


- Nervous and hormonal factors affect GFR and tubular reabsorption.
- These factors influence the kidney’s excretion of salt and water.
- Nervous and hormonal mechanisms work together with pressure natriuresis and pressure diuresis.
- Together, they make body fluid regulation more effective.
- They help minimize changes in blood volume.
- They help minimize changes in extracellular fluid volume.
- They help minimize changes in arterial pressure during daily challenges.
- In many situations, they regulate sodium and water excretion without major changes in blood pressure.
- Abnormal kidney function can disturb this regulation.
- Abnormal nervous or hormonal control can cause serious changes in blood pressure.
- Abnormal nervous or hormonal control can cause major changes in body fluid volume.
SYMPATHETIC NERVOUS SYSTEM CONTROL OF RENAL EXCRETION: ARTERIAL BARORECEPTOR AND LOW-PRESSURE STRETCH RECEPTOR REFLEXES
- The kidneys receive extensive sympathetic nerve supply.
- Changes in sympathetic activity can alter renal sodium excretion.
- Changes in sympathetic activity can alter renal water excretion.
- Changes in sympathetic activity can influence extracellular fluid volume regulation.
- When blood volume decreases because of hemorrhage, pressure in pulmonary blood vessels falls.
- Pressure also falls in other low-pressure regions of the thorax.
- This activates the sympathetic nervous system through reflexes.
- Renal sympathetic nerve activity increases.
Effects of Increased Renal Sympathetic Activity
- Effect 1: Renal arterioles constrict.
- Severe sympathetic activation decreases GFR.
- Effect 2: Tubular reabsorption of salt increases.
- Tubular reabsorption of water increases.
- Effect 3: Renin release increases.
- Formation of Angiotensin II (Ang II) increases.
- Aldosterone secretion increases.
- Ang II further increases tubular reabsorption.
- Aldosterone further increases tubular reabsorption.
- If blood volume falls enough to reduce arterial pressure, sympathetic activity increases even more.
- This occurs because arterial baroreceptor stretch decreases.
- These baroreceptors are located in the carotid sinus.
- These baroreceptors are also located in the aortic arch.
- All these reflexes help rapidly restore blood volume.
- They are especially important during acute hemorrhage.
- Reflex inhibition of renal sympathetic activity can also occur.
- This helps rapidly remove excess fluid from the circulation.
- This response occurs after a meal containing large amounts of salt and water.
- Excessive sympathetic nervous system activation can be harmful.
- It increases renin secretion.
- It increases Ang II formation.
- It increases renal sodium reabsorption.
- These effects raise blood pressure.
- Renal sympathetic nerve ablation often lowers arterial pressure in hypertension.
- This effect is especially evident in hypertension associated with obesity.
KEY CONCEPT
- Nervous and hormonal mechanisms strengthen renal-body fluid feedback control.
- Sympathetic activation decreases sodium and water excretion.
- It acts through renal vasoconstriction, increased tubular reabsorption, and increased renin–Ang II–aldosterone activity.
- These responses help restore blood volume after hemorrhage.
- Excessive sympathetic activation can contribute to hypertension.
ROLE OF ANGIOTENSIN II IN CONTROLLING RENAL EXCRETION
- Angiotensin II (Ang II) is one of the body’s most powerful controllers of sodium excretion.
- Changes in sodium intake cause opposite changes in Ang II formation.
- These changes help maintain body sodium balance.
- When sodium intake increases above normal, renin secretion decreases.
- Ang II formation also decreases.
- Ang II normally increases tubular sodium reabsorption.
- A decrease in Ang II reduces sodium reabsorption.
- A decrease in Ang II reduces water reabsorption.
- Renal excretion of sodium increases.
- Renal excretion of water increases.
- This helps prevent excessive increases in extracellular fluid volume.
- This helps prevent excessive increases in arterial pressure.
- When sodium intake decreases below normal, Ang II levels increase.
- Increased Ang II causes sodium retention.
- Increased Ang II causes water retention.
- Increased Ang II opposes a fall in arterial blood pressure.
- Changes in renin-angiotensin system activity strongly regulate sodium excretion.
- The renin-angiotensin system amplifies the pressure natriuresis mechanism.
- This helps maintain stable blood pressure.
- This helps maintain stable body fluid volume.
IMPORTANCE OF CHANGES IN ANG II IN REGULATING SODIUM BALANCE AND ALTERING PRESSURE NATRIURESIS
FIGURE NUMBERS MENTIONED: FIG. 19.13 AND FIG. 30.17
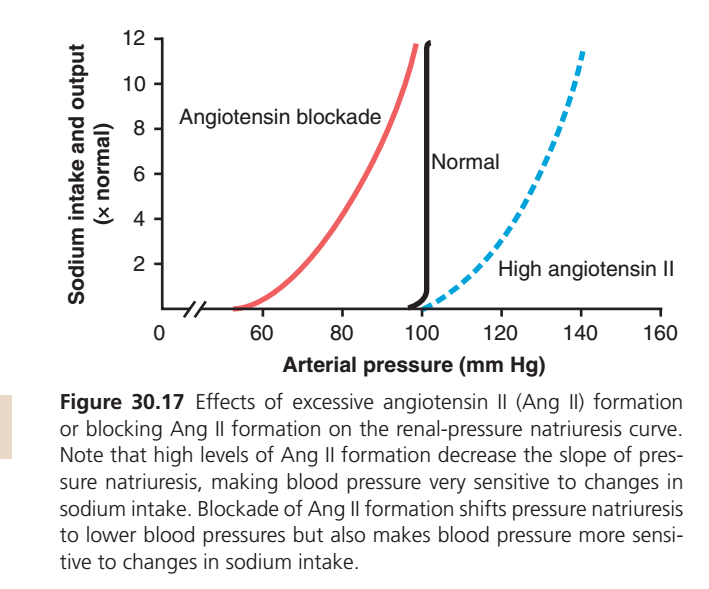
- The importance of Ang II is demonstrated in Fig. 19.13 and Fig. 30.17.
- When Ang II control of natriuresis functions normally, the pressure natriuresis curve is steep.
- This is called the normal curve.
- A steep curve means sodium excretion can increase greatly with only small changes in arterial pressure.
- This allows increased sodium intake to be handled efficiently.
- When Ang II levels cannot be suppressed during high sodium intake, a different curve occurs.
- This is called the high Ang II curve.
- This may occur in people who cannot adequately decrease renin secretion.
- This may occur in people who cannot adequately decrease Ang II formation.
- The pressure natriuresis curve becomes less steep.
- Greater increases in arterial pressure are required to increase sodium excretion.
- Greater increases in arterial pressure are required to maintain sodium balance.
- In most people, a 10-fold increase in sodium intake causes only a small increase in arterial pressure.
- In people who cannot suppress Ang II properly, the same sodium increase causes a larger rise in blood pressure.
- Failure to suppress Ang II reduces the slope of pressure natriuresis.
- Blood pressure becomes highly salt-sensitive.
- Drugs that block Ang II effects improve the kidney’s ability to excrete salt and water.
- Ang II formation can be blocked with an ACE inhibitor.
- Ang II effects can also be blocked with an Ang II receptor antagonist.
- These effects are shown in Fig. 19.13 and Fig. 30.17.
- Ang II blockade shifts the pressure natriuresis curve to lower pressures.
- The kidneys can excrete sodium more easily.
- Normal sodium excretion can occur at lower arterial pressures.
- This shift explains the long-term blood pressure–lowering effect of ACE inhibitors.
- This shift explains the long-term blood pressure–lowering effect of Ang II receptor antagonists.
- Blood pressure becomes more salt-sensitive after Ang II blockade.
- With high sodium intake, Ang II blockers become less effective at lowering blood pressure.
EXCESSIVE ANG II DOES NOT USUALLY CAUSE LARGE INCREASES IN EXTRACELLULAR FLUID VOLUME BECAUSE INCREASED ARTERIAL PRESSURE COUNTERBALANCES ANG II–MEDIATED SODIUM RETENTION
- Ang II is a very powerful sodium-retaining hormone.
- Ang II is a very powerful water-retaining hormone.
- Changes in circulating Ang II usually have little effect on extracellular fluid volume.
- Changes in circulating Ang II usually have little effect on blood volume.
- This is true as long as heart failure or kidney failure is absent.
- Large increases in Ang II may occur with a renin-secreting kidney tumor.
- High Ang II initially causes sodium retention.
- High Ang II initially causes water retention.
- Extracellular fluid volume increases slightly.
- The increase in extracellular fluid volume raises arterial pressure.
- Higher arterial pressure increases kidney excretion of sodium.
- Higher arterial pressure increases kidney excretion of water.
- This overcomes the sodium-retaining effect of Ang II.
- Sodium intake and sodium output become balanced again.
- The new balance occurs at a higher blood pressure.
- ACE inhibitors block Ang II formation.
- Ang II receptor antagonists block Ang II action.
- These drugs initially cause sodium loss.
- These drugs initially cause water loss.
- Blood pressure falls.
- The fall in blood pressure rapidly offsets the sodium and water loss.
- Sodium excretion eventually returns to normal.
- If the heart is weakened by heart disease, cardiac pumping ability decreases.
- The heart may be unable to raise arterial pressure sufficiently.
- High Ang II sodium-retaining effects may not be overcome.
- Large amounts of sodium and water may be retained.
- This may progress to congestive heart failure.
- Blocking Ang II formation can reduce sodium retention in heart failure.
- Blocking Ang II formation can reduce water retention in heart failure.
- This helps reduce excessive expansion of extracellular fluid volume.
KEY CONCEPT
- Ang II is a major regulator of sodium and water balance.
- High Ang II increases sodium and water retention.
- Low Ang II increases sodium and water excretion.
- Ang II makes pressure natriuresis more effective.
- Fig. 19.13 and Fig. 30.17 show how Ang II alters the pressure natriuresis curve.
- ACE inhibitors and Ang II receptor blockers improve sodium excretion and lower blood pressure.
- Increased arterial pressure usually counteracts Ang II–induced fluid retention.
GRAPH UNDERSTANDING
This graph shows how Angiotensin II (Ang II) controls blood pressure by affecting sodium excretion (pressure natriuresis).
Step 1: Understand the Axes
X-Axis (Horizontal)
Arterial Pressure (Blood Pressure)
- Moving right = Higher blood pressure
- Moving left = Lower blood pressure
Y-Axis (Vertical)
Sodium Intake and Output (× Normal)
This means:
| Value | Meaning |
|---|---|
| 1 | Normal sodium intake/output |
| 2 | 2 times normal |
| 4 | 4 times normal |
| 8 | 8 times normal |
| 12 | 12 times normal |
At equilibrium:
Sodium Intake = Sodium Output
The kidney must excrete exactly as much sodium as enters the body.
The BLACK LINE = NORMAL
![Concept]
The black curve represents a person with normal Angiotensin II levels.
What does it show?
At about 100 mmHg, the kidneys can excrete:
- 1× sodium
- 2× sodium
- 4× sodium
- 8× sodium
with only a tiny change in blood pressure.
This line is almost vertical.
Meaning
A small increase in blood pressure causes a huge increase in sodium excretion.
This is called:
Pressure Natriuresis
Why is it vertical?
Because normal kidneys are extremely powerful.
If you eat extra salt:
- Blood volume rises slightly
- Blood pressure rises slightly
- Kidneys immediately excrete more sodium
- Salt balance returns
So blood pressure stays almost constant.
RED CURVE = ANGIOTENSIN BLOCKADE
(ACE inhibitors, ARBs, low Ang II)
What happened?
The whole curve shifts to the LEFT.
This means:
The kidney can excrete sodium at LOWER blood pressures.
Example
Normally:
- To excrete normal sodium → BP ≈ 100 mmHg
With Ang II blockade:
- Same sodium can be excreted at ≈ 60–70 mmHg
So kidneys are losing sodium more easily.
Why?
Normally Ang II:
- Reabsorbs sodium
- Holds salt in the body
When Ang II is blocked:
❌ Less sodium reabsorption
✅ More sodium excretion
Therefore kidneys can remove sodium even when blood pressure is low.
Why is the Red Curve Slanted?
Notice it is NOT vertical.
It bends upward gradually.
This is very important.
Meaning
Blood pressure becomes more dependent on salt intake.
For example:
| Sodium Intake | Required BP |
|---|---|
| 1× | ~60 mmHg |
| 4× | ~80 mmHg |
| 12× | ~95 mmHg |
Large changes in salt intake now require large BP changes.
Key Concept
When Ang II is blocked:
✅ BP becomes lower
❌ But BP becomes more sensitive to dietary salt changes.
BLUE DOTTED CURVE = HIGH ANGIOTENSIN II
This represents:
- Renal artery stenosis
- Renin-secreting tumor
- Excess RAAS activation
What happened?
The entire curve shifts to the RIGHT.
This means higher pressure is required before kidneys excrete sodium.
Example
To excrete normal sodium:idneys now hold sodium strongly.
Why?
High Ang II:
✅ Increases sodium reabsorption
✅ Increases water retention
✅ Decreases sodium loss
The kidney behaves as if it wants to keep every sodium ion.
Why is the Blue Curve Dotted and Slanted?
Because high Ang II reduces the slope.
The curve becomes flatter.
Meaning
Blood pressure becomes extremely sensitive to salt intake.
Look at the curve:
| Sodium Intake | Required BP |
|---|---|
| 1× | ~110 mmHg |
| 4× | ~125 mmHg |
| 12× | ~145 mmHg |
A high-salt diet now causes a huge rise in blood pressure.
Comparing All Three Curves
| Condition | Curve Shift | Effect on Sodium Excretion | Blood Pressure |
|---|---|---|---|
| Normal Ang II | Black | Normal | ~100 mmHg |
| Ang II Blocked | Left (Red) | Easier sodium loss | Lower BP |
| High Ang II | Right (Blue) | Difficult sodium loss | Higher BP |
The Most Important Exam Concept
Angiotensin II normally acts like a “Sodium Saver”
It tells kidneys:
“Don’t throw sodium away.”
Therefore:
↑ Ang II
→ More sodium retained
→ More water retained
→ Higher blood volume
→ Higher blood pressure
→ Pressure-natriuresis curve shifts RIGHT↓ Ang II (ACE inhibitors/ARBs)
→ Less sodium retained
→ More sodium excreted
→ Lower blood volume
→ Lower blood pressure
→ Pressure-natriuresis curve shifts LEFT
One-Line Memory Trick
BLACK (Normal)
Kidneys maintain sodium balance around 100 mmHg.
RED (Ang II Blocked)
Kidneys waste sodium easily → BP falls → Curve shifts LEFT.
BLUE DOTTED (High Ang II)
Kidneys hold sodium strongly → BP rises → Curve shifts RIGHT.
Ultimate Concept
Angiotensin II determines at what blood pressure the kidneys are willing to excrete sodium.
- More Ang II → kidneys need a higher BP to excrete sodium.
- Less Ang II → kidneys can excrete sodium at a lower BP.
ROLE OF ALDOSTERONE IN CONTROLLING RENAL EXCRETION
- Aldosterone increases sodium reabsorption.
- This effect is strongest in the collecting tubules.
- This effect is strongest in the collecting ducts.
- Increased sodium reabsorption is associated with increased water reabsorption.
- Increased sodium reabsorption is associated with increased potassium secretion.
- Aldosterone causes the kidneys to retain sodium.
- Aldosterone causes the kidneys to retain water.
- Aldosterone increases potassium excretion in urine.
- The role of aldosterone in sodium balance is closely related to Ang II.
- When sodium intake decreases, Ang II levels increase.
- Increased Ang II stimulates aldosterone secretion.
- Aldosterone helps reduce urinary sodium excretion.
- Aldosterone helps maintain sodium balance.
- When sodium intake is high, aldosterone formation is suppressed.
- Reduced aldosterone decreases tubular reabsorption.
- The kidneys excrete larger amounts of sodium.
- Changes in aldosterone help the pressure natriuresis mechanism.
- This helps maintain sodium balance during changes in salt intake.
DURING CHRONIC EXCESS ALDOSTERONE SECRETION, THE KIDNEYS ESCAPE FROM SODIUM RETENTION AS ARTERIAL PRESSURE RISES
FIGURE NUMBER MENTIONED: FIG. 78.3
- Aldosterone has powerful effects on sodium reabsorption.
- Excess aldosterone secretion occurs in adrenal gland tumors.
- This condition is called Conn syndrome.
- Excess aldosterone increases sodium reabsorption.
- Excess aldosterone decreases sodium excretion.
- These effects are temporary.
- After a few days, sodium and water retention occur.
- Extracellular fluid volume increases by about 10% to 15%.
- Arterial blood pressure increases at the same time.
- When arterial pressure rises enough, the kidneys escape from sodium and water retention.
- The kidneys then excrete sodium equal to daily intake.
- This occurs despite continued high aldosterone levels.
- One reason for this escape is suppression of Ang II formation.
- Another reason is pressure natriuresis.
- Another reason is pressure diuresis.
- These occur when arterial pressure rises.
- This mechanism is shown in Fig. 78.3.
- In adrenal insufficiency, aldosterone secretion is inadequate.
- This condition is called Addison disease.
- Sodium excretion increases.
- Water excretion increases.
- Extracellular fluid volume decreases.
- There is a tendency toward low blood pressure.
- Complete absence of aldosterone can cause severe volume depletion.
- Large amounts of salt and water must be ingested to compensate.
- This helps balance the increased urinary loss of salt and water.
ROLE OF ANTIDIURETIC HORMONE IN CONTROLLING RENAL WATER EXCRETION
- ADH plays an important role in renal water conservation.
- ADH allows the kidneys to produce a small volume of concentrated urine.
- Normal amounts of salt can still be excreted.
- ADH becomes especially important during water deprivation.
- Water deprivation increases plasma ADH levels.
- Increased ADH increases water reabsorption by the kidneys.
- This helps minimize decreases in extracellular fluid volume.
- This helps minimize decreases in arterial pressure.
- Water deprivation for 24 to 48 hours usually causes only a small decrease in extracellular fluid volume.
- Water deprivation for 24 to 48 hours usually causes only a small decrease in arterial pressure.
- If ADH effects are blocked, the same period of water deprivation causes a major fall in extracellular fluid volume.
- If ADH effects are blocked, the same period of water deprivation causes a major fall in arterial pressure.
- When extracellular fluid volume is excessive, ADH levels decrease.
- Reduced ADH decreases water reabsorption.
- The kidneys remove excess water from the body.
EXCESS ANTIDIURETIC HORMONE SECRETION USUALLY CAUSES ONLY SMALL INCREASES IN EXTRACELLULAR FLUID VOLUME BUT LARGE DECREASES IN SODIUM CONCENTRATION
- ADH is important in regulating extracellular fluid volume.
- Excessive ADH usually does not cause large increases in arterial pressure.
- Excessive ADH usually does not cause large increases in extracellular fluid volume.
- Infusion of large amounts of ADH initially causes water retention by the kidneys.
- Extracellular fluid volume increases by about 10% to 15%.
- Increased extracellular fluid volume raises arterial pressure.
- Pressure diuresis excretes much of the excess volume.
- Increased blood pressure also causes pressure natriuresis.
- Sodium is lost from the extracellular fluid.
- After several days of ADH infusion, blood volume increases by only 5% to 10%.
- After several days of ADH infusion, extracellular fluid volume increases by only 5% to 10%.
- Arterial pressure increases by less than 10 mm Hg.
- Similar effects occur in inappropriate ADH syndrome.
- ADH levels may increase severalfold in this condition.
- High ADH levels do not cause major increases in body fluid volume.
- High ADH levels do not cause major increases in arterial pressure.
- High ADH levels can cause severe reductions in extracellular sodium concentration.
- Increased water reabsorption dilutes extracellular sodium.
- The small increase in blood pressure causes sodium loss through pressure natriuresis.
- Destruction of the supraoptic nuclei prevents ADH secretion.
- Urine volume may become 5 to 10 times normal.
- Increased urine volume is usually compensated by increased water intake.
- Fluid balance can therefore be maintained.
- If access to water is prevented, blood volume may decrease markedly.
- If access to water is prevented, arterial pressure may decrease markedly.
ROLE OF ATRIAL NATRIURETIC PEPTIDE IN CONTROLLING RENAL EXCRETION
- Several natriuretic hormones contribute to volume regulation.
- One of the most important is atrial natriuretic peptide (ANP).
- ANP is released from cardiac atrial muscle fibers.
- Increased atrial stretch is a major stimulus for ANP release.
- Excess blood volume can increase atrial stretch.
- ANP enters the circulation after release.
- ANP acts on the kidneys.
- ANP causes a small increase in GFR.
- ANP decreases renin secretion.
- ANP decreases Ang II formation.
- ANP reduces sodium reabsorption in the collecting ducts.
- These actions increase salt excretion.
- These actions increase water excretion.
- This helps compensate for excess blood volume.
- Changes in ANP levels help minimize blood volume changes.
- This occurs during disturbances such as increased salt and water intake.
- Excessive ANP production does not cause major changes in blood volume.
- Complete absence of ANP does not cause major changes in blood volume.
- Small changes in blood pressure can overcome these effects through pressure natriuresis.
- Large ANP infusions initially increase salt and water excretion.
- Blood volume decreases slightly.
- In less than 24 hours, a slight decrease in blood pressure occurs.
- Urine output returns toward normal.
- This occurs despite continued excess ANP.
KEY CONCEPT
- Aldosterone → ↑ Sodium reabsorption, ↑ Water reabsorption, ↑ Potassium secretion.
- Excess Aldosterone (Conn syndrome) → Initial sodium retention → ↑ ECF volume (10–15%) → ↑ BP → Kidney escape phenomenon.
- Aldosterone deficiency (Addison disease) → ↑ Sodium and water loss → ↓ ECF volume → Low BP.
- ADH → Conserves water and produces concentrated urine.
- Excess ADH → Small increase in ECF volume but marked decrease in sodium concentration.
- Lack of ADH → Massive urine output (5–10× normal).
- ANP → Released by atrial stretch → ↑ GFR, ↓ Renin, ↓ Ang II, ↓ Sodium reabsorption → ↑ Salt and water excretion.
- Figure Mentioned: Fig. 78.3.
INTEGRATED RESPONSES TO CHANGES IN SODIUM INTAKE
- Different control systems work together to regulate sodium and fluid excretion.
- These integrated responses can be understood by examining increases in dietary sodium intake.
- The kidneys can closely match sodium and water excretion to intake.
- Sodium intake may fall to one-tenth of normal.
- Sodium intake may rise to 10 times normal.
- The kidneys can still maintain balance over this wide range.
HIGH SODIUM INTAKE SUPPRESSES ANTINATRIURETIC SYSTEMS AND ACTIVATES NATRIURETIC SYSTEMS
- When sodium intake increases, sodium output initially increases more slowly.
- Sodium output temporarily lags behind sodium intake.
- This delay causes a small positive sodium balance.
- The cumulative sodium balance increases slightly.
- Extracellular fluid volume increases slightly.
- This small increase in extracellular fluid volume triggers mechanisms that increase sodium excretion.
1. ACTIVATION OF LOW-PRESSURE RECEPTOR REFLEXES
- Stretch receptors in the right atrium are activated.
- Stretch receptors in the pulmonary blood vessels are activated.
- Signals travel from these stretch receptors to the brain stem.
- The brain stem inhibits sympathetic nerve activity to the kidneys.
- Reduced sympathetic activity decreases tubular sodium reabsorption.
- This mechanism is most important during the first few hours after increased salt and water intake.
- This mechanism may remain important during the first day after increased salt and water intake.
2. SUPPRESSION OF ANG II AND ALDOSTERONE FORMATION
- Increased arterial pressure suppresses Ang II formation.
- Expansion of extracellular fluid volume suppresses Ang II formation.
- Increased arterial pressure suppresses aldosterone formation.
- Expansion of extracellular fluid volume suppresses aldosterone formation.
- Reduced Ang II decreases tubular sodium reabsorption.
- Reduced aldosterone decreases tubular sodium reabsorption.
- Sodium excretion increases.
3. STIMULATION OF NATRIURETIC SYSTEMS
- Natriuretic systems become activated.
- ANP is especially important among these systems.
- ANP contributes to increased sodium excretion.
- Activation of natriuretic systems promotes sodium loss.
- Suppression of sodium-retaining systems promotes sodium loss.
- Suppression of water-retaining systems promotes sodium loss.
- Together these changes increase sodium excretion when sodium intake rises.
- Opposite changes occur when sodium intake falls below normal.
- Natriuretic systems decrease their activity.
- Sodium-retaining systems become more active.
- Water-retaining systems become more active.
4. SMALL INCREASES IN ARTERIAL PRESSURE
- Large increases in sodium intake may cause slight volume expansion.
- Volume expansion may slightly increase arterial pressure.
- This effect is especially important in salt-sensitive individuals.
- Increased arterial pressure raises sodium excretion through pressure natriuresis.
- Increased arterial pressure suppresses the renin-angiotensin-aldosterone system (RAAS).
- RAAS suppression further increases sodium excretion.
- If nervous, hormonal, and intrarenal mechanisms function effectively, measurable increases in blood pressure may not occur.
- This remains true even with large increases in sodium intake for several days.
- High sodium intake sustained for months or years may damage the kidneys.
- Damaged kidneys become less effective at excreting sodium.
- Higher arterial pressure may then be required to maintain sodium balance.
- This occurs through the pressure natriuresis mechanism.
KEY CONCEPT
- Increased sodium intake → Slight positive sodium balance → Slight increase in ECF volume.
- Increased ECF volume activates mechanisms that increase sodium excretion.
- Low-pressure receptor reflexes ↓ Renal sympathetic activity.
- Ang II and Aldosterone are suppressed.
- ANP and other natriuretic systems are activated.
- Pressure natriuresis increases sodium excretion.
- These mechanisms work together to maintain sodium balance over a very wide range of sodium intake.