


Blood Flow to the Kidneys
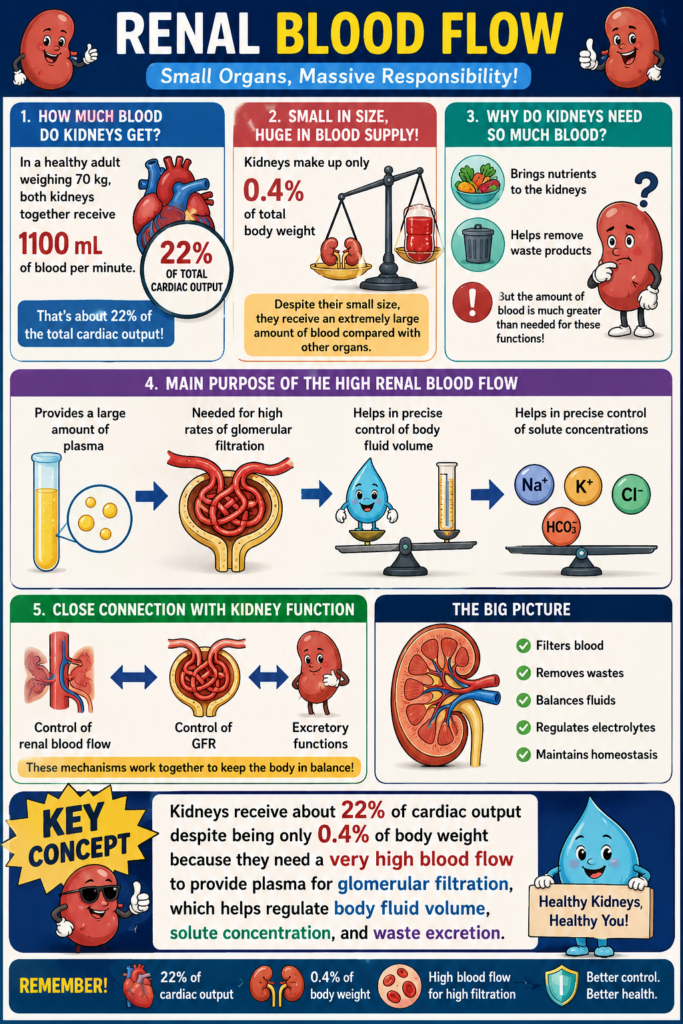
- In a healthy adult weighing 70 kg, both kidneys together receive about 1100 mL of blood per minute.
- This is about 22% of the total cardiac output.
- Renal blood flow can vary depending on a person’s body size, age, and sex, just like GFR varies.
Kidneys Receive a Very High Blood Supply
- The two kidneys make up only about 0.4% of total body weight.
- Despite their small size, they receive an extremely large amount of blood compared with other organs.
Why Do Kidneys Need So Much Blood?
- Like other tissues, blood brings nutrients to the kidneys.
- Blood also helps remove waste products from the kidneys.
- However, the amount of blood flowing to the kidneys is much greater than needed for these functions.
Main Purpose of the High Renal Blood Flow
- The extra blood flow provides a large amount of plasma to the kidneys.
- This plasma is needed for the high rates of glomerular filtration.
- High filtration rates are necessary for precise control of body fluid volume.
- High filtration rates are also necessary for precise control of solute concentrations in the body.
Relationship with Kidney Function
- The mechanisms that control renal blood flow are closely connected with the control of GFR.
- These mechanisms are also closely connected with the excretory functions of the kidneys.
KEY CONCEPT
Kidneys receive about 22% of cardiac output despite being only 0.4% of body weight because they need a very high blood flow to provide plasma for glomerular filtration, which helps regulate body fluid volume, solute concentration, and waste excretion.
RENAL BLOOD FLOW AND OXYGEN CONSUMPTION
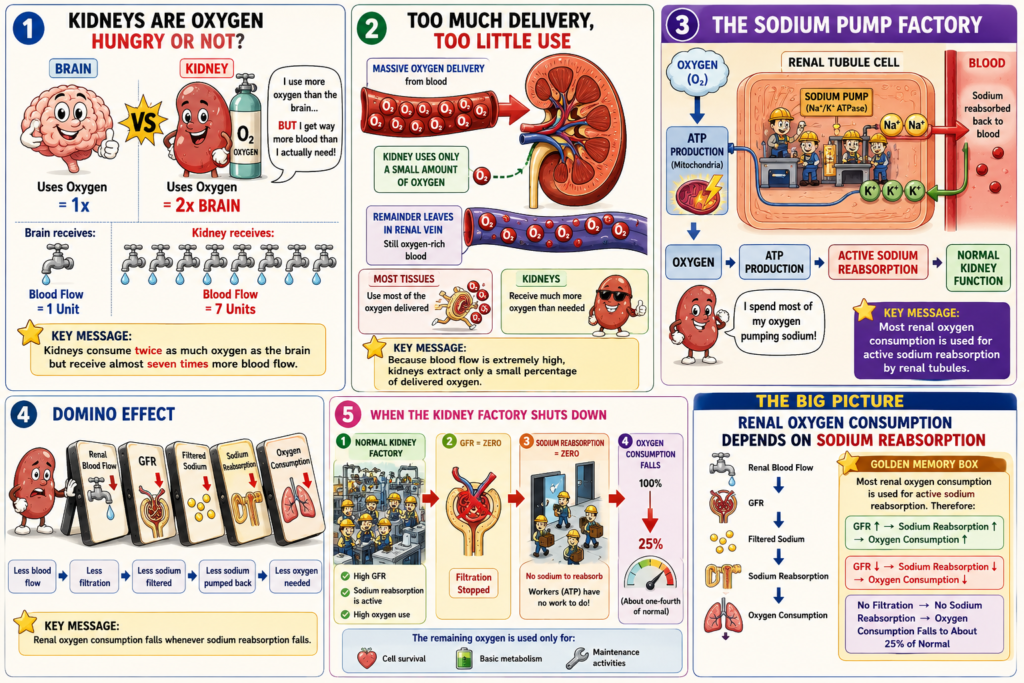
- Per gram of tissue weight, the kidneys normally consume oxygen at twice the rate of the brain.
- However, the kidneys receive almost seven times more blood flow than the brain.
- Therefore, the oxygen delivered to the kidneys is much greater than their metabolic needs.
- As a result, the kidneys extract a relatively small amount of oxygen from the blood compared with most other tissues.
- A large portion of the oxygen consumed by the kidneys is related to the high rate of active sodium reabsorption by the renal tubules.
- If renal blood flow decreases, GFR also decreases.
- When GFR decreases, less sodium is filtered.
- When less sodium is filtered, less sodium is reabsorbed.
- When less sodium is reabsorbed, less oxygen is consumed.
- Renal oxygen consumption changes in proportion to renal tubular sodium reabsorption.
- Renal tubular sodium reabsorption is closely related to GFR.
- Renal tubular sodium reabsorption is also closely related to the amount of sodium filtered.
- If glomerular filtration stops completely, renal sodium reabsorption also stops completely.
- In this situation, oxygen consumption falls to about one-fourth of normal.
- The remaining oxygen consumption reflects the basic metabolic needs of the renal cells.
KEY CONCEPT
Most renal oxygen consumption is used for active sodium reabsorption. Therefore, renal oxygen consumption is directly related to GFR, filtered sodium load, and tubular sodium reabsorption.
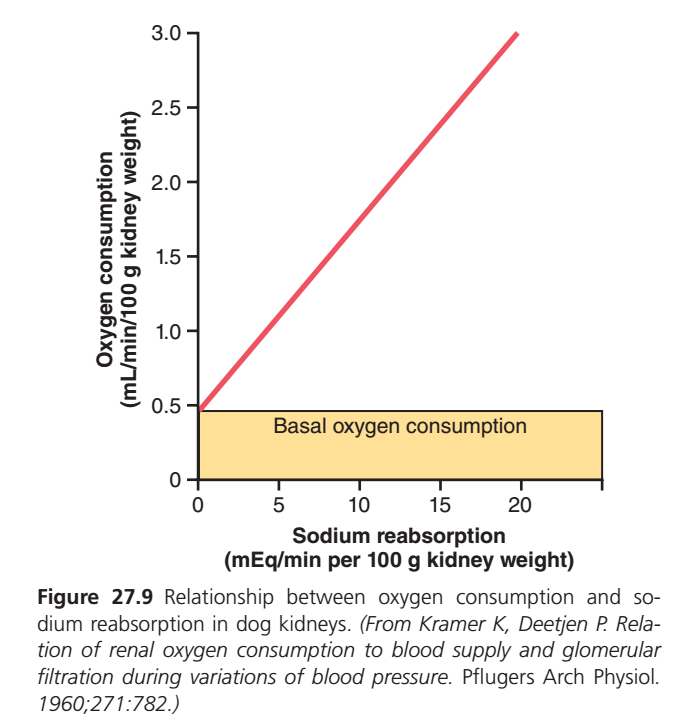
This graph shows:
👉 How much oxygen the kidney uses when it reabsorbs sodium (Na⁺).
The main message is:
The more sodium the kidney reabsorbs, the more oxygen it consumes.
FIRST UNDERSTAND THE AXES
X-Axis (Horizontal Line)
Sodium Reabsorption
(mEq/min per 100 g kidney weight)
This tells us:
➡️ How much sodium is being taken back from the filtrate into the blood.
Moving from left to right means:
- Kidney is reabsorbing more sodium.
- Kidney tubule cells are working harder.
Y-Axis (Vertical Line)
Oxygen Consumption
(mL/min per 100 g kidney weight)
This tells us:
➡️ How much oxygen kidney cells are using.
Moving upward means:
- More oxygen is being consumed.
- More energy (ATP) is being produced.
THE RED LINE
The red line is the most important part of the graph.
It starts at:
0 sodium reabsorption
but oxygen consumption is still about 0.5 mL/min.
Then it rises steadily upward.
What Does This Mean?
As sodium reabsorption increases:
- ATP use increases
- Na⁺/K⁺ pumps work harder
- Oxygen consumption increases
Therefore:
More Na⁺ Reabsorption = More O₂ Consumption
The relationship is almost linear.
WHY DOES THE RED LINE RISE?
Think of kidney tubule cells as workers.
Little Sodium Reabsorption
👨🔧 Worker is doing little work
Needs little ATP
Needs little oxygen
Large Sodium Reabsorption
👨🔧👨🔧👨🔧 Worker is very busy
Needs lots of ATP
Needs lots of oxygen
Therefore oxygen consumption rises.
WHY IS THE LINE STRAIGHT?
A straight line means:
Every extra amount of sodium reabsorbed requires approximately the same extra amount of oxygen.
For example:
| Sodium Reabsorption | Oxygen Consumption |
|---|---|
| Low | Low |
| Medium | Medium |
| High | High |
The increase is proportional.
THE YELLOW SHADED AREA
“Basal Oxygen Consumption”
This is the most tested concept.
The yellow box represents:
Oxygen used even when NO sodium is being reabsorbed.
Notice:
At X = 0
Oxygen consumption is still around 0.5 mL/min per 100 g kidney weight.
So the kidney never reaches zero oxygen use.
WHY DOES THE KIDNEY STILL USE OXYGEN?
Even if sodium transport stopped completely, kidney cells are still alive.
They must perform:
1. Protein synthesis
Making proteins continuously.
2. Cell repair
Replacing damaged cell components.
3. Maintaining cell membranes
Keeping cells alive.4. Basic metabolism
Producing ATP for survival.
5. Housekeeping functions
All cells require energy just to stay alive.
EASY ANALOGY
Imagine a car.
Engine Running but Car Not Moving
Fuel is still consumed.
This is like:
Basal Oxygen Consumption
(Yellow Area)
The kidney is alive and consuming oxygen even though sodium transport is zero.
Car Starts Driving
Now fuel consumption rises.
This is like:
Sodium Reabsorption
The harder the kidney works, the more oxygen it consumes.
WHAT DOES THE YELLOW AREA REPRESENT MATHEMATICALLY?
The yellow area corresponds to about:
0.5 mL O₂/min/100 g kidney
This is the oxygen requirement for:
Basic cellular survival
and is independent of sodium transport.
WHAT DOES THE RED PORTION ABOVE THE YELLOW AREA REPRESENT?
Everything above the yellow area is:
Oxygen used specifically for sodium reabsorption.
This oxygen is needed to generate ATP for:
Na⁺/K⁺-ATPase Pumps
These pumps:
- Move sodium out of tubular cells
- Reabsorb sodium into blood
- Consume large amounts of ATP
ATP production requires oxygen.
Therefore:
Sodium Reabsorption → ATP Use → Oxygen Consumption
KEY CONCEPT
🟨 Yellow Area (Basal Oxygen Consumption)
- Oxygen needed for cell survival
- Present even when sodium reabsorption is zero
- About 0.5 mL/min/100 g kidney
🔴 Red Rising Line
- Represents oxygen used for sodium transport
- Directly proportional to sodium reabsorption
- More Na⁺ reabsorbed = more ATP required = more O₂ consumed
ONE-LINE EXAM POINT
About 80–90% of renal oxygen consumption is used for active sodium reabsorption, while the remaining oxygen consumption (yellow area) represents basal metabolic needs of kidney cells.
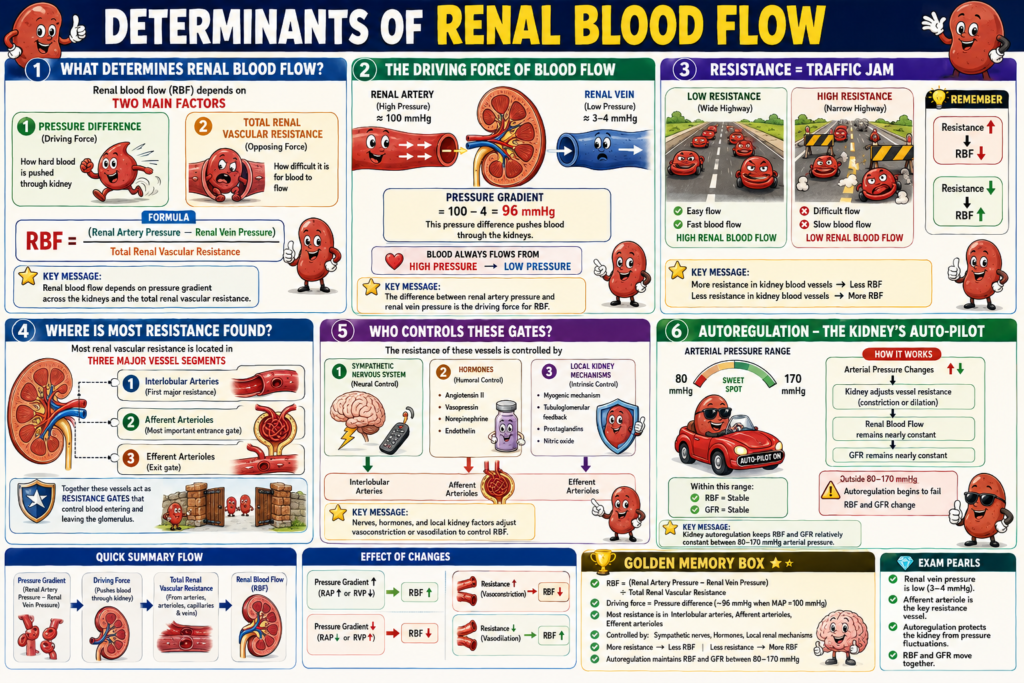
DETERMINANTS OF RENAL BLOOD FLOW
- Renal blood flow (RBF) depends on the pressure difference across the kidney blood vessels.
- It also depends on the total resistance of the kidney blood vessels.
Formula
RBF = (Renal artery pressure − Renal vein pressure) ÷ Total renal vascular resistance
Conceptual Understanding of the Formula
- Blood flows because there is a pressure difference.
- The pressure in the renal artery pushes blood into the kidney.
- The pressure in the renal vein opposes blood leaving the kidney.
- The difference between these two pressures is the driving force for blood flow.
- This driving force is divided by the total resistance of the kidney blood vessels.
- More resistance → less renal blood flow.
- Less resistance → more renal blood flow.
Example Using the Given Values
- Renal artery pressure ≈ Systemic arterial pressure
- Renal vein pressure ≈ 3–4 mm Hg
If systemic arterial pressure = 100 mm Hg
Pressure gradient = 100 − 4 = 96 mm Hg
- Therefore, blood is pushed through the kidneys by a pressure difference of about 96 mm Hg.
- The actual renal blood flow depends on the total renal vascular resistance.
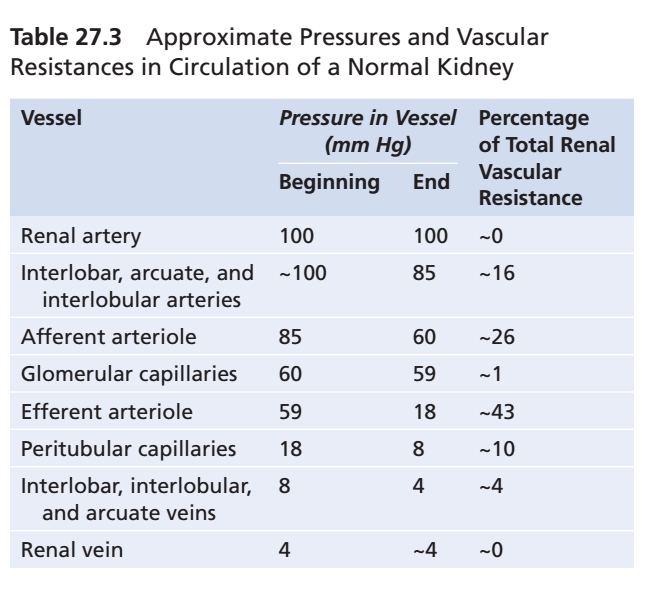
- Renal artery pressure is usually about the same as systemic arterial pressure.
- Renal vein pressure is normally about 3 to 4 mm Hg.
- Total renal vascular resistance is determined by the combined resistance of the arteries, arterioles, capillaries, and veins.
- Most renal vascular resistance is located in three major blood vessel segments.
- These are the interlobular arteries.
- These are the afferent arterioles.
- These are the efferent arterioles.
- The resistance of these vessels is controlled by the sympathetic nervous system.
- The resistance of these vessels is also controlled by various hormones.
- The resistance of these vessels is also controlled by local kidney mechanisms.
- An increase in resistance in any kidney blood vessel segment tends to decrease renal blood flow.
- A decrease in vascular resistance tends to increase renal blood flow.
- This occurs if renal artery pressure and renal vein pressure remain constant.
- Changes in arterial pressure can affect renal blood flow.
- However, the kidneys have powerful mechanisms that help keep renal blood flow relatively constant.
- These mechanisms also help keep GFR relatively constant.
- Renal blood flow and GFR remain relatively stable when arterial pressure is between 80 and 170 mm Hg.
- This process is called autoregulation.
- Autoregulation occurs through mechanisms that are present within the kidneys themselves.
KEY CONCEPT
Renal blood flow depends on the pressure gradient across the kidneys and the total renal vascular resistance. Increased resistance decreases renal blood flow, decreased resistance increases renal blood flow, and kidney autoregulation helps keep renal blood flow and GFR relatively constant between arterial pressures of 80–170 mm Hg.
BLOOD FLOW IN VASA RECTA OF RENAL MEDULLA IS LOW COMPARED WITH RENAL CORTEX FLOW
- The renal cortex receives most of the blood flow entering the kidneys.
- The renal medulla receives only 1% to 2% of the total renal blood flow.
- Blood flow to the renal medulla is supplied by a specialized part of the peritubular capillary system.
- This specialized capillary system is called the vasa recta.
- The vasa recta descend into the medulla alongside the loops of Henle.
- The vasa recta then return to the cortex together with the loops of Henle.
- After returning to the cortex, the vasa recta empty into the venous system.
- The vasa recta play an important role in helping the kidneys form concentrated urine.
KEY CONCEPT
Most renal blood flow goes to the renal cortex, while the renal medulla receives only 1% to 2% of total renal blood flow through the vasa recta, which are important for the formation of concentrated urine.
Renal Blood Flow: Summarized Essay
The kidneys receive an exceptionally large blood supply compared with most other organs. In a healthy adult, the combined renal blood flow (RBF) is approximately 1100 mL/min, which represents about 22% of the cardiac output. Although the kidneys make up only about 0.4% of total body weight, they receive a disproportionately high amount of blood. This large blood flow is necessary not only to provide oxygen and nutrients but also to supply sufficient plasma for the high rates of glomerular filtration required to maintain normal body fluid and electrolyte balance.
The primary function of this high renal blood flow is to support glomerular filtration. By filtering large amounts of plasma, the kidneys can precisely regulate water balance, electrolyte concentrations, acid-base status, and waste removal. Therefore, regulation of renal blood flow is closely linked to the regulation of glomerular filtration rate (GFR) and overall kidney function.
Although the kidneys receive a large blood supply, their oxygen extraction is relatively low compared with other organs. On a gram-for-gram basis, the kidneys consume oxygen at about twice the rate of the brain, yet they receive nearly seven times more blood flow. Most of the oxygen consumed by the kidneys is used for the active reabsorption of sodium by the renal tubules. Consequently, renal oxygen consumption is directly related to sodium reabsorption and GFR. When GFR decreases, less sodium is filtered and reabsorbed, resulting in lower oxygen consumption. If filtration stops completely, oxygen consumption falls to about one-fourth of normal, reflecting only the basic metabolic needs of kidney cells.
Renal blood flow is determined by the pressure gradient across the renal circulation and the total renal vascular resistance. In simple terms, blood flow increases when vascular resistance decreases and decreases when vascular resistance increases. The major resistance vessels are the interlobular arteries, afferent arterioles, and efferent arterioles. Their diameter is controlled by the sympathetic nervous system, hormones, and local kidney mechanisms. Constriction of these vessels reduces renal blood flow, whereas dilation increases blood flow.
Despite fluctuations in systemic blood pressure, the kidneys possess a remarkable ability called autoregulation. Through intrinsic mechanisms, they maintain relatively constant renal blood flow and GFR over a wide arterial pressure range of approximately 80–170 mm Hg. This ensures stable kidney function and prevents large changes in filtration despite normal variations in blood pressure.
Blood flow within the kidney is not distributed equally. The renal cortex receives most of the renal blood flow because it contains the majority of glomeruli where filtration occurs. In contrast, the renal medulla receives only about 1–2% of total renal blood flow. Blood reaches the medulla through specialized capillaries known as the vasa recta, which run alongside the loops of Henle. Although medullary blood flow is low, the vasa recta play a critical role in maintaining the osmotic gradient necessary for the formation of concentrated urine.
In summary, renal blood flow is exceptionally high because the kidneys require large amounts of plasma for filtration and precise regulation of body fluids. Renal oxygen consumption is closely linked to sodium reabsorption, and blood flow is controlled by vascular resistance and autoregulatory mechanisms. Most blood flows through the renal cortex, while the medulla receives only a small fraction through the vasa recta, which are essential for urine concentration. Together, these mechanisms ensure efficient filtration, waste removal, and maintenance of body homeostasis.