

- In a resting adult, the kidneys receive about 1.2–1.3 L of blood per minute.
- This is just under 25% of the cardiac output.
- Although the kidneys are small organs, they receive a very large blood supply.
- Renal blood flow (RBF) can be measured:
- Using flow meters, or
- By applying the Fick principle.
- The Fick principle calculates blood flow by:
- Measuring how much of a substance is taken up per minute.
- Dividing it by the arterial–venous concentration difference across the kidney.
- Because the kidneys filter plasma, renal plasma flow (RPF) can also be measured.
- A suitable substance for measuring RPF should:
- Be excreted by the kidney.
- Not be metabolized.
- Not be stored.
- Not be produced by the kidney.
- Not change renal blood flow.
- p-Aminohippuric acid (PAH) is commonly used to measure RPF.
- PAH is:
- Filtered by the glomerulus
- Secreted by the renal tubules
- Therefore, almost all PAH entering the kidney is removed in one circulation.
- At low PAH concentrations:
- About 90% of PAH is removed from arterial blood during one pass through the kidneys.
- This is called the PAH extraction ratio = 0.9 (90%).
- In clinical practice, renal venous PAH is not measured.
- Instead:
- Urine PAH concentration
- Urine flow rate
- Plasma PAH concentration
are measured.
- This gives the Effective Renal Plasma Flow (ERPF).
- In humans, the average ERPF is about 625 mL/min.
Formula 1: Effective Renal Plasma Flow (ERPF)
ERPF=PPAHUPAH×V
Where:
- UPAH = PAH concentration in urine
- V = Urine flow rate
- PPAH = PAH concentration in plasma
Example (Conceptual)
Given:
- Urine PAH = 14 mg/mL
- Urine flow = 0.9 mL/min
- Plasma PAH = 0.02 mg/mL
Step 1
Multiply urine concentration × urine flow14×0.9=12.6
Step 2
Divide by plasma concentration0.0212.6=630 mL/min
Answer
ERPF = 630 mL/min
This value is also called the PAH clearance.
Formula 2: Actual Renal Plasma Flow (RPF)
Because only 90% of PAH is removed,RPF=Extraction RatioERPF
Given:
- ERPF = 630 mL/min
- Extraction ratio = 0.9
Step
0.9630=700 mL/min
Answer
Actual RPF = 700 mL/min
Formula 3: Renal Blood Flow (RBF)
Since plasma is only part of whole blood,RBF=1−HematocritRPF
Given:
- RPF = 700 mL/min
- Hematocrit = 45% = 0.45
Step 1
1−0.45=0.55
Step 2
0.55700=1273 mL/min
Answer
Renal Blood Flow = 1273 mL/min (≈1.27 L/min)
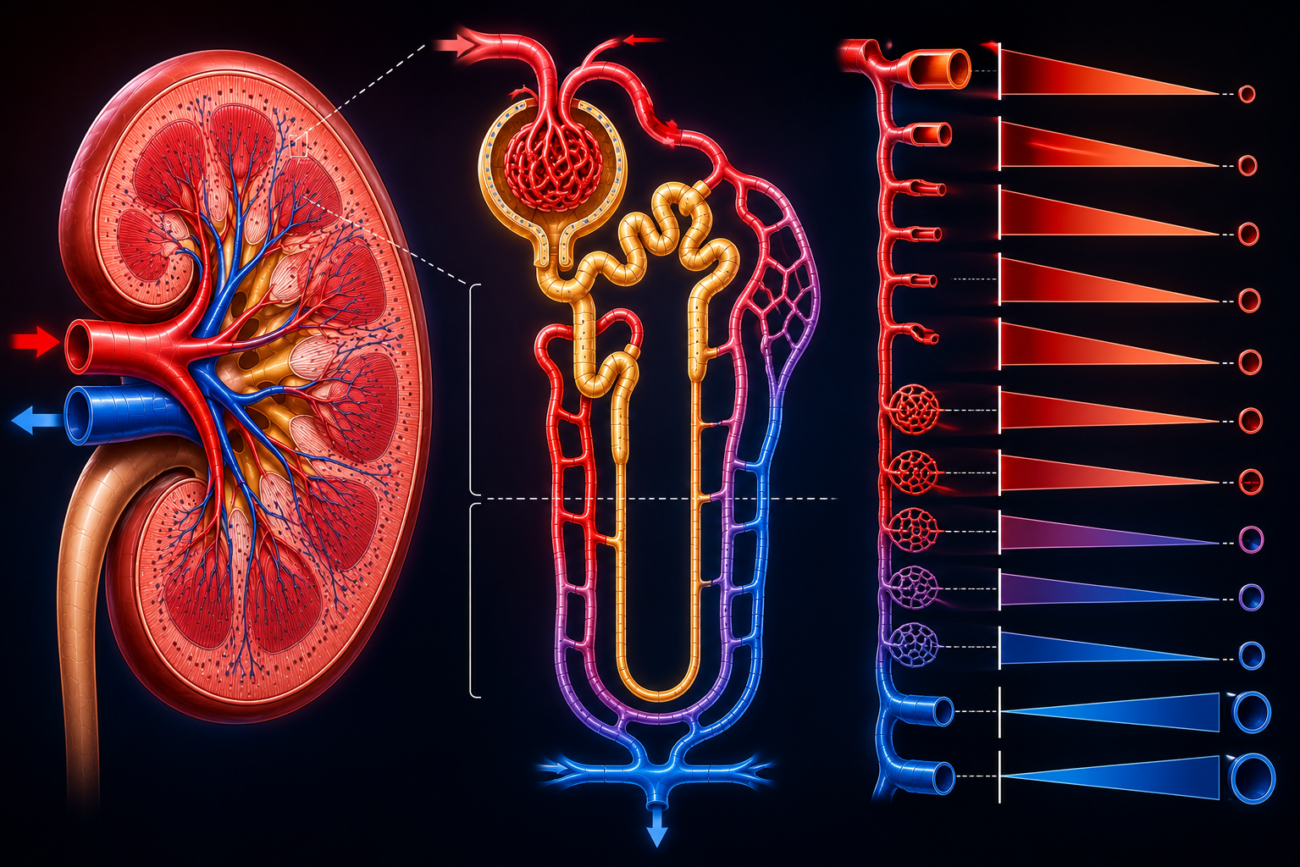
Figure 37–3
Shows the pathway of renal circulation:
Renal artery
↓
Interlobar artery
↓
Arcuate artery
↓
Interlobular artery
↓
Afferent arteriole
↓
Glomerulus
↓
Efferent arteriole
↓
Peritubular capillaries
↓
(Vasa recta in juxtamedullary nephrons)
↓
Interlobular vein
↓
Arcuate vein
↓
Interlobar vein
↓
Renal veinEasy Concept
Think of PAH as a colored dye.
Blood enters kidney
↓
PAH enters kidney
↓
Almost all PAH removed
(Filter + Tubular secretion)
↓
PAH appears in urine
↓
Amount removed tells us
how much plasma passed
through the kidneysKEY CONCEPT
- The kidneys receive about 1.2–1.3 L of blood per minute (≈25% of cardiac output). Renal plasma flow is measured using PAH because it is filtered and secreted efficiently. PAH clearance gives the Effective Renal Plasma Flow (ERPF), which can be converted to Actual Renal Plasma Flow (RPF) using the PAH extraction ratio (0.9). Renal Blood Flow (RBF) is then calculated from RPF using the hematocrit.
PRESSURE IN RENAL VESSELS
- The pressure inside the renal blood vessels varies at different parts of the kidney.
- Direct measurements in rats show that the glomerular capillary pressure is lower than previously expected.
- When the mean systemic arterial pressure is 100 mmHg:
- Glomerular capillary pressure ≈ 45 mmHg
- Therefore, the glomerular pressure is about 40% of the systemic arterial pressure.
- As blood passes through the glomerulus, the pressure falls only slightly.
- The pressure drop across the glomerulus is only about 1–3 mmHg.
- After blood enters the efferent arteriole, the pressure decreases further.
- Therefore:
- Peritubular capillary pressure ≈ 8 mmHg
- The pressure falls even more before the blood leaves the kidney.
- Renal vein pressure ≈ 4 mmHg.
- Similar pressure gradients are found in squirrel monkeys and are presumed to be similar in humans.
- Thus, in humans, glomerular capillary pressure is also about 40% of systemic arterial pressure.
Easy Concept
Think of blood flowing through a series of pipes.
Systemic Artery
100 mmHg
↓
Afferent Arteriole
↓
Glomerular Capillaries
45 mmHg
↓
(Only 1–3 mmHg pressure drop)
↓
Efferent Arteriole
↓
Peritubular Capillaries
8 mmHg
↓
Renal Vein
4 mmHgEasy Memory Trick
100 → 45 → 8 → 4
Systemic BP
↓
Glomerulus
↓
Peritubular Capillaries
↓
Renal VeinKEY CONCEPT
- When systemic arterial pressure is about 100 mmHg, glomerular capillary pressure is about 45 mmHg. Pressure falls only slightly across the glomerulus (1–3 mmHg), then drops markedly in the efferent arteriole to about 8 mmHg in the peritubular capillaries and finally to about 4 mmHg in the renal vein. This pressure gradient supports filtration in the glomerulus and reabsorption in the peritubular capillaries.
REGULATION OF THE RENAL BLOOD FLOW
- Renal blood flow is regulated by several hormones and chemical substances.
- Norepinephrine (noradrenaline):
- Causes constriction (narrowing) of the renal blood vessels.
- Its strongest effect is on:
- Interlobular arteries
- Afferent arterioles
- Dopamine:
- Is produced in the kidney.
- Causes renal vasodilation (widening of renal blood vessels).
- Also causes natriuresis (increased sodium excretion in urine).
- Angiotensin II:
- Causes vasoconstriction of both:
- Afferent arterioles
- Efferent arterioles
- Causes vasoconstriction of both:
- Prostaglandins:
- Increase blood flow in the renal cortex.
- Decrease blood flow in the renal medulla.
- Acetylcholine:
- Causes renal vasodilation.
- A high-protein diet:
- Raises glomerular capillary pressure.
- Increases renal blood flow.
Easy Concept
Think of the renal blood vessels as water pipes.
Norepinephrine
↓
Pipes Narrow
(Vasoconstriction)
↓
↓ Renal Blood FlowDopamine
↓
Pipes Widen
(Vasodilation)
↓
↑ Renal Blood Flow
+
↑ Sodium ExcretionAngiotensin II
↓
Constricts
Afferent + Efferent ArteriolesProstaglandins
↓
↑ Blood Flow → Renal Cortex
↓ Blood Flow → Renal MedullaAcetylcholine
↓
Renal VasodilationHigh-Protein Diet
↓
↑ Glomerular Pressure
↓
↑ Renal Blood FlowKEY CONCEPT
- Renal blood flow is regulated by vasoactive substances. Norepinephrine and angiotensin II constrict renal vessels, dopamine and acetylcholine dilate them, prostaglandins increase cortical but decrease medullary blood flow, and a high-protein diet increases glomerular pressure and renal blood flow.
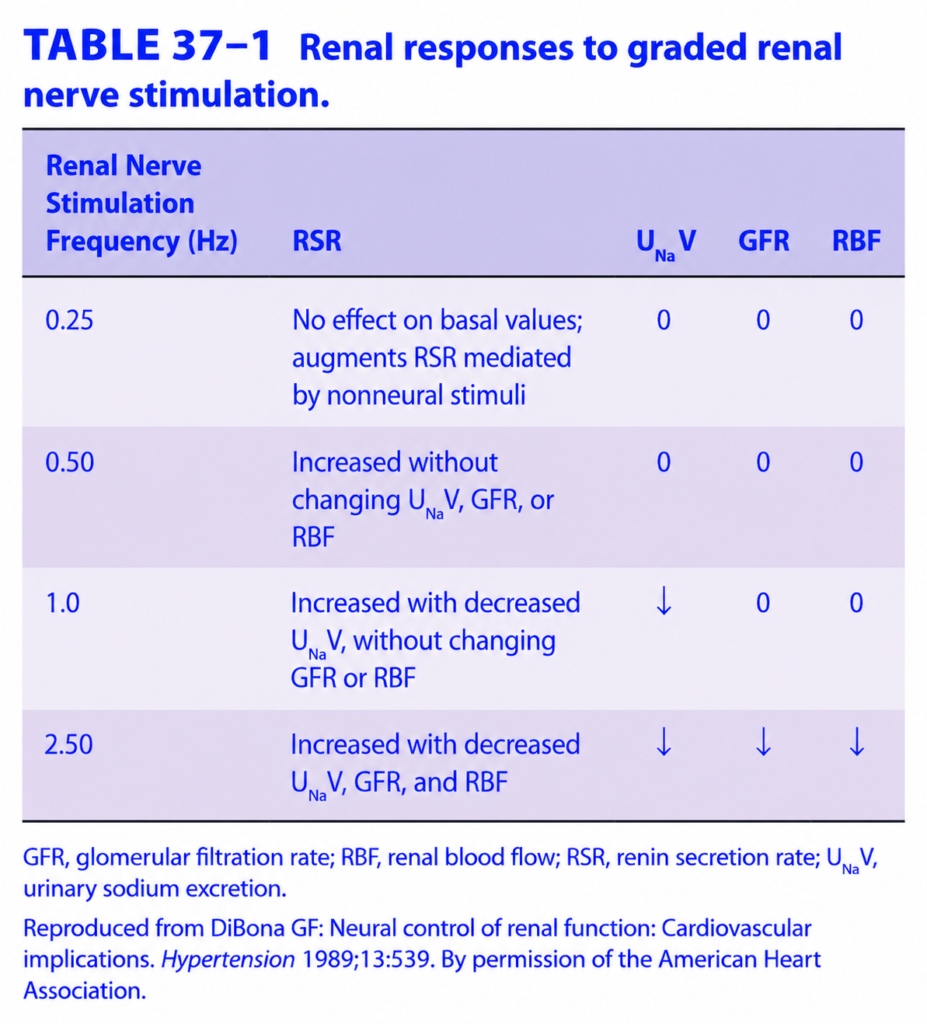
FUNCTIONS OF THE RENAL NERVES
- Stimulation of the renal nerves increases renin secretion.
- This occurs because released norepinephrine directly stimulates β₁-adrenergic receptors on the juxtaglomerular (granular) cells.
- Renal nerve stimulation also increases Na⁺ reabsorption.
- This probably occurs by the direct action of norepinephrine on renal tubular cells.
- The proximal tubule, distal tubule, and thick ascending limb of the Loop of Henle receive rich sympathetic nerve supply.
- As the strength of renal nerve stimulation increases, the responses occur in the following sequence:
1. Increased sensitivity of juxtaglomerular (granular) cells
- The first response is an increase in the sensitivity of the granular cells in the juxtaglomerular apparatus.
2. Increased renin secretion
- With stronger stimulation, renin secretion increases.
3. Increased Na⁺ reabsorption
- With further stimulation, the kidney reabsorbs more sodium (Na⁺).
4. Renal vasoconstriction
- At the highest level of stimulation:
- Renal blood vessels constrict.
- Glomerular filtration rate (GFR) decreases.
- Renal blood flow decreases.
- It is still uncertain whether the increase in Na⁺ reabsorption occurs through:
- α-adrenergic receptors
- β-adrenergic receptors
- Or both types of receptors.
- The normal physiological role of the renal nerves in sodium (Na⁺) homeostasis is still not fully understood.
- One reason is that transplanted kidneys usually function almost normally, even though:
- They initially lack functional nerve supply.
- Functional innervation develops only after some time.
- Strong sympathetic (noradrenergic) stimulation of the kidneys causes a marked decrease in renal blood flow.
- This decrease in renal blood flow is mediated mainly by:
- α₁-adrenergic receptors
- To a lesser extent by postsynaptic α₂-adrenergic receptors
- Even at rest, the renal sympathetic nerves have continuous low-level (tonic) activity.
- When systemic blood pressure falls:
- Baroreceptor activity decreases.
- This increases sympathetic outflow.
- As a result, renal vasoconstriction occurs.
- Renal blood flow also decreases:
- During exercise
- To a lesser extent when a person stands up from the supine (lying) position
Easy Concept
Think of the renal nerves as the kidney’s “sympathetic controller.”
Mild Stimulation
Renal nerves
↓
Granular cells become more sensitiveModerate Stimulation
Renal nerves
↓
↑ Renin secretionStronger Stimulation
Renal nerves
↓
↑ Na⁺ reabsorptionVery Strong Stimulation
Renal nerves
↓
α₁ receptors activated
↓
Renal vasoconstriction
↓
↓ Renal Blood Flow
↓ GFRLow Blood Pressure
↓ Blood Pressure
↓
↓ Baroreceptor firing
↓
↑ Sympathetic activity
↓
Renal vasoconstriction
↓
↓ Renal Blood FlowKEY CONCEPT
- Renal nerves regulate kidney function in a stepwise manner. Mild stimulation increases the sensitivity of juxtaglomerular cells, followed by increased renin secretion and sodium reabsorption. Strong sympathetic stimulation activates mainly α₁-adrenergic receptors, causing renal vasoconstriction, decreased renal blood flow, and reduced GFR. Renal blood flow also decreases during low blood pressure, exercise, and standing due to increased sympathetic activity.
AUTOREGULATION OF RENAL BLOOD FLOW
- Autoregulation means the kidney keeps its blood flow almost constant even when blood pressure changes.
- In dogs, autoregulation works when the renal perfusion pressure is between 90–220 mmHg.
- Within this pressure range:
- Renal vascular resistance changes automatically.
- As a result, renal blood flow remains relatively constant.
- Figure 37–4 demonstrates this relationship.
- Autoregulation is not unique to the kidney.
- Similar autoregulation also occurs in other organs.
- Renal autoregulation:
- Still occurs in denervated kidneys (without nerve supply).
- Still occurs in isolated perfused kidneys.
- Therefore, renal nerves are not essential for autoregulation.
- However, autoregulation is lost if drugs paralyze vascular smooth muscle.
- This shows that vascular smooth muscle is necessary for autoregulation.
- One important mechanism of autoregulation is:
- Stretch of the afferent arteriole
- This stretch causes the smooth muscle to contract automatically (myogenic response).
- This helps keep renal blood flow constant.
- Nitric oxide (NO) may also contribute to renal autoregulation.
- At low renal perfusion pressure:
- Angiotensin II also helps maintain kidney function.
- It constricts the efferent arteriole.
- This helps maintain the glomerular filtration rate (GFR) despite reduced blood pressure.
- This mechanism explains why some patients with poor renal perfusion develop renal failure after receiving ACE inhibitors.
- ACE inhibitors reduce angiotensin II formation.
- Without angiotensin II:
- Efferent arterioles cannot constrict adequately.
- GFR falls further.
- Renal failure may develop.
Figure 37–4
- Shows that:
- Between 90–220 mmHg, renal blood flow remains almost constant despite changes in blood pressure.
- This occurs because the renal blood vessels automatically adjust their resistance.
Easy Concept
Think of the kidney as having an automatic water-flow regulator.
Normal Autoregulation
Blood Pressure
90 → 220 mmHg
↓
Kidney adjusts vessel resistance automatically
↓
Renal Blood Flow stays almost constantLow Blood Pressure
↓ Renal Perfusion Pressure
↓
Angiotensin II
↓
Constricts Efferent Arteriole
↓
Maintains GFRACE Inhibitor in Poor Renal Perfusion
ACE Inhibitor
↓
↓ Angiotensin II
↓
Efferent arteriole cannot constrict
↓
GFR falls
↓
Possible Renal FailureEasy Memory Trick
Autoregulation
Pressure Changes
↓
Afferent arteriole adjusts itself
(Myogenic response)
↓
Stable Renal Blood FlowLow BP
↓
Angiotensin II
↓
Efferent arteriole constricts
↓
Maintains GFRKEY CONCEPT
- Renal autoregulation maintains nearly constant renal blood flow between perfusion pressures of about 90–220 mmHg by automatically changing renal vascular resistance. It depends mainly on the myogenic contraction of the afferent arteriole and may also involve nitric oxide (NO). During low perfusion pressure, angiotensin II constricts the efferent arteriole to preserve GFR, which explains why ACE inhibitors can sometimes precipitate renal failure in patients with poor renal perfusion.
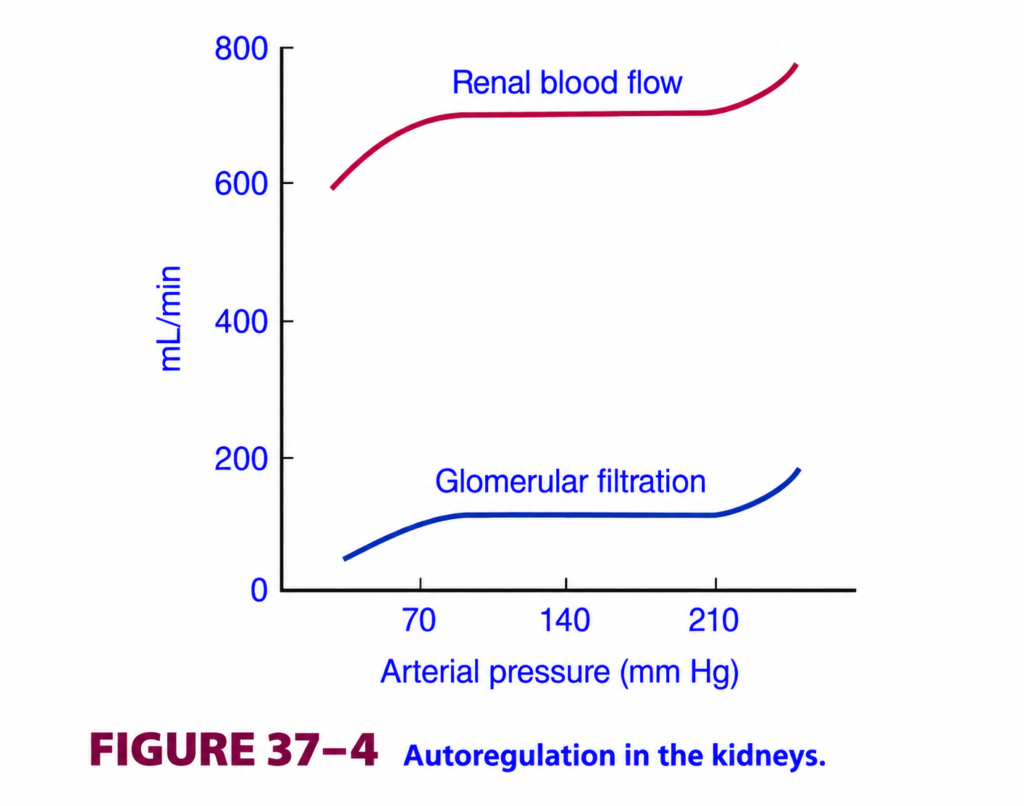
This is Figure 37.4 from Ganong Physiology, and it explains one of the most important concepts in renal physiology:
⭐ Renal Autoregulation
This graph answers the question:
How do the kidneys keep renal blood flow (RBF) and glomerular filtration rate (GFR) almost constant even when blood pressure changes?
The answer is:
The kidneys automatically adjust the resistance of their blood vessels (mainly the afferent arteriole).
This automatic mechanism is called Autoregulation.
🎯 One-Line Concept
Between about 80 and 180 mmHg (approximately 90–180 mmHg in humans), the kidneys maintain nearly constant renal blood flow (RBF) and glomerular filtration rate (GFR) despite changes in arterial pressure.
Simply,
- Blood pressure ↑ → Kidneys constrict renal arterioles → RBF & GFR stay almost constant.
- Blood pressure ↓ → Kidneys dilate renal arterioles → RBF & GFR stay almost constant.
First Understand Why This Is Needed
Imagine if the kidneys had no autoregulation.
Suppose blood pressure changes.
Blood Pressure = 80 mmHg
↓
Kidneys receive little blood.
↓
Very little urine forms.
Now,
Blood Pressure = 180 mmHg
↓
Huge amount of blood enters kidneys.
↓
Massive filtration occurs.
↓
Large water and salt loss.
This would be dangerous.
So,
the kidneys prevent this by autoregulation.
Step 1: Understand the Axes
X-Axis (Horizontal)
Arterial Pressure (mmHg)
This is the
Systemic arterial blood pressure.
Starts around
50 mmHg
↓
250 mmHg
Easy Memory
Move right
↓
Higher blood pressure
Move left
↓
Lower blood pressure
Y-Axis (Vertical)
Flow (mL/min)
This axis shows
two different things:
- Upper curve = Renal Blood Flow (RBF)
- Lower curve = Glomerular Filtration Rate (GFR)
Upper Curve
⭐ Renal Blood Flow (RBF)
Normal value
≈ 700 mL/min (as shown in this graph)
In most physiology texts, total renal blood flow is about 1.1–1.3 L/min (≈20–25% of cardiac output). This figure is illustrating the autoregulation pattern, not emphasizing the exact human value.
Lower Curve
⭐ Glomerular Filtration Rate (GFR)
Normal value
≈ 120–125 mL/min
This graph shows approximately
120 mL/min.Look at the Shape
Notice
Both curves have
three regions.
Region 1
Low Blood Pressure
Left side of graph
Pressure
below about
80 mmHg
What Happens?
Blood pressure is too low.
Kidneys cannot completely compensate.
Therefore,
RBF falls.
GFR also falls.
Why?
Not enough pressure is available
to push blood through the kidneys.
Clinical Examples
- Severe hemorrhage
- Shock
- Severe dehydration
Region 2
Plateau
This is
the most important region.
Pressure
approximately
80–180 mmHg (about 90–180 mmHg in many human physiology texts).
What Happens?
Blood pressure changes.
But
RBF hardly changes.
GFR hardly changes.
Both remain almost constant.
Why?
Because of
Autoregulation
Easy Memory
Pressure changes
↓
Kidneys automatically adjust
↓
Flow stays constant
Region 3
Very High Blood Pressure
Pressure
above
180–200 mmHg
What Happens?
Autoregulation reaches its limit.
Now
both
RBF
and
GFR
begin to rise again.Why?
Renal blood vessels cannot constrict any further.
Therefore,
extra pressure enters the glomeruli.
Why Is the Plateau Flat?
This is the key question.
Suppose
Blood pressure increases
from
100
↓
160 mmHg.
Normally,
blood flow should increase.
But it doesn’t.
Why?
Because
the kidneys increase
vascular resistance.
Therefore,
blood flow remains constant.
The Kidney Behaves Like a Smart Tap
Imagine
A garden hose.
Water pressure suddenly increases.
Normally,
more water flows.
Now imagine
someone partially closes the tap.
The water flow remains almost the same.
Exactly the same happens in kidneys.
How Do Kidneys Do This?
Two major mechanisms.
① Myogenic Mechanism
This is the
fastest mechanism.
Suppose
Blood pressure suddenly increases.
↓
Afferent arteriole stretches.
↓
Smooth muscle contracts automatically.
↓
Blood vessel narrows.
↓
Blood flow returns toward normal.
Suppose
Blood pressure falls.
↓
Stretch decreases.
↓
Smooth muscle relaxes.
↓
Blood vessel dilates.
↓
Blood flow increases.
Easy Memory
Stretch
↓
Contraction
No stretch
↓
Relaxation
② Tubuloglomerular Feedback
This is slightly slower.
It involves
the
Macula Densa
of the juxtaglomerular apparatus.
High GFR
↓
More NaCl reaches macula densa.
↓
Macula densa signals
afferent arteriole
to constrict.
↓
GFR falls back toward normal.
Low GFR
↓
Less NaCl reaches macula densa.
↓
Macula densa causes
afferent arteriole dilation
and stimulates renin release.
↓
GFR rises toward normal.
Understanding the Upper Curve
Suppose
Pressure increases
80
↓
160 mmHg.
Renal blood flow remains
almost
700 mL/min.
Why?
Kidneys increase vascular resistance.
Thus,
blood flow hardly changes.
Understanding the Lower Curve
Now
look at GFR.
Pressure changes greatly.
But
GFR remains
around
120 mL/min.
Why Is This Important?
Because
constant GFR means
stable urine formation,
stable electrolyte excretion,
and stable body fluid balance.
Why Is Autoregulation So Important?
Without autoregulation
Even small BP changes
would produce
large urine changes.
This would cause
- Dehydration
- Fluid overload
- Sodium imbalance
- Blood pressure instability
Autoregulation prevents all of these.
Clinical Correlation
1. Exercise
Blood pressure increases.
Despite this,
kidneys maintain
nearly constant GFR.
2. Mild Hypertension
Blood pressure rises.
Autoregulation protects glomeruli
within its operating range.
3. Severe Hypotension
Blood pressure falls below the autoregulatory range.
Now
RBF
↓
GFR
↓
Urine output decreases.
This can contribute to acute kidney injury if prolonged.
4. Severe Hypertension
Blood pressure exceeds autoregulatory capacity.
Now
GFR rises.
Glomerular capillaries are exposed to excessive pressure,
which may contribute to kidney damage over time.
High-Yield MBBS Viva Points
Normal Values
| Parameter | Value |
|---|---|
| Renal Blood Flow (RBF) | ≈1.2 L/min (about 20–25% of cardiac output) |
| Glomerular Filtration Rate (GFR) | ≈125 mL/min |
| Autoregulation Range | ≈80–180 mmHg (about 90–180 mmHg in many texts) |
Compare the Three Regions
| Blood Pressure | RBF | GFR | Explanation |
|---|---|---|---|
| Low (<80–90 mmHg) | ↓ | ↓ | Autoregulation fails because perfusion pressure is too low |
| Normal (≈80–180 mmHg) | Constant | Constant | Autoregulation maintains stable kidney function |
| Very High (>180–200 mmHg) | ↑ | ↑ | Autoregulatory mechanisms are overwhelmed |
Super Easy Memory Story
Imagine a water tank supplying a factory.
- 🚰 Water pressure = Blood pressure
- 🏭 Factory = Kidney
- 💧 Water flow = Renal blood flow
Situation 1
Pressure increases.
The factory partly closes the valve.
Water flow stays the same.
↓
Autoregulation.
Situation 2
Pressure decreases.
The factory opens the valve wider.
Water flow stays almost the same.
↓
Autoregulation.
Situation 3
Pressure becomes extremely high.
The valve is already fully closed.
Now
extra water still enters.
↓
Autoregulation fails.
🎯 MBBS Golden Rule
Renal Autoregulation
- ↑ Blood Pressure → Afferent arteriole constricts → RBF & GFR remain nearly constant
- ↓ Blood Pressure → Afferent arteriole dilates → RBF & GFR remain nearly constant
Two Main Mechanisms
- Myogenic mechanism
- Tubuloglomerular feedback (Macula densa)
Final Concept to Never Forget
The central message of Figure 37.4 is that the kidneys are self-regulating organs.
Within a broad physiological blood pressure range, they automatically adjust the tone of the renal arterioles so that:
- Renal blood flow remains nearly constant.
- Glomerular filtration rate remains nearly constant.
- Urine formation and body fluid balance remain stable despite everyday fluctuations in arterial pressure.
This remarkable autoregulatory ability is essential for maintaining normal kidney function and overall homeostasis.
prepare and written by ceo and founder Dr sheen medical lectures