Acidosis Occurs When the HCO₃⁻/CO₂ Ratio Decreases
- According to the Henderson-Hasselbalch equation, acidosis develops when the HCO₃⁻/CO₂ ratio decreases, causing the pH to fall.
- If the ratio decreases because HCO₃⁻ concentration falls, the condition is called metabolic acidosis.
- If the pH decreases because PCO₂ increases, the condition is called respiratory acidosis.
Equation (Henderson-Hasselbalch)
\boxed{\textbf{pH = 6.1 + \log \left(\frac{HCO_3^-}{0.03 \times PCO_2}\right)}}
Conceptual Solution
- ↓ HCO₃⁻ → ↓ HCO₃⁻/CO₂ ratio → ↓ pH = Metabolic Acidosis
- ↑ PCO₂ → ↓ HCO₃⁻/CO₂ ratio → ↓ pH = Respiratory Acidosis
Acidosis Decreases HCO₃⁻/H⁺ Ratio in Renal Tubular Fluid
- Both respiratory acidosis and metabolic acidosis decrease the HCO₃⁻/H⁺ ratio in the renal tubular fluid.
- As a result, there is excess H⁺ in the renal tubules.
- This causes complete reabsorption of all filtered HCO₃⁻.
- Extra H⁺ remains available to combine with the urinary buffers:
- NH₄⁺ (ammonium)
- HPO₄²⁻ (phosphate buffer)
- Therefore, during acidosis:
- All filtered HCO₃⁻ is reabsorbed.
- New HCO₃⁻ is added to the extracellular fluid through the formation of:
- NH₄⁺
- Titratable acid
Metabolic Acidosis
- In metabolic acidosis, H⁺ becomes greater than HCO₃⁻ in the tubular fluid.
- This mainly occurs because:
- Extracellular HCO₃⁻ concentration decreases.
- Glomerular filtration of HCO₃⁻ decreases.
Respiratory Acidosis
- In respiratory acidosis, excess H⁺ in the tubular fluid occurs mainly because:
- Extracellular PCO₂ increases.
- The increased PCO₂ stimulates H⁺ secretion by the renal tubules.
Chronic Acidosis
- During chronic acidosis, whether respiratory or metabolic, the kidneys produce more NH₄⁺.
- Increased NH₄⁺ formation further:
- Increases H⁺ excretion.
- Adds new HCO₃⁻ to the extracellular fluid.
- In severe chronic acidosis:
- Up to 500 mEq/day of H⁺ can be excreted in urine.
- Most H⁺ is excreted as NH₄⁺.
- This also adds up to 500 mEq/day of new HCO₃⁻ to the blood.
Role of the Kidneys in Correcting Acidosis
- Increased tubular H⁺ secretion removes excess H⁺ from the body.
- At the same time, the kidneys increase extracellular HCO₃⁻ concentration.
- This increases the HCO₃⁻ component of the bicarbonate buffer system.
- According to the Henderson-Hasselbalch equation, increased HCO₃⁻ helps:
- Increase extracellular pH.
- Correct acidosis.
- If the acidosis is metabolic, the lungs provide additional compensation by:
- Reducing PCO₂, which also helps correct acidosis.
Table 31.3
- Table 31.3 summarizes the extracellular fluid characteristics of:
- Respiratory acidosis
- Metabolic acidosis
- Respiratory alkalosis
- Metabolic alkalosis
Respiratory Acidosis (Table 31.3)
- pH decreases.
- Extracellular H⁺ concentration increases.
- PCO₂ increases (primary cause).
- The compensatory response is:
- Increased plasma HCO₃⁻.
- The kidneys add new HCO₃⁻ to the extracellular fluid.
- Increased HCO₃⁻ helps offset the increased PCO₂.
- Plasma pH moves back toward normal.
Metabolic Acidosis (Table 31.3)
- pH decreases.
- Extracellular H⁺ concentration increases.
- The primary abnormality is:
- Decreased plasma HCO₃⁻.
- Primary compensatory responses include:
- Increased ventilation, which decreases PCO₂.
- Renal compensation, which adds new HCO₃⁻ to the extracellular fluid.
- Renal compensation helps reduce the initial fall in extracellular HCO₃⁻ concentration.
Table 31.2 – Plasma or Extracellular Fluid Factors That Increase or Decrease H⁺ Secretion and HCO₃⁻ Reabsorption
Increase H⁺ Secretion and HCO₃⁻ Reabsorption
- ↑ PCO₂
- ↑ H⁺, ↓ HCO₃⁻
- ↓ Extracellular fluid volume
- ↑ Angiotensin II
- ↑ Aldosterone
- Hypokalemia
Decrease H⁺ Secretion and HCO₃⁻ Reabsorption
- ↓ PCO₂
- ↓ H⁺, ↑ HCO₃⁻
- ↑ Extracellular fluid volume
- ↓ Angiotensin II
- ↓ Aldosterone
- Hyperkalemia
KEY CONCEPT
- Acidosis develops when the HCO₃⁻/CO₂ ratio decreases, causing a fall in pH.
- Metabolic acidosis results from ↓ HCO₃⁻, while respiratory acidosis results from ↑ PCO₂.
- During acidosis, the kidneys reabsorb all filtered HCO₃⁻ and excrete excess H⁺ mainly as NH₄⁺ and titratable acid.
- Chronic acidosis increases NH₄⁺ production, allowing excretion of up to 500 mEq/day of H⁺ and addition of up to 500 mEq/day of new HCO₃⁻ to the blood.
- Respiratory acidosis is compensated mainly by increased renal HCO₃⁻ production, while metabolic acidosis is compensated by increased ventilation and renal addition of new HCO₃⁻.
- Figure Number: Not provided in the given prompt.
- Table Numbers Mentioned: Table 31.2 and Table 31.3.
RENAL CORRECTION OF ALKALOSIS—DECREASED TUBULAR SECRETION OF H⁺ AND INCREASED EXCRETION OF HCO₃⁻
- The compensatory responses to alkalosis are the opposite of those seen in acidosis.
- In alkalosis, the HCO₃⁻/CO₂ ratio in the extracellular fluid increases.
- The increased HCO₃⁻/CO₂ ratio causes:
- Increase in pH
- Decrease in H⁺ concentration
- This relationship is explained by the Henderson-Hasselbalch equation.
Equation (Henderson-Hasselbalch)
\boxed{\textbf{pH = 6.1 + \log \left(\frac{HCO_3^-}{0.03 \times PCO_2}\right)}}
Conceptual Solution
- ↑ HCO₃⁻ or ↓ PCO₂ → ↑ HCO₃⁻/CO₂ ratio → ↑ pH = Alkalosis
Alkalosis Increases HCO₃⁻/H⁺ Ratio in Renal Tubular FluidRespiratory Alkalosis
- Table 31.3 shows the extracellular fluid characteristics of respiratory alkalosis and metabolic alkalosis.
- In respiratory alkalosis:
- Extracellular fluid pH increases.
- H⁺ concentration decreases.
- The primary cause is:
- Decreased plasma PCO₂
- Caused by hyperventilation
- Decreased PCO₂ leads to:
- Decreased renal tubular H⁺ secretion
- Because less H⁺ is secreted:
- There is not enough H⁺ to react with all the filtered HCO₃⁻.
- Therefore:
- Some filtered HCO₃⁻ is not reabsorbed.
- The excess HCO₃⁻ is excreted in the urine.
- This causes:
- Decrease in plasma HCO₃⁻ concentration
- Correction of alkalosis
- Thus, the compensatory response to respiratory alkalosis is:
- Increased renal excretion of HCO₃⁻
- Reduced plasma HCO₃⁻ concentration
Metabolic Alkalosis
- In metabolic alkalosis:
- Plasma H⁺ concentration decreases.
- pH increases.
- The primary cause is:
- Increase in extracellular fluid HCO₃⁻ concentration
- This increase is partly compensated by:
- Reduced respiration rate
- Reduced respiration causes:
- Increase in PCO₂
- This helps return extracellular fluid pH toward normal.
- Increased extracellular HCO₃⁻ also:
- Increases the filtered load of HCO₃⁻.
- As a result:
- HCO₃⁻ becomes greater than secreted H⁺ in the renal tubular fluid.
- The excess HCO₃⁻:
- Cannot react with H⁺
- Cannot be reabsorbed
- Is excreted in the urine
- The primary compensation in metabolic alkalosis is:
- Increased renal HCO₃⁻ excretion
- This helps compensate for the initial increase in extracellular HCO₃⁻ concentration.
- A reduced ventilation rate may also provide a weak compensatory response by increasing PCO₂.
KEY CONCEPT
- In alkalosis, the HCO₃⁻/CO₂ ratio increases, causing increased pH and decreased H⁺ concentration.
- In both respiratory and metabolic alkalosis, the HCO₃⁻/H⁺ ratio increases in renal tubular fluid.
- Excess HCO₃⁻ cannot be completely reabsorbed and is excreted in urine.
- Respiratory alkalosis is caused by ↓ PCO₂ (hyperventilation) and is compensated by increased renal HCO₃⁻ excretion.
- Metabolic alkalosis is caused by ↑ HCO₃⁻ concentration and is compensated mainly by increased renal HCO₃⁻ excretion, with a minor contribution from reduced ventilation.
Clinical Causes of Acid–Base Disorders
Respiratory Acidosis Results From Decreased Ventilation and Increased PCO₂
- Any factor that decreases pulmonary ventilation causes PCO₂ to increase in the extracellular fluid.
- Increased PCO₂ causes:
- Increase in H₂CO₃ (carbonic acid)
- Increase in H⁺ concentration
- This results in acidosis.
- Because the acidosis is caused by a respiratory problem, it is called respiratory acidosis.
- Respiratory acidosis can occur due to diseases that:
- Damage the respiratory centers.
- Reduce the lungs’ ability to remove CO₂.
- Damage to the respiratory center in the medulla oblongata can cause respiratory acidosis.
- Respiratory acidosis can also result from:
- Obstruction of the respiratory airways.
- Pneumonia.
- Emphysema.
- Decreased pulmonary membrane surface area.
- Any condition that interferes with gas exchange between blood and alveolar air.
- The compensatory responses in respiratory acidosis are:
- Body fluid buffers.
- Kidneys, which require several days for compensation.
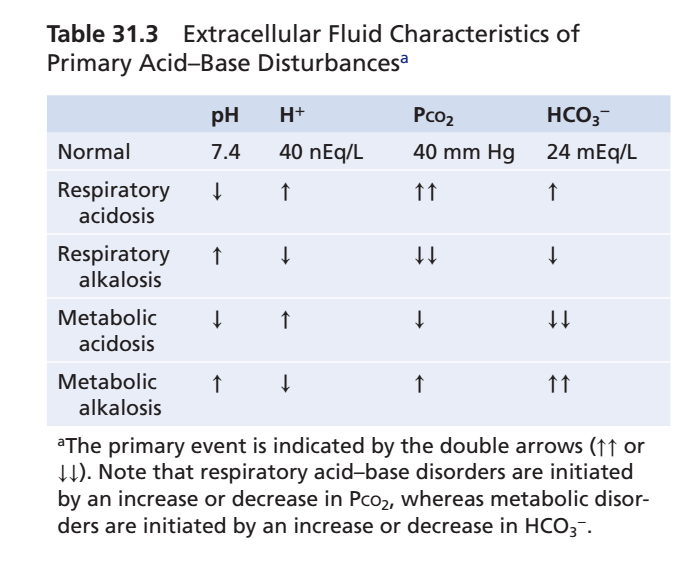
Table 31.3 – Extracellular Fluid Characteristics of Primary Acid–Base Disturbances
| Condition | pH | H⁺ | PCO₂ | HCO₃⁻ |
|---|---|---|---|---|
| Normal | 7.4 | 40 nEq/L | 40 mm Hg | 24 mEq/L |
| Respiratory Acidosis | ↓ | ↑ | ↑↑ (Primary Event) | ↑ |
| Respiratory Alkalosis | ↑ | ↓ | ↓↓ (Primary Event) | ↓ |
| Metabolic Acidosis | ↓ | ↑ | ↓ | ↓↓ (Primary Event) |
| Metabolic Alkalosis | ↑ | ↓ | ↑ | ↑↑ (Primary Event) |
Important Note
- Double arrows (↑↑ or ↓↓) indicate the primary abnormality.
- Respiratory acid–base disorders begin with a change in PCO₂.
- Metabolic acid–base disorders begin with a change in HCO₃⁻.
Respiratory Alkalosis Results From Increased Ventilation and Decreased PCO₂
- Respiratory alkalosis is caused by excessive ventilation.
- It rarely occurs due to physical disease.
- A psychoneurosis may increase breathing enough to produce respiratory alkalosis.
- A physiological type of respiratory alkalosis occurs at high altitude.
- At high altitude:
- Low oxygen stimulates respiration.
- Increased respiration causes excessive loss of CO₂.
- Mild respiratory alkalosis develops.
- The major compensatory mechanisms are:
- Chemical buffers of body fluids.
- Kidneys, which increase HCO₃⁻ excretion.
Metabolic Acidosis Results From Decreased Extracellular Fluid HCO₃⁻ Concentration
- Metabolic acidosis includes all types of acidosis except those caused by excess CO₂.
- Metabolic acidosis can result from:
- Failure of the kidneys to reabsorb HCO₃⁻ and excrete metabolic acids normally.
- Formation of excessive metabolic acids in the body.
- Addition of metabolic acids by ingestion or infusion.
- Loss of base (HCO₃⁻) from body fluids.
Renal Tubular Acidosis
- Renal tubular acidosis occurs because of:
- Defective renal H⁺ secretion.
- Defective HCO₃⁻ reabsorption.
- Or both.
- Two major types are:
- Impaired renal tubular HCO₃⁻ reabsorption, causing loss of HCO₃⁻ in urine.
- Failure of renal tubular H⁺ secretion, causing alkaline urine.
- As a result:
- Too little titratable acid is excreted.
- Too little NH₄⁺ is excreted.
- Acid accumulates in the body fluids.
- Causes of renal tubular acidosis include:
- Chronic renal failure.
- Insufficient aldosterone secretion (Addison disease).
- Hereditary disorders affecting tubular function.
- Acquired disorders affecting tubular function.
- Fanconi syndrome.
Diarrhea
- Severe diarrhea is probably the most common cause of metabolic acidosis.
- It causes loss of large amounts of sodium bicarbonate in the feces.
- Gastrointestinal secretions normally contain large amounts of HCO₃⁻.
- Loss of HCO₃⁻ in diarrhea has the same effect as losing HCO₃⁻ in urine.
- Severe metabolic acidosis from diarrhea can be life-threatening, especially in young children.
Vomiting of Intestinal Contents
- Vomiting only gastric contents causes:
- Loss of acid.
- Tendency toward alkalosis.
- Vomiting large amounts of intestinal contents causes:
- Loss of HCO₃⁻.
- Metabolic acidosis, similar to diarrhea.
Diabetes Mellitus
- Diabetes mellitus results from:
- Lack of insulin secretion (Type 1 diabetes).
- Insufficient insulin action due to decreased sensitivity (Type 2 diabetes).
- Without adequate insulin:
- Normal glucose metabolism is impaired.
- Fat is broken down to produce acetoacetic acid.
- Acetoacetic acid is used by tissues for energy.
- In severe diabetes mellitus:
- Blood acetoacetic acid levels become very high.
- Severe metabolic acidosis develops.
- To compensate:
- Large amounts of acid are excreted in urine.
- Acid excretion may reach 500 mmol/day.
Ingestion of Acids
- Large amounts of acids are rarely consumed in normal food.
- Severe metabolic acidosis may occur after ingestion of acidic poisons.
- Examples include:
- Some acetylsalicylic compounds (aspirin).
- Methyl alcohol, which is converted into formic acid after metabolism.
Chronic Renal Failure
- Marked reduction in kidney function causes:
- Accumulation of weak acid anions in body fluids.
- Reduced excretion of these acids by the kidneys.
- Decreased glomerular filtration rate also:
- Reduces phosphate excretion.
- Reduces NH₄⁺ excretion.
- Decreases the amount of new HCO₃⁻ returned to the body fluids.
- Therefore, chronic renal failure can produce severe metabolic acidosis.
KEY CONCEPT
- Respiratory acidosis results from ↓ ventilation → ↑ PCO₂ → ↑ H₂CO₃ → ↑ H⁺ → Acidosis.
- Respiratory acidosis may be caused by medullary respiratory center damage, airway obstruction, pneumonia, emphysema, decreased pulmonary membrane surface area, or impaired gas exchange.
- Respiratory alkalosis results from ↑ ventilation → ↓ PCO₂, commonly due to hyperventilation or high altitude.
- Metabolic acidosis occurs due to ↓ HCO₃⁻ from kidney failure, excess acid production, acid ingestion, or bicarbonate loss.
- Common causes of metabolic acidosis include renal tubular acidosis, diarrhea, vomiting of intestinal contents, diabetes mellitus, acid poisoning, and chronic renal failure.
- Table Number Mentioned: Table 31.3.
Metabolic Alkalosis Results From Increased Extracellular Fluid HCO₃⁻ Concentration
- Metabolic alkalosis occurs due to:
- Excess retention of HCO₃⁻
- Loss of H⁺ from the body
- Metabolic alkalosis is less common than metabolic acidosis.
- Some important causes of metabolic alkalosis are described below.
Administration of Diuretics (Except Carbonic Anhydrase Inhibitors)
- All diuretics increase the flow of fluid through the renal tubules.
- They usually increase fluid flow in the:
- Distal tubules
- Collecting tubules
- Increased tubular flow causes:
- Increased Na⁺ reabsorption from these nephron segments.
- Sodium reabsorption is coupled with H⁺ secretion.
- Therefore, increased Na⁺ reabsorption also causes:
- Increased H⁺ secretion
- Increased HCO₃⁻ reabsorption
- Diuretics also reduce extracellular fluid volume.
- Reduced extracellular fluid volume is associated with:
- Increased Angiotensin II (Ang II) formation
- Increased aldosterone secretion
- Both Ang II and aldosterone stimulate:
- H⁺ secretion
- HCO₃⁻ reabsorption
- These changes produce metabolic alkalosis.
- Metabolic alkalosis is characterized by:
- Increased extracellular fluid HCO₃⁻ concentration
Excess Aldosterone
- Excess secretion of aldosterone by the adrenal glands causes mild metabolic alkalosis.
- Aldosterone promotes:
- Extensive Na⁺ reabsorption from the distal and collecting tubules.
- At the same time, aldosterone stimulates:
- H⁺ secretion
- HCO₃⁻ reabsorption
- These effects occur through the intercalated cells of the collecting tubules.
- Increased H⁺ secretion and HCO₃⁻ reabsorption result in:
- Metabolic alkalosis
Vomiting of Gastric Contents
- Vomiting only the gastric contents causes loss of:
- Hydrochloric acid (HCl) secreted by the stomach mucosa.
- The net effect is:
- Loss of acid from the extracellular fluid
- Development of metabolic alkalosis
- This type of alkalosis occurs especially in:
- Neonates with pyloric stenosis
- Pyloric stenosis is caused by:
- Hypertrophy of the pyloric sphincter muscles
Ingestion of Alkaline Drugs
- A common cause of metabolic alkalosis is the ingestion of alkaline drugs.
- An example is:
- Sodium bicarbonate
- Sodium bicarbonate is commonly used to treat:
- Gastritis
- Peptic ulcer
- Excess ingestion of sodium bicarbonate can cause:
- Metabolic alkalosis
KEY CONCEPT
- Metabolic alkalosis results from ↑ HCO₃⁻ retention or loss of H⁺.
- Diuretics (except carbonic anhydrase inhibitors) increase Na⁺ reabsorption, H⁺ secretion, and HCO₃⁻ reabsorption, leading to metabolic alkalosis.
- Reduced extracellular fluid volume caused by diuretics increases Ang II and aldosterone, which further stimulate H⁺ secretion and HCO₃⁻ reabsorption.
- Excess aldosterone promotes Na⁺ reabsorption, H⁺ secretion, and HCO₃⁻ reabsorption, causing metabolic alkalosis.
- Vomiting of gastric contents causes loss of HCl, producing metabolic alkalosis.
- Excess sodium bicarbonate ingestion for treatment of gastritis or peptic ulcer can also cause metabolic alkalosis.
Treatment of Acidosis or Alkalosis
- The best treatment for acidosis or alkalosis is to correct the underlying cause of the disorder.
- Treating the underlying cause is often difficult in:
- Chronic lung diseases.
- Kidney failure.
- In these situations, different agents can be used to neutralize excess acid or excess base in the extracellular fluid.
Treatment of Acidosis
- Excess acid can be neutralized by giving large amounts of sodium bicarbonate by mouth.
- Sodium bicarbonate is:
- Absorbed from the gastrointestinal tract into the blood.
- Increases the HCO₃⁻ component of the bicarbonate buffer system.
- Increased HCO₃⁻ helps:
- Increase pH toward normal.
- Sodium bicarbonate can also be given:
- Intravenously (IV).
- Intravenous sodium bicarbonate may produce potentially dangerous physiological effects.
- Therefore, other substances are often preferred, such as:
- Sodium lactate
- Sodium gluconate
- In the body:
- Lactate is metabolized.
- Gluconate is metabolized.
- After metabolism:
- Sodium remains in the extracellular fluid as sodium bicarbonate.
- This increases:
- Extracellular HCO₃⁻
- pH toward normal
Treatment of Alkalosis
- Ammonium chloride can be given by mouth to treat alkalosis.
- After absorption into the blood:
- The ammonia portion is converted by the liver into urea.
- This reaction releases:
- Hydrochloric acid (HCl)
- The released HCl:
- Immediately reacts with body fluid buffers.
- Shifts the H⁺ concentration toward the acidic direction.
- Ammonium chloride may also be given:
- Intravenously (IV).
- Intravenous NH₄⁺ can be dangerous because:
- NH₄⁺ is highly toxic.
- The most appropriate treatment is:
- Correction of the underlying cause of alkalosis.
- Example:
- If metabolic alkalosis is associated with extracellular fluid volume depletion, but not heart failure:
- Infusion of isotonic saline solution is often helpful.
- If metabolic alkalosis is associated with extracellular fluid volume depletion, but not heart failure:
- Isotonic saline infusion helps:
- Correct metabolic alkalosis.
KEY CONCEPT
- The best treatment for acid–base disorders is to treat the underlying cause.
- Acidosis can be treated with oral or intravenous sodium bicarbonate, or with sodium lactate and sodium gluconate, which are converted into sodium bicarbonate in the body.
- Alkalosis can be treated with oral ammonium chloride, which is converted to urea and releases HCl, increasing H⁺ concentration.
- Intravenous ammonium chloride is used cautiously because NH₄⁺ is highly toxic.
- In metabolic alkalosis with extracellular fluid volume depletion (without heart failure), isotonic saline infusion is often effective.
Clinical Measurements and Analysis of Acid–Base Disorders
- Choosing the correct treatment for an acid–base disorder requires an accurate diagnosis.
- Simple acid–base disorders can be diagnosed by measuring three values from an arterial blood sample:
- pH
- Plasma HCO₃⁻ concentration
- PCO₂
Diagnosis of Simple Acid–Base Disorders
- Diagnosis follows several steps, as shown in Figure 31.11.
Step 1: Measure pH
- Measure the arterial blood pH.
- If pH < 7.4, the disorder is acidosis.
- If pH > 7.4, the disorder is alkalosis.
Step 2: Measure PCO₂ and HCO₃⁻
- Measure:
- Plasma PCO₂
- Plasma HCO₃⁻ concentration
- Normal values are:
- PCO₂ = 40 mm Hg
- HCO₃⁻ = 24 mEq/L
Diagnosis of Respiratory Acidosis
- If pH is low, the disorder is acidosis.
- If PCO₂ is increased, there is a respiratory component.
- After renal compensation:
- Plasma HCO₃⁻ increases above normal.
- Therefore, simple respiratory acidosis is characterized by:
- ↓ pH
- ↑ PCO₂
- ↑ Plasma HCO₃⁻ (after partial renal compensation)
Diagnosis of Metabolic Acidosis
- Metabolic acidosis also shows:
- ↓ Plasma pH
- The primary abnormality is:
- ↓ Plasma HCO₃⁻ concentration
- If low pH is associated with low HCO₃⁻, there is a metabolic component.
- In simple metabolic acidosis:
- PCO₂ decreases because of partial respiratory compensation.
- This differs from respiratory acidosis, where PCO₂ increases.
- Therefore, simple metabolic acidosis is characterized by:
- ↓ pH
- ↓ Plasma HCO₃⁻
- ↓ PCO₂ (after partial respiratory compensation)
Diagnosis of Alkalosis
- The diagnosis of alkalosis follows the same basic steps.
- First, identify:
- ↑ Plasma pH
- If increased pH is associated with:
- ↓ PCO₂, there is a respiratory component.
- ↑ HCO₃⁻, there is a metabolic component.
Diagnosis of Respiratory Alkalosis
- Simple respiratory alkalosis is characterized by:
- ↑ pH
- ↓ PCO₂
- ↓ Plasma HCO₃⁻
Diagnosis of Metabolic Alkalosis
- Simple metabolic alkalosis is characterized by:
- ↑ pH
- ↑ Plasma HCO₃⁻
- ↑ PCO₂
KEY CONCEPT
- Diagnosis of simple acid–base disorders requires three arterial blood measurements:
- pH
- Plasma HCO₃⁻
- PCO₂
- Step 1: Determine whether the disorder is acidosis (pH < 7.4) or alkalosis (pH > 7.4).
- Step 2: Compare PCO₂ and HCO₃⁻ with normal values:
- PCO₂ = 40 mm Hg
- HCO₃⁻ = 24 mEq/L
- Respiratory acidosis: ↓ pH, ↑ PCO₂, ↑ HCO₃⁻ (after renal compensation).
- Metabolic acidosis: ↓ pH, ↓ HCO₃⁻, ↓ PCO₂ (after respiratory compensation).
- Respiratory alkalosis: ↑ pH, ↓ PCO₂, ↓ HCO₃⁻.
- Metabolic alkalosis: ↑ pH, ↑ HCO₃⁻, ↑ PCO₂.
- Figure 31.11.
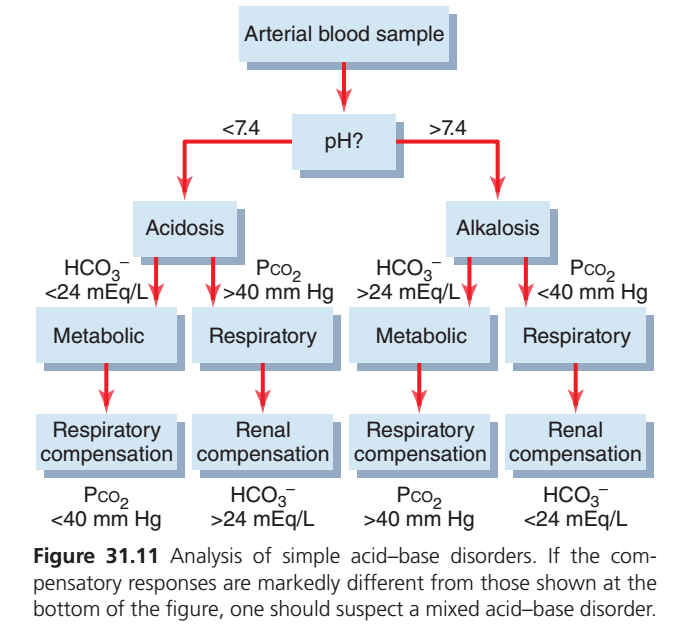
Figure 31.11: Simple Acid–Base Disorders (Guyton) — The Easiest Concept
This flowchart is simply a step-by-step method to identify which acid–base disorder a patient has using three values from an arterial blood sample:
- pH
- HCO₃⁻ (Bicarbonate)
- PCO₂ (Carbon dioxide pressure)
Think of it as 3 simple questions.
STEP 1: Look at the pH
Ask:
Is the pH less than 7.4?
➡ YES → Acidosis
(The blood is too acidic.)
Is the pH greater than 7.4?
➡ YES → Alkalosis
(The blood is too alkaline.)
STEP 2: Find the Cause
Now ask:
Which value is abnormal?
There are only two possibilities:
- HCO₃⁻ problem → Metabolic
- PCO₂ problem → Respiratory
A. If pH < 7.4 (Acidosis)
Option 1
HCO₃⁻ < 24 mEq/L
↓
The kidneys have lost bicarbonate or acid has increased.
➡ Metabolic Acidosis
Examples
- Diarrhea
- Kidney failure
- Diabetic ketoacidosis
Compensation
The lungs try to remove acid by blowing off CO₂.
Therefore
PCO₂ becomes LOW (<40 mmHg)
This is called
Respiratory Compensation
Easy Memory
Low HCO₃⁻
↓
Metabolic Acidosis
↓
Lungs compensate
↓
Low PCO₂
Option 2
PCO₂ >40 mmHg
↓
Too much CO₂ is retained.
➡ Respiratory Acidosis
Examples
- COPD
- Asthma attack
- Respiratory depression
Compensation
The kidneys retain bicarbonate.
Therefore
HCO₃⁻ becomes HIGH (>24 mEq/L)
This is called
Renal Compensation
Easy Memory
High CO₂
↓
Respiratory Acidosis
↓
Kidneys save HCO₃⁻
↓
High HCO₃⁻
B. If pH >7.4 (Alkalosis)
Option 1
HCO₃⁻ >24 mEq/L
↓
Too much bicarbonate.
➡ Metabolic Alkalosis
Examples
- Vomiting
- Excess antacids
- Diuretics
Compensation
The lungs retain CO₂.
Therefore
PCO₂ becomes HIGH (>40 mmHg)
This is
Respiratory Compensation
Easy Memory
High HCO₃⁻
↓
Metabolic Alkalosis
↓
Lungs retain CO₂
↓
High PCO₂
Option 2
PCO₂ <40 mmHg
↓
Too much CO₂ is lost.
➡ Respiratory Alkalosis
Examples
- Hyperventilation
- Anxiety
- High altitude
Compensation
The kidneys excrete bicarbonate.
Therefore
HCO₃⁻ becomes LOW (<24 mEq/L)
This is
Renal CompensationEasy Memory
Low CO₂
↓
Respiratory Alkalosis
↓
Kidneys remove HCO₃⁻
↓
Low HCO₃⁻
One-Page Summary Table
| pH | Primary Change | Diagnosis | Compensation |
|---|---|---|---|
| ↓ (<7.4) | ↓ HCO₃⁻ | Metabolic Acidosis | ↓ PCO₂ (lungs) |
| ↓ (<7.4) | ↑ PCO₂ | Respiratory Acidosis | ↑ HCO₃⁻ (kidneys) |
| ↑ (>7.4) | ↑ HCO₃⁻ | Metabolic Alkalosis | ↑ PCO₂ (lungs) |
| ↑ (>7.4) | ↓ PCO₂ | Respiratory Alkalosis | ↓ HCO₃⁻ (kidneys) |
Super Easy Memory Trick
ROME = Respiratory Opposite, Metabolic Equal
Respiratory Disorders
- PCO₂ ↑ → pH ↓ (Opposite directions)
- PCO₂ ↓ → pH ↑
Metabolic Disorders
- HCO₃⁻ ↓ → pH ↓ (Same direction)
- HCO₃⁻ ↑ → pH ↑
Compensation Rule
If the problem starts in the lungs (Respiratory disorder)
➡ Kidneys compensate by changing HCO₃⁻.
Respiratory → Kidneys
If the problem starts in the kidneys/metabolism (Metabolic disorder)
➡ Lungs compensate by changing PCO₂.
Metabolic → Lungs
Final Exam Shortcut (3-Step Algorithm)
- Check pH
- < 7.4 = Acidosis
- > 7.4 = Alkalosis
- Find the primary abnormality
- HCO₃⁻ abnormal → Metabolic disorder
- PCO₂ abnormal → Respiratory disorder
- Check compensation
- Metabolic disorders → Lungs change PCO₂
- Respiratory disorders → Kidneys change HCO₃⁻
Important (Guyton Figure 31.11): If the compensatory response is much greater or much less than expected, suspect a mixed acid–base disorder, meaning more than one acid–base problem is present simultaneously.
Complex Acid–Base Disorders and Use of Acid–Base Nomogram for Diagnosis
Mixed Acid–Base Disorder
- A patient with low pH is classified as having acidosis.
- If the acidosis is metabolic:
- Plasma HCO₃⁻ decreases.
- PCO₂ should decrease because of respiratory compensation.
- If low pH and low HCO₃⁻ are associated with:
- High PCO₂, there is also a respiratory component.
- Therefore, the disorder is classified as:
- Mixed acidosis
- Example:
- Diarrhea causes metabolic acidosis.
- Emphysema causes respiratory acidosis.
- Together they produce a mixed acid–base disorder.
Figure 31.11 – Analysis of Simple Acid–Base Disorders
- Figure 31.11 outlines the steps for analyzing simple acid–base disorders.
- If compensatory responses are markedly different from those shown in the figure:
- Suspect a mixed acid–base disorder.
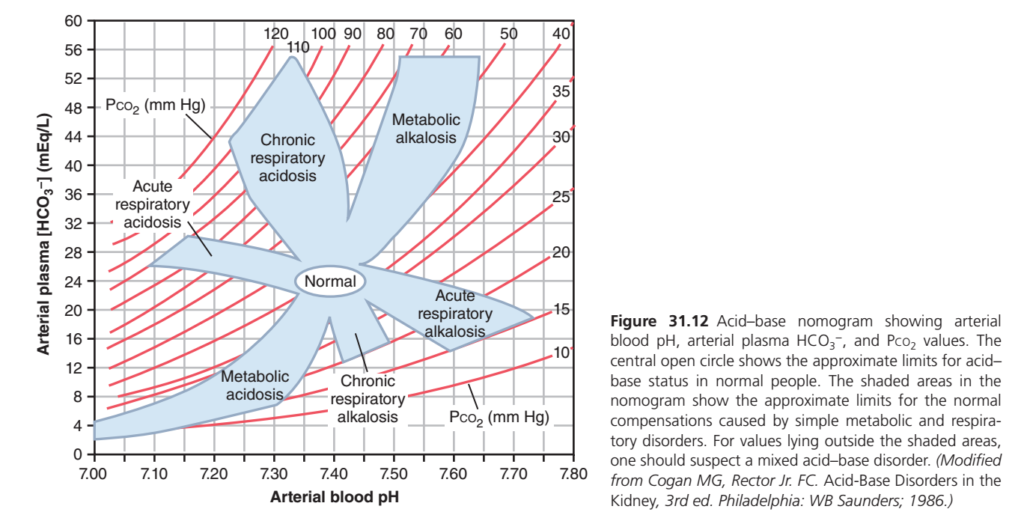
Acid–Base Nomogram
- An acid–base nomogram is a convenient tool for diagnosing acid–base disorders.
- It is shown in Figure 31.12.
- The nomogram helps determine:
- Type of acidosis or alkalosis
- Severity of the disorder
- In the nomogram:
- pH
- HCO₃⁻ concentration
- PCO₂
- These values intersect according to the Henderson-Hasselbalch equation.
- The central open circle represents:
- Normal values
- Normal range
- The shaded areas represent:
- 95% confidence limits
- Normal compensation for simple metabolic and respiratory disorders.
Using the Acid–Base Nomogram
- The nomogram should be used only after enough time has passed for full compensation.
- Required compensation times are:
- 6–12 hours for respiratory compensation in primary metabolic disorders.
- 3–5 days for metabolic compensation in primary respiratory disorders.
- If the patient’s values lie:
- Within the shaded area → Suggests a simple acid–base disorder.
- Outside the shaded area → Suggests a mixed acid–base disorder.
- A value inside the shaded area does not always guarantee a simple acid–base disorder.
- Even with this limitation, the nomogram provides a quick method to determine:
- Type
- Severity
- Of an acid–base disorder.
Example 1
Given Values
- pH = 7.30
- Plasma HCO₃⁻ = 12.0 mEq/L
- PCO₂ = 25 mm Hg
Interpretation
- Low pH → Acidosis
- Low HCO₃⁻ → Metabolic cause
- Low PCO₂ → Respiratory compensation
- Therefore:
- Simple metabolic acidosis
- Appropriate respiratory compensation
- Respiratory compensation reduces:
- PCO₂ from 40 mm Hg (normal) to 25 mm Hg
Example 2
Given Values
- pH = 7.15
- Plasma HCO₃⁻ = 17 mEq/L
- PCO₂ = 50 mm Hg
Interpretation
- Low pH → Acidosis
- Low HCO₃⁻ → Metabolic component
- Normally, respiratory compensation should:
- Decrease PCO₂
- Instead:
- PCO₂ is increased (50 mm Hg)
- Therefore:
- Respiratory compensation is absent.
- A respiratory problem is also present.
- Diagnosis:
- Mixed acid–base disorder
- Metabolic acidosis + Respiratory acidosis
Clinical Importance of the Acid–Base Nomogram
- The acid–base nomogram provides a quick assessment of:
- Type of acid–base disorder.
- Severity of the disorder.
- Possible causes of abnormal:
- pH
- PCO₂
- Plasma HCO₃⁻
- In clinical practice, diagnosis should also consider:
- Patient history
- Physical examination findings
- These provide additional clues about:
- Cause
- Treatment
- Of acid–base disorders.
KEY CONCEPT
- A mixed acid–base disorder occurs when two or more causes produce the acid–base disturbance.
- In metabolic acidosis, low HCO₃⁻ should normally be accompanied by low PCO₂ due to respiratory compensation.
- Low pH + low HCO₃⁻ + high PCO₂ indicates mixed metabolic and respiratory acidosis.
- Figure 31.11 is used to analyze simple acid–base disorders.
- Figure 31.12 is the acid–base nomogram, which helps determine the type and severity of acid–base disorders.
- The nomogram assumes complete compensation:
- 6–12 hours for respiratory compensation.
- 3–5 days for renal (metabolic) compensation.
- Values within the shaded area usually suggest a simple disorder, whereas values outside the shaded area suggest a mixed disorder.
- Diagnosis should always be combined with the patient’s history and physical findings.
- Figure Numbers Mentioned: Figure 31.11 and Figure 31.12.
This graph is one of the most important acid–base diagrams in Guyton Physiology. It is called the Acid–Base Nomogram.
Instead of memorizing it, understand it as a map of blood pH. Every point on this graph tells you three things simultaneously:
- Blood pH
- Blood bicarbonate (HCO₃⁻)
- PCO₂ (carbon dioxide pressure)
Once you understand what every line means, the whole graph becomes easy.Step 1. What is this graph showing?
The graph combines three variables into one figure.
Blood pH
+
Plasma HCO₃⁻
+
PCO₂These three determine whether blood is
- Normal
- Acidosis
- Alkalosis
Step 2. X-axis (Horizontal)
The horizontal axis is
Arterial Blood pHRange
7.00 -------------------7.80Normal blood
≈7.40Move LEFT
↓
Blood becomes more acidic
AcidosisMove RIGHT
↓
Blood becomes more alkaline
AlkalosisThink
LEFT = Acid
RIGHT = AlkaliStep 3. Y-axis (Vertical)
Vertical axis shows
Arterial Plasma HCO₃⁻Unit
mEq/LRange
0
↓
60Normal
≈24 mEq/LMove UP
↓
More bicarbonate
↓
More alkaline
Move DOWN
↓
Less bicarbonate
↓
More acidic
Think
Higher HCO₃⁻
=
More Base
Lower HCO₃⁻
=
More AcidStep 4. What are the RED curved lines?
These are PCO₂ lines.
Each red curve represents one constant carbon dioxide level.
Examples
10
15
20
25
30
35
40
50
60
70
80
90
100
110
120 mmHgEach red line means
Every point on that curve has the SAME PCO₂.
Exactly like contour lines on a mountain map.
Suppose blood lies on
PCO₂ =40Every point on that red curve has
PCO₂ =40 mmHgSuppose blood lies on
PCO₂ =80Every point has
PCO₂ =80 mmHgWhy are the PCO₂ lines curved?
Because of the Henderson-Hasselbalch equation.
pH depends on BOTH
HCO₃⁻
and
PCO₂When bicarbonate changes,
the relationship is not linear.
Therefore
the PCO₂ lines become curved.
Step 5. Why do higher PCO₂ lines lie toward the LEFT?
Remember
CO₂ behaves like acid.
More CO₂
↓
More carbonic acid
↓
Lower pHTherefore
Higher PCO₂
↓
Moves blood toward acidosis
↓
Moves LEFT
Example
PCO₂ =20
Blood is more alkaline
PCO₂ =80
Blood is more acidicStep 6. What is the WHITE circle?
The white central oval is
NORMALApproximate normal values
pH =7.40
HCO₃⁻ =24
PCO₂ =40This is where healthy people lie.
Step 7. What are the BLUE shaded regions?
These are the expected compensation zones.
This is the MOST IMPORTANT concept.
Guyton is saying
If the patient’s blood lies inside one shaded area,
it is probably a simple acid–base disorder with normal physiological compensation.
If blood lies
OUTSIDEthese shaded areas,
suspect
Mixed acid-base disorderUnderstanding each BLUE shaded area
1. Metabolic Acidosis
Located
Bottom LeftWhy?
Because
Metabolic acidosis means
HCO₃⁻ decreasesLow bicarbonate
↓
Moves downward
Low bicarbonate also lowers pH
↓
Moves left
Therefore
DOWN
+
LEFTExactly where this shaded region is.
Examples
- Diarrhea
- Renal failure
- DKA
- Lactic acidosis
Notice
This region is broad.
Why?
Because lungs compensate.
Patients
Hyperventilate
↓
Blow off CO₂
↓
PCO₂ decreases
↓
pH partially improves
Different patients compensate slightly differently.
Therefore the shaded region is wide.
2. Metabolic Alkalosis
Located
Upper RightWhy?
Because
HCO₃⁻ increasesHigher bicarbonate
↓
Moves upward
Higher bicarbonate raises pH
↓
Moves right
Exactly what this graph shows.
Examples
- Vomiting
- Diuretics
- Excess bicarbonate
Compensation
Lungs
Hypoventilate
↓
Retain CO₂
↓
PCO₂ increases
↓
Limits alkalosis
3. Acute Respiratory Acidosis
Located
Upper LeftThis means
CO₂ suddenly increasesExamples
- Drug overdose
- Airway obstruction
- Acute COPD attack
Initially
CO₂ rises
↓
pH falls
↓
Moves left
But kidneys have NOT had time to respond.
Therefore
Only a SMALL rise
in bicarbonate
Hence this shaded area stays
Mostly LEFT
Only slightly UP4. Chronic Respiratory Acidosis
Located
Higher UpWhy?
After several days
Kidneys compensate.
They retain
HCO₃⁻Therefore
Compared with acute respiratory acidosis
HCO₃⁻ rises MUCH MORE.
So
Same acidic pH
but
Much higher bicarbonateHence
the shaded region is
Higher upward.
Examples
- Chronic COPD
- Long-standing hypoventilation
Difference between Acute and Chronic Respiratory Acidosis
Acute
CO₂ ↑
Kidney has NO time
↓
Small HCO₃⁻ increaseChronic
CO₂ ↑
Kidney compensates
↓
Large HCO₃⁻ increaseThat is why
The chronic shaded area sits ABOVE the acute one.
5. Acute Respiratory Alkalosis
Located
Lower RightWhy?
CO₂ suddenly falls.
Examples
- Anxiety attack
- Pain
- Early high altitude
CO₂ decreases
↓
pH increases
↓
Moves right
Kidney has not yet compensated
↓
Only small bicarbonate decrease
Therefore
Slight downward movement.
6. Chronic Respiratory Alkalosis
Located
Lower MiddleAfter several days
Kidneys remove bicarbonate.
↓
HCO₃⁻ falls a lot.
Therefore
Compared with acute respiratory alkalosis
This region extends further downward.
Examples
- Living at high altitude
- Chronic hyperventilation
Acute vs Chronic Respiratory Alkalosis
Acute
CO₂↓
Small HCO₃⁻ fallChronic
CO₂↓
Large HCO₃⁻ fall
because kidneys compensateWhy are the shaded regions wide instead of thin?
Because compensation is not identical in every patient.
Age, kidney function, lung function, disease severity, and timing all affect the exact degree of compensation. The blue areas therefore represent an expected range, not a single line.
Why is there no overlap between all disorders?
Each disorder changes the body in a characteristic direction:
- Metabolic disorders primarily change HCO₃⁻ (vertical movement), with respiratory compensation following.
- Respiratory disorders primarily change PCO₂ (movement across the red isopleths), with slower renal compensation changing HCO₃⁻.
These different primary disturbances create the six distinct shaded regions.
The Most Important Clinical Rule (Guyton)
If the patient’s values fall inside one blue shaded region → think of a single acid–base disorder with appropriate compensation.
If the patient’s values fall outside all the blue shaded regions → suspect a mixed acid–base disorder (two or more disorders occurring together).
Examples:
- Metabolic acidosis plus respiratory alkalosis
- Metabolic alkalosis plus respiratory acidosis
Easy Memory Trick
| Region | pH | HCO₃⁻ | Primary Problem |
|---|---|---|---|
| Center | Normal | Normal | Healthy |
| Bottom Left | ↓ | ↓ | Metabolic acidosis |
| Upper Right | ↑ | ↑ | Metabolic alkalosis |
| Upper Left (slight ↑ HCO₃⁻) | ↓ | Slight ↑ | Acute respiratory acidosis |
| Upper Left (large ↑ HCO₃⁻) | ↓ | Large ↑ | Chronic respiratory acidosis |
| Lower Right | ↑ | Slight ↓ | Acute respiratory alkalosis |
| Lower Middle | ↑ | Large ↓ | Chronic respiratory alkalosis |
One-Sentence Concept
Think of this nomogram as a GPS map for acid–base disorders:
- Horizontal movement (left ↔ right) tells you how acidic or alkaline the blood is (pH).
- Vertical movement (up ↕ down) tells you how much bicarbonate (HCO₃⁻) is present.
- The red curved lines tell you the PCO₂ level.
- The blue shaded regions show where patients with simple acid–base disorders and normal physiological compensation are expected to fall.
- Any point outside the blue regions strongly suggests a mixed acid–base disorder.
Use of Anion Gap to Diagnose Acid–Base Disorders
- The total concentration of anions and cations in plasma must be equal to maintain electrical neutrality.
- Therefore, there is no true anion gap in plasma.
- However, only a few ions are routinely measured in the clinical laboratory.
- The routinely measured cation is:
- Na⁺ (Sodium)
- The routinely measured anions are:
- Cl⁻ (Chloride)
- HCO₃⁻ (Bicarbonate)
- The anion gap is a diagnostic concept.
- It represents the difference between:
- Unmeasured anions
- Unmeasured cations
Anion Gap Formula
\boxed{\textbf{Anion Gap = [Na^+] – ([HCO_3^-] + [Cl^-])}}
Calculation Given in the Text
Given:
- Na⁺ = 144 mEq/L
- HCO₃⁻ = 24 mEq/L
- Cl⁻ = 108 mEq/L
Solution
Anion Gap=144−(24+108) =144−132 =12 mEq/L
When Does the Anion Gap Increase?
- The anion gap increases when:
- Unmeasured anions increase, or
- Unmeasured cations decrease
Major Unmeasured Cations
- Calcium (Ca²⁺)
- Magnesium (Mg²⁺)
- Potassium (K⁺)
Major Unmeasured Anions
- Albumin
- Phosphate
- Sulfate
- Other organic anions
- Normally:
- Unmeasured anions are greater than unmeasured cations.
- Therefore, the normal anion gap is:
- 8–16 mEq/L
Role of the Anion Gap in Metabolic Acidosis
- The plasma anion gap is mainly used to diagnose:
- Different causes of metabolic acidosis
- In metabolic acidosis:
- Plasma HCO₃⁻ decreases.
- If plasma Na⁺ remains unchanged:
- Another anion must increase to maintain electrical neutrality.
Hyperchloremic Metabolic Acidosis (Normal Anion Gap)
- If Cl⁻ increases by the same amount that HCO₃⁻ decreases:
- The anion gap remains normal.
- This condition is called:
- Hyperchloremic metabolic acidosis
High Anion Gap Metabolic Acidosis
- If the decrease in HCO₃⁻ is not accompanied by an increase in Cl⁻:
- Unmeasured anions increase.
- As a result:
- Anion gap increases.
- Metabolic acidosis caused by excess nonvolatile acids produces:
- Increased plasma anion gap
- Examples of nonvolatile acids include:
- Lactic acid
- Ketoacids
- In these conditions:
- HCO₃⁻ decreases
- Cl⁻ does not increase equally
- Therefore:
- Anion gap increases
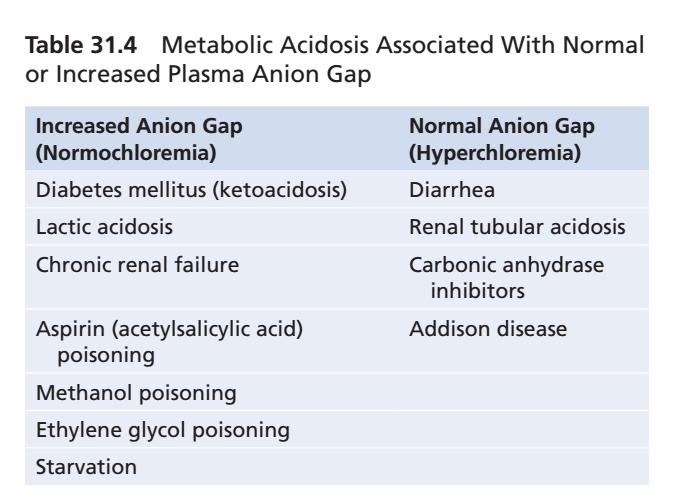
Table 31.4
- Table 31.4 shows examples of:
- Normal anion gap metabolic acidosis
- Increased anion gap metabolic acidosis
- Calculating the anion gap helps narrow the possible causes of metabolic acidosis.
Figure 31.12
- Figure 31.12 shows the acid–base nomogram.
- The nomogram displays:
- Arterial blood pH
- Plasma HCO₃⁻
- PCO₂
- The central open circle represents the normal acid–base range.
- The shaded areas represent the normal compensatory responses to simple metabolic and respiratory disorders.
- Values outside the shaded areas suggest a mixed acid–base disorder.
KEY CONCEPT
- The anion gap is a diagnostic calculation, not a true gap.
- Formula: \boxed{\textbf{Anion Gap = Na^+ – (HCO_3^- + Cl^-)}}
- Using the values in the text:
- 144 − (24 + 108) = 12 mEq/L
- Normal anion gap: 8–16 mEq/L
- Hyperchloremic metabolic acidosis occurs when Cl⁻ increases as HCO₃⁻ decreases, keeping the anion gap normal.
- High anion gap metabolic acidosis occurs when unmeasured anions (e.g., lactic acid, ketoacids) increase, causing the anion gap to rise.
- Calculating the anion gap helps identify the cause of metabolic acidosis.
- Figure 31.12
- Table 31.4