


- Feedback mechanisms that are intrinsic to the kidneys normally keep renal blood flow relatively constant.
- These mechanisms also keep GFR relatively constant.
- This occurs despite marked changes in arterial blood pressure.
- These mechanisms continue to function in blood-perfused kidneys removed from the body.
- These mechanisms function independently of systemic influences.
- The relative constancy of GFR and renal blood flow is called autoregulation.
- In most tissues, the primary function of blood flow autoregulation is to maintain normal delivery of oxygen and nutrients.
- In most tissues, autoregulation also helps remove metabolic waste products.
- This occurs despite changes in arterial pressure.
- In the kidneys, normal blood flow is much higher than that required for these functions.
- The major function of autoregulation in the kidneys is to maintain a relatively constant GFR.
- The major function of autoregulation in the kidneys is to allow precise control of renal excretion of water and solutes.
- GFR normally remains relatively constant despite considerable fluctuations in arterial pressure.
- These pressure fluctuations occur during a person’s normal daily activities.
Example
- Arterial pressure decreases from normal to 70–75 mm Hg.
- Or arterial pressure increases to 160–180 mm Hg.
- Despite these changes, GFR usually changes by less than 10%.
Conceptual Calculation
- If normal GFR = 100%
- Maximum change in GFR = less than 10%
Lowest GFR ≈ 90% of normal
Highest GFR ≈ 110% of normal
- Thus, even with large changes in arterial pressure, GFR remains close to normal.
- Renal blood flow is generally autoregulated in parallel with GFR.
- Under certain conditions, GFR is autoregulated more efficiently than renal blood flow.
KEY CONCEPT
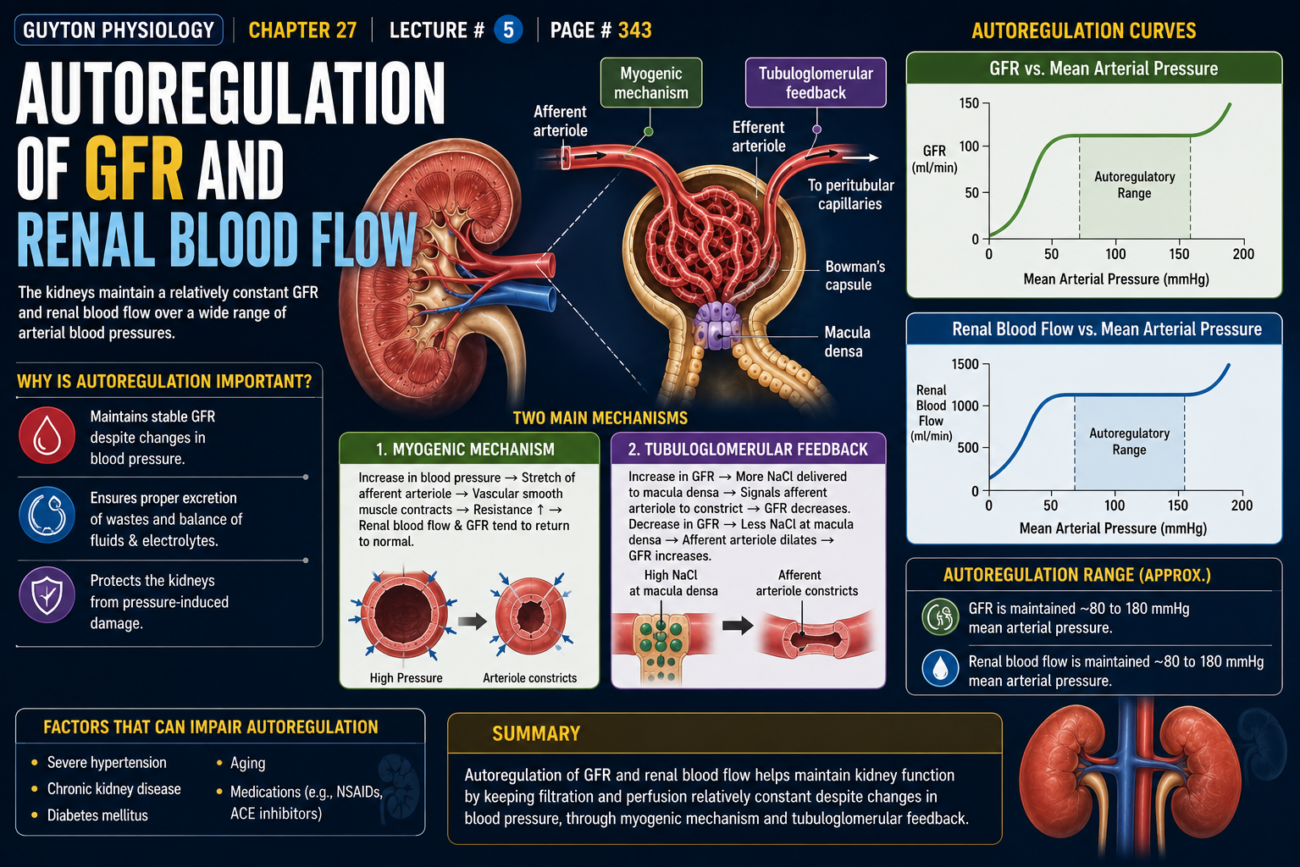
Autoregulation is the intrinsic ability of the kidneys to keep GFR and renal blood flow relatively constant despite large changes in arterial pressure. The main purpose is to maintain stable filtration and precise control of water and solute excretion.
AUTOREGULATION OF THE KIDNEY — CONCEPTUAL SUMMARY
First Understand the Main Idea
The kidney has a special ability called:
Autoregulation
This means:
👉 The kidney can keep Renal Blood Flow (RBF) and Glomerular Filtration Rate (GFR) almost constant even when blood pressure changes.
Think of the kidney as a smart water filter.
Even if water pressure changes, the filter tries to keep filtering at the same rate.
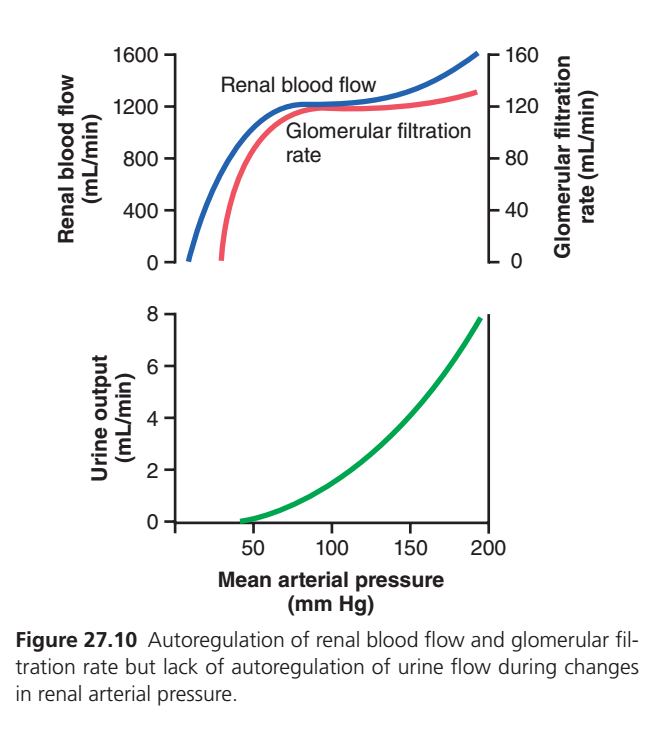
BLUE LINE = RENAL BLOOD FLOW (RBF)
What does it show?
The blue line represents:
Blood entering the kidneys per minute.
At Low Blood Pressure
When mean arterial pressure is very low:
- Little blood reaches the kidney.
- Renal blood flow is low.
Therefore the blue line rises sharply.
Between About 80–180 mm Hg
The blue line becomes almost flat.
This is the important part.
Although blood pressure keeps increasing:
- Kidney blood flow remains nearly constant.
- The kidney automatically adjusts vessel diameter.
This is called:
Autoregulation of Renal Blood Flow
Easy Analogy
Imagine a water pipe with an automatic valve.
If pressure increases:
🚰 Valve partially closes.
If pressure decreases:
🚰 Valve opens wider.
Result:
Water flow stays almost constant.
The kidney does the same thing.
RED LINE = GLOMERULAR FILTRATION RATE (GFR)
What does it show?
The red line represents:
Amount of filtrate formed each minute.
Normal value:
≈ 125 mL/min
At Low Blood Pressure
Blood pressure is too low.
Not enough filtration occurs.
GFR is low.
Therefore the red line rises steeply.
Between About 80–180 mm Hg
The red line becomes almost flat.
This means:
Even though arterial pressure changes greatly:
- GFR remains nearly constant.
- Nephrons keep filtering at almost the same rate.
This is:
Autoregulation of GFR
Easy Analogy
Think of a coffee filter.
Even if water pressure changes slightly:
☕ The amount of coffee produced per minute remains almost the same.
The kidney tries to do exactly this.
WHY ARE THE BLUE AND RED LINES FLAT?
Because of two major autoregulatory mechanisms:
1. Myogenic Mechanism
When pressure increases:
- Afferent arteriole stretches.
- It automatically constricts.
Less blood enters.
Flow stays stable.
2. Tubuloglomerular Feedback
Macula densa senses excess filtration.
Then:
- Signals afferent arteriole to constrict.
- Prevents excessive filtration.
Result:
GFR remains stable.
GREEN LINE = URINE OUTPUT
This graph is the most important part.
What Does It Show?
Green line represents:
Amount of urine produced per minute.
Unlike RBF and GFR
Urine output is NOT autoregulated.
The kidney intentionally allows urine formation to change.
As Blood Pressure Rises
Higher pressure causes:
- More sodium excretion
- More water excretion
Therefore:
Urine output increases greatly.
This phenomenon is called:
Pressure Diuresis
Easy Analogy
Imagine a dam.
Normal water level:
💧 Small amount released.
High water level:
💧💧💧 Large amount released.
The kidney behaves similarly.
Higher pressure → more urine released.
Why Doesn’t the Green Line Stay Flat?
Because the body uses urine formation to control blood volume and blood pressure.
If blood pressure becomes high:
Kidneys remove:
- More water
- More sodium
This lowers:
- Blood volume
- Blood pressure
Therefore urine output increases.
WHAT IS THE MAIN DIFFERENCE?
| Line | Represents | Autoregulated? |
|---|---|---|
| 🔵 Blue | Renal Blood Flow (RBF) | Yes |
| 🔴 Red | Glomerular Filtration Rate (GFR) | Yes |
| 🟢 Green | Urine Output | No |
SIMPLE STORY OF THE WHOLE GRAPH
Imagine blood pressure rises from 80 to 180 mm Hg.
Kidney Blood Flow (Blue)
🟦 “I will stay almost the same.”
GFR (Red)
🟥 “I will also stay almost the same.”Urine Output (Green)
🟩 “I will increase a lot to remove extra water and salt.”
KEY CONCEPT
🔵 Blue Line: Renal blood flow remains nearly constant because of autoregulation.
🔴 Red Line: GFR remains nearly constant because of autoregulation.
🟢 Green Line: Urine output is not autoregulated and increases markedly with rising arterial pressure (pressure diuresis).
ONE-LINE EXAM POINT
The kidneys autoregulate renal blood flow and GFR over a wide range of arterial pressures, but urine output increases markedly with increasing arterial pressure because of pressure diuresis and natriuresis.
IMPORTANCE OF GFR AUTOREGULATION — CONCEPTUAL UNDERSTANDING
Imagine the Kidney as a Water Treatment Plant 🚰
Every day, the kidneys filter a huge amount of fluid:
Normal Situation
- GFR = 180 L/day filtered
- Tubules reabsorb = 178.5 L/day
- Urine excreted = 1.5 L/day
So:
180 L filtered − 178.5 L reabsorbed = 1.5 L urine
The kidneys filter a lot but return almost everything back to the blood.
What Would Happen Without GFR Autoregulation?
Suppose blood pressure rises:
From 100 mm Hg → 125 mm Hg
This is only a 25% increase in pressure.
Without autoregulation:
GFR would also increase by 25%
- GFR = 180 L/day → 225 L/day
Now the kidneys are filtering much more fluid.
The Big Problem
Assume tubular reabsorption remains unchanged:
- Reabsorption = 178.5 L/day
Then:
Urine Output
225 − 178.5 = 46.5 L/day
Compare This With Normal
Normal urine:
➡️ 1.5 L/day
Without autoregulation:
➡️ 46.5 L/day
This is more than:
30 TIMES NORMAL
Why Is This Dangerous?
The total plasma volume is only about:
3 Liters
If kidneys suddenly lost:
46.5 Liters/day
The blood volume would be rapidly depleted.
Result:
- Severe dehydration
- Low blood pressure
- Circulatory collapse
- Death if not corrected
Therefore, the Kidney Needs Autoregulation
The kidney says:
🧠 “Blood pressure increased, but I won’t allow filtration to increase dramatically.”
So:
- Renal Blood Flow remains nearly constant.
- GFR remains nearly constant.
- Massive fluid loss is prevented.
How Does the Kidney Prevent Huge Urine Loss?
Mechanism 1: GFR Autoregulation
When blood pressure rises:
- Afferent arteriole constricts.
- GFR changes very little.
Result:
✅ Prevents huge increases in filtration.
Mechanism 2: Glomerulotubular Balance
Even if GFR rises slightly:
Tubules automatically respond by:
Reabsorbing more fluid
This phenomenon is called:
Glomerulotubular Balance
Meaning:
More filtered → More reabsorbed
Result:
✅ Less fluid reaches the urine.
Does Blood Pressure Still Affect Urine Formation?
YES
Autoregulation is not perfect.
As blood pressure increases:
- More sodium is excreted.
- More water is excreted.
This is called:
Pressure Natriuresis
(Na⁺ loss)
and
Pressure Diuresis
(Water loss)
Why Is Pressure Diuresis Important?
It helps control:
- Body fluid volume
- Extracellular fluid volume
- Blood volume
- Arterial pressure
Easy Analogy
Imagine a house water tank.
Small Rise in Water Pressure
A smart valve prevents flooding.
This is:
GFR Autoregulation
If Water Level Still Becomes Slightly High
An overflow pipe removes extra water.
This is:
Pressure Diuresis
SIMPLE FLOW CHART
↑ Blood Pressure
↓
Kidney Autoregulation Activated
↓
GFR Remains Nearly Constant
↓
Prevents Massive Urine Loss
↓
Protects Blood Volume
KEY CONCEPT
GFR autoregulation is essential because even a small increase in blood pressure could otherwise cause a huge increase in filtration and urine output, rapidly depleting body fluids. Autoregulation and glomerulotubular balance prevent this, while pressure diuresis and pressure natriuresis help regulate body fluid volume and blood pressure.**
ONE-LINE EXAM POINT
The major importance of GFR autoregulation is to prevent extreme changes in renal excretion that would occur with changes in arterial pressure, thereby protecting body fluid volume and blood pressure.
TUBULOGLOMERULAR FEEDBACK AND AUTOREGULATION OF GFR
- The kidneys have a special mechanism called tubuloglomerular feedback (TGF).
- TGF links changes in sodium chloride concentration at the macula densa with the control of renal arteriolar resistance.
- TGF also helps in autoregulation of GFR.
- This feedback helps maintain a relatively constant delivery of sodium chloride to the distal tubule.
- This feedback prevents unnecessary fluctuations in renal excretion.
- In many situations, TGF autoregulates renal blood flow and GFR together.
- In some situations, GFR is autoregulated at the expense of changes in renal blood flow.
- In other situations, TGF may cause changes in GFR in response to primary changes in renal tubular sodium chloride reabsorption.
- The TGF mechanism has two components.
- The first component is an afferent arteriolar feedback mechanism.
- The second component is an efferent arteriolar feedback mechanism.
- These feedback mechanisms depend on the juxtaglomerular complex.
- The juxtaglomerular complex contains macula densa cells in the initial part of the distal tubule.
- The juxtaglomerular complex also contains juxtaglomerular cells in the walls of the afferent and efferent arterioles.
- The macula densa is a specialized group of epithelial cells.
- These cells are located in the distal tubule.
- These cells come into close contact with the afferent and efferent arterioles.
- The macula densa cells contain the Golgi apparatus.
- The Golgi apparatus is directed toward the arterioles.
- This suggests that the macula densa cells may secrete substances toward the arterioles.
- Macula densa cells detect changes in sodium chloride delivery to the distal tubule.
- The exact signaling mechanism is not completely understood.
- Adenosine is likely involved in this signaling process.
- Increased GFR increases sodium chloride delivery to the macula densa.
- Increased sodium chloride delivery activates the sodium-potassium-chloride cotransporter in the macula densa cells.
- Activation of this transporter causes cell depolarization.
- Cell depolarization causes release of ATP.
- ATP is eventually converted into adenosine.
- Adenosine constricts the afferent arterioles.
- Afferent arteriolar constriction decreases glomerular hydrostatic pressure.
- This helps return GFR toward normal.
- Several other factors can influence TGF sensitivity.
- Angiotensin II increases TGF sensitivity.
- Nitric oxide decreases TGF sensitivity.
- Some prostaglandins also decrease TGF sensitivity.
- These factors help regulate sodium chloride excretion.
- Increased sodium chloride intake expands extracellular fluid volume.
- Increased sodium chloride intake reduces renin release.
- Increased sodium chloride intake reduces angiotensin II formation.
- Reduced angiotensin II decreases TGF sensitivity.
- Reduced TGF sensitivity allows increased sodium chloride delivery to the macula densa and distal tubule.
- This occurs without causing TGF-mediated constriction of the afferent arterioles.
- This also occurs without causing a decrease in GFR.
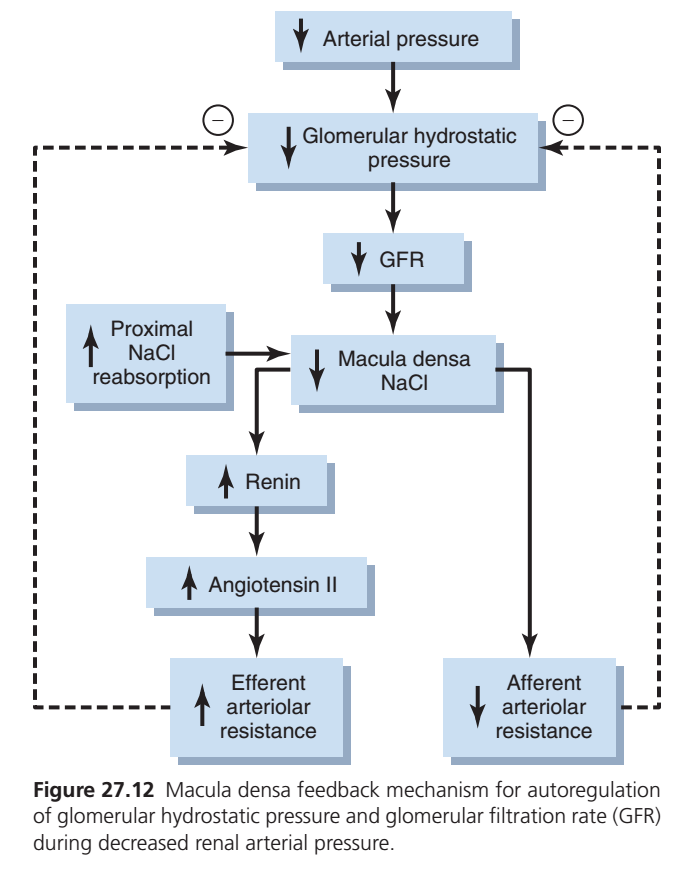
- Decreased GFR slows sodium chloride delivery to the macula densa.
- This causes decreased resistance in the afferent arterioles.
- Decreased afferent arteriolar resistance increases glomerular hydrostatic pressure.
- This helps return GFR toward normal.
- Decreased GFR also increases renin release from juxtaglomerular cells.
- Juxtaglomerular cells are the major storage sites for renin.
- Renin increases the formation of angiotensin I.
- Angiotensin I is converted to angiotensin II.
- Angiotensin II constricts the efferent arterioles.
- Efferent arteriolar constriction increases glomerular hydrostatic pressure.
- This helps return GFR toward normal.
- The afferent and efferent feedback mechanisms work together through the juxtaglomerular apparatus.
- These mechanisms provide feedback signals to the afferent and efferent arterioles.
- These mechanisms allow efficient autoregulation of GFR during changes in arterial pressure.
- When both mechanisms are functioning, GFR changes by only a few percentage points.
- This occurs even when arterial pressure varies between 75 and 160 mm Hg.
KEY CONCEPT
Tubuloglomerular feedback (TGF) maintains stable GFR by sensing sodium chloride delivery at the macula densa. Increased NaCl causes afferent arteriolar constriction and decreased renin release, while decreased NaCl causes afferent arteriolar dilation and increased renin release, leading to efferent arteriolar constriction by angiotensin II. Together, these mechanisms keep GFR nearly constant despite changes in arterial pressure.
HYPOPERFUSION FURTHER REDUCES GFR
- Angiotensin II preferentially constricts the efferent arterioles.
- Efferent arteriolar constriction helps prevent major decreases in glomerular hydrostatic pressure.
- Efferent arteriolar constriction also helps prevent major decreases in GFR.
- This effect becomes important when renal perfusion pressure falls below normal.
- Some drugs block the formation of angiotensin II.
- Angiotensin-converting enzyme (ACE) inhibitors are examples of these drugs.
- Some drugs block the action of angiotensin II.
- Angiotensin II receptor antagonists are examples of these drugs.
- When renal arterial pressure falls below normal, these drugs may cause a greater decrease in GFR than usual.
- Renal artery stenosis is a partial blockage of the renal artery.
- Renal artery stenosis can reduce renal arterial pressure.
- Some patients develop hypertension because of renal artery stenosis.
- In these patients, angiotensin II helps maintain GFR.
- Blocking angiotensin II in these patients may cause a severe decrease in GFR.
- In some cases, a severe decrease in GFR can lead to acute renal failure.
- Despite this risk, angiotensin II–blocking drugs are important therapeutic agents.
- These drugs are used to treat hypertension.
- These drugs are used to treat congestive heart failure.
- These drugs are used to treat other medical conditions.
- Patients receiving these drugs should be monitored carefully.
- Monitoring helps ensure that severe decreases in GFR do not occur.
KEY CONCEPT
When renal perfusion pressure falls, angiotensin II helps maintain GFR by constricting the efferent arteriole. Blocking angiotensin II can cause a marked fall in GFR, especially in patients with renal artery stenosis, and may lead to acute renal failure.
MYOGENIC AUTOREGULATION OF RENAL BLOOD FLOW AND GLOMERULAR FILTRATION RATE
- Another mechanism helps maintain relatively constant renal blood flow and GFR.
- This mechanism is called the myogenic mechanism.
- The myogenic mechanism is the ability of blood vessels to resist stretching when arterial pressure increases.
- Studies show that small arterioles respond to increased wall tension or wall stretch by contracting.
- Stretching of the vascular wall allows more calcium ions to enter the smooth muscle cells.
- Increased calcium entry causes vascular smooth muscle contraction.
- This contraction prevents excessive stretching of the blood vessel.
- This contraction increases vascular resistance.
- Increased vascular resistance helps prevent excessive increases in renal blood flow.
- Increased vascular resistance helps prevent excessive increases in GFR when arterial pressure rises.
- The myogenic mechanism operates in most arterioles throughout the body.
- Some physiologists question its importance in renal blood flow and GFR autoregulation.
- This mechanism cannot directly detect changes in renal blood flow.
- This mechanism cannot directly detect changes in GFR.
- The myogenic mechanism may help protect the kidneys from hypertension-induced injury.
- When blood pressure suddenly increases, afferent arterioles constrict within seconds.
- This rapid constriction reduces transmission of high arterial pressure to the glomerular capillaries.
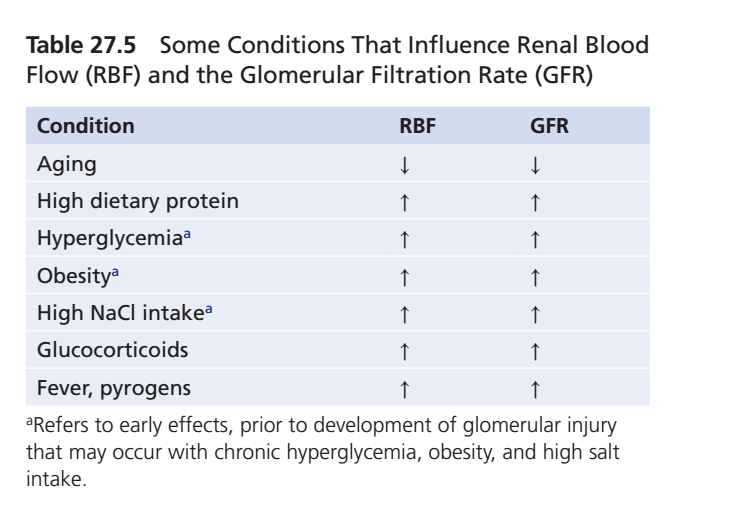
- Renal blood flow and GFR are relatively stable under most conditions.
- However, some conditions can significantly increase renal blood flow and GFR.
- A high-protein intake increases renal blood flow.
- A high-protein intake increases GFR.
- During a long-term high-protein diet, part of the increase in renal blood flow and GFR is due to kidney growth.
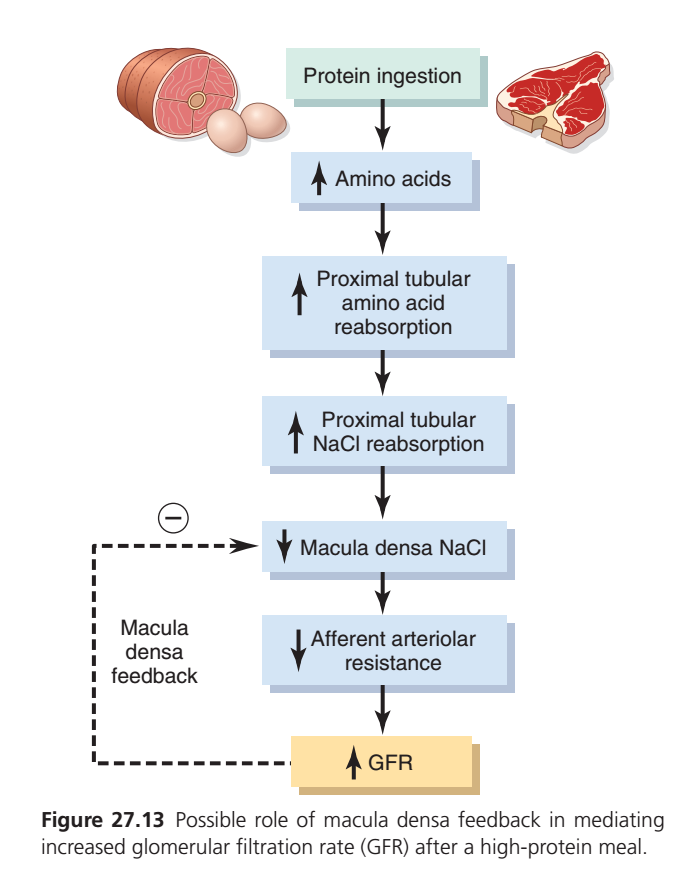
- Renal blood flow and GFR can increase by 20% to 30% within 1 to 2 hours after a high-protein meal.
- Digestion of a high-protein meal releases amino acids into the blood.
- Amino acids are reabsorbed in the proximal tubules.
- Amino acids and sodium are reabsorbed together by co-transport.
- Increased amino acid reabsorption increases sodium reabsorption.
- Increased sodium reabsorption decreases sodium delivery to the macula densa.
High-Protein Meal Sequence
- High-protein meal
→ Increased amino acids in blood - Increased amino acid reabsorption
→ Increased sodium reabsorption - Increased sodium reabsorption
→ Decreased sodium delivery to macula densa - Decreased sodium at macula densa
→ Afferent arteriolar dilation - Afferent arteriolar dilation
→ Increased renal blood flow - Increased renal blood flow
→ Increased GFR - Increased GFR
→ Increased excretion of protein waste products such as urea - A similar mechanism occurs in uncontrolled diabetes mellitus.
- Increased blood glucose levels increase glucose delivery to the tubules.
- Glucose is reabsorbed with sodium in the proximal tubule.
- Increased glucose reabsorption increases sodium reabsorption.
- Increased sodium reabsorption decreases sodium chloride concentration at the macula densa.
- Decreased sodium chloride at the macula densa causes afferent arteriolar dilation.
- Afferent arteriolar dilation increases renal blood flow.
- Afferent arteriolar dilation increases GFR.
Uncontrolled Diabetes Mellitus Sequence
- Increased blood glucose
→ Increased glucose reabsorption
→ Increased sodium reabsorption
→ Decreased sodium chloride at macula densa
→ Afferent arteriolar dilation
→ Increased renal blood flow
→ Increased GFR
- These examples show that renal blood flow and GFR are not the primary variables controlled by tubuloglomerular feedback.
- The main purpose of tubuloglomerular feedback is to maintain a constant delivery of sodium chloride to the distal tubule.
- Increased sodium reabsorption before the macula densa often causes increased renal blood flow.
- Increased sodium reabsorption before the macula densa often causes increased GFR.
- These responses help restore sodium chloride delivery to the distal tubule toward normal.
- These responses help maintain normal sodium and water excretion.
- The opposite response occurs when proximal tubular reabsorption decreases.
- Proximal tubular damage can reduce sodium chloride reabsorption.
- Heavy metal poisoning, such as mercury, can damage proximal tubules.
- Large doses of drugs such as tetracyclines can damage proximal tubules.
- Reduced proximal tubular reabsorption increases sodium chloride delivery to the distal tubule.
- Excess sodium chloride delivery could cause excessive volume depletion if not corrected.
- An important compensatory response is tubuloglomerular feedback–mediated renal vasoconstriction.
- This feedback mechanism helps ensure the proper delivery of sodium chloride to the distal tubule.
- This feedback mechanism helps ensure the proper delivery of other tubular solutes.
- This feedback mechanism helps ensure the proper delivery of tubular fluid volume.
- This allows appropriate amounts of these substances to be excreted in the urine.
KEY CONCEPT
The myogenic mechanism protects the kidney from sudden increases in blood pressure by causing rapid afferent arteriolar constriction. Tubuloglomerular feedback mainly regulates sodium chloride delivery to the distal tubule. High protein intake and hyperglycemia increase sodium reabsorption, decrease macula densa sodium chloride, cause afferent arteriolar dilation, and increase renal blood flow and GFR.
OTHER FACTORS THAT INFLUENCE RENAL BLOOD FLOW AND GFR
- Renal blood flow and GFR are low at birth.
- Renal blood flow and GFR approach normal adult levels by about 2 years of age.
- In the absence of kidney disease, renal blood flow and GFR remain relatively constant until about the fourth decade of life.
- After the fourth decade, GFR decreases by about 5% to 10% per decade.
- There is considerable variation among individuals.
Conceptual Calculation
- If GFR at age 40 = 100%
- Decline per decade = 5% to 10%
Age 50 → GFR ≈ 90% to 95%
Age 60 → GFR ≈ 80% to 90%
Age 70 → GFR ≈ 70% to 85%
- This calculation shows the gradual decline in GFR with aging.
- The decline in GFR is associated with nitric oxide deficiency.
- The decline in GFR is associated with increased oxidative stress.
- The decline in GFR is associated with loss of functional nephrons.
- Loss of functional nephrons may be partly related to increasing blood pressure.
- Loss of functional nephrons may be partly related to metabolic disorders.
- Loss of functional nephrons may be partly related to other factors that cause cumulative glomerular injury with aging.
- Men have higher renal blood flow than women.
- Men have higher GFR than women.
- This difference remains even after correction for body mass.
- Men experience a more rapid decline in GFR with aging than premenopausal women.
- The exact causes of these sex differences are not fully understood.
- Beneficial effects of estrogens may help explain these differences.
- Damaging effects of androgens may help explain these differences.
- Additional factors also influence the regulation of renal blood flow.
- Additional factors also influence the regulation of GFR.
- These factors should be considered when assessing kidney function.
KEY CONCEPT
Renal blood flow and GFR are low at birth, reach adult levels by about 2 years of age, remain relatively stable until the fourth decade, and then decline by about 5% to 10% per decade. Aging, loss of nephrons, nitric oxide deficiency, and oxidative stress contribute to this decline. Men generally have higher renal blood flow and GFR but experience a faster age-related decline than premenopausal women.
Summarized Essay
The kidneys possess powerful intrinsic autoregulatory mechanisms that maintain relatively constant renal blood flow (RBF) and glomerular filtration rate (GFR) despite large changes in arterial blood pressure. This process, known as autoregulation, can function even in kidneys removed from the body and perfused with blood, demonstrating that it is largely independent of external nervous and hormonal influences. The primary purpose of renal autoregulation is not simply to maintain oxygen delivery but to ensure stable filtration and precise control of water and solute excretion. As a result, GFR usually changes less than 10% even when arterial pressure varies between approximately 70–180 mm Hg.
Autoregulation is extremely important because small changes in GFR could produce enormous changes in urine output. Normally, the kidneys filter about 180 liters of fluid per day, reabsorb approximately 178.5 liters, and excrete only about 1.5 liters as urine. Without autoregulation, a modest increase in arterial pressure could greatly increase GFR and lead to excessive fluid loss, rapidly depleting blood volume. Therefore, autoregulatory mechanisms protect the body from dangerous fluctuations in fluid and electrolyte balance.
The most important autoregulatory mechanism is tubuloglomerular feedback (TGF). This mechanism links the amount of sodium chloride reaching the distal tubule with adjustments in renal arteriolar resistance and GFR. The TGF system is centered around the juxtaglomerular apparatus, which consists of the macula densa cells of the distal tubule and the juxtaglomerular cells of the afferent and efferent arterioles. The macula densa continuously monitors sodium chloride delivery and sends signals that help stabilize GFR.
When GFR increases, more sodium chloride reaches the macula densa. This stimulates the release of ATP and adenosine, which cause constriction of the afferent arteriole. As a result, glomerular hydrostatic pressure falls and GFR returns toward normal. At the same time, renin release is suppressed, reducing angiotensin II formation. These responses prevent excessive filtration and stabilize kidney function.
When GFR decreases, less sodium chloride reaches the macula densa. This produces the opposite effect. The afferent arteriole dilates, allowing greater blood flow into the glomerulus, while renin secretion increases. Increased renin stimulates the formation of angiotensin II, which preferentially constricts the efferent arteriole. Together, these responses raise glomerular hydrostatic pressure and help restore GFR toward normal. Through these coordinated mechanisms, GFR remains remarkably stable despite large changes in arterial pressure.
Another important autoregulatory mechanism is the myogenic mechanism. When arterial pressure increases, stretching of the afferent arteriole triggers contraction of vascular smooth muscle. This contraction increases vascular resistance and prevents excessive transmission of high pressure to the glomerular capillaries. Consequently, renal blood flow and GFR remain relatively constant and the glomeruli are protected from pressure-induced injury. This response occurs rapidly, within seconds, making it an important first line of protection against sudden changes in blood pressure.
Certain physiological conditions can alter renal blood flow and GFR. A high-protein meal increases amino acid reabsorption in the proximal tubule, which also increases sodium reabsorption. As less sodium chloride reaches the macula densa, tubuloglomerular feedback causes dilation of the afferent arteriole, increasing renal blood flow and GFR. This adaptation allows the kidneys to excrete the additional waste products generated from protein metabolism.
A similar mechanism occurs in uncontrolled diabetes mellitus. Increased glucose filtration leads to increased sodium-glucose reabsorption in the proximal tubule, reducing sodium chloride delivery to the macula densa. The resulting afferent arteriolar dilation increases renal blood flow and GFR. Persistent hyperfiltration, however, may contribute to long-term kidney damage in diabetic patients.
The opposite effect occurs when proximal tubular sodium reabsorption decreases, such as in certain toxic injuries to the tubules. Increased sodium chloride delivery to the macula densa activates tubuloglomerular feedback, causing renal vasoconstriction and reducing GFR. This protective response prevents excessive losses of sodium and water.
Several additional factors influence renal blood flow and GFR. Both are relatively low at birth and gradually reach adult levels by about two years of age. They remain fairly stable through early adulthood but decline progressively with aging due to loss of functional nephrons, reduced nitric oxide production, and cumulative kidney injury. Men generally have higher renal blood flow and GFR than women, although they also tend to experience a more rapid age-related decline in kidney function.
In summary, renal autoregulation maintains stable renal blood flow and GFR despite fluctuations in blood pressure. The two principal mechanisms are tubuloglomerular feedback and the myogenic response. Together, they ensure a constant delivery of sodium chloride to the distal tubule, prevent excessive fluid loss or retention, protect the glomeruli from injury, and maintain normal kidney function under a wide range of physiological conditions.