


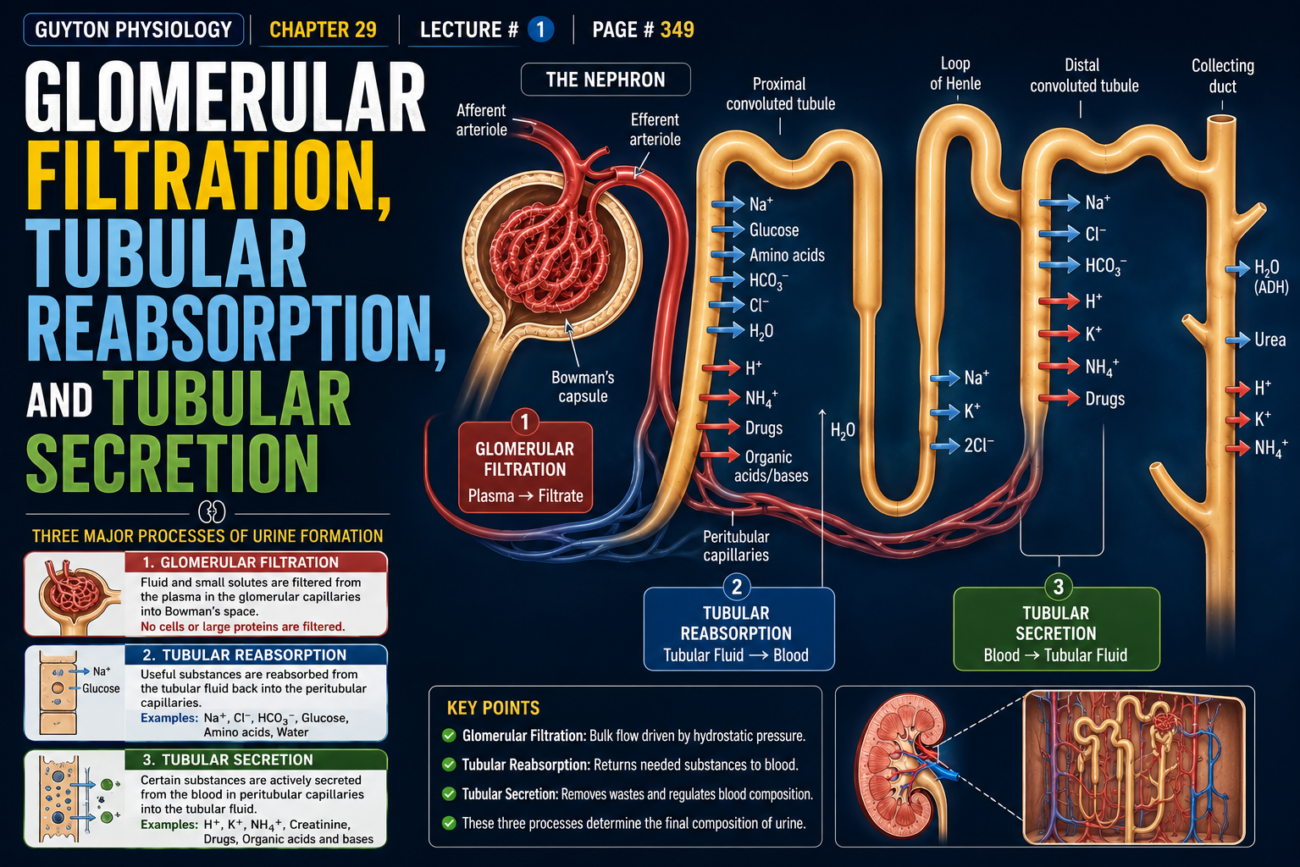
- After glomerular filtration, the filtrate enters the renal tubules.
- The filtrate flows through the proximal tubules.
- The filtrate then flows through the loops of Henle.
- The filtrate then flows through the distal tubules.
- The filtrate then flows through the collecting tubules.
- The filtrate then flows through the collecting ducts.
- Finally, the filtrate is excreted as urine.
- Along this pathway, some substances are selectively reabsorbed from the tubules back into the blood.
- Other substances are secreted from the blood into the tubular lumen.
- The final urine is the result of three basic renal processes.
- These processes are glomerular filtration.
- These processes are tubular reabsorption.
- These processes are tubular secretion.
Formula
Urinary Excretion = Glomerular Filtration − Tubular Reabsorption + Tubular Secretion
Conceptual Calculation
If:
- Glomerular Filtration = 100 units
- Tubular Reabsorption = 90 units
- Tubular Secretion = 5 units
Then:
Urinary Excretion = 100 − 90 + 5
Urinary Excretion = 15 units
- Therefore, 15 units are excreted in the urine.
- For many substances, tubular reabsorption is more important than tubular secretion in determining the final urinary excretion rate.
- Tubular secretion contributes significant amounts of potassium ions to the urine.
- Tubular secretion contributes significant amounts of hydrogen ions to the urine.
- Tubular secretion also contributes a few other substances to the urine.
KEY CONCEPT
Final urinary excretion depends on three renal processes: glomerular filtration, tubular reabsorption, and tubular secretion. Most substances are mainly controlled by tubular reabsorption, while substances such as potassium and hydrogen ions are significantly affected by tubular secretion.
GLOMERULAR FILTRATION, TUBULAR REABSORPTION, AND TUBULAR SECRETION
- After glomerular filtration, the filtrate enters the renal tubules.
- The filtrate flows through the proximal tubules.
- The filtrate then flows through the loops of Henle.
- The filtrate then flows through the distal tubules.
- The filtrate then flows through the collecting tubules.
- The filtrate then flows through the collecting ducts.
- Finally, the filtrate is excreted as urine.
- Along this pathway, some substances are selectively reabsorbed from the tubules back into the blood.
- Other substances are secreted from the blood into the tubular lumen.
- The final urine is the result of three basic renal processes.
- These processes are glomerular filtration.
- These processes are tubular reabsorption.
- These processes are tubular secretion.
Formula
Urinary Excretion = Glomerular Filtration − Tubular Reabsorption + Tubular Secretion
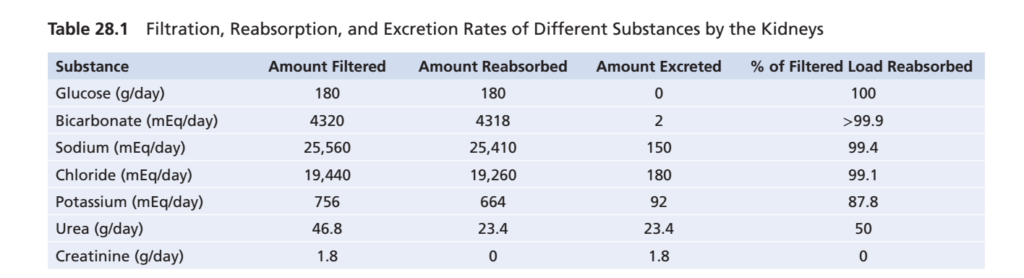
- Many substances are freely filtered by the glomeruli.
- These substances are reabsorbed from the tubules at different rates.
Filtration Formula
Filtered Amount = GFR × Plasma Concentration
- This formula applies only to substances that are freely filtered.
- The substance must not be bound to plasma proteins.
Example: Glucose Filtration
- Plasma glucose concentration = 1 g in each liter of plasma
- GFR = 180 liters filtered per day
Calculation
Step 1
- Each liter of filtrate contains 1 g glucose.
Step 2
- Kidneys filter 180 liters per day.
Step 3
- Therefore:
1 g glucose × 180 liters
= 180 g glucose/day
Result
- The kidneys filter 180 g of glucose every day.
What Happens to This Glucose?
- Normally, almost no glucose appears in the urine.
- Therefore, almost all filtered glucose must be reabsorbed.
Easy Calculation
Filtered glucose = 180 g/day
Urinary glucose = 0 g/day
Reabsorbed glucose = 180 − 0
= 180 g/day
Result
- About 180 g/day of glucose is reabsorbed.
- Almost 100% of filtered glucose returns to the blood.
Important Observation
- The amount filtered is very large.
- The amount reabsorbed is also very large.
- The amount excreted is extremely small.
Simple Concept
Filtered = 180 g/day
↓
Reabsorbed = 180 g/day
↓
Excreted = 0 g/day
- This shows that tubular reabsorption is quantitatively very large.
- Glomerular filtration and tubular reabsorption are much larger than urinary excretion for many substances.
- Therefore, even a small change in tubular reabsorption can cause a large change in urinary excretion.
- Tubular reabsorption is highly selective.
- Different substances are reabsorbed at different rates.
KEY CONCEPT
The kidneys filter huge amounts of substances each day, but most of these substances are reabsorbed back into the blood. For example, 180 g of glucose is filtered daily and almost all 180 g is reabsorbed, showing that tubular reabsorption is both massive and highly selective.
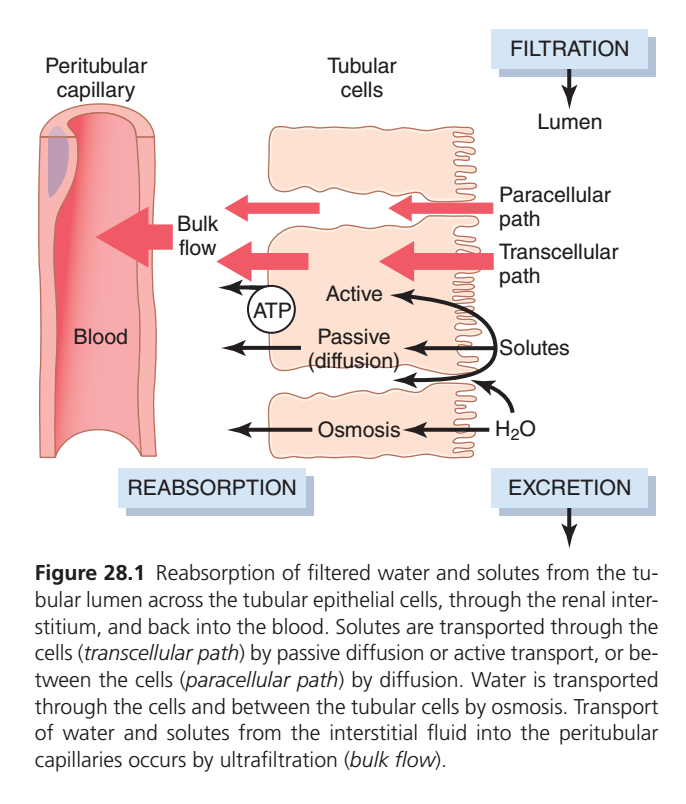
TUBULAR REABSORPTION INCLUDES PASSIVE AND ACTIVE MECHANISMS
- For a substance to be reabsorbed, it must first cross the tubular epithelial membrane into the renal interstitial fluid.
- The substance must then cross the peritubular capillary membrane back into the blood.
Reabsorption Pathway
Tubular Lumen → Tubular Epithelial Cell → Interstitial Fluid → Peritubular Capillary → Blood
- Therefore, reabsorption of water and solutes occurs through a series of transport steps.
- Reabsorption across the tubular epithelium may occur by active transport.
- Reabsorption across the tubular epithelium may occur by passive transport.
- These transport mechanisms are the same basic mechanisms used in other body cells.
- Water and solutes can move through the cell membrane.
- This pathway is called the transcellular route.
Transcellular Route
Tubular Lumen → Cell → Interstitial Fluid
- Water and solutes can also move through the spaces between adjacent cells.
- This pathway is called the paracellular route.
Paracellular Route
Tubular Lumen → Between Cells → Interstitial Fluid
- After crossing the tubular epithelial cells, water and solutes enter the interstitial fluid.
- Water and solutes then move through the peritubular capillary walls into the blood.
- This movement occurs by ultrafiltration (bulk flow).
- Ultrafiltration is controlled by hydrostatic forces.
- Ultrafiltration is also controlled by colloid osmotic forces.
- The peritubular capillaries behave like the venous ends of most capillaries.
- There is a net reabsorptive force in the peritubular capillaries.
- This force moves fluid from the interstitial fluid into the blood.
- This force also moves solutes from the interstitial fluid into the blood.
Review of Urine Formation
- After glomerular filtration, the filtrate enters the renal tubules.
- The filtrate flows through the proximal tubules.
- The filtrate then flows through the loops of Henle.
- The filtrate then flows through the distal tubules.
- The filtrate then flows through the collecting tubules.
- The filtrate then flows through the collecting ducts.
- Finally, the filtrate is excreted as urine.
- Some substances are selectively reabsorbed from the tubules into the blood.
- Other substances are secreted from the blood into the tubular lumen.
- Final urine is determined by three basic renal processes.
- These are glomerular filtration.
- These are tubular reabsorption.
- These are tubular secretion.
Formula
Urinary Excretion = Glomerular Filtration − Tubular Reabsorption + Tubular Secretion
Easy Conceptual Calculation
Suppose:
- Glomerular filtration = 100 units
- Tubular reabsorption = 85 units
- Tubular secretion = 5 units
Step 1
100 − 85 = 15 units
Step 2
15 + 5 = 20 units
Result
Urinary Excretion = 20 units
- For many substances, tubular reabsorption is more important than tubular secretion in determining urinary excretion.
- Tubular secretion contributes significant amounts of potassium ions to the urine.
- Tubular secretion contributes significant amounts of hydrogen ions to the urine.
- Tubular secretion also contributes several other substances to the urine.
Filtration of Glucose
Formula
Filtered Amount = GFR × Plasma Concentration
Suppose:
- Plasma glucose concentration = 1 g/L
- GFR = 180 L/day
Step 1
- Each liter of filtrate contains 1 g glucose.
Step 2
- Kidneys filter 180 liters per day.
Step 3
1 g × 180 L
= 180 g/day
Result
- The kidneys filter 180 g of glucose each day.
- Normally, almost no glucose is excreted in the urine.
Step 4
Reabsorbed Glucose = Filtered Glucose − Excreted Glucose
= 180 − 0
= 180 g/day
Result
- About 180 g/day of glucose is reabsorbed.
- This shows that tubular reabsorption is quantitatively very large.
- This also shows that tubular reabsorption is highly selective.
KEY CONCEPT
Tubular reabsorption occurs through active and passive transport mechanisms. Substances move from the tubular lumen to the blood through transcellular or paracellular pathways and then enter peritubular capillaries by bulk flow. Final urinary excretion depends on glomerular filtration, tubular reabsorption, and tubular secretion, with tubular reabsorption being the most important process for many substances.
TUBULAR REABSORPTION — UNDERSTANDING OF THE DIAGRAM
First Understand the Big Picture
The kidney initially filters a huge amount of fluid.
Most of this filtered fluid is not lost in urine.
Instead, the kidney takes back:
- Water
- Sodium
- Glucose
- Amino acids
- Bicarbonate
- Other useful substances
This process is called:
REABSORPTION
RIGHT SIDE = FILTRATION
Lumen
This is the inside of the renal tubule.
It contains:
- Filtered water
- Filtered solutes
Think of it as:
🪣 “The filtrate bucket”
Everything starts here.
MIDDLE = TUBULAR CELLS
These cells act like:
SECURITY GATES
They decide:
✅ What should return to blood
❌ What should remain in urine
LEFT SIDE = PERITUBULAR CAPILLARY
This is the blood vessel surrounding the tubule.
Anything reabsorbed eventually enters here.
Think of it as:
🩸 “The blood recovery vessel”
STEP 1: SOLUTES LEAVE THE LUMEN
Useful substances move from lumen toward blood.
Examples:
- Sodium
- Glucose
- Amino acids
- Chloride
TWO ROUTES FOR SOLUTES
1. TRANSCELLULAR PATH
Through the Cell
Lumen
↓
Tubular Cell
↓
Interstitial Fluid
↓
Blood
The substance passes THROUGH the cell.
Can Occur By
Active Transport
Requires ATP
Examples:
- Sodium
- Glucose (secondary active)
Passive Diffusion
No ATP needed
Moves down concentration gradient.
Diagram
The ATP circle represents:
⚡ Energy used for active transport.
Easy Analogy
Imagine entering a building through the main door.
You pass THROUGH the building.
This is:
Transcellular Path
2. PARACELLULAR PATH
Between Cells
Lumen
↓
Between adjacent cells
↓
Interstitial Fluid
↓
Blood
Substances never enter the cells.
They move through spaces between cells.
Easy Analogy
Instead of entering the building,
you walk through an alley between two buildings.
This is:
Paracellular Path
STEP 2: WATER FOLLOWS
After sodium and solutes are reabsorbed:
Water follows them.
Why?
Because water moves toward areas with higher solute concentration.
This process is called:
OSMOSIS
Diagram
H₂O
↓
Osmosis
↓
Leaves lumen
Easy Analogy
Salt attracts water.
Where sodium goes,
water follows.
STEP 3: INTERSTITIAL FLUID
Everything arriving from the tubule first enters:
Renal Interstitial Fluid
This acts like a:
🚉 Transit station
between tubule and blood.
STEP 4: BULK FLOW
Now water and solutes enter the peritubular capillary.
This movement is called:
BULK FLOW
What Is Bulk Flow?
Large amounts of fluid move together from interstitium into blood.
This occurs because of Starling forces.
Easy Analogy
People leave a train station and enter a bus.
Similarly:
Interstitial fluid
↓
Peritubular capillary
WHAT FINALLY HAPPENS?
Reabsorbed Substances
Lumen
↓
Tubular Cell / Between Cells
↓
Interstitial Fluid
↓
Peritubular Capillary
↓
Blood
Returned to the body
Non-Reabsorbed Substances
Remain inside tubule
↓
Move forward
↓
Become urine
↓
Excretion
COMPLETE STORY OF THE DIAGRAM
Filtration
Blood → Tubule
↓
Reabsorption
Tubule → Blood
↓
Solutes move by:
- Active transport (ATP)
- Passive diffusion
- Paracellular movement
↓
Water follows by osmosis
↓
Water and solutes enter capillaries by bulk flow
↓
Useful substances return to blood
↓
Unwanted substances remain for excretion
KEY CONCEPT
Reabsorption occurs when filtered solutes and water move from the tubular lumen back into the blood. Solutes can move through tubular cells (transcellular pathway) or between cells (paracellular pathway). Water follows by osmosis, and both water and solutes finally enter peritubular capillaries by bulk flow.
ONE-LINE EXAM POINT
Tubular reabsorption involves movement of solutes from the tubular lumen to blood by active transport, passive diffusion, or paracellular transport, while water follows mainly by osmosis and enters the peritubular capillaries by bulk flow.Q
10000 chACTIVE TRANSPORT
- Active transport moves a solute against its electrochemical gradient.
- Active transport requires energy derived from metabolism.
- Transport that uses energy directly from ATP hydrolysis is called primary active transport.
- ATP stands for adenosine triphosphate.
- An example of primary active transport is the Na⁺-K⁺ ATPase pump.
- The Na⁺-K⁺ ATPase pump functions throughout most parts of the renal tubule.
- The Na⁺-K⁺ ATPase pump also functions in many other cells of the body.
Primary Active Transport
ATP Energy → Na⁺-K⁺ ATPase Pump → Solute Transport
- Some transport processes use energy indirectly.
- These processes depend on an ion gradient.
- This type of transport is called secondary active transport.
Secondary Active Transport
Ion Gradient → Solute Transport
- Reabsorption of glucose by the renal tubule is an example of secondary active transport.
- Solutes can be reabsorbed by active transport.
- Solutes can also be reabsorbed by passive transport.
- Water is always reabsorbed passively across the tubular epithelial membrane.
- Water reabsorption occurs by osmosis.
Simple Comparison
Primary Active Transport
- Uses ATP directly.
- Example: Na⁺-K⁺ ATPase pump.
Secondary Active Transport
- Uses energy stored in an ion gradient.
- Example: Glucose reabsorption.
Water Reabsorption
- Always passive.
- Occurs by osmosis.
KEY CONCEPT
Active transport requires energy and can move substances against their electrochemical gradient. Primary active transport uses ATP directly, while secondary active transport uses energy stored in ion gradients. Water is never actively transported and is always reabsorbed passively by osmosis.
SOLUTES CAN BE TRANSPORTED THROUGH EPITHELIAL CELLS OR BETWEEN CELLS
- Renal tubular cells are held together by tight junctions.
- Tight junctions connect neighboring epithelial cells.
- Lateral intercellular spaces are located behind the tight junctions.
- These spaces separate the epithelial cells of the tubule.
- Solutes can be reabsorbed across the cells.
- Solutes can also be secreted across the cells.
- Movement through the cells is called the transcellular pathway.
Transcellular Pathway
Tubular Lumen → Tubular Cell → Interstitial Fluid
- Solutes can also move between the cells.
- This movement occurs across the tight junctions and intercellular spaces.
- Movement between the cells is called the paracellular pathway.
Paracellular Pathway
Tubular Lumen → Between Cells → Interstitial Fluid
- Tight junctions contain several proteins.
- These proteins include occludin.
- These proteins include claudins.
- These proteins include junctional adhesion molecules.
- These proteins join epithelial cells together.
- These proteins regulate paracellular movement of water and solutes.
- In mammalian kidneys, differences in tight junction proteins cause a greater than 100-fold decrease in paracellular permeability from the proximal tubule to the collecting duct.
Easy Concept
Proximal Tubule → High Paracellular Permeability
↓
Collecting Duct → Very Low Paracellular Permeability
More than 100-fold decrease
- Tight junction proteins also determine which substances can move through the paracellular pathway.
- These proteins can form pores.
- These proteins can also form barriers.
- In the proximal tubule, claudins help in paracellular reabsorption of salt.
- In the proximal tubule, claudins help in paracellular reabsorption of water.
- In the thick ascending loop of Henle, claudins help in paracellular reabsorption of calcium.
- In the thick ascending loop of Henle, claudins help in paracellular reabsorption of magnesium.
- These claudins are regulated by the calcium-sensing receptor.
- In the distal nephron, claudins form tight barriers to paracellular movement of cations.
- Some substances can move by both transcellular and paracellular pathways.
- Sodium is one example.
- In some nephron segments, especially the proximal tubule, water is reabsorbed through the paracellular pathway.
- Substances dissolved in this water move with the reabsorbed fluid between the cells.
- These substances include sodium ions.
- These substances include potassium ions.
- These substances include magnesium ions.
- These substances include chloride ions.
KEY CONCEPT
Solutes can move through renal tubular cells by the transcellular pathway or between cells by the paracellular pathway. Tight junction proteins regulate paracellular permeability and selectivity. In the proximal tubule, large amounts of water and ions are reabsorbed through the paracellular route, whereas the distal nephron forms a much tighter barrier to paracellular movement.
PRIMARY ACTIVE TRANSPORT THROUGH THE TUBULAR MEMBRANE IS LINKED TO HYDROLYSIS OF ADENOSINE TRIPHOSPHATASE
- Primary active transport can move solutes against an electrochemical gradient.
- This process requires energy.
- The energy comes from the hydrolysis of ATP (adenosine triphosphate).
- ATP is broken down by a membrane-bound enzyme called ATPase.
- ATPase is also part of the carrier mechanism that binds and transports solutes across the cell membrane.
- Important primary active transporters in the kidneys include:
- Na⁺-K⁺ ATPase
- Hydrogen ATPase
- Hydrogen-Potassium ATPase
- Calcium ATPase
Example: Sodium Reabsorption in the Proximal Tubule
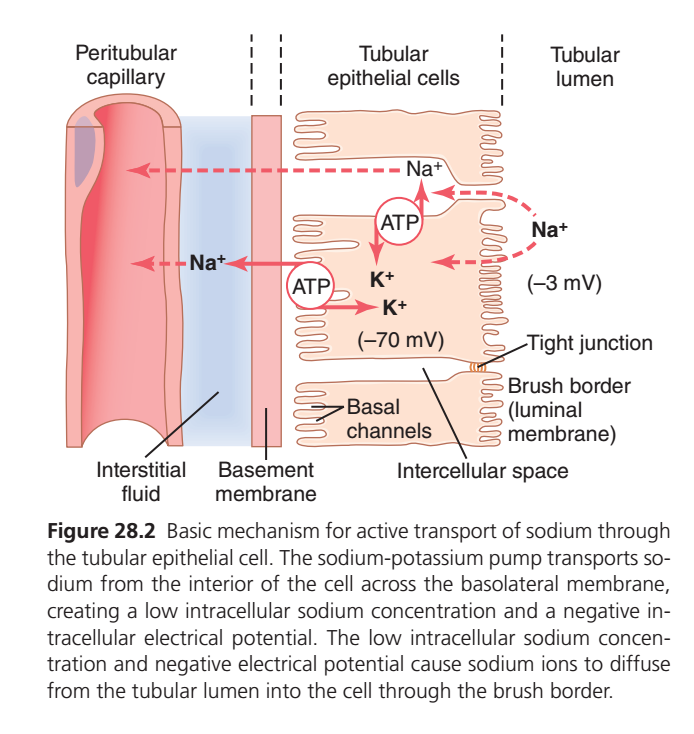
- Sodium reabsorption in the proximal tubule is an example of primary active transport.
- The basolateral membrane contains large amounts of Na⁺-K⁺ ATPase.
- Na⁺-K⁺ ATPase hydrolyzes ATP.
- The released energy pumps sodium out of the cell into the interstitial fluid.
- At the same time, potassium moves into the cell from the interstitial fluid.
Effect of the Na⁺-K⁺ ATPase Pump
- The pump keeps intracellular sodium concentration low.
- The pump keeps intracellular potassium concentration high.
- The pump creates an intracellular electrical potential of about −70 mV.
Easy Conceptual Values
Inside Cell Sodium = 12 mEq/L
Tubular Fluid Sodium = 140 mEq/L
Concentration Gradient Calculation
140 − 12 = 128 mEq/L
- Therefore, sodium has a strong tendency to move from the tubular fluid into the cell.
Electrical Gradient
Cell Potential = −70 mV
- The inside of the cell is negative.
- Sodium ions are positively charged.
- Therefore, the negative cell interior attracts sodium into the cell.
Why Sodium Enters the Cell Easily
Reason 1
- Sodium concentration is higher in the tubular fluid (140 mEq/L).
- Sodium concentration is lower inside the cell (12 mEq/L).
140 → 12
- Sodium diffuses down its concentration gradient into the cell.
Reason 2
- The cell interior is negatively charged (−70 mV).
- Positive sodium ions are attracted into the cell.
Net Effect
Low Intracellular Sodium + Negative Cell Interior
↓
Sodium Diffuses from Tubular Lumen into Cell
Special Adaptations in the Proximal Tubule
- The luminal membrane contains an extensive brush border.
- The brush border increases surface area by about 20-fold.
Easy Conceptual Calculation
Normal Surface Area = 1
Brush Border Surface Area = 20
Increase = 20-fold
- This large surface area increases sodium reabsorption.
- The luminal membrane also contains sodium carrier proteins.
- These carrier proteins bind sodium at the luminal surface.
- These carrier proteins release sodium inside the cell.
- This process facilitates sodium movement into the cell.
- These sodium carrier proteins also help transport glucose.
- These sodium carrier proteins also help transport amino acids.
Three Steps of Sodium Reabsorption
Step 1
- Sodium diffuses across the luminal (apical) membrane into the cell.
- This movement occurs down the electrochemical gradient created by the Na⁺-K⁺ ATPase pump.
Tubular Lumen → Cell
Step 2
- Sodium is actively transported across the basolateral membrane.
- The Na⁺-K⁺ ATPase pump moves sodium into the interstitial fluid.
Cell → Interstitial Fluid
Step 3
- Sodium moves from the interstitial fluid into the peritubular capillaries.
- Water and other substances move with it.
- This movement occurs by ultrafiltration.
- Ultrafiltration is a passive process.
- Ultrafiltration is driven by:
- Hydrostatic pressure gradients
- Colloid osmotic pressure gradients
Interstitial Fluid → Peritubular Capillary → Blood
Complete Pathway
Tubular Lumen
↓
Tubular Cell
↓
Interstitial Fluid
↓
Peritubular Capillary
↓
Blood
KEY CONCEPT
The Na⁺-K⁺ ATPase pump is the most important primary active transport mechanism in the kidney. It uses ATP to pump sodium out of tubular cells, creating low intracellular sodium and a negative intracellular charge. These gradients drive sodium entry from the tubular lumen, allowing efficient reabsorption of sodium and many other substances.
ACTIVE REABSORPTION OF SODIUM (Na⁺) — EASIEST CONCEPTUAL UNDERSTANDING
Main Idea of the Diagram
This figure explains:
How sodium (Na⁺) moves from the tubular fluid back into the blood.
The entire process is driven by:
Na⁺/K⁺ ATPase Pump
located on the basolateral membrane of tubular cells.
FIRST IDENTIFY THE THREE AREAS
1. Tubular Lumen (Right Side)
Contains filtered fluid.
This is where sodium starts.
Think of it as:
🪣 “Filtered urine before reabsorption”
2. Tubular Epithelial Cell (Middle)
Acts as a transporter.
Sodium must enter this cell first.
3. Peritubular Capillary (Left Side)
Final destination.
This is where sodium returns to blood.
🩸 “Recovery vessel”
STEP 1
Na⁺/K⁺ Pump Creates the Driving Force
Look at the ATP circles.
These represent:
Na⁺/K⁺ ATPase Pump
What Does This Pump Do?
Using ATP:
Pumps 3 Na⁺ OUT
and
Pumps 2 K⁺ IN
Result
Inside the cell:
- Sodium becomes very low.
- Potassium becomes high.
Why Is This Important?
The cell is constantly removing sodium.
Therefore:
Cell “wants” more sodium.
A concentration gradient is created.
STEP 2
Cell Becomes Negatively Charged
The figure shows:
Cell Interior = −70 mV
Tubular Lumen = −3 mV
Because positive sodium is pumped out:
the inside becomes more negative.
Why Is This Important?
Positive sodium ions are attracted toward negative areas.
Therefore:
Na⁺ is pulled into the cell.
STEP 3
Sodium Enters From the Lumen
The brush border (luminal membrane) faces the tubular lumen.
Because:
✅ Sodium concentration inside cell is low
AND
✅ Cell interior is negative
Na⁺ easily diffuses from lumen into cell.
EASY ANALOGY
Imagine a room.
Someone continuously removes people from the room.
Now the room becomes empty.
More people naturally enter.
Similarly:
Na⁺/K⁺ pump removes sodium
↓
Cell becomes sodium-poor
↓
More sodium enters from lumen
STEP 4
Sodium Leaves Cell Toward Blood
After entering the cell:
Na⁺ cannot stay there.
The Na⁺/K⁺ pump again removes it.
Direction
Tubular Lumen
↓
Tubular Cell
↓
Interstitial Fluid
↓
Peritubular Capillary
↓
Blood
ROLE OF POTASSIUM (K⁺)
The pump continuously brings K⁺ into the cell.
Some K⁺ leaves again through:
Basal Potassium Channels
(shown in the diagram)
This helps maintain:
- Negative membrane potential
- Pump activity
WHAT IS THE REAL ENERGY-REQUIRING STEP?
Students often think:
“Sodium entering from lumen requires ATP.”
❌ Wrong
Sodium Entry Into Cell
Occurs by diffusion.
No ATP directly needed.
Sodium Exit From Cell
Via Na⁺/K⁺ Pump
Requires ATP.
✅ This is the active step.
WHY IS SODIUM SO IMPORTANT?
When sodium is reabsorbed:
Many other substances follow:
- Water
- Chloride
- Glucose
- Amino acids
- Bicarbonate
Therefore:
Sodium Reabsorption Drives Most Renal Reabsorption
SIMPLE FLOW CHART
ATP Used
↓
Na⁺/K⁺ Pump Removes Na⁺ From Cell
↓
Intracellular Na⁺ Falls
↓
Cell Becomes Negative (−70 mV)
↓
Na⁺ Moves From Lumen Into Cell
↓
Na⁺ Moves Into Interstitial Fluid
↓
Na⁺ Enters Peritubular Capillary
↓
Na⁺ Returns To Blood
KEY CONCEPT
The Na⁺/K⁺ ATPase pump on the basolateral membrane is the primary driving force for sodium reabsorption. By pumping sodium out of the cell, it creates a low intracellular sodium concentration and a negative intracellular potential, causing sodium to diffuse from the tubular lumen into the cell and ultimately back into the blood.
ONE-LINE EXAM POINT
Renal tubular sodium reabsorption is driven primarily by the basolateral Na⁺/K⁺ ATPase pump, which creates a low intracellular sodium concentration and negative intracellular potential that favor sodium entry from the tubular lumen.
SECONDARY ACTIVE REABSORPTION THROUGH THE TUBULAR MEMBRANE
- In secondary active transport, two or more substances are transported together across the membrane.
- These substances use a specific membrane protein called a carrier protein.
- One substance moves down its electrochemical gradient.
- The energy released from this movement drives another substance against its electrochemical gradient.
Basic Concept
Sodium moves downhill
↓
Energy is released
↓
Glucose or amino acid moves uphill
- Secondary active transport does not use ATP directly.
- Secondary active transport does not directly use other high-energy phosphate sources.
- The immediate source of energy comes from the facilitated diffusion of another substance down its own electrochemical gradient.
Example: Glucose Reabsorption
- Glucose reabsorption in the proximal tubule occurs by secondary active transport.
- Specific carrier proteins are present in the brush border.
- These carrier proteins bind a sodium ion and a glucose molecule at the same time.
Co-Transport Process
Sodium + Glucose
↓
Carrier Protein
↓
Enter Tubular Cell Together
- These transport mechanisms are highly efficient.
- They remove almost all glucose from the tubular lumen.
- Amino acids are reabsorbed by a similar mechanism.
Amino Acid Reabsorption
Sodium + Amino Acid
↓
Carrier Protein
↓
Enter Tubular Cell Together
- After entering the cell, glucose moves across the basolateral membrane by diffusion.
- This movement is facilitated by specific transport proteins.
- Amino acids also leave the cell by diffusion through specific transport proteins.
Sodium-Glucose Co-Transporters
- Two sodium-glucose co-transporters are present in the proximal tubule.
- These are SGLT2 and SGLT1.
- These transporters are located on the brush border of proximal tubular cells.
- SGLT2 reabsorbs approximately 90% of filtered glucose.
- SGLT2 is located in the early proximal tubule (S1 segment).
Easy Conceptual Calculation
Total Filtered Glucose = 100%
SGLT2 Reabsorbs = 90%
Remaining = 100% − 90%
Remaining = 10%
- Therefore, only 10% of filtered glucose remains after SGLT2 action.
- SGLT1 reabsorbs the remaining 10% of filtered glucose.
- SGLT1 is located in the later segments of the proximal tubule.
Easy Concept
Filtered Glucose = 100%
↓
SGLT2 Reabsorbs = 90%
↓
Remaining = 10%
↓
SGLT1 Reabsorbs = 10%
↓
Glucose Remaining in Tubule ≈ 0%
- On the basolateral membrane, glucose leaves the cell through glucose transporters.
- GLUT2 is present in the S1 segment.
- GLUT1 is present in the later S3 segment.
Complete Glucose Reabsorption Pathway
Tubular Lumen
↓
SGLT2 / SGLT1
↓
Tubular Cell
↓
GLUT2 / GLUT1
↓
Interstitial Fluid
↓
Peritubular Capillary
↓
Blood
- Glucose transport against its concentration gradient does not directly use ATP.
- However, glucose reabsorption depends on the energy used by the Na⁺-K⁺ ATPase pump.
- The Na⁺-K⁺ ATPase pump creates a sodium gradient across the cell membrane.
Sodium Gradient Formation
Na⁺-K⁺ ATPase Uses ATP
↓
Intracellular Sodium Becomes Low
↓
Sodium Moves into Cell Easily
↓
Energy Becomes Available
↓
Glucose Moves into Cell with Sodium
- Therefore, glucose transport depends indirectly on ATP.
- For this reason, glucose reabsorption is called secondary active transport.
Why Is It Called Secondary Active Transport?
Primary Active Transport
↓
Na⁺-K⁺ ATPase Uses ATP
↓
Creates Sodium Gradient
↓
Secondary Active Transport
↓
Glucose Uses Sodium Gradient to Enter Cell
- A substance is considered actively transported if at least one step in its reabsorption uses primary or secondary active transport.
- Other steps may occur by passive transport.
Glucose Reabsorption Steps
Step 1
- Glucose enters the tubular cell with sodium by secondary active transport.
Step 2
- Glucose leaves the cell across the basolateral membrane by facilitated diffusion.
Step 3
- Glucose enters the peritubular capillaries by bulk flow.
Easy Summary Flow
Tubular Lumen
↓
Secondary Active Transport
↓
Tubular Cell
↓
Facilitated Diffusion
↓
Interstitial Fluid
↓
Bulk Flow
↓
Blood
KEY CONCEPT
Secondary active transport uses the energy stored in the sodium gradient created by the Na⁺-K⁺ ATPase pump. Glucose and amino acids are reabsorbed by co-transport with sodium. About 90% of glucose is reabsorbed by SGLT2 and the remaining 10% by SGLT1, resulting in almost complete glucose reabsorption under normal conditions.
SECONDARY ACTIVE SECRETION INTO THE TUBULES
- Some substances are secreted into the tubules by secondary active transport.
- Secondary active secretion often involves counter-transport with sodium ions.
Counter-Transport
- In counter-transport, two substances move in opposite directions.
- One substance moves down its electrochemical gradient.
- The energy released from this movement drives another substance against its electrochemical gradient.
Basic Concept
Sodium moves downhill
↓
Energy is released
↓
Another substance moves uphill in the opposite direction
- One example is the secretion of hydrogen ions (H⁺) into the tubular lumen.
- This process occurs in the proximal tubule.
- Hydrogen ion secretion is coupled with sodium reabsorption.
Sodium-Hydrogen Counter-Transport
Sodium enters the cell
↓
Hydrogen leaves the cell
↓
Both occur at the same time
- This transport is carried out by a sodium-hydrogen exchanger protein.
- The exchanger is located in the brush border of the luminal membrane.
Step-by-Step Process
Step 1
- Sodium is present in high concentration in the tubular lumen.
Step 2
- Sodium moves into the tubular cell down its electrochemical gradient.
Step 3
- The energy released by sodium entry powers the transport process.
Step 4
- Hydrogen ions are moved out of the cell into the tubular lumen.
Easy Flow Diagram
Tubular Lumen
Na⁺ → Cell
H⁺ ← Cell
(Opposite Directions)
Net Effect
- Sodium is reabsorbed from the tubular lumen into the cell.
- Hydrogen ions are secreted from the cell into the tubular lumen.
Why Is It Called Secondary Active Transport?
- Hydrogen ions move against their gradient.
- The energy does not come directly from ATP.
- The energy comes indirectly from the sodium gradient.
Complete Sequence
Na⁺-K⁺ ATPase Uses ATP
↓
Creates Sodium Gradient
↓
Sodium Moves Into Cell
↓
Energy Released
↓
Hydrogen Secreted Into Tubular Lumen
KEY CONCEPT
Secondary active secretion uses the energy stored in the sodium gradient to move substances into the tubular lumen. In the proximal tubule, sodium reabsorption is coupled with hydrogen ion secretion through the sodium-hydrogen exchanger, causing sodium to enter the cell while hydrogen ions are secreted into the tubular fluid.
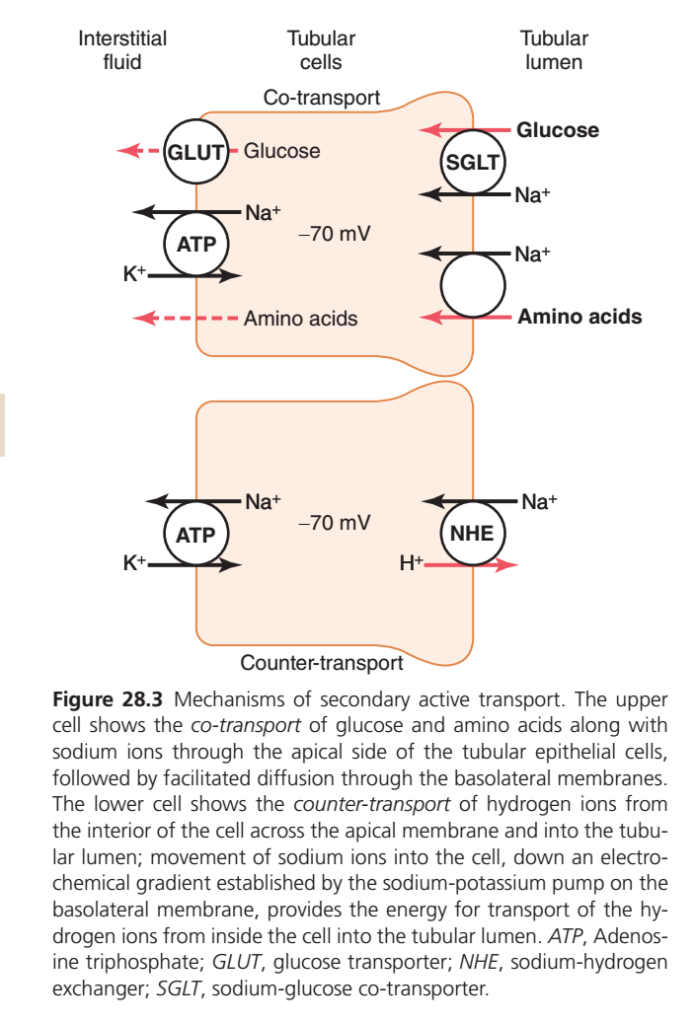
SECONDARY ACTIVE TRANSPORT
Main Idea of the Diagram
The kidney wants to reabsorb:
- Glucose
- Amino acids
- Sodium
and secrete:
- Hydrogen ions (H⁺)
But glucose and amino acids cannot easily move by themselves.
So the kidney uses:
Sodium as a “Transport Taxi” 🚕
The energy ultimately comes from:
Na⁺/K⁺ ATPase Pump
This is why it is called:
Secondary Active Transport
WHY IS IT CALLED SECONDARY ACTIVE?
Primary Active Transport
ATP is used directly.
Example:
Na⁺/K⁺ ATPase Pump
ATP
↓
Pump works
Secondary Active Transport
ATP is NOT used directly by the transporter.
Instead:
ATP
↓
Na⁺/K⁺ Pump creates Na⁺ gradient
↓
Na⁺ gradient provides energy
↓
Other substances move
THE WHOLE SECRET OF THIS DIAGRAM
Everything depends on:
Na⁺/K⁺ ATPase Pump
Located on the basolateral membrane.
It:
- Pumps Na⁺ out
- Brings K⁺ in
Result:
Intracellular Na⁺ becomes very low
and
Cell becomes negative (−70 mV)
Now sodium strongly wants to enter the cell.
This stored energy drives secondary active transport.
UPPER CELL = CO-TRANSPORT (SYMPORT)
Concept
Two substances move in:
SAME DIRECTION
Think:
🚶🚶 Walking together
Example 1: Sodium + Glucose
SGLT
(Sodium-Glucose Cotransporter)
Located on luminal membrane.
What Happens?
Na⁺ wants to enter the cell.
Glucose hitches a ride.
Both enter together
Tubular Lumen
↓
SGLT
↓
Cell
Easy Analogy
Na⁺ = Taxi 🚕
Glucose = Passenger 🧍
Taxi enters the city.
Passenger comes along free.
What Happens Next?
Inside the cell:
Glucose exits through:
GLUT
(Glucose Transporter)
↓
Interstitial Fluid
↓
Blood
Final Result
Glucose Reabsorbed
Example 2: Sodium + Amino Acids
Same principle.
Na⁺ enters cell.
Amino acid rides along.
Both move together.
Memory Trick
CO-TRANSPORT
“CO = Come Together”
Na⁺ + Glucose
Na⁺ + Amino Acid
Move in SAME direction.
LOWER CELL = COUNTER-TRANSPORT (ANTI-PORT)
Concept
Two substances move in:
OPPOSITE DIRECTIONS
Think:
🚶 ← → 🚶
Example: Na⁺ / H⁺ Exchanger (NHE)
Located on luminal membrane.
What Happens?
Na⁺ enters the cell.
At the same time:
H⁺ leaves the cell.
Direction
Na⁺
⬅ Into Cell
H⁺
➡ Into Tubular Lumen
Easy AnalogyA revolving door.
One person enters.
One person exits.
At the same time.
Why Is This Important?
The kidney removes:
Hydrogen ions (H⁺)
This helps regulate:
- Acid-base balance
- Blood pH
MEMORY TRICK
CO-TRANSPORT
Same Direction
Na⁺ + Glucose
Na⁺ + Amino Acids
⬅ ⬅
COUNTER-TRANSPORT
Opposite Directions
Na⁺ enters
H⁺ exits
⬅ ➡
COMPLETE STORY OF THE FIGURE
ATP
↓
Na⁺/K⁺ Pump Creates Low Intracellular Na⁺
↓
Na⁺ Wants To Enter Cell
↓
Na⁺ Gradient Stores Energy
↓
Energy Used For:
Co-Transport
- Na⁺ + Glucose
- Na⁺ + Amino Acids
OR
Counter-Transport
- Na⁺ In
- H⁺ Out
KEY CONCEPTSecondary active transport uses the energy stored in the sodium gradient created by the Na⁺/K⁺ ATPase pump. Sodium moving into the cell drives the reabsorption of glucose and amino acids by co-transport and the secretion of hydrogen ions by counter-transport.
ONE-LINE EXAM POINT
The sodium gradient generated by the Na⁺/K⁺ ATPase pump is the driving force for secondary active transport, including Na⁺-glucose cotransport (SGLT), Na⁺-amino acid cotransport, and Na⁺-H⁺ countertransport (NHE).
PINOCYTOSIS — EASIEST CONCEPTUAL UNDERSTANDING
Main Idea
Most substances are reabsorbed through:
- Channels
- Carriers
- Pumps
But proteins are very large molecules.
❌ Too big to pass through normal transporters.
Therefore the kidney uses:
PINOCYTOSIS
which means:
“Cell Drinking”
or
“Cell Engulfing”
WHERE DOES THIS OCCUR?
Mainly in:
Proximal Tubule
because almost all filtered proteins must be recovered.
WHY IS PINOCYTOSIS NEEDED?
Imagine:
Sodium = Small Person 🚶
Can pass through a door.
Protein = Large Sofa 🛋️
Cannot fit through the door.
The cell must take the whole package inside.
STEP-BY-STEP PROCESS
Step 1: Protein Reaches Tubular Lumen
A small amount of protein is filtered at the glomerulus.
Now it is present in:
Tubular Fluid
Step 2: Protein Attaches to Brush Border
The protein sticks to the:
Brush Border
of proximal tubular cells.
Think of it as:
📦 Package arriving at a warehouse.tep 3: Cell Membrane Folds Around Protein
The luminal membrane bends inward.This is called:
Invagination
Step 4: Vesicle Formation
The membrane pinches off.
A small sac forms.
This sac is called:
Vesicle
The protein is now inside the cell.
Easy Analogy
Imagine catching a fish using a net.
🎣
The membrane wraps around the protein and traps it.
Step 5: Protein Is Digested
Inside the cell:
Protein
↓
Broken into amino acids
by intracellular enzymes.
Step 6: Amino Acids Leave the Cell
The amino acids move through the:
Basolateral Membrane
↓
Interstitial Fluid
↓
Peritubular Capillary
↓
Blood
WHY IS PINOCYTOSIS AN ACTIVE PROCESS?
The cell must:
- Bend its membrane
- Form vesicles
- Move vesicles
- Digest proteins
All of these require:
ATP
Therefore:
Pinocytosis = Active Transport
SIMPLE FLOW CHART
Filtered Protein
↓
Brush Border
↓
Membrane Invagination
↓
Vesicle Formation
↓
Protein Enters Cell
↓
Protein Digested
↓
Amino Acids Formed
↓
Amino Acids Reabsorbed Into Blood
EASY STORY
Imagine a warehouse receiving a large package.
📦 Package arrives
↓
Worker wraps it and brings it inside
↓
Package is opened
↓
Items are separated
↓
Useful items are sent back to the city
This is exactly what proximal tubular cells do with proteins.
KEY CONCEPT
Proteins are too large to be reabsorbed by ordinary transport mechanisms. Proximal tubular cells reabsorb them by pinocytosis, in which the cell membrane surrounds the protein, forms a vesicle, digests the protein into amino acids, and returns the amino acids to the blood.
ONE-LINE EXAM POINT
Pinocytosis is an energy-dependent form of endocytosis used mainly in the proximal tubule for reabsorption of filtered proteins, which are subsequently digested into amino acids and returned to the blood.
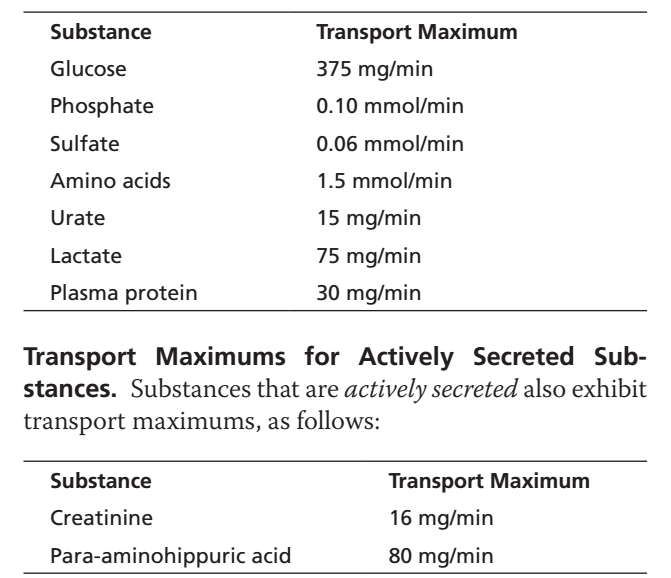
TRANSPORT MAXIMUM FOR SUBSTANCES THAT ARE ACTIVELY REABSORBED
- Most substances that are actively reabsorbed or secreted have a limit to the rate at which they can be transported.
- This limit is called the transport maximum (Tm).
- The transport maximum occurs because the specific transport systems become saturated.
- Saturation occurs when the amount of solute delivered to the tubule becomes greater than the transport capacity.
- The amount of solute delivered to the tubule is called the tubular load.
- The transport capacity depends on the number of carrier proteins.
- The transport capacity also depends on the availability of specific enzymes involved in transport.
- When the tubular load exceeds the transport capacity, the transport systems become saturated.
- The glucose transport system in the proximal tubule is a good example of transport maximum.
- Normally, measurable glucose does not appear in the urine.
- This is because almost all filtered glucose is reabsorbed in the proximal tubule.
- When the filtered load of glucose exceeds the reabsorptive capacity of the tubules, glucose cannot be completely reabsorbed.
- In this situation, glucose appears in the urine.
- Therefore, urinary excretion of glucose occurs when the filtered load exceeds the transport maximum for glucose reabsorption.
KEY CONCEPT
Transport maximum (Tm) is the maximum rate at which a substance can be actively transported. When the tubular load exceeds the transport capacity of carrier proteins and enzymes, the transport system becomes saturated and the excess substance appears in the urine.
TRANSPORT MAXIMUM FOR GLUCOSE
- In an adult human, the transport maximum (Tm) for glucose is about 375 mg/min.
- Under normal conditions, the filtered load of glucose is about 125 mg/min.
Calculation of Normal Filtered Load
Filtered Load = GFR × Plasma Glucose Concentration
= 125 mL/min × 1 mg/mL
= 125 mg/min
Easy Concept
Kidneys filter 125 mg of glucose each minute
↓
Tubules can reabsorb up to 375 mg each minute
↓
All filtered glucose is reabsorbed
↓
No glucose appears in urine
- When GFR increases greatly, the filtered load of glucose increases.
- When plasma glucose concentration increases greatly, the filtered load of glucose also increases.
- If the filtered load rises above 375 mg/min, the tubules cannot reabsorb all the filtered glucose.
- The excess glucose remains in the tubular fluid.
- The excess glucose is excreted in the urine.
Normal Plasma Glucose
- Normal plasma glucose concentration is about 100 mg/100 mL.
Calculation
100 mg/100 mL = 1 mg/mL
Filtered Load = 125 mL/min × 1 mg/mL
= 125 mg/min
- At this level, glucose does not appear in the urine.
Glucose Threshold
- When plasma glucose rises above about 200 mg/100 mL, glucose begins to appear in the urine.
Calculation
200 mg/100 mL = 2 mg/mL
Filtered Load = 125 mL/min × 2 mg/mL
= 250 mg/min
Easy Concept
Plasma Glucose = 200 mg/100 mL
↓
Filtered Load = 250 mg/min
↓
Small amount of glucose begins to appear in urine
- This point is called the renal threshold for glucose.
- The threshold occurs before the transport maximum is reached.
- Not all nephrons have the same transport maximum for glucose.
- Some nephrons begin excreting glucose earlier than others.
- Therefore, glucose appears in the urine before all nephrons reach their maximum transport capacity.
When Transport Maximum Is Reached
Filtered Load = 375 mg/min
↓
All nephrons are working at maximum capacity
↓
Transport Maximum (Tm) Reached
↓
Additional glucose cannot be reabsorbed
↓
Glucose is excreted in urine
- In healthy people, plasma glucose usually does not rise high enough to cause glucose excretion in the urine.
- Even after a meal, plasma glucose usually remains below the threshold level.
- In uncontrolled diabetes mellitus, plasma glucose may rise to very high levels.
- High plasma glucose increases the filtered load of glucose.
- The filtered load may exceed the transport maximum.
- As a result, glucose appears in the urine.
KEY CONCEPT
The transport maximum (Tm) for glucose is about 375 mg/min. Normally, only about 125 mg/min of glucose is filtered, so all of it is reabsorbed. When plasma glucose rises above the renal threshold (about 200 mg/100 mL), glucose begins to appear in the urine. When the filtered load exceeds the transport maximum, the excess glucose cannot be reabsorbed and is excreted in the urine.
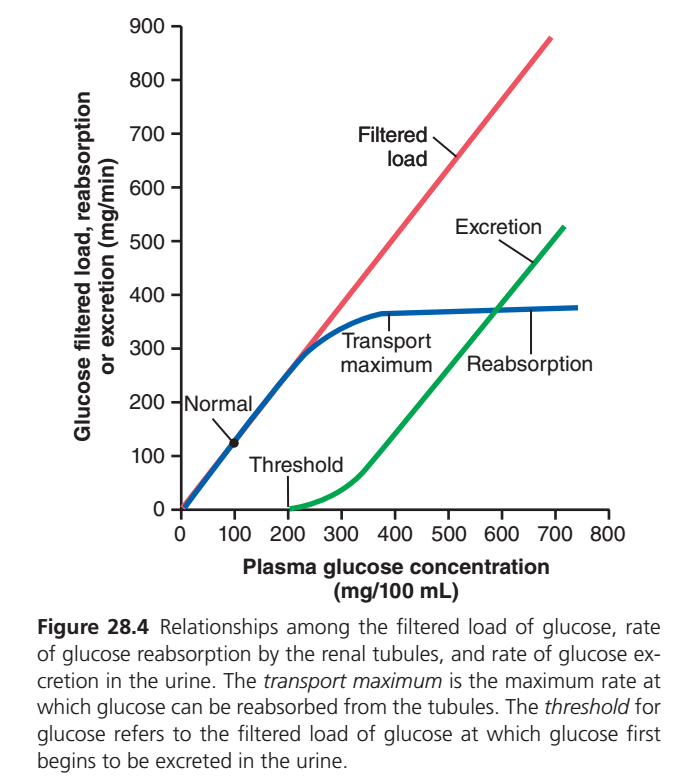
GLUCOSE TRANSPORT MAXIMUM (Tm) GRAPH — EASIEST CONCEPTUAL UNDERSTANDING
This graph explains:
What happens to glucose as blood glucose concentration increases.
The graph contains:
🔴 Filtered Load
🔵 Reabsorption
🟢 Excretion
FIRST UNDERSTAND THE AXES
X-Axis
Plasma Glucose Concentration
(Blood glucose level)
Moving right means:
➡️ Blood glucose is increasing.
Y-Axis
Amount of Glucose
(mg/min)
Represents:
- Filtered glucose
- Reabsorbed glucose
- Excreted glucose
🔴 RED LINE = FILTERED LOAD
What Does It Mean?
Filtered load is:
Amount of glucose filtered by the glomerulus each minute.
Formula:
Filtered Load = GFR × Plasma Glucose
Why Is It a Straight Line?
As blood glucose increases:
More glucose is filtered.
Therefore:
Higher Plasma Glucose
↓
Higher Filtered Load
The increase is proportional.
Easy Analogy
Imagine a conveyor belt.
The more boxes arriving,
the more boxes enter the factory.
🔵 BLUE LINE = REABSORPTION
Initial Part
At normal glucose levels:
All filtered glucose is reabsorbed.
Therefore:
🔵 Blue line overlaps the red line.
Meaning:
Filtered = Reabsorbed
No glucose is lost.Why Does Reabsorption Eventually Flatten?
The kidney has limited glucose transporters:
SGLT transporters
Once all transporters become occupied:
They cannot work any faster.
This maximum capacity is called:
Transport Maximum (Tm)
Approximately:
375 mg/min
Easy Analogy
Imagine 100 seats on a bus.
Once all seats are filled:
No additional passengers can sit.
What Does the Flat Blue Line Mean?
The kidney has reached:
Tm (Maximum Reabsorption Capacity)
All transporters are saturated.
No more glucose can be reabsorbed.
THRESHOLD
Notice the point labeled:
Threshold
What Is Threshold?
The plasma glucose concentration at which:
Glucose first begins to appear in urine.
Important Concept
Threshold occurs BEFORE Tm.
Why?
Because not all nephrons are identical.
Some nephrons become saturated earlier than others.
Therefore:
A small amount of glucose appears in urine before the overall Tm is reached.
Normal Threshold
Approximately:
180–200 mg/100 mL (mg/dL)
🟢 GREEN LINE = EXCRETION
Initially
At normal glucose levels:
All glucose is reabsorbed.
Therefore:
Excretion = Zero
The green line remains on the baseline.
After Threshold
Some transporters become saturated.
Now:
Not all glucose can be reabsorbed.
Excess glucose remains in tubular fluid.
Therefore:
Glucose appears in urine.
The green line begins to rise.
After Tm Is Reached
All transporters are fully saturated.
Now:
Any extra filtered glucose:
Cannot be reabsorbed.
Must be excreted.
Therefore:
Excretion increases rapidly.
The green line rises almost parallel to the red line.
THE MOST IMPORTANT STORY OF THE GRAPH
Normal Blood Glucose (~100 mg/dL)
Filtered glucose
↓
Completely reabsorbed
↓
No glucose in urine
Blood Glucose Reaches Threshold (~180–200 mg/dL)
Some nephrons saturate
↓
Small amount of glucose appears in urine
Blood Glucose Continues Rising
More transporters become saturated
↓
Urinary glucose increases
Tm Reached (~375 mg/min)
All transporters occupied
↓
Maximum reabsorption achieved
↓
Extra glucose must be excreted
EASY MEMORY TRICK
RED LINE
🔴 What enters the nephron
(Filtering)
BLUE LINE
🔵 What returns to blood
(Reabsorption)
GREEN LINE
🟢 What leaves in urine
(Excretion)
WHY IS THIS IMPORTANT IN DIABETES?
In diabetes mellitus:
Blood glucose becomes very high.
↓
Filtered glucose increases greatly.
↓
Tm is exceeded.
↓
Glucose appears in urine.
↓
Glucosuria develops.
↓
Water follows glucose.
↓
Polyuria (excessive urination).
KEY CONCEPT
At normal plasma glucose levels, all filtered glucose is reabsorbed. As plasma glucose rises, glucose transporters become saturated. When the threshold is reached, glucose first appears in urine. Once the transport maximum (Tm) is reached, any additional filtered glucose is excreted in urine.
ONE-LINE EXAM POINT
The threshold is the plasma glucose level at which glucose first appears in urine, whereas the transport maximum (Tm) is the maximum rate at which renal tubules can reabsorb glucose (about 375 mg/min).
SUBSTANCES THAT ARE ACTIVELY TRANSPORTED BUT DO NOT EXHIBIT A TYPICAL TRANSPORT MAXIMUM
- Many actively transported substances show a transport maximum (Tm).
- This occurs because the carrier transport system becomes saturated as tubular load increases.
- Some actively reabsorbed substances do not show a typical transport maximum.
- For these substances, the transport rate is determined by other factors.
Factors Determining Transport Rate
- The electrochemical gradient across the membrane.
- The permeability of the membrane to the substance.
- The time that the fluid remains inside the tubule.
- The time a substance remains in the tubule depends on the tubular flow rate.
- This type of transport is called gradient-time transport.
Gradient-Time Transport
Transport Rate Depends On:
- Electrochemical Gradient
- Time in Tubule
Example: Sodium Reabsorption in the Proximal Tubule
- Sodium reabsorption in the proximal tubule is an example of gradient-time transport.
- The maximum transport capacity of the Na⁺-K⁺ ATPase pump is usually much greater than the actual sodium reabsorption rate.
- This occurs because some sodium leaks back into the tubular lumen.
Sodium Reabsorption Cycle
Na⁺ Reabsorbed into Cell
↓
Na⁺ Pumped into Interstitial Fluid
↓
Some Na⁺ Leaks Back into Tubular Lumen
- This back-leak occurs down an electrochemical gradient.
- The back-leak occurs through the junctions between epithelial cells.
Factors Affecting Sodium Back-Leak
- Permeability of the tight junctions.
- Physical forces in the interstitial fluid.
- These physical forces determine the rate of bulk flow reabsorption into the peritubular capillaries.
- Therefore, sodium transport in the proximal tubule follows gradient-time transport principles.
- Sodium transport in the proximal tubule does not follow a typical transport maximum pattern.
Effect of Sodium Concentration
- The higher the sodium concentration in the proximal tubule, the greater the sodium reabsorption rate.
Easy Concept
More Tubular Sodium
↓
Stronger Gradient
↓
More Sodium Reabsorption
Effect of Tubular Flow Rate
- The slower the tubular fluid flow, the longer sodium remains in the tubule.
- The longer sodium remains in the tubule, the more sodium can be reabsorbed.
Easy Concept
Slow Tubular Flow
↓
More Time for Reabsorption
↓
More Sodium Reabsorbed
Distal Nephron
- In the distal parts of the nephron, epithelial cells have much tighter junctions.
- These segments transport smaller amounts of sodium.
- Sodium reabsorption in these segments behaves more like a typical transport maximum system.
- In these segments, sodium transport can become saturated.
- Certain hormones can increase this transport maximum.
- Aldosterone is one example.
- Aldosterone increases sodium reabsorption in the distal nephron.
KEY CONCEPT
Some actively transported substances do not show a true transport maximum. Sodium reabsorption in the proximal tubule mainly follows gradient-time transport, where reabsorption depends on the electrochemical gradient, membrane permeability, and the time tubular fluid remains in the tubule. Slower tubular flow and higher tubular sodium concentration increase sodium reabsorption.
PASSIVE WATER REABSORPTION BY OSMOSIS IS COUPLED MAINLY TO SODIUM REABSORPTION
- When solutes are transported out of the tubule by primary or secondary active transport, their concentration decreases inside the tubule.
- At the same time, solute concentration increases in the renal interstitium.
Easy Concept
Solutes Move Out of Tubule
↓
Tubular Solute Concentration Decreases
↓
Interstitial Solute Concentration Increases
↓
Osmotic Gradient Is Created
- This concentration difference causes water to move by osmosis.
- Water moves in the same direction as the transported solutes.
Water Movement
Tubular Lumen
↓
Renal Interstitium
- Some parts of the nephron are highly permeable to water.
- The proximal tubule is especially permeable to water.
- Water reabsorption occurs very rapidly in the proximal tubule.
- Therefore, only a small concentration gradient develops across the tubular membrane.
Water Reabsorption in the Proximal Tubule
- A large amount of water moves through Aquaporin-1 (AQP-1) channels.
- Water also moves through the tight junctions between epithelial cells.
- The tight junctions permit significant movement of water.
- The tight junctions also allow movement of small ions.
Ions That Can Move Through Tight Junctions
- Sodium
- Chloride
- Potassium
- Calcium
- Magnesium
Solvent Drag
- Water moving through tight junctions carries some dissolved solutes with it.
- This process is called solvent drag.
Easy Concept
Water Moves
↓
Solutes Move With Water
↓
Solvent Drag
- Water reabsorption is closely linked to sodium reabsorption.
- Organic solute reabsorption is also linked to sodium reabsorption.
- Ion reabsorption is also linked to sodium reabsorption.
- Therefore, changes in sodium reabsorption significantly affect water reabsorption.
Easy Concept
More Sodium Reabsorbed
↓
More Water Reabsorbed
↓
More Solutes Reabsorbed
- In the distal parts of the nephron, tight junctions are much less permeable.
- These segments begin in the loop of Henle and continue through the collecting tubule.
- Epithelial cells in these regions have a much smaller membrane surface area.
- Therefore, water cannot easily move through tight junctions in these segments.
Role of ADH
- Antidiuretic hormone (ADH) greatly increases water permeability.
- ADH increases Aquaporin-2 (AQP-2) channels in epithelial cell membranes.
- This occurs in the distal tubules.
- This occurs in the collecting tubules.
Easy Concept
ADH Present
↓
More AQP-2 Channels
↓
Higher Water Permeability
↓
More Water Reabsorption
- Water can move across the tubular epithelium only if the membrane is permeable to water.
- Even a large osmotic gradient cannot move water through an impermeable membrane.
Proximal Tubule
- Water permeability is always high.
- Water is rapidly reabsorbed.
- Water reaches osmotic equilibrium with the surrounding interstitial fluid.
- This high permeability is due to abundant AQP-1 channels.
- AQP-1 channels are present in the luminal membrane.
- AQP-1 channels are present in the basolateral membrane.
Ascending Loop of Henle
- Water permeability is always low.
- Almost no water is reabsorbed.
- This occurs despite a large osmotic gradient.
Distal Tubule and Collecting Duct
- Water permeability depends on the presence or absence of ADH.
- Water moves through aquaporins.
Easy Comparison
Proximal Tubule
- AQP-1 abundant
- Water permeability always high
- Rapid water reabsorption
Ascending Loop of Henle
- Water permeability always low
- Almost no water reabsorption
Distal Tubule & Collecting Duct
- Water permeability depends on ADH
- AQP-2 channels regulate water movement
KEY CONCEPT
Water is reabsorbed passively by osmosis and is closely coupled to sodium reabsorption. In the proximal tubule, abundant AQP-1 channels and leaky tight junctions allow rapid water reabsorption. In the ascending loop of Henle, water permeability is very low. In the distal nephron and collecting ducts, water permeability is controlled by ADH through AQP-2 channels.
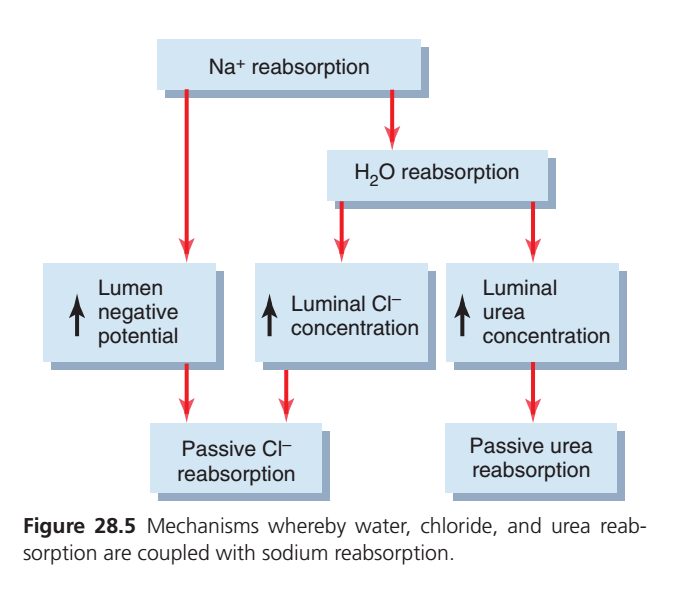
REABSORPTION OF CHLORIDE, UREA, AND OTHER SOLUTES BY PASSIVE DIFFUSION
- When sodium is reabsorbed through the tubular epithelial cells, negative ions such as chloride are transported along with sodium because of electrical potentials.
- Reabsorption of positively charged sodium ions leaves the tubular lumen negatively charged compared with the interstitial fluid.
- This negative charge causes chloride ions to diffuse passively through the paracellular pathway.
- Additional chloride reabsorption occurs because a chloride concentration gradient develops when water is reabsorbed from the tubule by osmosis.
- Water reabsorption concentrates chloride ions in the tubular lumen.
- Thus, active sodium reabsorption is closely coupled to passive chloride reabsorption through:
- An electrical potential.
- A chloride concentration gradient.
- Chloride ions can also be reabsorbed by secondary active transport.
- An important mechanism for chloride reabsorption is co-transport with sodium and potassium across the luminal membrane of the thick ascending loop of Henle.
- Chloride is also co-transported with sodium across the luminal membrane of the distal tubules.
- Urea is also passively reabsorbed from the tubule.
- Urea is reabsorbed to a much lesser extent than chloride ions.
- As water is reabsorbed from the tubules by osmosis coupled to sodium reabsorption, the concentration of urea in the tubular lumen increases.
- This increase in urea concentration creates a concentration gradient that favors urea reabsorption.
- Urea does not pass through the tubular membrane as readily as water.
- In some parts of the nephron, especially the inner medullary collecting duct, passive urea reabsorption is facilitated by specific urea transporters.
- Only about half of the urea filtered by the glomerular capillaries is reabsorbed from the tubules.
- The remaining urea passes into the urine.
- This allows the kidneys to excrete large amounts of this waste product of metabolism.
- In mammals, more than 90% of waste nitrogen is normally excreted by the kidneys as urea.
- Most of this waste nitrogen is generated in the liver as a product of protein metabolism.
- Creatinine is another waste product of metabolism.
- Creatinine is a larger molecule than urea.
- Creatinine is essentially impermeable to the tubular membrane.
- Therefore, almost none of the filtered creatinine is reabsorbed.
- Virtually all creatinine filtered by the glomerulus is excreted in the urine.
KEY CONCEPT
Active sodium reabsorption promotes passive chloride reabsorption through electrical and concentration gradients. Urea is partially reabsorbed because water reabsorption increases its concentration in the tubular lumen, whereas creatinine is almost not reabsorbed and is therefore excreted almost completely in the urine.
Summarized Essay
After glomerular filtration, the filtrate enters the renal tubules and passes through the proximal tubule, loop of Henle, distal tubule, collecting tubule, and collecting duct before becoming urine. During this journey, some substances are reabsorbed back into the blood, while others are secreted into the tubular fluid. Therefore, the final amount of any substance excreted in the urine depends on the balance between glomerular filtration, tubular reabsorption, and tubular secretion. For most substances, tubular reabsorption is much more important than secretion in determining urinary excretion.
Tubular reabsorption is both quantitatively enormous and highly selective. Although the kidneys filter about 180 liters of fluid per day, only about 1–2 liters are excreted as urine because most filtered water and solutes are reabsorbed. Even small changes in tubular reabsorption can produce very large changes in urine volume. Unlike glomerular filtration, which is relatively nonselective, tubular reabsorption is highly selective. Essential nutrients such as glucose and amino acids are almost completely reabsorbed, while electrolytes such as sodium, chloride, and bicarbonate are reabsorbed according to the body’s needs. In contrast, waste products such as urea and creatinine are poorly reabsorbed and are therefore excreted.
For a substance to be reabsorbed, it must first move from the tubular lumen into the renal interstitial fluid and then from the interstitium into the peritubular capillaries. Reabsorption may occur through the cells (transcellular pathway) or between adjacent cells (paracellular pathway). Water and solutes are then returned to the blood through the peritubular capillaries by bulk flow driven by hydrostatic and osmotic forces.
Tubular reabsorption occurs through both active and passive transport mechanisms. Active transport requires energy and can move substances against their concentration gradients. The most important active transport system in the kidney is the Na⁺-K⁺ ATPase pump, located on the basolateral membrane of tubular epithelial cells. This pump actively transports sodium out of the cell and potassium into the cell, creating conditions that favor sodium entry from the tubular lumen. Because sodium transport drives many other transport processes, it serves as the major force behind tubular reabsorption.
Many substances are reabsorbed through secondary active transport, in which sodium moving down its electrochemical gradient provides energy for transport of another substance. Glucose and amino acids are important examples. In the proximal tubule, sodium and glucose enter the cell together through sodium-glucose co-transporters (SGLT2 and SGLT1). Glucose then leaves the cell through glucose transporters and enters the blood. Because of these highly efficient transport systems, virtually all filtered glucose is normally reabsorbed.
Secondary active transport is also involved in tubular secretion. For example, hydrogen ions are secreted into the tubular lumen through a sodium-hydrogen exchanger. As sodium enters the tubular cell, hydrogen ions are simultaneously moved into the tubular fluid, helping regulate acid-base balance.
Large molecules such as proteins are reabsorbed mainly by pinocytosis, a special form of active transport. In this process, proteins attach to the tubular cell membrane, are engulfed into vesicles, and then digested into amino acids that are returned to the bloodstream. This mechanism is especially important in the proximal tubule.
Many actively transported substances exhibit a transport maximum (Tm), which represents the maximum rate at which they can be reabsorbed or secreted. Glucose is a classic example. Normally, all filtered glucose is reabsorbed, but when blood glucose levels become excessively high, as in uncontrolled diabetes mellitus, the filtered load exceeds the transport maximum. Excess glucose then appears in the urine, producing glucosuria. The plasma concentration at which glucose first appears in urine is known as the renal threshold for glucose.
Water reabsorption occurs entirely by osmosis and is closely linked to sodium reabsorption. When sodium is actively transported from the tubular lumen into the interstitial fluid, an osmotic gradient develops that causes water to follow. The proximal tubule is highly permeable to water because it contains abundant aquaporin-1 (AQP-1) water channels. Consequently, large amounts of water are reabsorbed in this segment.
In the distal nephron and collecting ducts, water permeability is much lower and depends largely on antidiuretic hormone (ADH). ADH increases insertion of aquaporin-2 (AQP-2) channels into the tubular membrane, greatly increasing water reabsorption. In the absence of ADH, these segments remain relatively impermeable to water, resulting in the excretion of more dilute urine.
Many solutes are reabsorbed passively. Chloride ions often follow sodium because sodium reabsorption creates electrical and concentration gradients that favor chloride diffusion. Similarly, as water is reabsorbed, the concentration of urea in the tubular fluid increases, promoting passive urea diffusion back into the interstitium. However, only about half of the filtered urea is reabsorbed, allowing the kidneys to eliminate large amounts of nitrogenous waste. In contrast, creatinine is minimally reabsorbed and is therefore excreted almost entirely in the urine.
In summary, tubular reabsorption is a highly selective and energy-dependent process that allows the kidneys to conserve essential substances while eliminating waste products. Through a combination of active transport, passive diffusion, secondary active transport, pinocytosis, and osmotic water movement, the kidneys precisely regulate body fluid composition and maintain homeostasis.