- The kidneys maintain acid–base balance by making the urine either acidic or basic.
- Acidic urine removes acid from the body and decreases acid in the extracellular fluid.
- Basic urine removes base (bicarbonate) from the body and decreases base in the extracellular fluid.
- A large amount of bicarbonate (HCO₃⁻) is continuously filtered into the kidney tubules.
- If this filtered HCO₃⁻ is excreted in urine, the body loses base from the blood.
- Kidney tubular cells also secrete large amounts of H⁺ into the tubular lumen.
- This H⁺ secretion removes acid from the blood.
- If H⁺ secretion is greater than filtered HCO₃⁻, there is a net loss of acid from the extracellular fluid.
- If filtered HCO₃⁻ is greater than H⁺ secretion, there is a net loss of base from the extracellular fluid.
- Every day, the body produces about 80 mEq of nonvolatile strong acids.
- These acids include sulfuric acid, phosphoric acid, and hydrochloric acid.
- They are mainly produced during protein metabolism.
- These acids are called nonvolatile acids because they are not carbonic acid (H₂CO₃).
- Therefore, they cannot be removed by the lungs.
- The kidneys are the main organs that eliminate these acids from the body.
- These strong acids release H⁺ ions.
- The released H⁺ reacts mainly with HCO₃⁻.
- This reaction forms H₂CO₃ (carbonic acid).
- Carbonic acid then breaks down into H₂O and CO₂.
- This reaction buffers the strong acids.
- However, it also reduces extracellular fluid HCO₃⁻ concentration.
- The lost HCO₃⁻ is replaced when the kidneys produce new HCO₃⁻.
- New HCO₃⁻ is formed when H⁺ is excreted with renal tubular buffers, mainly NH₄⁺ and H₂PO₄⁻.
- The kidneys must also prevent HCO₃⁻ loss in urine.
- This function is more important quantitatively than removing nonvolatile acids.
- Each day, the kidneys filter about 4320 mEq of HCO₃⁻.
Mathematical Equation (Solved)
- Filtered HCO₃⁻ = 180 L/day × 24 mEq/L
- = 4320 mEq/day
- Under normal conditions, almost all of this HCO₃⁻ is reabsorbed.
- This preserves the main extracellular fluid buffer system.
- HCO₃⁻ reabsorption and H⁺ excretion both occur through H⁺ secretion by the tubules.
- Before HCO₃⁻ can be reabsorbed, it must first combine with secreted H⁺ to form H₂CO₃.
- Therefore, 4320 mEq of H⁺ must be secreted every day just to reabsorb filtered HCO₃⁻.
- An additional 80 mEq of H⁺ must be secreted daily to eliminate nonvolatile acids.
- Thus, the kidneys secrete a total of 4400 mEq of H⁺ per day into the tubular fluid.
Mathematical Equation (Solved)
- Total H⁺ secretion = 4320 mEq + 80 mEq
- = 4400 mEq/day
- During alkalosis, extracellular fluid H⁺ concentration decreases.
- The kidneys secrete less H⁺.
- They also do not reabsorb all filtered HCO₃⁻.
- As a result, more HCO₃⁻ is excreted in urine.
- Since HCO₃⁻ normally buffers H⁺, losing HCO₃⁻ has the same effect as adding H⁺ to the extracellular fluid.
- Therefore, during alkalosis, H⁺ concentration increases back toward normal.
- During acidosis, extracellular fluid H⁺ concentration increases.
- The kidneys secrete more H⁺.
- They do not excrete HCO₃⁻ in urine.
- Instead, they reabsorb all filtered HCO₃⁻.
- They also produce new HCO₃⁻.
- The new HCO₃⁻ is returned to the extracellular fluid.
- This reduces H⁺ concentration back toward normal.
- The kidneys regulate extracellular fluid H⁺ concentration through three basic mechanisms:
- Secretion of H⁺
- Reabsorption of filtered HCO₃⁻
- Production of new HCO₃⁻
- All three processes occur through the same basic mechanisms, which are explained in the following sections.
Figure Number
- No figure number is mentioned in the provided text.
KEY CONCEPT
- Kidneys maintain acid–base balance by secreting H⁺, reabsorbing filtered HCO₃⁻, and producing new HCO₃⁻.
- 4320 mEq/day of filtered HCO₃⁻ is normally reabsorbed.
- Total daily H⁺ secretion = 4400 mEq/day (4320 + 80).
- Alkalosis: ↓ H⁺ secretion and ↑ HCO₃⁻ excretion.
- Acidosis: ↑ H⁺ secretion, complete HCO₃⁻ reabsorption, and new HCO₃⁻ production.
SECRETION OF H⁺ AND REABSORPTION OF HCO₃⁻ BY THE RENAL TUBULES
- H⁺ secretion and HCO₃⁻ reabsorption occur in almost all parts of the renal tubules.
- These processes do not occur in the descending thin limb and ascending thin limb of the loop of Henle.
- Figure 31.4 summarizes HCO₃⁻ reabsorption along different parts of the renal tubule.
- Remember that for every one HCO₃⁻ reabsorbed, one H⁺ must be secreted.
- About 80%–90% of HCO₃⁻ reabsorption and H⁺ secretion occurs in the proximal tubule.
- Therefore, only a small amount of HCO₃⁻ reaches the distal tubules and collecting ducts.
- In the thick ascending limb of the loop of Henle, about 10% of the filtered HCO₃⁻ is reabsorbed.
- The remaining HCO₃⁻ is reabsorbed in the distal tubules and collecting ducts.
- As explained previously, HCO₃⁻ reabsorption always occurs together with H⁺ secretion.
- However, different parts of the renal tubule use different mechanisms to perform this process.
Figure Number
- Figure 31.4 – Summary of HCO₃⁻ reabsorption along the renal tubule.
KEY CONCEPT
- H⁺ secretion and HCO₃⁻ reabsorption occur in almost all nephron segments, except the descending and ascending thin limbs of the loop of Henle.
- For every 1 HCO₃⁻ reabsorbed, 1 H⁺ is secreted.
- 80–90% of HCO₃⁻ is reabsorbed in the proximal tubule.
- About 10% is reabsorbed in the thick ascending limb of the loop of Henle.
- The remaining HCO₃⁻ is reabsorbed in the distal tubules and collecting ducts.
- Figure 31.4 is mentioned in the provided text.
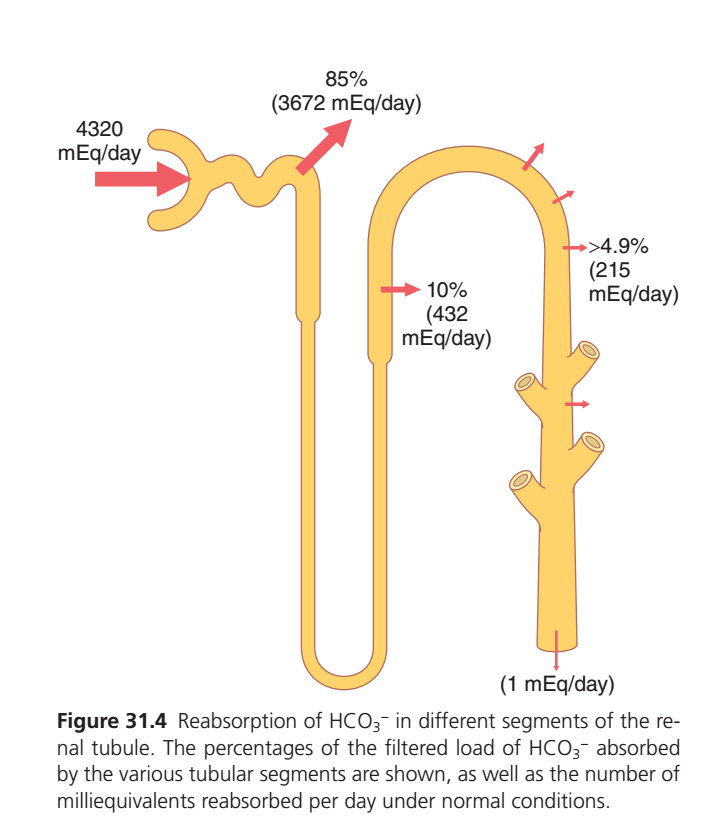
Figure 31.4: Reabsorption of HCO₃⁻ in Different Segments of the Renal Tubule
- (Figure 31.4) shows how filtered bicarbonate (HCO₃⁻) is reabsorbed by different parts of the nephron under normal conditions.
Understanding the Figure
This figure follows the path of bicarbonate (HCO₃⁻) as it moves through the nephron.
The red arrows pointing outward represent:
➡ HCO₃⁻ being reabsorbed back into the blood.
The amount left inside the tubule becomes smaller and smaller as the filtrate flows through the nephron.
Step 1: Glomerulus (Beginning of the Nephron)
Filtered Load
4320 mEq/day
This means:
- Every day, the kidneys filter about 4320 mEq of HCO₃⁻ from the blood into the nephron.
- At this point,
100% of filtered bicarbonate is still inside the tubular fluid.
Nothing has been reabsorbed yet.Step 2: Proximal Tubule
Reabsorbed Amount
85% (3672 mEq/day)
Mathematical Calculation
Filtered bicarbonate = 4320 mEq/day
Reabsorbed = 85%4320×10085=3672 mEq/day
Solved Answer = 3672 mEq/day
Meaning
The proximal tubule reabsorbs the largest amount of bicarbonate.
Out of 4320 mEq/day,
3672 mEq/day returns to the blood.
Only4320−3672=648
648 mEq/day
remain in the tubular fluid.
Step 3: Loop of Henle
Reabsorbed Amount
10% (432 mEq/day)
Mathematical Calculation
4320×10010=432
Solved Answer = 432 mEq/day
Meaning
The Loop of Henle reabsorbs another 432 mEq/day.
After this,
Remaining bicarbonate:648−432=216
216 mEq/day
remain inside the nephron.
Step 4: Distal Tubule and Collecting Tubule
Reabsorbed Amount
About 4.9% (215 mEq/day)
Mathematical Calculation
4320×1004.9=211.68
The figure gives the rounded physiological value:
≈215 mEq/day
Meaning
The distal nephron reabsorbs almost all of the bicarbonate that is still present.
After this,
Remaining bicarbonate:216−215=1
1 mEq/day
remains.
Step 5: Final Urine
Excreted Amount
1 mEq/day
Meaning
Only about
1 mEq/day
of bicarbonate is normally lost in urine.
This means
Almost all filtered bicarbonate is reabsorbed.
Total Reabsorption
Add all reabsorbed amounts.
Proximal Tubule
3672 mEq/day
Loop of Henle
432 mEq/day
Distal Tubule & Collecting Tubule
215 mEq/day
=3672+432+215=4319
Total Reabsorbed = 4319 mEq/day
Filtered amount:
4320 mEq/day
Urinary loss:
1 mEq/day4320−4319=1
Final Urinary Excretion = 1 mEq/day
Easy Flow of the Figure
Glomerulus
4320 mEq/day filtered
↓
Proximal Tubule
Reabsorbs 85%
3672 mEq/day
↓
Remaining
648 mEq/day
↓
Loop of Henle
Reabsorbs 10%
432 mEq/day
↓
Remaining
216 mEq/day
↓
Distal Tubule & Collecting Duct
Reabsorbs about 4.9%
215 mEq/day
↓
Remaining
1 mEq/day
↓
Urine
Only 1 mEq/day of bicarbonate is excreted
Why is the Proximal Tubule the Biggest Contributor?
The figure shows that the proximal tubule performs most of the bicarbonate reabsorption.
It alone reabsorbs:
85%
which is the largest share of filtered bicarbonate.
Why is Urinary Loss So Small?
The kidneys try to conserve bicarbonate, because it is the major extracellular buffer.
Therefore,
almost 100% of filtered bicarbonate is reclaimed, and only about 1 mEq/day is normally excreted.
One-Line Memory Trick
Filtered → 4320 mEq/day
⬇
Proximal Tubule → 85% (3672 mEq/day)
⬇
Loop of Henle → 10% (432 mEq/day)
⬇
Distal Tubule & Collecting Duct → 4.9% (215 mEq/day)
⬇
Urine → 1 mEq/day
KEY CONCEPT
- Figure 31.4 shows the reabsorption of filtered bicarbonate (HCO₃⁻) along different parts of the nephron.
- 4320 mEq/day of bicarbonate is filtered by the glomeruli.
- Proximal tubule: Reabsorbs 85% = 3672 mEq/day.
- Loop of Henle: Reabsorbs 10% = 432 mEq/day.
- Distal tubule and collecting duct: Reabsorb about 4.9% ≈ 215 mEq/day.
- Total bicarbonate reabsorbed = 4319 mEq/day.
- Only about 1 mEq/day of bicarbonate is normally excreted in the urine, showing that the kidneys almost completely conserve filtered bicarbonate.
H⁺ Is Secreted Mainly By Secondary Active Transport in Early Tubular Segments
Figure Mentioned: Fig. 31.4 and Fig. 31.5
- The proximal tubule, thick ascending limb of the loop of Henle, and early distal tubule secrete H⁺ into the tubular fluid.
- Fig. 31.5 shows that H⁺ is secreted by Na⁺-H⁺ counter-transport.
- This is a secondary active transport mechanism.
- H⁺ secretion is coupled with Na⁺ entry into the tubular cell.
- The Na⁺-H⁺ exchanger protein in the luminal membrane carries out this transport.
- The energy for H⁺ secretion comes from the Na⁺ concentration gradient.
- The Na⁺ gradient is created by the Na⁺-K⁺ ATPase pump in the basolateral membrane.
Easy Concept
Na⁺-K⁺ ATPase Pump
↓
Creates Na⁺ gradient
↓
Na⁺ enters tubular cell
↓
Na⁺-H⁺ exchanger works
↓
H⁺ is secreted into tubular lumen
- About 95% of filtered HCO₃⁻ is reabsorbed by this mechanism.
- About 4000 mEq of H⁺ must be secreted each day for this process.
Mathematical Values
HCO₃⁻ Reabsorbed95%
Daily H⁺ Secreted4000 mEq/day
- This mechanism can lower tubular fluid pH only to about 6.7.
Mathematical Value
Minimum Tubular Fluid pH6.7
- The collecting tubules and collecting ducts make the tubular fluid much more acidic.
- They can lower urine pH to about 4.5.
Mathematical Value
Minimum Urine pH4.5
Easy Concept
Early Tubules
↓
Minimum pH
6.7
Collecting Ducts
↓
Minimum urine pH
4.5
- Proximal tubular epithelial cells also secrete a small amount of H⁺.
- This occurs through an H⁺-ATPase pump.
- The H⁺-ATPase is located in the luminal membrane.
- This pump contributes only a small percentage of total H⁺ secretion.
Easy Concept
Two H⁺ Secretion Mechanisms
- Na⁺-H⁺ Exchanger → Major mechanism
- H⁺-ATPase → Minor mechanism
- Fig. 31.5 shows how H⁺ secretion causes HCO₃⁻ reabsorption.
Step 1: CO₂ Enters the Tubular Cell
- CO₂ diffuses into the tubular cell.
- CO₂ may also be produced by tubular cell metabolism.
Step 2: Carbonic Acid Formation
Biochemical Equation
CO2+H2OCarbonic AnhydraseH2CO3
Easy Concept
CO₂
H₂O
↓
Carbonic Anhydrase
↓
H₂CO₃
Step 3: Carbonic Acid Dissociation
Biochemical Equation
H2CO3→H++HCO3−
Easy Concept
Carbonic Acid
↓
H⁺
HCO₃⁻ep 4: H⁺ Secretion
- H⁺ is secreted into the tubular lumen.
- Secretion occurs through the Na⁺-H⁺ exchanger.
- H⁺ is also secreted by the H⁺-ATPase pump.
Easy Concept
H⁺
↓
Na⁺-H⁺ Exchanger
↓
Tubular Lumen
OR
H⁺
↓
H⁺-ATPase
↓
Tubular Lumen
Step 5: HCO₃⁻ Reabsorption
- HCO₃⁻ formed inside the cell crosses the basolateral membrane.
- HCO₃⁻ enters the renal interstitial fluid.
- HCO₃⁻ then enters the peritubular capillary blood.
Easy Concept
HCO₃⁻
↓
Basolateral Membrane
↓
Renal Interstitial Fluid
↓
Peritubular Capillary Blood
- The net result is that each H⁺ secreted into the tubular lumen allows one HCO₃⁻ to enter the blood.
Easy Concept
1 H+ Secreted=1 HCO3− Returned to Blood
Figure 31.4 (Concept from Provided Text)
Figure Mentioned: Fig. 31.4
Normal HCO₃⁻ Reabsorption
- Proximal Tubule: 85% (3672 mEq/day)
- Thick Ascending Loop of Henle: 10% (432 mEq/day)
- Distal Tubule: 4.9% (215 mEq/day)
- Collecting Tubule/Duct: ≈1 mEq/day
Mathematical Values
Total Filtered HCO₃⁻4320 mEq/day
KEY CONCEPT
- Figures Mentioned: Fig. 31.4 and Fig. 31.5
- Early renal tubules secrete H⁺ mainly by secondary active transport (Na⁺-H⁺ exchanger).
- The Na⁺-K⁺ ATPase pump provides the energy indirectly.
- About 95% of filtered HCO₃⁻ is reabsorbed by this mechanism.
- About 4000 mEq of H⁺ is secreted each day.
- Early tubules lower tubular pH only to 6.7.
- Collecting ducts lower urine pH to about 4.5.
- Carbonic Anhydrase converts CO₂ + H₂O → H₂CO₃.
- H₂CO₃ → H⁺ + HCO₃⁻.
- H⁺ is secreted into the lumen, while HCO₃⁻ enters the blood.
- One H⁺ secreted = One HCO₃⁻ reabsorbed into blood.
Mathematical/Biochemical Equations Solved
- Carbonic Acid Formation
CO2+H2OCarbonic AnhydraseH2CO3
- Carbonic Acid Dissociation
H2CO3→H++HCO3−
- Na⁺-H⁺ Exchange
NaLumen+→Cell⟺HCell+→Lumen
- One-to-One Relationship
1 H+ Secreted=1 HCO3− Reabsorbed
- HCO₃⁻ Reabsorption (Fig. 31.4)
4320 mEq/day
- 85% = 3672 mEq/day (Proximal Tubule)
- 10% = 432 mEq/day (Thick Ascending Limb)
- 4.9% = 215 mEq/day (Distal Tubule)
- ≈1 mEq/day (Collecting Tubule/Duct)
- Minimum Tubular Fluid pH
6.7
- Minimum Urine pH
4.5
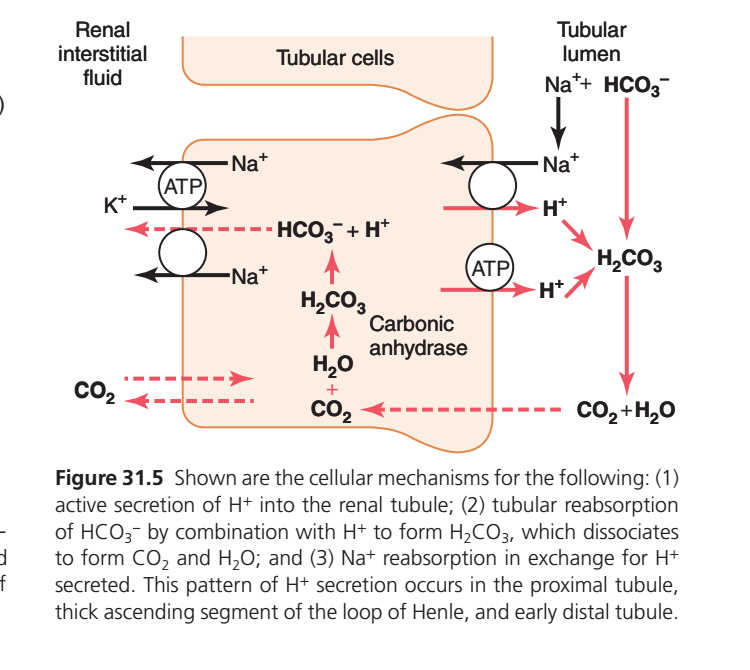
Figure 31.5: Cellular Mechanism of H⁺ Secretion and HCO₃⁻ Reabsorption
- (Figure 31.5) shows the cellular mechanism for:
- Active secretion of H⁺ into the renal tubule.
- Reabsorption of filtered HCO₃⁻ (bicarbonate).
- Reabsorption of Na⁺ in exchange for H⁺ secretion.
- This mechanism occurs in:
- Proximal tubule
- Thick ascending limb of the loop of Henle
- Early distal tubule
Understanding the Parts of the Figure
Top Middle
Tubular Cells
- These are the kidney tubular epithelial cells.
- All transport processes occur inside these cells.
Right Side
Tubular Lumen
- This is the inside of the kidney tubule.
- It contains the filtered fluid (urine filtrate).
Left Side
Renal Interstitial Fluid
- This is the fluid surrounding the tubular cells.
- Reabsorbed substances enter this fluid and then return to the blood.
Step 1: Filtered Sodium (Na⁺) and Bicarbonate (HCO₃⁻) Enter the Tubular Lumen
- Na⁺ and HCO₃⁻ are present in the filtered tubular fluid.
- At this stage,
HCO₃⁻ cannot directly cross the luminal membrane into the tubular cell.
Step 2: H⁺ Is Secreted into the Tubular Lumen
Look at the right cell membrane.
Two transporters secrete H⁺ into the tubular lumen.
A. Na⁺–H⁺ Exchanger
- Na⁺ enters the tubular cell from the tubular lumen.
- At the same time,
H⁺ leaves the cell and enters the tubular lumen.
This is an exchange process.
One Na⁺ enters ↔ One H⁺ leaves.
B. H⁺-ATPase Pump
- Another transporter uses ATP (energy).
- ATP provides energy to pump H⁺ actively into the tubular lumen.
- This is called active H⁺ secretion.
Step 3: Secreted H⁺ Meets Filtered HCO₃⁻
Inside the tubular lumen,
Secreted H⁺ combines with filtered HCO₃⁻.
Reaction
H++HCO3−→H2CO3
Meaning
- Hydrogen ion combines with bicarbonate.
- Carbonic acid (H₂CO₃) is formed.
Step 4: Carbonic Acid Breaks Down
Carbonic acid is unstable.
It rapidly breaks down into:H2CO3→CO2+H2O
Meaning
Carbonic acid becomes:
- Carbon dioxide (CO₂)
- Water (H₂O)
This reaction occurs rapidly in the tubular lumen.
Step 5: CO₂ Diffuses into the Tubular Cell
CO₂ easily crosses the cell membrane.
Therefore,
CO₂ diffuses from the tubular lumen into the tubular cell.
Water also enters.
Step 6: Carbonic Anhydrase Acts Inside the Cell
Inside the tubular cell,
The enzyme carbonic anhydrase catalyzes the reaction:CO2+H2O→H2CO3
Meaning
CO₂ combines with water.
Carbonic acid forms again.
Step 7: Carbonic Acid Dissociates
Carbonic acid immediately dissociates into:H2CO3→H++HCO3−
Meaning
One molecule of carbonic acid produces:
- One H⁺
- One HCO₃⁻
Step 8: H⁺ Is Recycled
The newly formed H⁺ does not stay inside the cell.
It is secreted again into the tubular lumen through:
- Na⁺–H⁺ exchanger
- H⁺-ATPase pump
Therefore,
The same H⁺ is recycled repeatedly.
Step 9: HCO₃⁻ Leaves the Cell
The newly formed HCO₃⁻ leaves the tubular cell through the basolateral membrane.
It enters the:
Renal interstitial fluid
and then returns to the blood.
This is called:
Reabsorption of bicarbonate.
Step 10: Na⁺ Also Leaves the Cell
Na⁺ is pumped out through the Na⁺/K⁺-ATPase pump.
How?
- ATP provides energy.
- 3 Na⁺ are pumped out of the cell.
- 2 K⁺ enter the cell.
This maintains a low intracellular Na⁺ concentration, allowing more Na⁺ to enter from the tubular lumen via the Na⁺–H⁺ exchanger.
Solving the Biological Reactions Step-by-Step
Reaction 1 (In Tubular Lumen)
H++HCO3−→H2CO3
Concept
Secreted H⁺ combines with filtered bicarbonate.
Result:
Carbonic acid forms.
Reaction 2 (In Tubular Lumen)
H2CO3→CO2+H2O
Concept
Carbonic acid breaks into:
- CO₂
- Water
Reaction 3 (Inside Tubular Cell)
CO2+H2OCarbonic AnhydraseH2CO3
Concept
Carbon dioxide and water combine again.
Carbonic acid reforms.
Reaction 4 (Inside Tubular Cell)
H2CO3→H++HCO3−
Concept
Carbonic acid splits into:
- H⁺
- HCO₃⁻
H⁺ is secreted again.
HCO₃⁻ returns to the blood.
Overall Concept
Notice carefully:
- Filtered bicarbonate never actually enters the tubular cell.
Instead,
- It combines with secreted H⁺.
- It becomes CO₂.
- CO₂ enters the cell.
- Inside the cell, a new bicarbonate molecule is formed.
- This newly formed bicarbonate enters the blood.
Thus,
The filtered HCO₃⁻ is effectively reabsorbed, even though it does not cross the luminal membrane directly.
Easy Flow of the Figure
Tubular Lumen
HCO₃⁻ + H⁺
↓
H₂CO₃
↓
CO₂ + H₂O
↓
CO₂ diffuses into the cell
↓
Inside Tubular Cell
CO₂ + H₂O
↓
H₂CO₃
↓
H⁺ + HCO₃⁻
↓
H⁺ → Secreted back into lumen
↓
HCO₃⁻ → Reabsorbed into blood
One-Line Memory Trick
H⁺ is secreted → combines with filtered HCO₃⁻ → forms CO₂ → CO₂ enters the cell → new HCO₃⁻ is formed → HCO₃⁻ returns to the blood, while H⁺ is recycled.
KEY CONCEPT
- Figure 31.5 shows the mechanism of H⁺ secretion, HCO₃⁻ reabsorption, and Na⁺ reabsorption in the proximal tubule, thick ascending limb of the loop of Henle, and early distal tubule.
- H⁺ is secreted into the tubular lumen by the Na⁺–H⁺ exchanger and H⁺-ATPase pump.
- In the tubular lumen: H⁺ + HCO₃⁻ → H₂CO₃ → CO₂ + H₂O.
- CO₂ diffuses into the tubular cell, where carbonic anhydrase catalyzes: CO₂ + H₂O → H₂CO₃ → H⁺ + HCO₃⁻.
- H⁺ is recycled back into the tubular lumen, while the newly formed HCO₃⁻ is reabsorbed into the blood.
- Na⁺ is reabsorbed and transported into the blood by the Na⁺/K⁺-ATPase pump.
Filtered HCO₃⁻ Is Reabsorbed By Interaction with H⁺ in the Tubules
Bicarbonate ions do not readily permeate the luminal membranes of the renal tubular cells; therefore, HCO₃⁻ that is filtered by the glomerulus cannot be directly reabsorbed.
- Filtered HCO₃⁻ cannot directly enter renal tubular cells.
- Therefore, it cannot be reabsorbed directly.
Instead, HCO₃⁻ is reabsorbed by a special process in which it first combines with H⁺ to form H₂CO₃, which eventually becomes CO₂ and H₂O, as shown in Fig. 31.5.
- HCO₃⁻ + H⁺ → H₂CO₃
- H₂CO₃ → CO₂ + H₂O
- This special process reabsorbs bicarbonate.
- Figure: Fig. 31.5
This reabsorption of HCO₃⁻ is initiated by a reaction in the tubules between HCO₃⁻ filtered at the glomerulus and H⁺ secreted by the tubular cells.
- Filtered HCO₃⁻ meets secreted H⁺ in the tubule.
- Their reaction starts bicarbonate reabsorption.
The H₂CO₃ formed then dissociates into CO₂ and H₂O.
- H₂CO₃ → CO₂ + H₂O
The CO₂ can move easily across the tubular membrane; therefore, it instantly diffuses into the tubular cell, where it recombines with H₂O, under the influence of carbonic anhydrase, to generate a new H₂CO₃ molecule.
- CO₂ easily enters the tubular cell.
- Inside the cell:
- CO₂ + H₂O → H₂CO₃
- This reaction is catalyzed by carbonic anhydrase.
This H₂CO₃ dissociates to form HCO₃⁻ and H⁺; the HCO₃⁻ is then transported through the basolateral membrane into the interstitial fluid and is taken up into the peritubular capillary blood.
- H₂CO₃ → HCO₃⁻ + H⁺
- Newly formed HCO₃⁻ leaves the cell.
- It enters the interstitial fluid.
- Then it enters the peritubular capillary blood.
The transport of HCO₃⁻ across the basolateral membrane is facilitated by two mechanisms:
- Na⁺–HCO₃⁻ cotransport → Proximal tubule.
- Cl⁻–HCO₃⁻ exchange → Late proximal tubule, thick ascending loop of Henle, collecting tubules, and collecting ducts.
Thus, each time a H⁺ is formed in the tubular epithelial cells, a HCO₃⁻ is also formed and released back into the blood.
- Formation of 1 H⁺ produces 1 HCO₃⁻.
- The new HCO₃⁻ returns to the blood.
The net effect of these reactions is “reabsorption” of HCO₃⁻ from the tubules, although the HCO₃⁻ that actually enters the extracellular fluid is not the same as that filtered into the tubules.
- Overall result = filtered HCO₃⁻ is reabsorbed.
- The returned HCO₃⁻ is newly formed, not the original filtered bicarbonate.
The reabsorption of filtered HCO₃⁻ does not result in net secretion of H⁺ because the secreted H⁺ combines with the filtered HCO₃⁻ and is therefore not excreted.
- Secreted H⁺ combines with filtered HCO₃⁻.
- Therefore, H⁺ is not lost in urine.
- No net H⁺ secretion occurs.
HCO₃⁻ Is Titrated Against H⁺ in the Tubules.
- Normally, HCO₃⁻ and H⁺ neutralize each other inside the tubules.
Under normal conditions, the rate of tubular H⁺ secretion is about 4400 mEq/day, and the rate of filtration by HCO₃⁻ is about 4320 mEq/day.
- Tubular H⁺ secretion = 4400 mEq/day
- Filtered HCO₃⁻ = 4320 mEq/day
Mathematical Calculation:
- 4400 − 4320 = 80 mEq/day
- Excess H⁺ = 80 mEq/day
Thus, the quantities of these two ions entering the tubules are almost equal, and they combine with each other to form CO₂ and H₂O.
- Nearly equal amounts of H⁺ and HCO₃⁻ enter the tubules.
- They react to form:
- CO₂
- H₂O
Therefore, HCO₃⁻ and H⁺ normally “titrate” each other in the tubules.
- Normally, HCO₃⁻ and H⁺ neutralize each other.
The titration process is not quite exact because there is usually a slight excess of H⁺ in the tubules to be excreted in the urine.
- A small amount of H⁺ remains after titration.
- This excess H⁺ is excreted in urine.
This excess H⁺ (~80 mEq/day) rids the body of nonvolatile acids produced by metabolism.
- About 80 mEq/day of H⁺ removes nonvolatile metabolic acids from the body.
As discussed later, most of this H⁺ is not excreted as free H⁺ but is in combination with other urinary buffers, especially phosphate and ammonia.
- Most H⁺ is not excreted freely.
- It is excreted after combining with:
- Phosphate
- Ammonia
When there is an excess of HCO₃⁻ over H⁺ in the urine, as occurs in metabolic alkalosis, the excess HCO₃⁻ cannot be reabsorbed.
- In metabolic alkalosis:
- HCO₃⁻ > H⁺
- Extra HCO₃⁻ cannot be reabsorbed.
Therefore, the excess HCO₃⁻ remains in the tubules to be excreted into the urine, which helps correct the metabolic alkalosis.
- Excess HCO₃⁻ stays in the tubules.
- It is excreted in urine.
- This helps correct metabolic alkalosis.
In acidosis, there is excess H⁺ relative to HCO₃⁻ in the tubules, causing complete reabsorption of the HCO₃⁻; the excess H⁺ passes into the urine in combination with urinary buffers, especially phosphate and ammonia, and eventually is excreted as salts.
- In acidosis:
- H⁺ > HCO₃⁻
- All filtered HCO₃⁻ is reabsorbed.
- Extra H⁺ combines with:
- Phosphate
- Ammonia
- It is excreted as salts.
Thus, the basic mechanism whereby the kidneys correct acidosis or alkalosis is incomplete titration of H⁺ against HCO₃⁻, leaving one or the other to pass into the urine and be removed from the extracellular fluid.
- Kidneys regulate acid-base balance by incomplete titration of H⁺ and HCO₃⁻.
- The ion left in excess is excreted in urine.
- This removes the excess from the extracellular fluid.
KEY CONCEPT
- Figure: Fig. 31.5
- Filtered HCO₃⁻ is reabsorbed indirectly, not directly.
- HCO₃⁻ + H⁺ → H₂CO₃ → CO₂ + H₂O
- Inside tubular cells: CO₂ + H₂O → H₂CO₃ → HCO₃⁻ + H⁺
- New HCO₃⁻ returns to blood.
- H⁺ secretion = 4400 mEq/day
- Filtered HCO₃⁻ = 4320 mEq/day
- Excess H⁺ = 80 mEq/day
- Metabolic alkalosis: excess HCO₃⁻ is excreted.
- Acidosis: all HCO₃⁻ is reabsorbed, and excess H⁺ is excreted with phosphate and ammonia.
Primary Active Secretion of H⁺ in the Intercalated Cells of Late Distal and Collecting Tubules
Beginning in the late distal tubules and continuing through the remainder of the tubular system, the tubular epithelium secretes H⁺ by primary active transport.
- H⁺ secretion begins in the late distal tubule.
- It continues throughout the remaining tubular system.
- H⁺ is secreted by primary active transport.
The mechanism for primary active H⁺ secretion was discussed in Chapter 28 and is shown in Fig. 31.6.
- The mechanism is explained in Chapter 28.
- Figure: Fig. 31.6
It occurs at the luminal membrane of the tubular cell, where H⁺ is transported directly by specific proteins, a H⁺-ATPase and a hydrogen-potassium-ATPase (H⁺-K⁺-ATPase) transporter.
- H⁺ is secreted across the luminal membrane.
- Two transport proteins are involved:
- H⁺-ATPase
- H⁺-K⁺-ATPase
The energy required for pumping the H⁺ is derived from the breakdown of ATP to adenosine diphosphate.
- ATP provides the energy.
- ATP → ADP + Energy
- This energy pumps H⁺ into the tubular lumen.
Primary active secretion of H⁺ occurs in special types of cells called the type A intercalated cells of the late distal tubules and collecting tubules.
- Primary active H⁺ secretion occurs in:
- Type A intercalated cells
- These cells are present in:
- Late distal tubules
- Collecting tubules
Hydrogen ion secretion in these cells is accomplished in two steps:
- H⁺ secretion occurs in two steps.
(1) The dissolved CO₂ in this cell combines with H₂O to form H₂CO₃.
- CO₂ + H₂O → H₂CO₃
(2) The H₂CO₃ then dissociates into HCO₃⁻, which is reabsorbed into the blood, plus H⁺, which is secreted into the tubule by means of the H⁺-ATPase and the H⁺-K⁺-ATPase transporters.
- H₂CO₃ → HCO₃⁻ + H⁺
- HCO₃⁻ is reabsorbed into the blood.
- H⁺ is secreted into the tubule.
- H⁺ secretion occurs through:
- H⁺-ATPase
- H⁺-K⁺-ATPase
For each H⁺ secreted, a HCO₃⁻ is reabsorbed, similar to the process in the proximal tubules.
- 1 H⁺ secreted = 1 HCO₃⁻ reabsorbed
- This is similar to the proximal tubule.
The main difference is that H⁺ moves across the luminal membrane by an active H⁺ pump instead of mainly by counter-transport, as occurs in the early parts of the nephron.
- In the late distal and collecting tubules:
- H⁺ crosses the luminal membrane by an active H⁺ pump.
- In the early nephron:
- H⁺ is secreted mainly by counter-transport.
Figure 31.6
- Figure: Fig. 31.6
- Type A intercalated cells actively secrete H⁺ through:
- H⁺-ATPase
- H⁺-K⁺-ATPase
- HCO₃⁻ is reabsorbed into the blood.
- K⁺ is reabsorbed during acidosis.
- 1 HCO₃⁻ is reabsorbed for every 1 H⁺ secreted.
- Cl⁻ is passively secreted with H⁺.
Although secretion of H⁺ in the late distal tubules and collecting tubules accounts for only about 5% of the total H⁺ secreted, this mechanism is important in forming maximally acidic urine.
- This segment secretes only about 5% of total H⁺.
- It is essential for producing maximally acidic urine.
Although large amounts of H⁺ are secreted in the proximal tubules, H⁺ concentration can be increased only about 3-fold to 4-fold and the tubular fluid pH can be reduced to only about 6.7 by this nephron segment.
- In the proximal tubules:
- H⁺ concentration increases only 3–4 times.
- Tubular fluid pH decreases only to about 6.7.
However, H⁺ concentration can be increased as much as 900-fold in the collecting tubules.
- In the collecting tubules:
- H⁺ concentration increases up to 900-fold.
This mechanism decreases the pH of the tubular fluid to about 4.5, which is the lower limit of pH that can be achieved in normal kidneys.
- Tubular fluid pH decreases to about 4.5.
- pH 4.5 is the lowest urine pH that normal kidneys can produce.
KEY CONCEPT
- Figure: Fig. 31.6
- Primary active H⁺ secretion occurs in Type A intercalated cells of the late distal and collecting tubules.
- H⁺ is secreted by H⁺-ATPase and H⁺-K⁺-ATPase using energy from ATP → ADP.
- CO₂ + H₂O → H₂CO₃ → HCO₃⁻ + H⁺
- 1 H⁺ secreted = 1 HCO₃⁻ reabsorbed.
- This mechanism contributes only 5% of total H⁺ secretion but is responsible for producing maximally acidic urine.
- Proximal tubule: 3–4-fold increase in H⁺ concentration; minimum pH ≈ 6.7.
- Collecting tubule: 900-fold increase in H⁺ concentration; minimum pH ≈ 4.5.
COMBINATION OF EXCESS H⁺ WITH PHOSPHATE AND AMMONIA BUFFERS IN THE TUBULE GENERATES “NEW” HCO₃⁻
When H⁺ is secreted in excess of the HCO₃⁻ filtered into the tubular fluid, only a small part of the excess H⁺ can be excreted in the ionic form in the urine.
- When H⁺ > filtered HCO₃⁻:
- Only a small amount of free H⁺ can be excreted in urine.
This is because the minimal urine pH is about 4.5, corresponding to an H⁺ concentration of 10⁻⁴⋅⁵ mEq/L, or 0.03 mEq/L.
- Lowest urine pH = 4.5
- At pH 4.5:
- H⁺ concentration = 10⁻⁴⋅⁵ mEq/L
- = 0.03 mEq/L
Thus, for each liter of urine formed, a maximum of only about 0.03 mEq of free H⁺ can be excreted.
- 1 liter of urine can excrete only:
- 0.03 mEq of free H⁺
To excrete the 80 mEq of nonvolatile acid formed by metabolism each day, about 2667 liters of urine would have to be excreted if the H⁺ remained free in solution.
- Daily nonvolatile acid produced:
- 80 mEq/day
Mathematical Calculation:
- Urine required = 80 ÷ 0.03
- = 2666.7 L
- ≈ 2667 liters of urine/day
The excretion of large amounts of H⁺ (on occasion as much as 500 mEq/day) in the urine is accomplished primarily by combining H⁺ with buffers in the tubular fluid.
- Large amounts of H⁺ can be excreted by:
- Combining H⁺ with urinary buffers
- H⁺ excretion can reach:
- 500 mEq/day
The most important buffers are phosphate buffer and ammonia buffer.
- Main urinary buffers:
- Phosphate buffer
- Ammonia buffer
Other weak buffer systems, such as urate and citrate, are much less important.
- Less important buffers:
- Urate
- Citrate
When H⁺ is titrated in the tubular fluid with HCO₃⁻, this leads to reabsorption of one HCO₃⁻ for each H⁺ secreted, as discussed earlier.
- H⁺ + HCO₃⁻ react in the tubule.
- 1 H⁺ secreted = 1 HCO₃⁻ reabsorbed
However, when there is excess H⁺ in the tubular fluid, it combines with buffers other than HCO₃⁻, and this leads to generation of new HCO₃⁻ that can also enter the blood.
- When H⁺ is in excess:
- It combines with phosphate or ammonia instead of HCO₃⁻.
- This generates new HCO₃⁻.
- The new HCO₃⁻ enters the blood.
Thus, when there is excess H⁺ in the extracellular fluid, the kidneys not only reabsorb all the filtered HCO₃⁻ but also generate new HCO₃⁻, thereby helping replenish the HCO₃⁻ lost from the extracellular fluid in acidosis.
- In acidosis:
- Kidneys reabsorb all filtered HCO₃⁻.
- Kidneys also produce new HCO₃⁻.
- This replaces the HCO₃⁻ lost from the extracellular fluid.
In the next two sections, we discuss the mechanisms whereby phosphate and ammonia buffers contribute to generation of new HCO₃⁻.
- The next sections explain:
- How phosphate buffer generates new HCO₃⁻.
- How ammonia buffer generates new HCO₃⁻.
KEY CONCEPT
- Excess H⁺ cannot be excreted efficiently as free H⁺ because the lowest urine pH is 4.5.
- At pH 4.5, free H⁺ concentration = 0.03 mEq/L.
- 1 liter of urine can excrete only 0.03 mEq of free H⁺.
- 80 ÷ 0.03 = 2666.7 L ≈ 2667 L/day of urine would be required if H⁺ remained free.
- Therefore, H⁺ combines mainly with phosphate and ammonia buffers.
- 1 H⁺ secreted with HCO₃⁻ = 1 HCO₃⁻ reabsorbed.
- Excess H⁺ + phosphate/ammonia buffers = generation of new HCO₃⁻.
- In acidosis, kidneys reabsorb all filtered HCO₃⁻ and generate new HCO₃⁻.
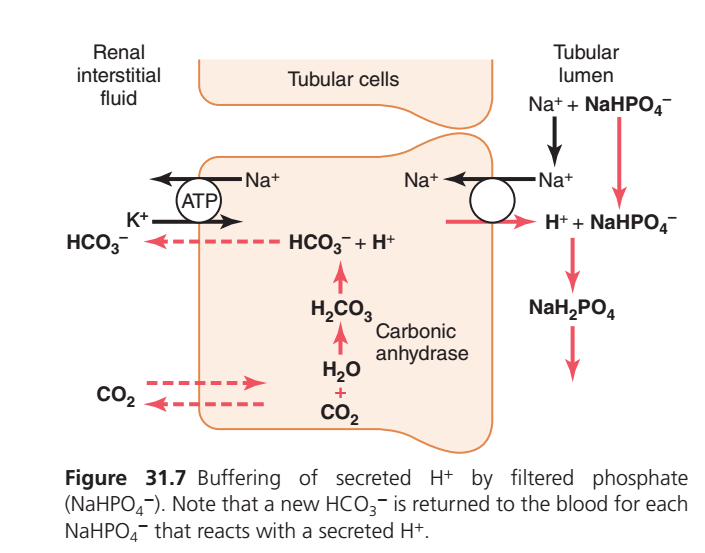
BUFFERING OF SECRETED H⁺ BY FILTERED PHOSPHATE (GUYTON FIGURE 31.7)
ONE-LINE SUMMARY
The kidney secretes H⁺ into the tubular fluid, where it combines with filtered phosphate (NaHPO₄²⁻). This removes H⁺ in the urine and generates one new HCO₃⁻ (bicarbonate) that is added back to the blood.
WHY IS THIS PROCESS IMPORTANT?
The body continuously produces acids.
The kidneys must:
- Remove excess H⁺ from the body.
- Prevent urine from becoming too acidic.
- Replace the bicarbonate (HCO₃⁻) that is lost while buffering acids.
Filtered phosphate acts as a urinary buffer that helps achieve all three goals.
STEP 1: CO₂ ENTERS THE TUBULAR CELL
CO₂ from the blood easily diffuses into the tubular cell.
Inside the cell:
CO₂ + H₂O
↓ (Carbonic Anhydrase)
H₂CO₃
↓
H⁺ + HCO₃⁻Result
One molecule of:
- H⁺ is produced.
- HCO₃⁻ is produced.
STEP 2: H⁺ IS SECRETED INTO THE TUBULAR LUMEN
H⁺ is transported from the tubular cell into the urine by the Na⁺–H⁺ exchanger.
At the same time:
- Na⁺ enters the tubular cell.
Result
H⁺ enters the tubular fluid.
STEP 3: FILTERED PHOSPHATE BUFFERS H⁺
The tubular fluid already contains filtered phosphate.
It is mainly present as:
NaHPO₄²⁻ (disodium hydrogen phosphate)
The secreted H⁺ combines with it:
H⁺ + NaHPO₄²⁻
↓
NaH₂PO₄Result
- H⁺ is trapped.
- It cannot diffuse back into the cell.
- It is excreted safely in urine.
STEP 4: A NEW HCO₃⁻ RETURNS TO THE BLOOD
While H⁺ is excreted:
The HCO₃⁻ formed inside the tubular cell moves into the blood.
Result
Blood gains:
One NEW bicarbonate (HCO₃⁻).
This bicarbonate replaces the bicarbonate that was previously used to buffer acids in the body.
WHAT HAPPENS TO NaH₂PO₄?
After H⁺ binds phosphate:
NaHPO₄²⁻
+
H⁺
↓
NaH₂PO₄NaH₂PO₄ remains in the urine and is excreted.
This is called titratable acid excretion.
WHAT IS THE ROLE OF CARBONIC ANHYDRASE?
Carbonic anhydrase speeds up the reaction:
CO₂ + H₂O
⇌
H₂CO₃
⇌
H⁺ + HCO₃⁻Without this enzyme:
- Less H⁺ would be produced.
- Less HCO₃⁻ would be formed.
- Acid excretion would decrease.
SIMPLE FLOW CHART
CO₂ enters tubular cell
↓
Carbonic anhydrase
↓
CO₂ + H₂O → H₂CO₃
↓
H⁺ + HCO₃⁻
↓ ↓
H⁺ → Tubular lumen HCO₃⁻ → Blood
↓
H⁺ + NaHPO₄²⁻
↓
NaH₂PO₄
↓
Excreted in urineWHAT DOES THE FIGURE TEACH?
Left Side (Blood Side)
- Na⁺/K⁺-ATPase pumps Na⁺ into the blood.
- Newly formed HCO₃⁻ also enters the blood.
- CO₂ freely diffuses into the cell.
Middle (Tubular Cell)
- Carbonic anhydrase produces H⁺ and HCO₃⁻ from CO₂ and H₂O.
Right Side (Tubular Lumen)
- H⁺ is secreted.
- Filtered phosphate buffers H⁺.
- NaH₂PO₄ is excreted in urine.
EXAM PEARL
For every one H⁺ that combines with one phosphate (NaHPO₄²⁻) and is excreted as NaH₂PO₄, one new HCO₃⁻ is added to the blood.
Therefore:
1 H⁺ excreted with phosphate
=
1 New HCO₃⁻ added to bloodEASY MEMORY TRICK
“Phosphate carries H⁺ out, bicarbonate goes back in.”
- Phosphate = Urinary acid carrier
- H⁺ = Excreted in urine
- HCO₃⁻ = Returned to the blood
KEY CONCEPT
Filtered phosphate is an important urinary buffer. Secreted H⁺ combines with NaHPO₄²⁻ to form NaH₂PO₄, which is excreted in urine. At the same time, the bicarbonate produced inside the tubular cell is transported into the blood. Thus, each H⁺ excreted with phosphate generates one new HCO₃⁻, helping the kidneys eliminate acid while replenishing the body’s bicarbonate stores.
Phosphate Buffer System Carries Excess H⁺ Into the Urine and Generates New HCO₃⁻
The phosphate buffer system is composed of HPO₄²⁻ as the proton acceptor (base) and H₂PO₄⁻ as the proton donor (acid).
- HPO₄²⁻ acts as the proton acceptor (base).
- H₂PO₄⁻ acts as the proton donor (acid).
Both become concentrated in the tubular fluid because water is normally reabsorbed to a greater extent than phosphate by the renal tubules.
- Water is reabsorbed more than phosphate.
- Therefore, phosphate becomes more concentrated in the tubular fluid.
Therefore, although phosphate is not an important extracellular fluid buffer, it is much more effective as a buffer in the tubular fluid.
- Phosphate is not an important extracellular fluid buffer.
- It is a very effective buffer in the tubular fluid.
Another factor that makes phosphate important as a tubular buffer is the fact that the pK of this system is about 6.8.
- pK of the phosphate buffer = 6.8
- This makes phosphate an effective tubular buffer.
Under normal conditions, the urine is slightly acidic, and the urine pH is near the pK of the phosphate buffer system.
- Normal urine is slightly acidic.
- Urine pH is close to 6.8.
Therefore, in the tubules, the phosphate buffer system normally functions near its most effective pH range.
- Phosphate buffer works near its maximum effectiveness in the tubules.
Fig. 31.7 shows the sequence of events whereby H⁺ is excreted in combination with phosphate buffer and the mechanism whereby new HCO₃⁻ is added to the blood.
- Figure: Fig. 31.7
- The figure shows:
- H⁺ excretion with phosphate buffer.
- Formation of new HCO₃⁻ that enters the blood.
The process of H⁺ secretion into the tubules is the same as described earlier.
- H⁺ secretion occurs by the same mechanism described previously.
As long as there is excess HCO₃⁻ in the tubular fluid, most of the secreted H⁺ combines with HCO₃⁻.
- When HCO₃⁻ is available:
- Most secreted H⁺ combines with HCO₃⁻.
However, once all the HCO₃⁻ has been reabsorbed and is no longer available to combine with H⁺, any excess H⁺ can combine with HPO₄²⁻ and other tubular buffers.
- After all HCO₃⁻ is reabsorbed:
- Excess H⁺ combines with:
- HPO₄²⁻
- Other tubular buffers
- Excess H⁺ combines with:
After the H⁺ combines with HPO₄²⁻ to form H₂PO₄⁻, it can be excreted as a sodium salt (NaH₂PO₄), carrying with it the excess H⁺.
- H⁺ + HPO₄²⁻ → H₂PO₄⁻
- H₂PO₄⁻ + Na⁺ → NaH₂PO₄
- NaH₂PO₄ is excreted in urine.
- This removes the excess H⁺ from the body.
There is one important difference in this sequence of H⁺ excretion from that discussed previously.
- This mechanism differs from the previous mechanism.
In this case, the HCO₃⁻ that is generated in the tubular cell and enters the peritubular blood represents a net gain of HCO₃⁻ by the blood, rather than merely a replacement of filtered HCO₃⁻.
- The HCO₃⁻ formed in the tubular cell enters the blood.
- It is a net gain of HCO₃⁻.
- It does not simply replace filtered HCO₃⁻.
Therefore, whenever a H⁺ secreted into the tubular lumen combines with a buffer other than HCO₃⁻, the net effect is the addition of a new HCO₃⁻ to the blood.
- If H⁺ combines with buffers other than HCO₃⁻:
- A new HCO₃⁻ is added to the blood.
This process demonstrates one of the mechanisms whereby the kidneys can replenish the extracellular fluid stores of HCO₃⁻.
- This mechanism helps the kidneys:
- Restore extracellular HCO₃⁻ stores.
Under normal conditions, much of the filtered phosphate is reabsorbed, and only 30 to 40 mEq/day are available for buffering H⁺.
- Most filtered phosphate is reabsorbed.
- Only 30–40 mEq/day is available to buffer H⁺.
Therefore, much of the buffering of excess H⁺ in the tubular fluid in acidosis occurs through the ammonia buffer system.
- In acidosis:
- Most excess H⁺ is buffered by the ammonia buffer system.
KEY CONCEPT
- Figure: Fig. 31.7
- HPO₄²⁻ = Base (proton acceptor).
- H₂PO₄⁻ = Acid (proton donor).
- pK of phosphate buffer = 6.8.
- Phosphate is a better buffer in tubular fluid than in extracellular fluid.
- While HCO₃⁻ is present, secreted H⁺ combines with HCO₃⁻.
- After HCO₃⁻ is completely reabsorbed, excess H⁺ combines with HPO₄²⁻.
- H⁺ + HPO₄²⁻ → H₂PO₄⁻ → NaH₂PO₄ (urine).
- Each H⁺ buffered by phosphate results in the addition of one new HCO₃⁻ to the blood.
- Only 30–40 mEq/day of phosphate is available for buffering H⁺, so the ammonia buffer system becomes the major buffer during acidosis.
Excretion of Excess H⁺ and Generation of New HCO₃⁻ By Ammonia Buffer System
A second buffer system in the tubular fluid that is even more important quantitatively than the phosphate buffer system is composed of ammonia (NH₃) and the ammonium ion (NH₄⁺).
- The ammonia buffer system is more important than the phosphate buffer system.
- It consists of:
- Ammonia (NH₃)
- Ammonium ion (NH₄⁺)
Ammonium ion is synthesized from glutamine, which comes mainly from metabolism of amino acids in the liver.
- NH₄⁺ is produced from glutamine.
- Glutamine mainly comes from amino acid metabolism in the liver.
The glutamine delivered to the kidneys is transported into epithelial cells of the proximal tubules, thick ascending limb of the loop of Henle, and distal tubules (Fig. 31.8).
- Glutamine enters epithelial cells of:
- Proximal tubules
- Thick ascending limb of the loop of Henle
- Distal tubules
- Figure: Fig. 31.8
Once inside the cell, each molecule of glutamine is metabolized in a series of reactions to ultimately form two NH₄⁺ and two HCO₃⁻.
- 1 glutamine molecule → 2 NH₄⁺ + 2 HCO₃⁻
The NH₄⁺ is secreted into the tubular lumen by a counter-transport mechanism in exchange for sodium, which is reabsorbed.
- NH₄⁺ is secreted into the tubular lumen.
- It is exchanged with Na⁺, which is reabsorbed.
The HCO₃⁻ is transported across the basolateral membrane, along with the reabsorbed Na⁺, into the interstitial fluid and is taken up by the peritubular capillaries.
- HCO₃⁻ crosses the basolateral membrane.
- It moves with Na⁺ into the interstitial fluid.
- Then it enters the peritubular capillaries.
Thus, for each molecule of glutamine metabolized in the proximal tubules, two NH₄⁺ are secreted into the urine and two HCO₃⁻ are reabsorbed into the blood.
- 1 glutamine molecule produces:
- 2 NH₄⁺ secreted into urine.
- 2 HCO₃⁻ reabsorbed into blood.
The HCO₃⁻ generated by this process constitutes new HCO₃⁻.
- The formed HCO₃⁻ is new HCO₃⁻ added to the blood.
In the collecting tubules, the addition of NH₄⁺ to the tubular fluid occurs through a different mechanism (Fig. 31.9).
- In the collecting tubules, NH₄⁺ is added by a different mechanism.
- Figure: Fig. 31.9
Here, H⁺ is actively secreted by the tubular membrane into the lumen, where it combines with NH₃ to form NH₄⁺, which is then excreted.
- H⁺ is actively secreted into the tubular lumen.
- H⁺ + NH₃ → NH₄⁺
- NH₄⁺ is excreted in urine.
The collecting ducts are permeable to NH₃, which can easily diffuse into the tubular lumen.
- NH₃ easily diffuses into the tubular lumen.
- Collecting ducts are permeable to NH₃.
However, the luminal membrane of this part of the tubules is much less permeable to NH₄⁺; therefore, once the H⁺ has reacted with NH₃ to form NH₄⁺, the NH₄⁺ is trapped in the tubular lumen and eliminated in the urine.
- The luminal membrane is poorly permeable to NH₄⁺.
- After NH₄⁺ is formed:
- It becomes trapped in the tubular lumen.
- It is excreted in urine.
For each NH₄⁺ excreted, a new HCO₃⁻ is generated and added to the blood.
- 1 NH₄⁺ excreted = 1 new HCO₃⁻ added to the blood
KEY CONCEPT
- The ammonia buffer system (NH₃/NH₄⁺) is quantitatively more important than the phosphate buffer system.
- Figure: Fig. 31.8 and Fig. 31.9
- Glutamine enters the proximal tubule, thick ascending limb, and distal tubule.
- 1 glutamine molecule → 2 NH₄⁺ + 2 HCO₃⁻
- 2 NH₄⁺ are secreted into urine.
- 2 HCO₃⁻ are reabsorbed into blood as new HCO₃⁻.
- In the collecting tubule:
- H⁺ + NH₃ → NH₄⁺
- NH₄⁺ becomes trapped in the tubular lumen and is excreted.
- 1 NH₄⁺ excreted = 1 new HCO₃⁻ generated and added to the blood.
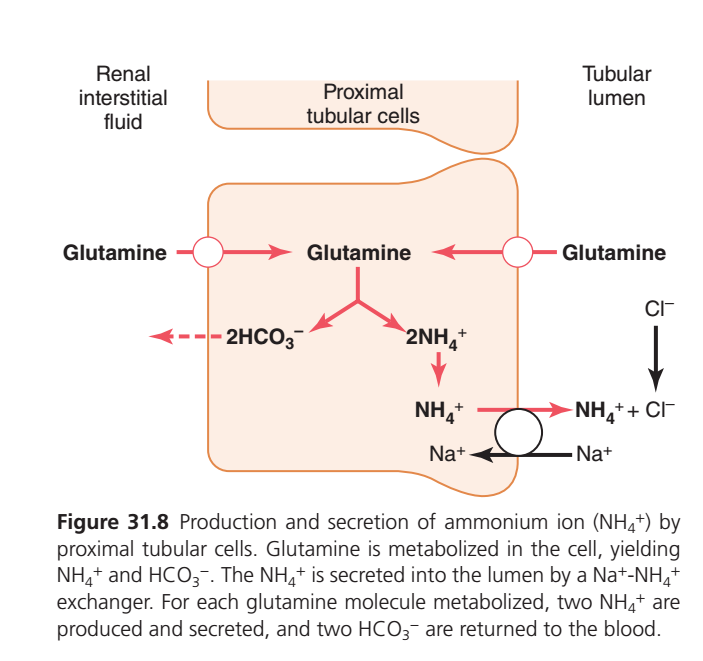
PRODUCTION AND SECRETION OF AMMONIUM (NH₄⁺) BY PROXIMAL TUBULE CELLS (GUYTON FIGURE 31.8)
ONE-LINE SUMMARY
The proximal tubule converts glutamine into NH₄⁺ (to remove acid) and HCO₃⁻ (to replace lost bicarbonate). For every 1 glutamine molecule, 2 NH₄⁺ are excreted in urine and 2 new HCO₃⁻ are added to the blood.
WHY IS THIS PROCESS IMPORTANT?
The phosphate buffer system has a limited capacity.
When the body has excess acid (H⁺), the kidneys use the ammonia (NH₃)/ammonium (NH₄⁺) buffer system, which is the most important mechanism for long-term acid excretion.
Its two major functions are:
- ✅ Remove excess H⁺ from the body.
- ✅ Generate new bicarbonate (HCO₃⁻) for the blood.
STEP 1: GLUTAMINE ENTERS THE PROXIMAL TUBULE CELL
Glutamine comes from:
- Blood (renal interstitial fluid)
- Tubular fluid (filtered glutamine)
Both sources supply glutamine to the proximal tubule cell.
Result
The tubular cell now has glutamine available for metabolism.
STEP 2: GLUTAMINE IS METABOLIZED
Inside the proximal tubule cell:
One glutamine molecule is broken down into:
1 Glutamine
↓
2 NH₄⁺ + 2 HCO₃⁻Result
Two useful products are formed:
- 2 NH₄⁺ (Ammonium ions) → To remove acid
- 2 HCO₃⁻ (Bicarbonate ions) → To replace bicarbonate in blood
STEP 3: NH₄⁺ IS SECRETED INTO THE TUBULAR LUMEN
NH₄⁺ leaves the cell through the Na⁺–NH₄⁺ exchanger.
Normally:
- Na⁺ enters the cell.
- NH₄⁺ moves into the tubular lumen.
Result
NH₄⁺ enters the urine.EP 4: HCO₃⁻ RETURNS TO THE BLOOD
At the same time:
The 2 newly formed HCO₃⁻ leave the tubular cell and enter the renal interstitial fluid (blood).
Result
The blood gains 2 new bicarbonate ions.
This helps restore the body’s buffering capacity.
STEP 5: NH₄⁺ IS EXCRETED IN URINE
In the tubular lumen:
NH₄⁺ combines with chloride (Cl⁻):
NH₄⁺ + Cl⁻
↓
NH₄ClNH₄Cl remains in the urine and is excreted.
Result
The body removes excess acid safely through urine.
WHAT DOES THE FIGURE SHOW?
Left Side (Blood Side)
- Glutamine enters the proximal tubule cell.
- Newly formed 2 HCO₃⁻ move into the blood.
Meaning
Blood gains new bicarbonate.
Middle (Tubular Cell)
Glutamine is metabolized:
Glutamine
↓
2 NH₄⁺ + 2 HCO₃⁻Meaning
One molecule produces:
- 2 ammonium ions
- 2 bicarbonate ions
Right Side (Tubular Lumen)
NH₄⁺ is secreted through the Na⁺–NH₄⁺ exchanger.
Na⁺ enters the cell while NH₄⁺ enters the urine.
NH₄⁺ combines with Cl⁻ and is excreted.SIMPLE FLOW CHART
Glutamine enters proximal tubule cell
↓
Glutamine metabolism
↓
2 NH₄⁺ + 2 HCO₃⁻
↓ ↓
NH₄⁺ → Tubular lumen HCO₃⁻ → Blood
↓
Excreted in urine (as NH₄Cl)WHY IS THIS SYSTEM BETTER THAN THE PHOSPHATE BUFFER?
Phosphate Buffer
- Limited amount of phosphate is filtered.
- Acid excretion is therefore limited.
Ammonia (NH₄⁺) Buffer
- The kidney can produce more NH₄⁺ from glutamine whenever needed, especially during acidosis.
- Therefore, it can excrete much larger amounts of acid.
Result
The ammonia buffer system is the major mechanism for chronic acid excretion.
EXAM PEARL
One Glutamine Molecule Produces:
| Product | Number |
|---|---|
| NH₄⁺ secreted into urine | 2 |
| New HCO₃⁻ added to blood | 2 |
Easy equation:
1 Glutamine
↓
2 NH₄⁺ + 2 HCO₃⁻EASY MEMORY TRICK
“Glutamine gives TWO to urine and TWO to blood.”
- 2 NH₄⁺ → Urine (acid removal)
- 2 HCO₃⁻ → Blood (bicarbonate replacement)
KEY CONCEPT
In the proximal tubule, glutamine metabolism produces two NH₄⁺ and two HCO₃⁻. The NH₄⁺ is secreted into the tubular lumen and excreted in urine, removing acid from the body. Simultaneously, the two newly formed HCO₃⁻ are returned to the blood, replenishing the body’s bicarbonate stores. This ammonia buffer system is the kidney’s most important mechanism for long-term acid excretion.
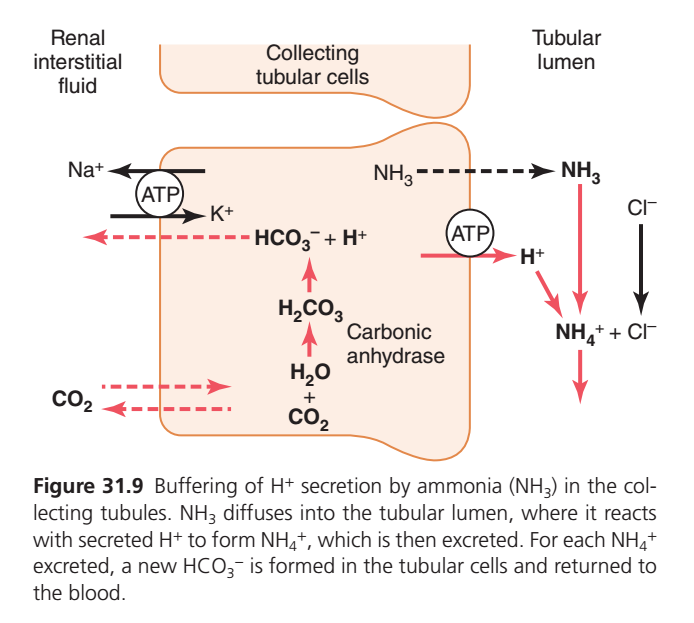
BUFFERING OF H⁺ BY AMMONIA (NH₃) IN THE COLLECTING TUBULE (GUYTON FIGURE 31.9)
ONE-LINE SUMMARY
In the collecting tubule, NH₃ (ammonia) diffuses into the tubular lumen, where it combines with secreted H⁺ to form NH₄⁺ (ammonium). NH₄⁺ becomes trapped in the urine and is excreted, while one new HCO₃⁻ is added to the blood.
WHY IS THIS PROCESS IMPORTANT?
The collecting tubule is the final site for acid excretion.
Here, the kidney:
- ✅ Removes excess H⁺ from the body.
- ✅ Prevents urine from becoming extremely acidic.
- ✅ Produces new HCO₃⁻ for the blood.
Ammonia (NH₃) acts as a buffer by trapping H⁺ in the urine.
STEP 1: CO₂ ENTERS THE COLLECTING TUBULE CELL
CO₂ diffuses from the blood into the collecting tubule cell.
Inside the cell:
CO₂ + H₂O
↓ (Carbonic Anhydrase)
H₂CO₃
↓
H⁺ + HCO₃⁻Result
The cell produces:
- H⁺
- HCO₃⁻
STEP 2: H⁺ IS SECRETED INTO THE TUBULAR LUMEN
An H⁺-ATPase (proton pump) uses ATP to actively pump H⁺ into the tubular lumen.
Result
- H⁺ enters the urine.
- The cell retains the newly formed HCO₃⁻.
STEP 3: NH₃ DIFFUSES INTO THE TUBULAR LUMEN
NH₃ (ammonia) easily diffuses from the collecting tubule cell into the tubular lumen.
Unlike NH₄⁺, NH₃ can freely cross cell membranes.
Result
NH₃ reaches the urine.
STEP 4: NH₃ COMBINES WITH H⁺
Inside the tubular lumen:
NH₃ + H⁺
↓
NH₄⁺Result
- NH₃ captures H⁺.
- NH₄⁺ (ammonium) is formed.
STEP 5: NH₄⁺ IS TRAPPED IN THE URINE
NH₄⁺ cannot easily diffuse back into the tubular cell.
Therefore, it remains in the tubular fluid.
It commonly combines with chloride:
NH₄⁺ + Cl⁻
↓
NH₄ClResult
NH₄Cl is excreted in the urine, removing acid from the body.
STEP 6: NEW HCO₃⁻ RETURNS TO THE BLOOD
While H⁺ is excreted as NH₄⁺:
The HCO₃⁻ produced inside the cell moves into the blood.
Result
The blood gains one new bicarbonate ion (HCO₃⁻).
This helps restore the body’s buffering capacity.
WHAT DOES THE FIGURE SHOW?
Left Side (Blood Side)
- CO₂ enters the collecting tubule cell.
- Newly formed HCO₃⁻ leaves the cell and enters the blood.
- Na⁺/K⁺-ATPase maintains the ionic gradient needed for cell function.
Meaning
The blood receives new bicarbonate (HCO₃⁻).
Middle (Collecting Tubule Cell)
Carbonic anhydrase catalyzes:
CO₂ + H₂O
↓
H₂CO₃
↓
H⁺ + HCO₃⁻Meaning
The cell generates:
- H⁺ for secretion
- HCO₃⁻ for the blood
Right Side (Tubular Lumen)
- H⁺ is actively pumped into the lumen by H⁺-ATPase.
- NH₃ diffuses into the lumen.
- NH₃ combines with H⁺ to form NH₄⁺.
- NH₄⁺ combines with Cl⁻ and is excreted as NH₄Cl.
SIMPLE FLOW CHART
CO₂ enters collecting tubule cell
↓
Carbonic anhydrase
↓
CO₂ + H₂O → H₂CO₃
↓
H⁺ + HCO₃⁻
↓ ↓
H⁺ → Tubular lumen HCO₃⁻ → Blood
↓
NH₃ + H⁺
↓
NH₄⁺
↓
NH₄Cl
↓
Excreted in urineWHY IS NH₃ BETTER THAN PHOSPHATE?
Phosphate Buffer
- Depends on the amount of filtered phosphate.
- Buffering capacity is limited.
Ammonia Buffer
- The kidneys can increase NH₃ production from glutamine during acidosis.
- More NH₃ means more H⁺ can be trapped as NH₄⁺.
- This allows the kidneys to excrete large amounts of acid.
Result
The ammonia buffer system is the most important renal mechanism for long-term acid excretion, especially during chronic acidosis.
EXAM PEARL
For every NH₄⁺ excreted in urine, one new HCO₃⁻ is returned to the blood.
Easy Equation
1 NH₄⁺ Excreted
=
1 New HCO₃⁻ Added to BloodDIFFERENCE BETWEEN FIGURE 31.8 AND FIGURE 31.9
| Figure 31.8 | Figure 31.9 |
|---|---|
| Site: Proximal tubule | Site: Collecting tubule |
| Glutamine is metabolized to produce NH₄⁺ and HCO₃⁻ | NH₃ buffers secreted H⁺ in the lumen |
| NH₄⁺ is directly secreted into the lumen | NH₃ first diffuses into the lumen, then combines with H⁺ to form NH₄⁺ |
| 1 glutamine → 2 NH₄⁺ + 2 HCO₃⁻ | 1 NH₄⁺ excreted → 1 new HCO₃⁻ added to blood |
EASY MEMORY TRICK
“NH₃ goes into the urine, catches H⁺, becomes NH₄⁺, and gets trapped.”
- NH₃ = Free traveler
- H⁺ = Acid
- NH₄⁺ = Trapped and excreted
- HCO₃⁻ = Returned to the blood
KEY CONCEPT
In the collecting tubule, NH₃ diffuses into the tubular lumen and combines with actively secreted H⁺ to form NH₄⁺. Because NH₄⁺ cannot easily diffuse back into the cell, it becomes trapped and is excreted in the urine, removing acid from the body. At the same time, one new HCO₃⁻ produced inside the tubular cell is transported into the blood. Thus, each NH₄⁺ excreted generates one new HCO₃⁻, making the ammonia buffer system the kidney’s most important mechanism for long-term acid excretion.
Chronic Acidosis Increases NH₄⁺ Excretion
One of the most important features of the renal ammonium-ammonia buffer system is that it is subject to physiological control.
- The ammonium-ammonia buffer system is physiologically regulated.
An increase in extracellular fluid H⁺ concentration stimulates renal glutamine metabolism and, therefore, increases formation of NH₄⁺ and new HCO₃⁻ to be used in H⁺ buffering; a decrease in H⁺ concentration has the opposite effect.
- Increase in extracellular H⁺:
- Stimulates glutamine metabolism in the kidneys.
- Increases NH₄⁺ production.
- Increases new HCO₃⁻ formation.
- Enhances H⁺ buffering.
- Decrease in extracellular H⁺:
- Produces the opposite effect.
Under normal conditions, the amount of H⁺ eliminated by the ammonia buffer system accounts for 30% to 50% of the acid excreted and 30% to 50% of the new HCO₃⁻ generated by the kidneys.
- Normally, the ammonia buffer system:
- Eliminates 30–50% of the acid excreted.
- Produces 30–50% of the new HCO₃⁻ generated by the kidneys.
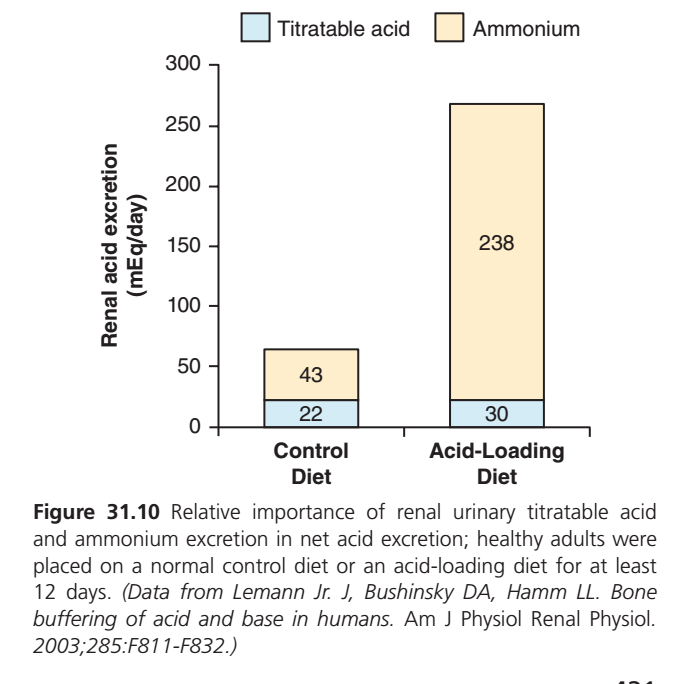
However, with chronic acidosis the dominant mechanism for acid elimination is excretion of NH₄⁺ (Fig. 31.10), which can increase to as high as 500 mEq/day.
- In chronic acidosis:
- NH₄⁺ excretion becomes the main mechanism of acid elimination.
- Figure: Fig. 31.10
- NH₄⁺ excretion can increase to:
- 500 mEq/day
This process also provides the most important mechanism for generating new HCO₃⁻ during chronic acidosis.
- During chronic acidosis:
- NH₄⁺ excretion is the major mechanism for producing new HCO₃⁻.
Figure 31.8
- Figure: Fig. 31.8
- Glutamine enters proximal tubular cells.
- 1 glutamine molecule → 2 NH₄⁺ + 2 HCO₃⁻
- NH₄⁺ is secreted into the tubular lumen by Na⁺-NH₄⁺ exchange.
- 2 HCO₃⁻ are returned to the blood.
Figure 31.9
- Figure: Fig. 31.9
- NH₃ diffuses into the tubular lumen.
- Secreted H⁺ combines with NH₃:
- NH₃ + H⁺ → NH₄⁺
- NH₄⁺ is excreted in urine.
- 1 NH₄⁺ excreted = 1 new HCO₃⁻ returned to the blood
Figure 31.10
- Figure: Fig. 31.10
- Control diet:
- Titratable acid = 30 mEq/day
- Ammonium = 43 mEq/day
- Acid-loading diet:
- Titratable acid = 22 mEq/day
- Ammonium = 238 mEq/day
Mathematical Calculations:
- Control diet total acid excretion = 30 + 43 = 73 mEq/day
- Acid-loading diet total acid excretion = 22 + 238 = 260 mEq/day
- Increase in total acid excretion = 260 − 73 = 187 mEq/day
- Increase in NH₄⁺ excretion = 238 − 43 = 195 mEq/day
- Change in titratable acid = 22 − 30 = −8 mEq/day
KEY CONCEPT
- The ammonium-ammonia buffer system is under physiological control.
- ↑ Extracellular H⁺ → ↑ glutamine metabolism → ↑ NH₄⁺ production → ↑ new HCO₃⁻ generation.
- ↓ Extracellular H⁺ produces the opposite effect.
- Normally, the ammonia buffer system removes 30–50% of acid and generates 30–50% of new HCO₃⁻.
- During chronic acidosis, NH₄⁺ excretion becomes the major mechanism for acid elimination and can increase to 500 mEq/day.
- Figure 31.8: 1 glutamine → 2 NH₄⁺ + 2 HCO₃⁻.
- Figure 31.9: NH₃ + H⁺ → NH₄⁺; 1 NH₄⁺ excreted = 1 new HCO₃⁻.
- Figure 31.10: Acid loading greatly increases NH₄⁺ excretion, making it the main contributor to increased renal acid excretion.
QUANTIFYING RENAL ACID–BASE EXCRETION
Based on the principles discussed earlier, we can quantify the kidneys’ net excretion of acid or net addition or elimination of HCO₃⁻ from the blood as follows.
- The kidneys’ acid-base function can be measured by:
- Net acid excretion
- Net addition of HCO₃⁻ to blood
- Net removal of HCO₃⁻ from blood
Bicarbonate excretion is calculated as urine flow rate multiplied by the urinary HCO₃⁻ concentration and indicates how rapidly the kidneys are removing HCO₃⁻ from the blood, which is the same as adding an H⁺ to the blood.
- Bicarbonate excretion = Urine flow rate × Urinary HCO₃⁻ concentration
- This measures how fast the kidneys remove HCO₃⁻ from the blood.
- Removing HCO₃⁻ from blood is the same as adding H⁺ to the blood.
In alkalosis, the increased excretion of HCO₃⁻ helps return the plasma pH toward normal.
- In alkalosis:
- HCO₃⁻ excretion increases.
- Plasma pH moves toward normal.
The amount of new HCO₃⁻ contributed to the blood at any given time is equal to the amount of H⁺ secreted that ends up in the tubular lumen with nonbicarbonate urinary buffers.
- New HCO₃⁻ added to blood equals:
- H⁺ secreted that combines with nonbicarbonate urinary buffers.
As discussed previously, the primary sources of nonbicarbonate urinary buffers are NH₄⁺ and phosphate.
- Main nonbicarbonate urinary buffers:
- NH₄⁺
- Phosphate
Therefore, part of the HCO₃⁻ added to the blood (and H⁺ excreted by NH₄⁺) is calculated by measuring NH₄⁺ excretion (urine flow rate multiplied by urinary NH₄⁺ concentration).
- NH₄⁺ excretion = Urine flow rate × Urinary NH₄⁺ concentration
- This measures:
- H⁺ excreted as NH₄⁺
- New HCO₃⁻ added to blood
The rest of the nonbicarbonate, non-NH₄⁺ buffer excreted in the urine is measured by determining a value known as titratable acid.
- The remaining urinary buffers are measured as:
- Titratable acid
The amount of titratable acid in the urine is measured by titrating the urine with a strong base, such as NaOH, to a pH of 7.4, the pH of normal plasma and the pH of the glomerular filtrate.
- Titratable acid is measured by:
- Adding NaOH to urine.
- Titrating until pH = 7.4.
- pH 7.4 is:
- Normal plasma pH.
- Normal glomerular filtrate pH.
This titration reverses the events that occurred in the tubular lumen when the tubular fluid was titrated by secreted H⁺.
- Adding NaOH reverses the reaction caused by secreted H⁺ in the tubule.
Therefore, the number of milliequivalents of NaOH required to return the urinary pH to 7.4 equals the number of milliequivalents of H⁺ added to the tubular fluid that combined with phosphate and other organic buffers.
- mEq of NaOH used = mEq of H⁺ buffered by:
- Phosphate
- Other organic buffers
The titratable acid measurement does not include H⁺ in association with NH₄⁺ because the pK of the ammonia-ammonium reaction is 9.2, and titration with NaOH to a pH of 7.4 does not remove the H⁺ from NH₄⁺.
- Titratable acid does not measure NH₄⁺-bound H⁺.
- pK of NH₃/NH₄⁺ system = 9.2
- Titrating to pH 7.4 does not remove H⁺ from NH₄⁺.
Thus, the net acid excretion by the kidneys can be assessed as follows:
- Net Acid Excretion = NH₄⁺ Excretion + Urinary Titratable Acid − HCO₃⁻ Excretion
The reason we subtract HCO₃⁻ excretion is that the loss of HCO₃⁻ is the same as the addition of H⁺ to the blood.
- HCO₃⁻ loss equals H⁺ gain in the blood.
- Therefore, HCO₃⁻ excretion is subtracted.
To maintain acid-base balance, the net acid excretion must equal the nonvolatile acid production in the body.
- For normal acid-base balance:
- Net acid excretion = Nonvolatile acid production
In acidosis, the net acid excretion increases markedly, especially because of increased NH₄⁺ excretion, thereby removing acid from the blood.
- In acidosis:
- Net acid excretion increases.
- NH₄⁺ excretion increases greatly.
- More acid is removed from the blood.
The net acid excretion also equals the rate of net HCO₃⁻ addition to the blood.
- Net acid excretion = Net HCO₃⁻ addition to blood
Therefore, in acidosis, the kidneys compensate with a net addition of HCO₃⁻ back to the blood as more NH₄⁺ and urinary titratable acid are excreted.
- In acidosis:
- More NH₄⁺ is excreted.
- More titratable acid is excreted.
- More HCO₃⁻ is added back to the blood.
In alkalosis, titratable acid and NH₄⁺ excretion drop to 0, whereas HCO₃⁻ excretion increases.
- In alkalosis:
- Titratable acid = 0
- NH₄⁺ excretion = 0
- HCO₃⁻ excretion increases
Therefore, in alkalosis, there is a negative net acid secretion, which means that there is a net loss of HCO₃⁻ from the blood, which is the same as adding H⁺ to the blood, and that no new HCO₃⁻ is generated by the kidneys.
- In alkalosis:
- Net acid excretion becomes negative.
- HCO₃⁻ is lost from the blood.
- This is equivalent to adding H⁺ to the blood.
- No new HCO₃⁻ is generated by the kidneys.
KEY CONCEPT
- Bicarbonate excretion = Urine flow rate × Urinary HCO₃⁻ concentration
- NH₄⁺ excretion = Urine flow rate × Urinary NH₄⁺ concentration
- Titratable acid is measured by titrating urine with NaOH to pH 7.4.
- pK of NH₃/NH₄⁺ system = 9.2, so NH₄⁺ is not included in titratable acid.
- Net Acid Excretion = NH₄⁺ Excretion + Urinary Titratable Acid − HCO₃⁻ Excretion
- HCO₃⁻ loss = H⁺ gain in the blood.
- Net acid excretion must equal nonvolatile acid production.
- Acidosis: ↑ NH₄⁺ excretion, ↑ titratable acid, ↑ net HCO₃⁻ added to blood.
- Alkalosis: NH₄⁺ excretion = 0, titratable acid = 0, ↑ HCO₃⁻ excretion, no new HCO₃⁻ generated.
REGULATION OF RENAL TUBULAR H⁺ SECRETION
As discussed earlier, H⁺ secretion by the tubular epithelium is necessary for HCO₃⁻ reabsorption and generation of new HCO₃⁻ associated with titratable acid formation and NH₄⁺ excretion.
- H⁺ secretion is necessary for:
- HCO₃⁻ reabsorption
- Formation of new HCO₃⁻
- Titratable acid formation
- NH₄⁺ excretion
Therefore, the rate of H⁺ secretion must be carefully regulated if the kidneys are to perform their functions in acid–base homeostasis effectively.
- H⁺ secretion must be carefully regulated.
- This allows the kidneys to maintain acid–base homeostasis.
Under normal conditions, the kidney tubules must secrete at least enough H⁺ to reabsorb almost all the HCO₃⁻ that is filtered, and there must be enough H⁺ left over to be excreted as titratable acid or NH₄⁺ to rid the body of the nonvolatile acids produced each day from metabolism.
- Normally, the kidneys secrete enough H⁺ to:
- Reabsorb almost all filtered HCO₃⁻.
- Leave extra H⁺ to be excreted as:
- Titratable acid
- NH₄⁺
- This removes nonvolatile acids produced during metabolism.
In alkalosis, the tubular secretion of H⁺ is reduced to a level that is too low to achieve complete HCO₃⁻ reabsorption, enabling the kidneys to increase HCO₃⁻ excretion.
- In alkalosis:
- H⁺ secretion decreases.
- HCO₃⁻ reabsorption becomes incomplete.
- HCO₃⁻ excretion increases.
Titratable acid and ammonia are not excreted in alkalosis because there is no excess H⁺ available to combine with nonbicarbonate buffers; therefore, no new HCO₃⁻ is added to the blood in alkalosis.
- In alkalosis:
- Titratable acid is not excreted.
- Ammonia (NH₄⁺) is not excreted.
- There is no excess H⁺ to bind nonbicarbonate buffers.
- No new HCO₃⁻ is added to the blood.
During acidosis, the tubular H⁺ secretion is increased sufficiently to reabsorb all the filtered HCO₃⁻, with enough H⁺ left over to excrete large amounts of NH₄⁺ and titratable acid, thereby contributing large amounts of new HCO₃⁻ to the total body extracellular fluid.
- In acidosis:
- H⁺ secretion increases.
- All filtered HCO₃⁻ is reabsorbed.
- Extra H⁺ is excreted as:
- NH₄⁺
- Titratable acid
- Large amounts of new HCO₃⁻ are added to the extracellular fluid.
The most important stimuli for increasing H⁺ secretion by the tubules in acidosis are as follows:
- Main stimuli for increased H⁺ secretion:
- Increased PCO₂
- Increased H⁺ concentration (decreased pH)
(1) An increase in PCO₂ of the extracellular fluid in respiratory acidosis.
- Respiratory acidosis:
- ↑ PCO₂
- Stimulates H⁺ secretion.
(2) An increase in H⁺ concentration of the extracellular fluid (decreased pH) in respiratory or metabolic acidosis.
- Respiratory or metabolic acidosis:
- ↑ H⁺ concentration
- ↓ pH
- Stimulates H⁺ secretion.
The tubular cells respond directly to an increase in PCO₂ of the blood, as in respiratory acidosis, with an increase in the rate of H⁺ secretion.
- ↑ Blood PCO₂
- Directly increases H⁺ secretion by tubular cells.
The increased PCO₂ raises the PCO₂ of the tubular cells, causing increased formation of H⁺ in the tubular cells, which in turn stimulates secretion of H⁺.
- ↑ Blood PCO₂
- → ↑ Tubular cell PCO₂
- → ↑ H⁺ formation
- → ↑ H⁺ secretion
The second factor that stimulates H⁺ secretion is an increase in extracellular fluid H⁺ concentration (decreased pH).
- ↑ Extracellular H⁺ (↓ pH)
- Stimulates H⁺ secretion.
Another factor that can increase H⁺ secretion under some pathophysiological conditions is excessive aldosterone secretion.
- Excess aldosterone also increases H⁺ secretion.
Aldosterone stimulates secretion of H⁺ by type A intercalated cells of the collecting tubules and ducts.
- Aldosterone stimulates Type A intercalated cells.
- These cells increase H⁺ secretion in:
- Collecting tubules
- Collecting ducts
Therefore, excessive secretion of aldosterone, as occurs in persons with Conn syndrome, increases secretion of H⁺ into the tubular fluid and, consequently, increases the amount of HCO₃⁻ added back to the blood.
- In Conn syndrome:
- Aldosterone increases.
- H⁺ secretion increases.
- More HCO₃⁻ returns to the blood.
This action usually causes alkalosis in patients with excessive aldosterone secretion.
- Excess aldosterone usually causes:
- Alkalosis
The tubular cells usually respond to a decrease in H⁺ concentration (alkalosis) by reducing H⁺ secretion.
- In alkalosis:
- Tubular cells decrease H⁺ secretion.
The decreased H⁺ secretion results from decreased extracellular PCO₂, as in respiratory alkalosis, or from a decrease in H⁺ concentration, as in both respiratory and metabolic alkalosis.
- Respiratory alkalosis:
- ↓ PCO₂
- → ↓ H⁺ secretion
- Respiratory or metabolic alkalosis:
- ↓ H⁺ concentration
- → ↓ H⁺ secretion
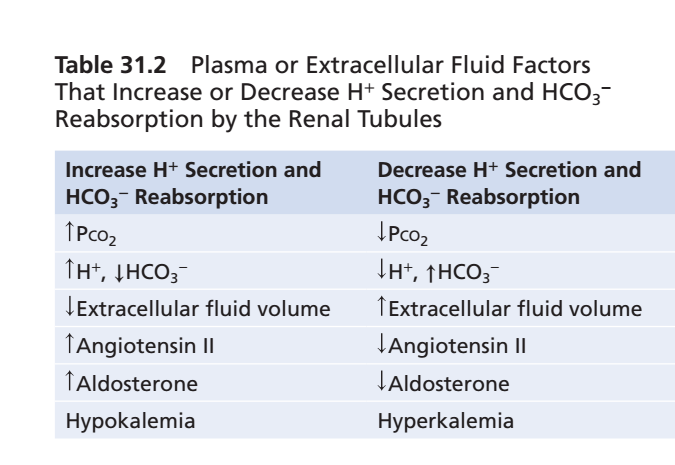
Table 31.2 summarizes the major factors that influence H⁺ secretion and HCO₃⁻ reabsorption.
- Table 31.2 summarizes:
- Factors affecting H⁺ secretion
- Factors affecting HCO₃⁻ reabsorption
Some of these factors are not directly related to the regulation of acid–base balance.
- Some factors affect H⁺ secretion indirectly.
For example, H⁺ secretion is coupled to Na⁺ reabsorption by the Na⁺-H⁺ exchanger in the proximal tubule and the thick ascending loop of Henle.
- H⁺ secretion is linked with Na⁺ reabsorption.
- This occurs through the Na⁺-H⁺ exchanger in:
- Proximal tubule
- Thick ascending loop of Henle
Therefore, factors that stimulate Na⁺ reabsorption, such as decreased extracellular fluid volume and increased angiotensin II (Ang II), may also secondarily increase H⁺ secretion and HCO₃⁻ reabsorption.
- ↓ Extracellular fluid volume
- → ↑ Na⁺ reabsorption
- → ↑ H⁺ secretion
- → ↑ HCO₃⁻ reabsorption
- ↑ Angiotensin II (Ang II)
- Produces the same effects.
Extracellular fluid volume depletion stimulates sodium reabsorption by the renal tubules and increases H⁺ secretion and HCO₃⁻ reabsorption through multiple mechanisms, including the following:
- Extracellular fluid volume depletion:
- ↑ Na⁺ reabsorption
- ↑ H⁺ secretion
- ↑ HCO₃⁻ reabsorption
(1) Increased Ang II, which directly stimulates activity of the Na⁺-H⁺ exchanger in the renal tubules.
- ↑ Ang II
- Directly stimulates the Na⁺-H⁺ exchanger.
(2) Increased aldosterone, which stimulates H⁺ secretion by the intercalated cells of the cortical collecting tubules.
- ↑ Aldosterone
- Stimulates H⁺ secretion by intercalated cells of the cortical collecting tubules.
Therefore, extracellular fluid volume depletion tends to cause alkalosis due to excess H⁺ secretion and HCO₃⁻ reabsorption.
- Extracellular fluid volume depletion tends to cause:
- Alkalosis
- Due to:
- ↑ H⁺ secretion
- ↑ HCO₃⁻ reabsorption
Changes in plasma potassium concentration can also influence H⁺ secretion, with hypokalemia stimulating and hyperkalemia inhibiting H⁺ secretion in the proximal tubule.
- Hypokalemia
- Stimulates H⁺ secretion.
- Hyperkalemia
- Inhibits H⁺ secretion.
Decreased plasma potassium concentration tends to increase H⁺ concentration in the renal tubular cells.
- ↓ Plasma K⁺
- ↑ H⁺ concentration inside tubular cells.
This, in turn, stimulates H⁺ secretion and HCO₃⁻ reabsorption and leads to alkalosis.
- ↑ H⁺ inside tubular cells
- → ↑ H⁺ secretion
- → ↑ HCO₃⁻ reabsorption
- → Alkalosis
Hyperkalemia decreases H⁺ secretion and HCO₃⁻ reabsorption and tends to cause acidosis.
- Hyperkalemia
- ↓ H⁺ secretion
- ↓ HCO₃⁻ reabsorption
- Tends to cause Acidosis
KEY CONCEPT
- H⁺ secretion is essential for:
- HCO₃⁻ reabsorption
- New HCO₃⁻ formation
- Titratable acid formation
- NH₄⁺ excretion
- Alkalosis:
- ↓ H⁺ secretion
- ↓ HCO₃⁻ reabsorption
- ↑ HCO₃⁻ excretion
- No NH₄⁺ excretion
- No titratable acid excretion
- No new HCO₃⁻ added to blood
- Acidosis:
- ↑ H⁺ secretion
- Complete HCO₃⁻ reabsorption
- ↑ NH₄⁺ excretion
- ↑ Titratable acid excretion
- ↑ New HCO₃⁻ added to blood
- Main stimulants of H⁺ secretion:
- ↑ PCO₂
- ↑ H⁺ concentration (↓ pH)
- ↑ Aldosterone
- Conn syndrome: ↑ Aldosterone → ↑ H⁺ secretion → ↑ HCO₃⁻ reabsorption → Alkalosis
- ↓ Extracellular fluid volume: ↑ Ang II + ↑ Aldosterone → ↑ H⁺ secretion → ↑ HCO₃⁻ reabsorption → Alkalosis
- Hypokalemia: ↑ H⁺ secretion → Alkalosis
- Hyperkalemia: ↓ H⁺ secretion → Acidosis