instead of normal biconcave discs .
These RBCs lack the normal loose, bag-like membrane.
Therefore, they cannot tolerate compression.
While passing through the splenic pulp and other narrow blood vessels, they rupture easily with even slight compression.
Sickle cell anemia
RBCs contain an abnormal hemoglobin called hemoglobin S .
Hemoglobin S contains abnormal beta (β) chains .
When exposed to low oxygen concentration , hemoglobin S forms long crystals inside the RBC.
These crystals elongate the RBC.
The RBC becomes sickle-shaped instead of a biconcave disc.
The crystals also damage the RBC membrane.
As a result, the RBCs become highly fragile.
This leads to serious anemia .
Sickle cell disease crisis
Low tissue oxygen tension causes RBC sickling.
Sickled RBCs rupture.
RBC destruction further decreases oxygen tension.
Lower oxygen tension causes even more sickling.
This creates a vicious cycle of sickling and RBC destruction.
An important clinical feature of sickle cell crisis is acute pain .
Acute pain occurs because sickled RBCs block small blood vessels .
Once sickle cell crisis begins, it may progress rapidly.
Within a few hours, there may be a severe decrease in RBCs.
In some cases, sickle cell crisis may cause:
Target organ injury
Death
Erythroblastosis fetalis
In this condition, Rh-positive fetal RBCs are attacked by antibodies from an Rh-negative mother .
These antibodies make the fetal RBCs fragile.
Fragile RBCs rupture rapidly.
As a result, the baby is born with severe anemia .
Because RBC destruction is very rapid in erythroblastosis fetalis:
The bone marrow rapidly increases RBC production.
Many early blast forms of RBCs are released into the bloodstream.
KEY CONCEPT
Hemolytic anemia results from premature destruction of RBCs .
Fragile RBCs are destroyed faster than they are produced, causing anemia.
Hereditary spherocytosis:
Small, spherical RBCs
Easily rupture during passage through the spleen.
Sickle cell anemia:
Hemoglobin S contains abnormal β chains .
Low oxygen causes crystal formation, sickling, membrane damage, and RBC destruction.
Sickle cell crisis:
Low oxygen → Sickling → RBC destruction → Further low oxygen → More sickling.
Causes acute pain due to vascular occlusion and may lead to organ injury or death.
Erythroblastosis fetalis:
Maternal antibodies destroy Rh-positive fetal RBCs .
Rapid RBC destruction causes severe anemia.
Bone marrow releases many immature blast forms of RBCs into the blood.
Effects of Anemia on Circulatory System Function
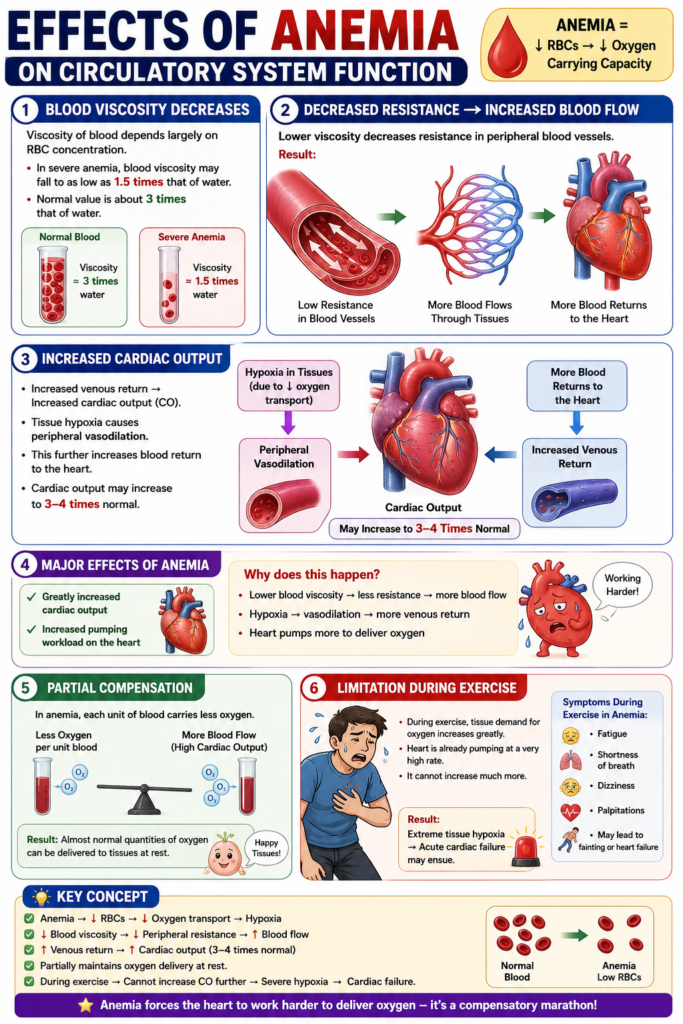
Blood viscosity depends mainly on the concentration of RBCs .
In people with severe anemia , blood viscosity may decrease to about 1.5 times the viscosity of water.
Normally, blood viscosity is about 3 times the viscosity of water.
Lower blood viscosity decreases the resistance to blood flow in the peripheral blood vessels.
As a result, much larger amounts of blood flow through the tissues.
More blood also returns to the heart .
This greatly increases cardiac output .
Reduced oxygen transport in anemia causes hypoxia .
Hypoxia causes the peripheral blood vessels to dilate .
Vasodilation allows even more blood to return to the heart .
This further increases cardiac output .
Cardiac output may increase to 3–4 times the normal value .
Therefore, one of the major effects of anemia is a marked increase in cardiac output .
The increased cardiac output also increases the pumping workload of the heart .
The increased cardiac output partly compensates for the reduced oxygen-carrying capacity of the blood.
Although each unit of blood carries less oxygen , the higher blood flow helps deliver almost normal amounts of oxygen to the tissues.
During exercise , tissue oxygen demand increases greatly.
In a person with anemia, the heart is already pumping at a high rate .
Therefore, the heart cannot increase cardiac output much further during exercise.
As a result, severe tissue hypoxia develops during exercise.
Severe tissue hypoxia may lead to acute cardiac failure .
KEY CONCEPT
Blood viscosity depends mainly on the RBC concentration .
In severe anemia:
Blood viscosity falls from about 3 to 1.5 times the viscosity of water.
Peripheral vascular resistance decreases.
Blood flow to tissues and venous return increase.
Hypoxia causes peripheral vasodilation , further increasing venous return and cardiac output.
Cardiac output may rise to 3–4 times normal .
Increased cardiac output partially compensates for reduced oxygen-carrying capacity.
During exercise, the heart cannot increase output much further, leading to severe tissue hypoxia and possible acute cardiac failure .
POLYCYTHEMIA
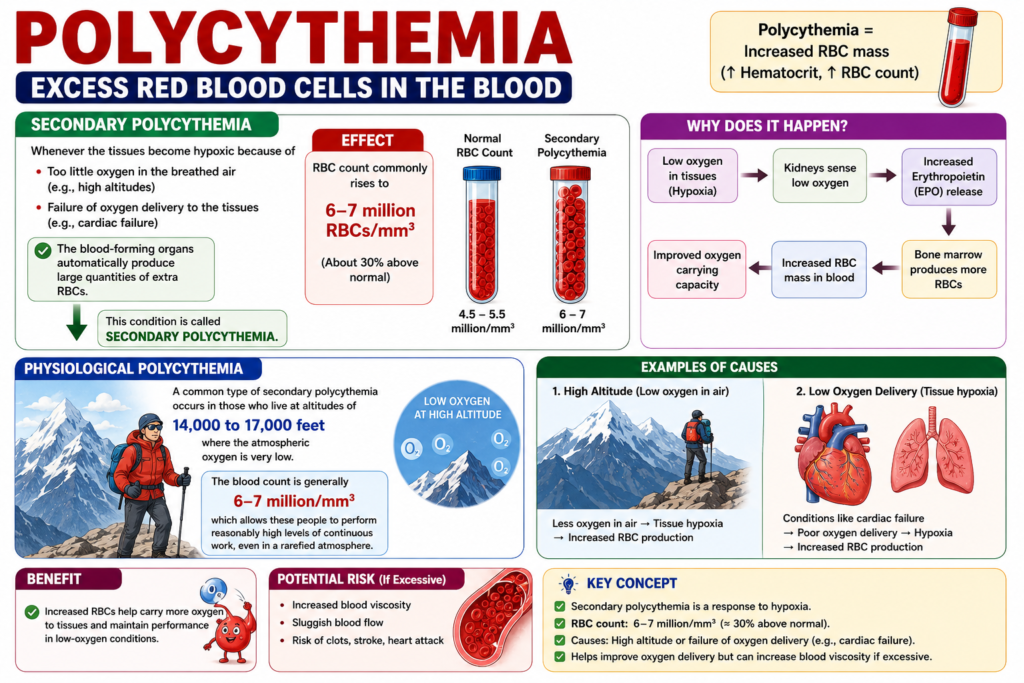
Secondary polycythemia occurs when the tissues become hypoxic .Tissue hypoxia may occur because:
Too little oxygen is present in the inspired air, such as at high altitudes .
Oxygen delivery to the tissues is reduced, such as in cardiac failure .
In response to hypoxia, the blood-forming organs automatically produce large numbers of additional RBCs .
This increase in RBC production is called secondary polycythemia .
In secondary polycythemia, the RBC count commonly increases to 6–7 million/mm³ .
This is about 30% above the normal RBC count .
A common type of secondary polycythemia is physiological polycythemia .
Physiological polycythemia occurs in people living at 14,000–17,000 feet above sea level.
At these high altitudes, the atmospheric oxygen level is very low .
The RBC count in these people is generally 6–7 million/mm³ .
This increased RBC count allows them to perform reasonably high levels of continuous work .
They are able to do this even in a rarefied (low-oxygen) atmosphere .
KEY CONCEPT
Secondary polycythemia develops due to tissue hypoxia .Causes of hypoxia include:
High altitude Cardiac failure
Hypoxia stimulates the blood-forming organs to produce more RBCs .
The RBC count commonly rises to 6–7 million/mm³ , about 30% above normal .
Physiological polycythemia occurs in people living at 14,000–17,000 feet , where atmospheric oxygen is low.The increased RBC count helps maintain work capacity in a low-oxygen (rarefied) environment .
POLYCYTHEMIA
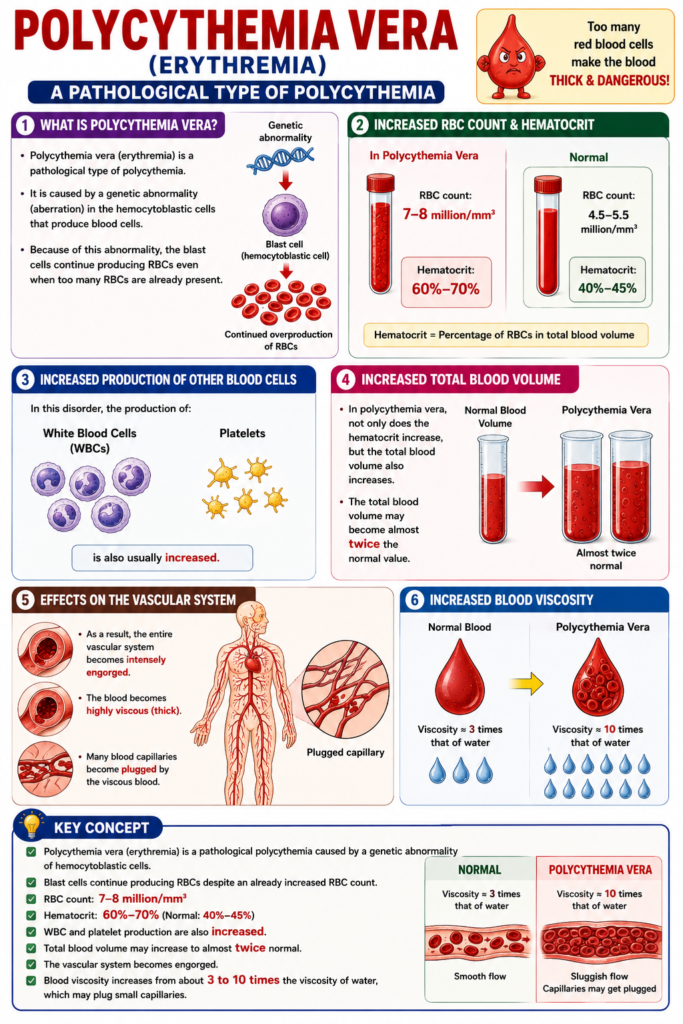
Polycythemia vera (erythremia) is a pathological type of polycythemia.It is caused by a genetic abnormality (aberration) in the hemocytoblastic cells that produce blood cells.
Because of this abnormality, the blast cells continue producing RBCs even when too many RBCs are already present.
In polycythemia vera , the RBC count may increase to 7–8 million/mm³ .
The hematocrit may increase to 60%–70% .
The normal hematocrit is 40%–45% .
In this disorder, the production of:White blood cells (WBCs) Platelets
In polycythemia vera, not only does the hematocrit increase , but the total blood volume also increases.
The total blood volume may become almost twice the normal value .
As a result, the entire vascular system becomes intensely engorged .
The blood becomes highly viscous (thick) .
Many blood capillaries become plugged by the viscous blood.
Normally, blood viscosity is about 3 times the viscosity of water.
In polycythemia vera, blood viscosity may increase to about 10 times the viscosity of water.
KEY CONCEPT
Polycythemia vera (erythremia) is a pathological polycythemia caused by a genetic abnormality of hemocytoblastic cells .Blast cells continue producing RBCs despite an already increased RBC count.
RBC count: 7–8 million/mm³ Hematocrit: 60%–70% (Normal: 40%–45% )WBC and platelet production are also increased.Total blood volume may increase to almost twice normal .The vascular system becomes engorged .
Blood viscosity increases from about 3 to 10 times the viscosity of water, which may plug small capillaries .
Effect of Polycythemia on Function of the Circulatory System
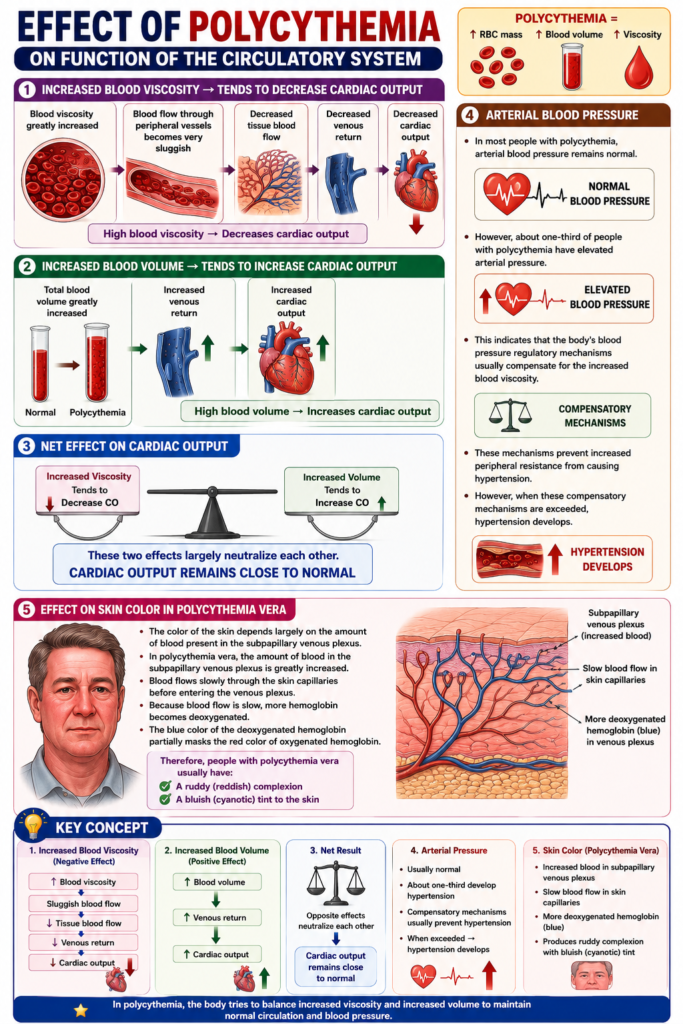
In polycythemia , blood viscosity is greatly increased .
Because the blood is more viscous, blood flow through the peripheral blood vessels becomes very sluggish .
Increased blood viscosity decreases tissue blood flow .
Reduced tissue blood flow decreases venous return .
Reduced venous return decreases cardiac output .
However, in polycythemia, the total blood volume is greatly increased .
The increased blood volume increases venous return .
The increased blood volume also increases cardiac output .
Therefore, in polycythemia:
Increased blood viscosity tends to decrease cardiac output .
Increased blood volume tends to increase cardiac output .
These two effects largely neutralize each other .
As a result, cardiac output remains close to normal .
In most people with polycythemia, arterial blood pressure remains normal .
However, about one-third of people with polycythemia have elevated arterial pressure .
This indicates that the body’s blood pressure regulatory mechanisms usually compensate for the increased blood viscosity.
These mechanisms prevent increased peripheral resistance from causing hypertension.
However, when these compensatory mechanisms are exceeded, hypertension develops .
The color of the skin depends largely on the amount of blood present in the subpapillary venous plexus .
In polycythemia vera , the amount of blood in the subpapillary venous plexus is greatly increased .
Blood flows slowly through the skin capillaries before entering the venous plexus.
Because blood flow is slow, more hemoglobin becomes deoxygenated .
The blue color of the deoxygenated hemoglobin partially masks the red color of oxygenated hemoglobin.
Therefore, people with polycythemia vera usually have:
A ruddy (reddish) complexion
A bluish (cyanotic) tint to the skin
KEY CONCEPT
Increased blood viscosity in polycythemia causes sluggish blood flow .
High blood viscosity:
Decreases tissue blood flow
Decreases venous return
Decreases cardiac output
Increased blood volume:
Increases venous return
Increases cardiac output
These opposite effects keep cardiac output near normal .
Arterial pressure is usually normal, but about one-third of patients develop hypertension when compensatory mechanisms fail.In polycythemia vera , increased blood in the subpapillary venous plexus and increased deoxygenated hemoglobin produce a ruddy complexion with a bluish (cyanotic) tint .
Post navigation