EXTRACELLULAR FLUID POTASSIUM CONCENTRATION
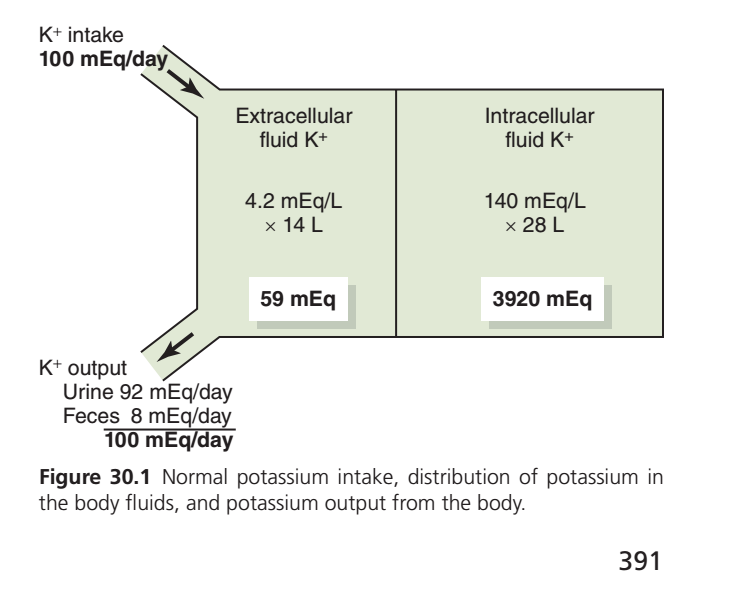
- Extracellular fluid potassium concentration is normally maintained at about 4.2 mEq/L.
- Potassium concentration usually changes by no more than ±0.3 mEq/L.
- Precise potassium regulation is essential because many cell functions depend on it.
- Even a small increase in plasma potassium can affect the heart.
- An increase of only 3–4 mEq/L may cause cardiac arrhythmias.
- Severe hyperkalemia can cause cardiac arrest or ventricular fibrillation.
- Less than 2% of total body potassium is present in the extracellular fluid.
- More than 98% of total body potassium is located inside cells.
- Therefore, extracellular potassium concentration can change rapidly if potassium moves between compartments.
- A typical meal may contain about 50 mEq of potassium.
- Daily potassium intake usually ranges from 50–200 mEq/day.
- Failure to rapidly remove excess potassium from extracellular fluid can cause life-threatening hyperkalemia.
- Small losses of extracellular potassium can cause severe hypokalemia if not corrected quickly.
- Potassium balance depends mainly on the kidneys.
- Only a small amount of potassium is excreted in the feces.
- The kidneys must rapidly adjust potassium excretion according to intake.
- Precise renal regulation is essential for maintaining normal potassium balance.
- Potassium distribution between extracellular and intracellular compartments is a major part of potassium homeostasis.
- Cells act as a storage site for excess extracellular potassium during hyperkalemia.
- Cells can release potassium during hypokalemia.
- Potassium shifting between cells and extracellular fluid provides the first line of defense against changes in plasma potassium concentration.
- Skeletal muscle is the body’s largest potassium reservoir.
- Skeletal muscles normally contain 60–75% of total body potassium.
- Muscle potassium storage depends on factors such as sex, age, and physical activity.
KEY CONCEPT
- Potassium is tightly regulated because small changes can cause serious cardiac problems.
- More than 98% of body potassium is intracellular.
- Cells provide the first line of defense by rapidly shifting potassium between compartments.
- Kidneys provide long-term potassium balance by adjusting potassium excretion.
- Skeletal muscle is the major storage site for body potassium.
REGULATION OF INTERNAL POTASSIUM DISTRIBUTION
- After a potassium-rich meal, potassium must rapidly move into cells to prevent dangerous hyperkalemia.
- If ingested potassium remained in the extracellular fluid, plasma potassium concentration would rise significantly.
- Most absorbed potassium quickly shifts into cells until the kidneys remove the excess.
- Between meals, cells release potassium to replace the potassium excreted by the kidneys.
- Internal potassium redistribution helps maintain a nearly constant plasma potassium concentration.
- Extracellular potassium concentration is tightly regulated around 4.2 mEq/L.
- Small changes in extracellular potassium can significantly affect cell function.
- Even a modest increase in plasma potassium can cause cardiac arrhythmias.
- Severe hyperkalemia may cause cardiac arrest or ventricular fibrillation.
- More than 98% of body potassium is located inside cells.
- Less than 2% is present in extracellular fluid.
- Because extracellular potassium is very small, even minor potassium shifts can greatly alter plasma potassium concentration.
- Potassium balance depends mainly on renal excretion.
- The kidneys must rapidly adjust potassium excretion according to intake.
- Cellular potassium shifts and renal excretion work together to maintain potassium homeostasis.
- Cells serve as a reservoir for potassium.
- During hyperkalemia, cells take up excess extracellular potassium.
- During hypokalemia, cells release potassium into the extracellular fluid.
- Potassium redistribution between cells and extracellular fluid provides the first line of defense against potassium imbalance.
FACTORS AFFECTING INTERNAL POTASSIUM DISTRIBUTION
INSULIN
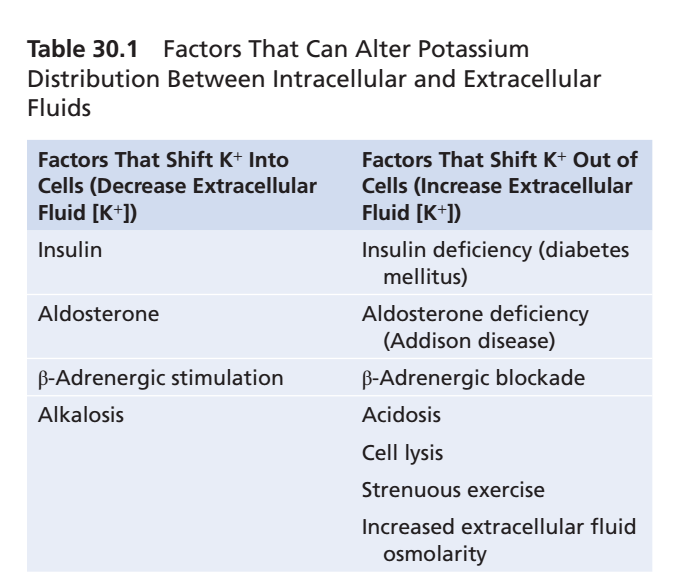
- Insulin stimulates potassium uptake into cells.
- Insulin increases Na⁺-K⁺ ATPase activity.
- After a meal, insulin helps move potassium from extracellular fluid into cells.
- Insulin deficiency causes a greater rise in plasma potassium after eating.
- Insulin administration can correct hyperkalemia.
- Excess insulin may cause hypokalemia.
ALDOSTERONE
- Aldosterone increases potassium uptake into cells.
- Aldosterone stimulates Na⁺-K⁺ ATPase activity.
- Aldosterone also increases renal potassium secretion.
- Insulin and aldosterone work together to promote cellular potassium uptake after a potassium-rich meal.
- Excess aldosterone (Conn syndrome) commonly causes hypokalemia.
- Aldosterone deficiency (Addison disease) commonly causes hyperkalemia.
β-ADRENERGIC STIMULATION
- Epinephrine promotes movement of potassium into cells.
- This effect occurs through stimulation of β₂-adrenergic receptors.
- β₂ stimulation increases Na⁺-K⁺ ATPase activity.
- β-blockers reduce cellular potassium uptake.
- β-blockers increase the tendency toward hyperkalemia.
ACID–BASE DISTURBANCES
- Metabolic acidosis causes potassium to move out of cells.
- Acidosis increases extracellular potassium concentration.
- Acidosis reduces Na⁺-K⁺ ATPase activity.
- Reduced cellular potassium uptake contributes to hyperkalemia.
- Metabolic alkalosis causes potassium to move into cells.
- Alkalosis decreases extracellular potassium concentration.
- Alkalosis can contribute to hypokalemia.
CELL LYSIS
- Cell destruction releases large amounts of intracellular potassium.
- Potassium released from damaged cells increases extracellular potassium concentration.
- Severe tissue injury can cause significant hyperkalemia.
- Red blood cell destruction can also cause hyperkalemia.
STRENUOUS EXERCISE
- Exercise causes potassium release from skeletal muscle.
- This release may increase extracellular potassium concentration.
- Hyperkalemia after exercise is usually mild.
- Intense exercise can occasionally cause clinically significant hyperkalemia.
- The risk is greater in patients with insulin deficiency or those taking β-blockers.
- Severe exercise-induced hyperkalemia may cause cardiac toxicity.
DEHYDRATION AND INCREASED EXTRACELLULAR OSMOLARITY
- Increased extracellular osmolarity causes water to move out of cells.
- Cellular dehydration increases intracellular potassium concentration.
- Increased intracellular potassium promotes potassium diffusion out of cells.
- This process raises extracellular potassium concentration.
- Decreased extracellular osmolarity has the opposite effect.
- Potassium moves into cells when extracellular osmolarity falls.
KEY CONCEPT
- Internal potassium redistribution provides the first line of defense against changes in plasma potassium concentration.
- Insulin, aldosterone, and β₂-adrenergic stimulation shift potassium into cells.
- Acidosis, cell lysis, strenuous exercise, and dehydration shift potassium out of cells.
- More than 98% of body potassium is intracellular, making cells the major potassium reservoir.
- Kidneys provide long-term potassium balance, while cellular shifts provide rapid short-term regulation.